
Epidemiology of HCV and HBV in a High Endemic Area of Southern Italy: Opportunities from the COVID-19 Pandemic—Standardized National Screening or One Tailored to Local Epidemiology?

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Regional Context of the Study
2.4. Laboratory Evaluation
2.5. Data Analysis
3. Results
3.1. General Characteristics of the Population
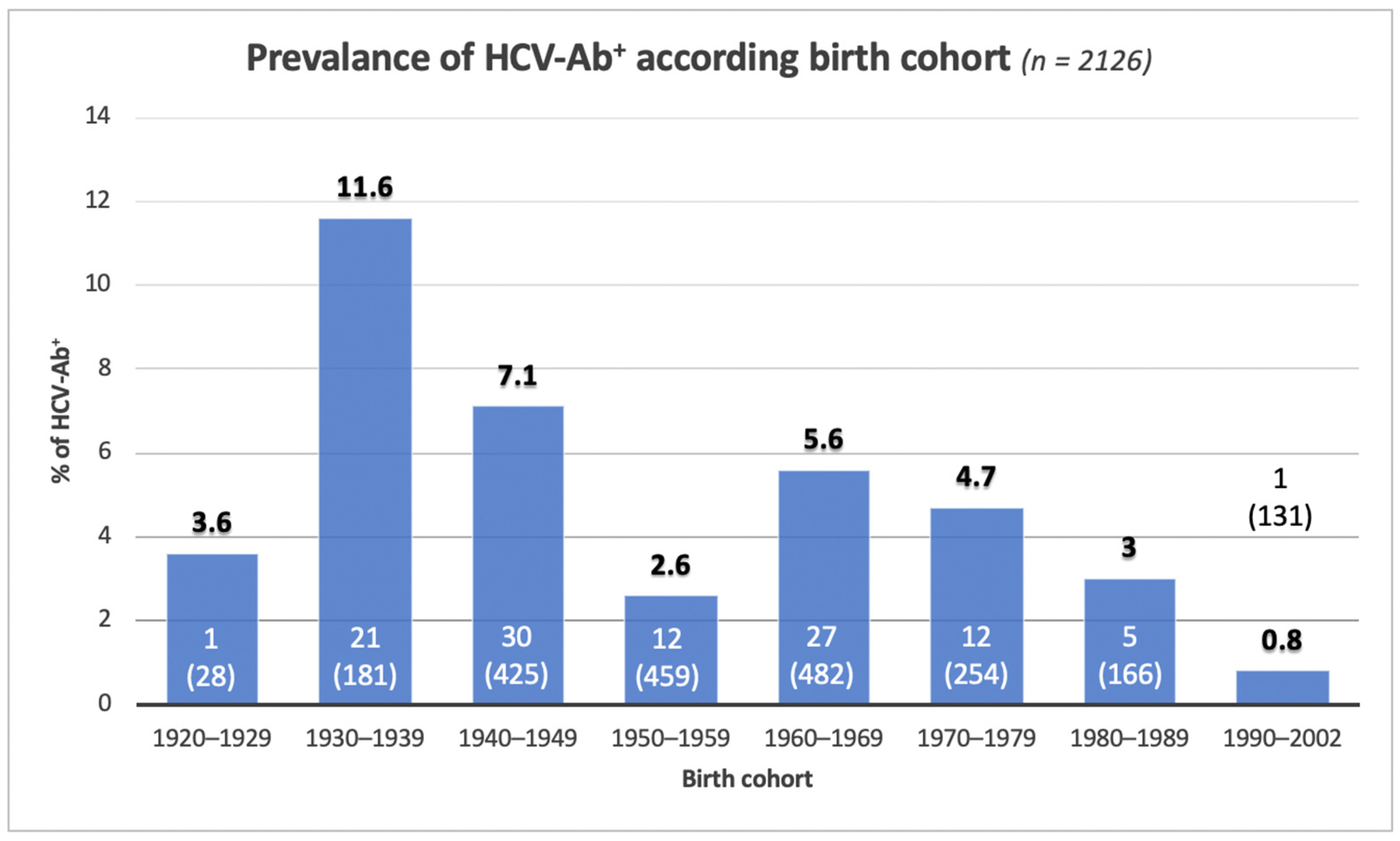
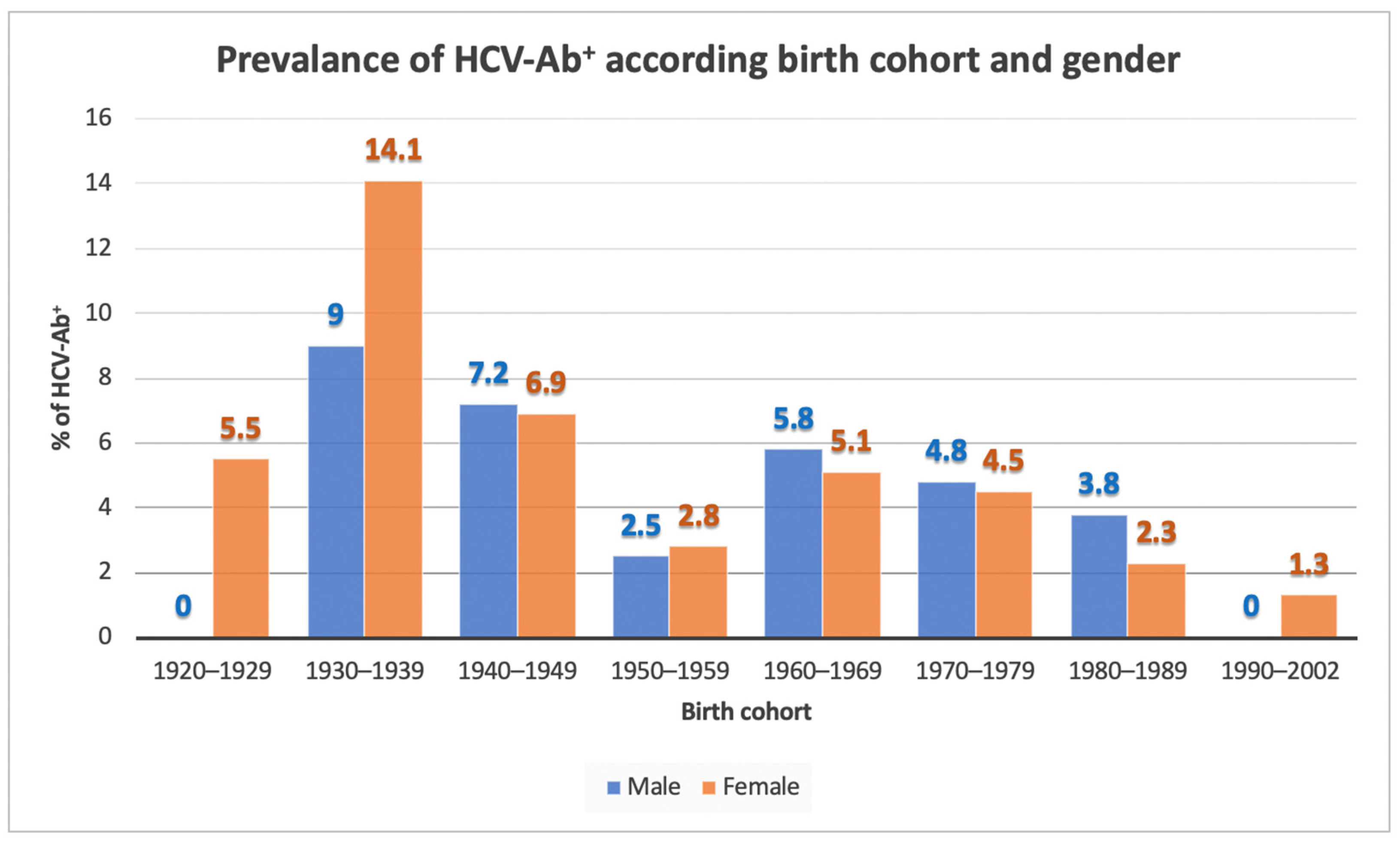
3.2. HCV-Ab Screening
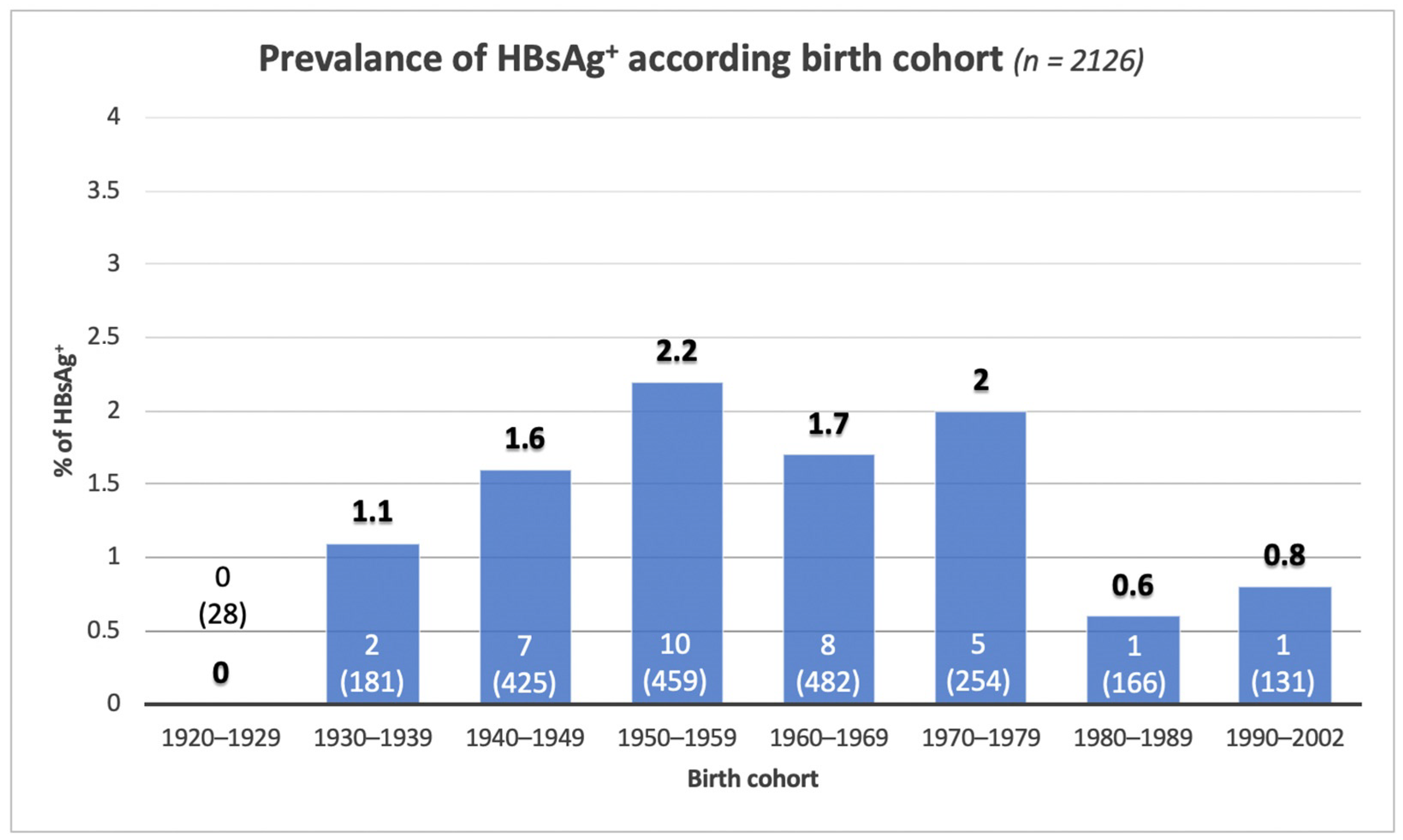
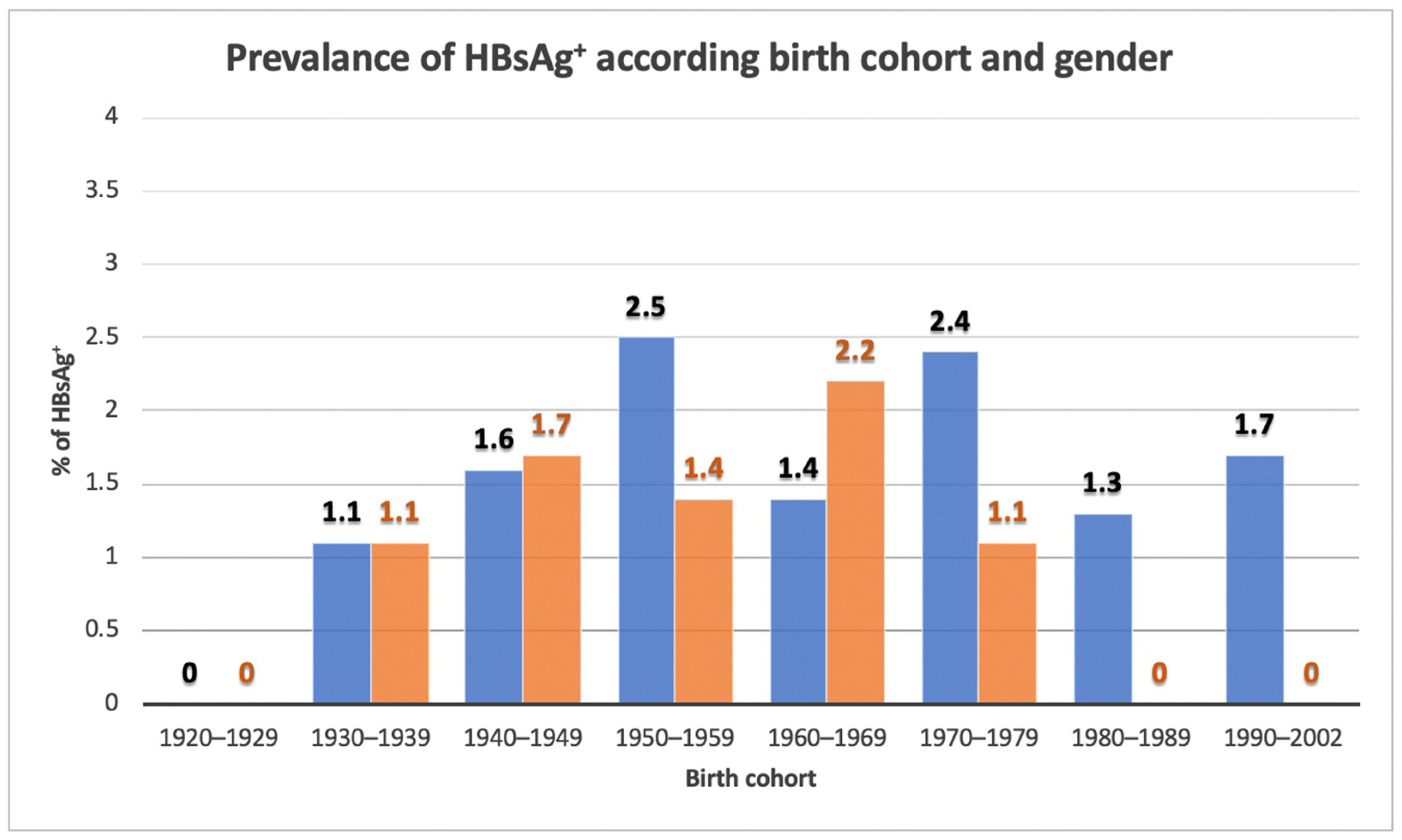
3.3. HBV Screening
3.4. Co-Infection HBV/HCV
3.5. Distribution of HCV-Ab Accordingly to Current Italian Health Ministry Screening Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Krassenburg, L.A.P.; Maan, R.; Ramji, A.; Manns, M.P.; Cornberg, M.; Wedemeyer, H.; de Knegt, R.J.; Hansen, B.E.; Janssen, H.L.A.; de Man, R.A.; et al. Clinical outcomes following DAA therapy in patients with HCV-related cirrhosis depend on disease severity. J. Hepatol. 2021, 74, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Politi, J.; Guerras, J.M.; Donat, M.; Belza, M.J.; Ronda, E.; Barrio, G.; Regidor, E. Favorable impact in hepatitis C-related mortality following free access to direct-acting antivirals in Spain. Hepatology, 2021; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Nevola, R.; Rinaldi, L.; Zeni, L.; Romano, C.; Marrone, A.; Galiero, R.; Pafundi, P.C.; Acierno, C.; Vetrano, E.; Adinolfi, L.E. Changes in clinical scenarios, management, and perspectives of patients with chronic hepatitis C after viral clearance by direct-acting antivirals. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 643–656. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Sector Strategies on Viral Hepatitis 2016–2021. Available online: http://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_32-en.pdf?ua=1 (accessed on 26 February 2022).
- Kondili, L.A.; Craxì, A.; Aghemo, A. Absolute targets for HCV elimination and national health policy paradigms: Foreseeing future requirements. Liver Int. 2021, 41, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Kondili, L.A.; Blach, S.; Razavi, H.; Craxì, A. Tailored screening and dedicated funding for direct acting antiviral drugs: How to keep Italy on the road to hepatitis C virus elimination? Ann. Ist. Super Sanita 2020, 56, 325–329. [Google Scholar] [CrossRef]
- Blach, S.; Kondili, L.A.; Aghemo, A.; Cai, Z.; Dugan, E.; Estes, C.; Gamkrelidze, I.; Ma, S.; Pawlotsky, J.M.; Razavi-Shearer, D.; et al. Impact of COVID-19 on global HCV elimination efforts. J. Hepatol. 2021, 74, 31–36. [Google Scholar] [CrossRef]
- Polaris Observatory HCV Collaborators. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: A modelling study. Lancet Gastroenterol. Hepatol. 2017, 2, 161–176. [Google Scholar] [CrossRef] [Green Version]
- Sroczynski, G.; Esteban, E.; Conrads-Frank, A.; Schwarzer, R.; Mühlberger, N.; Wright, D.; Zeuzem, S.; Siebert, U. Long-term effectiveness and cost-effectiveness of screening for hepatitis C virus infection. Eur. J. Public Health 2009, 19, 245–253. [Google Scholar] [CrossRef] [Green Version]
- Guadagnino, V.; Stroffolini, T.; Caroleo, B.; Menniti Ippolito, F.; Rapicetta, M.; Ciccaglione, A.R.; Chionne, P.; Madonna, E.; Costantino, A.; De Sarro, G.; et al. Sersale’s Study Group. Hepatitis C virus infection in an endemic area of Southern Italy 14 years later: Evidence for a vanishing infection. Dig. Liver Dis. 2013, 45, 403–407. [Google Scholar] [CrossRef]
- Maio, G.; d’Argenio, P.; Stroffolini, T.; Bozza, A.; Sacco, L.; Tosti, M.E.; Intorcia, M.; Fossi, E.; d’Alessio, G.; Kondili, L.A.; et al. Hepatitis C virus infection and alanine transaminase levels in the general population: A survey in a southern Italian town. J. Hepatol. 2000, 33, 116–120. [Google Scholar] [CrossRef]
- Gazzetta Ufficiale della Repubblica Italiana–Ministero della Salute. Available online: https://www.gazzettaufficiale.it/eli/id/2021/07/08/21A04075/sg. (accessed on 26 February 2022).
- Chiaramonte, M.; Stroffolini, T.; Caporaso, N.; Coppola, R.; Craxì, A.; Gaeta, G.B.; Sagnelli, E.; Zanetti, A.R. Hepatitis-C virus infection in Italy: A multicentric sero-epidemiological study (a report from the HCV study group of the Italian Association for the Study of the Liver). Ital. J. Gastroenterol. 1991, 23, 555–558. [Google Scholar] [PubMed]
- Guadagnino, V.; Stroffolini, T.; Rapicetta, M.; Costantino, A.; Kondili, L.A.; Menniti-Ippolito, F.; Caroleo, B.; Costa, C.; Griffo, G.; Loiacono, L.; et al. Prevalence, risk factors, and genotype distribution of hepatitis C virus infection in the general population: A community-based survey in southern Italy. Hepatology 1997, 26, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Lai, A.; Sagnelli, C.; Presti, A.L.; Cella, E.; Angeletti, S.; Spoto, S.; Costantino, S.; Sagnelli, E.; Ciccozzi, M. What is changed in HBV molecular epidemiology in Italy? J. Med. Virol. 2018, 90, 786–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancusi, R.L.; Andreoni, M.; d’Angela, D.; Sarrecchia, C.; Spandonaro, F. Epidemiological burden estimates for pathologies with a nonconstant risk: An application to HCV in Italy according to age, Metavir score, and genotype: A systematic review and meta-analysis. Medicine 2016, 95, e5143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andriulli, A.; Stroffolini, T.; Mariano, A.; Valvano, M.R.; Grattagliano, I.; Ippolito, A.M.; Grossi, A.; Brancaccio, G.; Coco, C.; Russello, M.; et al. Declining prevalence and increasing awareness of HCV infection in Italy: A population-based survey in five metropolitan areas. Eur. J. Intern. Med. 2018, 53, 79–84. [Google Scholar] [CrossRef]
- Stroffolini, T.; Sagnelli, E.; Sagnelli, C.; Smedile, A.; Morisco, F.; Coppola, N.; Furlan, C.; Almasio, P.L. Geographical pattern of chronic liver diseases in Italy: Results from two pooled national surveys. Eur. J. Intern. Med. 2019, 61, 40–43. [Google Scholar] [CrossRef] [Green Version]
- Ansaldi, F.; Bruzzone, B.; Salmaso, S.; Rota, M.C.; Durando, P.; Gasparini, R.; Icardi, G. Different seroprevalence and molecular epidemiology patterns of hepatitis C virus infection in Italy. J. Med. Virol. 2005, 76, 327–332. [Google Scholar] [CrossRef]
- Montella, M.; Crispo, A.; Serraino, D.; Rezza, G.; Franceschi, S. Is the spread of HCV in Southern Italy attributable to iatrogenic transmission through unsterile injections? Eur. J. Cancer Prev. 2003, 12, 85–86. [Google Scholar] [CrossRef]
- Fusco, M.; Girardi, E.; Piselli, P.; Palombino, R.; Polesel, J.; Maione, C.; Scognamiglio, P.; Pisanti, F.A.; Solmone, M.; Di Cicco, P.; et al. Epidemiology of viral hepatitis infections in an area of southern Italy with high incidence rates of liver cancer. Eur. J. Cancer 2008, 44, 847–853. [Google Scholar] [CrossRef]
- Morisco, F.; Loperto, I.; Stroffolini, T.; Lombardo, F.L.; Cossiga, V.; Guarino, M.; De Feo, A.; Caporaso, N. Prevalence and risk factors of HCV infection in a metropolitan area in southern Italy: Tail of a cohort infected in past decades. J. Med. Virol. 2017, 89, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, C.; Bartolacci, S.; Pepe, P.; Monnini, M.; Voller, F.; Cipriani, F.; Stasi, C. Attempt to calculate the prevalence and features of chronic hepatitis C infection in Tuscany using administrative data. World J. Gastroenterol. 2016, 22, 9829–9835. [Google Scholar] [CrossRef] [PubMed]
- Kondili, L.A.; Chionne, P.; Costantino, A.; Villano, U.; Lo Noce, C.; Pannozzo, F.; Mele, A.; Giampaoli, S.; Rapicetta, M. Infection rate and spontaneous seroreversion of anti-hepatitis C virus during the natural course of hepatitis C virus infection in the general population. Gut 2002, 50, 693–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polilli, E.; Tontodonati, M.; Flacco, M.E.; Ursini, T.; Striani, P.; Di Giammartino, D.; Paoloni, M.; Vallarola, L.; Pressanti, G.L.; Fragassi, G.; et al. High seroprevalence of HCV in the Abruzzo Region, Italy: Results on a large sample from opt-out pre-surgical screening. Infection 2016, 44, 85–91. [Google Scholar] [CrossRef]
- Giacomelli, A.; Pagani, G.; Conti, F.; Bassoli, C.; Galli, M. Detecting HCV infection by means of mass population SARS-CoV-2 screening: A pilot experience in Northern Italy. J Hepatol. 2021, 75, 484–486. [Google Scholar] [CrossRef]
- Di Stefano, R.; Stroffolini, T.; Ferraro, D.; Usticano, A.; Valenza, L.M.; Montalbano, L.; Pomara, G.; Craxì, A. Endemic hepatitis C virus infection in a Sicilian town: Further evidence for iatrogenic transmission. J. Med. Virol. 2002, 67, 339–344. [Google Scholar] [CrossRef]
- Cozzolongo, R.; Osella, A.R.; Elba, S.; Petruzzi, J.; Buongiorno, G.; Giannuzzi, V.; Leone, G.; Bonfiglio, C.; Lanzilotta, E.; Manghisi, O.G.; et al. Epidemiology of HCV infection in the general population: A survey in a southern Italian town. Am. J. Gastroenterol. 2009, 104, 2740–2746. [Google Scholar] [CrossRef]
- Fabris, P.; Baldo, V.; Baldovin, T.; Bellotto, E.; Rassu, M.; Trivello, R.; Tramarin, A.; Tositti, G.; Floreani, A. Changing epidemiology of HCV and HBV infections in Northern Italy: A survey in the general population. J. Clin. Gastroenterol. 2008, 42, 527–532. [Google Scholar] [CrossRef]
- Frank, C.; Mohamed, M.K.; Strickland, G.T.; Lavanchy, D.; Arthur, R.R.; Magder, L.S.; El Khoby, T.; Abdel-Wahab, Y.; Aly Ohn, E.S.; Anwar, W.; et al. The role of parenteral antischistosomal therapy in the spread of hepatitis C virus in Egypt. Lancet 2000, 355, 887–891. [Google Scholar] [CrossRef]
- Scognamiglio, P.; Piselli, P.; Fusco, M.; Pisanti, F.A.; Serraino, D.; Ippolito, G.; Girardi, E.; Collaborating Study Group. Declining unawareness of HCV-infection parallel to declining prevalence in Southern Italy. J. Med. Virol. 2017, 89, 1691–1692. [Google Scholar] [CrossRef]
- Puoti, M.; Girardi, E. Chronic hepatitis C in Italy: The vanishing of the first and most consistent epidemic wave. Dig. Liver Dis. 2013, 45, 369–370. [Google Scholar] [CrossRef] [PubMed]
- Sagnelli, E.; Stroffolini, T.; Sagnelli, C.; Pirisi, M.; Babudieri, S.; Colloredo, G.; Russello, M.; Coppola, N.; Gaeta, G.B.; Cacopardo, B.; et al. Gender differences in chronic liver diseases in two cohorts of 2001 and 2014 in Italy. Infection 2018, 46, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Crespo, J.; Díaz-González, Á.; Iruzubieta, P.; Llerena, S.; Cabezas, J. SARS-CoV-2 massive testing: A window of opportunity to catch up with HCV elimination. J. Hepatol. 2021, 74, 966–967. [Google Scholar] [CrossRef] [PubMed]
- Calvaruso, V.; Craxì, A. Hepatic benefits of HCV cure. J. Hepatol. 2020, 73, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Coppola, C.; Narciso, V.; Nevola, R.; Rinaldi, L.; Calvaruso, V.; Staiano, L.; Di Marco, V.; et al. Impact of hepatitis C virus clearance by direct-acting antiviral treatment on the incidence of major cardiovascular events: A prospective multicentre study. Atherosclerosis 2020, 296, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Nevola, R.; Coppola, C.; Narciso, V.; Rinaldi, L.; Calvaruso, V.; Pafundi, P.C.; Lombardi, R.; et al. Reduced incidence of type 2 diabetes in patients with chronic hepatitis C virus infection cleared by direct-acting antiviral therapy: A prospective study. Diabetes Obes. Metab. 2020, 22, 2408–2416. [Google Scholar] [CrossRef]
- Nevola, R.; Rinaldi, L.; Zeni, L.; Sasso, F.C.; Pafundi, P.C.; Guerrera, B.; Marrone, A.; Giordano, M.; Adinolfi, L.E. Metabolic and renal changes in patients with chronic hepatitis C infection after hepatitis C virus clearance by direct-acting antivirals. JGH Open 2020, 4, 713–721. [Google Scholar] [CrossRef]
- Istituto Nazionale di Statistica (I.STAT). Available online: http://dati.istat.it/Index.aspx?QueryId=42869 (accessed on 26 February 2022).
- Kondili, L.A.; Robbins, S.; Blach, S.; Gamkrelidze, I.; Zignego, A.L.; Brunetto, M.R.; Raimondo, G.; Taliani, G.; Iannone, A.; Russo, F.P.; et al. PITER Collaborating Group. Forecasting Hepatitis C liver disease burden on real-life data. Does the hidden iceberg matter to reach the elimination goals? Liver Int. 2018, 38, 2190–2198. [Google Scholar] [CrossRef] [Green Version]
- Kondili, L.A.; Gamkrelidze, I.; Blach, S.; Marcellusi, A.; Galli, M.; Petta, S.; Puoti, M.; Vella, S.; Razavi, H.; Craxi, A.; et al. Optimization of hepatitis C virus screening strategies by birth cohort in Italy. Liver Int. 2020, 40, 1545–1555. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | AOU Vanvitelli Naples | Cotugno Hospital Naples | Betania Evangelical Hospital Naples | AORN “Sant’Anna e San Sebastiano” Caserta | ||||
|---|---|---|---|---|---|---|---|---|
| Internal Medicine Unit | Infectious Diseases Unit | Infectious Diseases and Neurology Unit | IVth Division of Immunodeficiency and Gender Infectious Diseases | IIIrd Infectious Diseases Unit | Internal Medicine Unit | Infectious Diseases Unit and COVID Centers | ||
| Admitted patients, n | 2361 | 208 | 403 | 207 | 205 | 219 | 124 | 995 |
| Evaluated patients, n (%) | 2126 (90) | 191 (91.8) | 390 (96.8) | 201 (97.1) | 179 (87.3) | 138 (63.0) | 109 (87.9) | 918 (92.3) |
| Male, n (%) | 1313 (61.8) | 114 (59.7) | 216 (55.4) | 151 (75.1) | 111 (62.0) | 97 (70.3) | 40 (36.7) | 584 (58.7) |
| Age, median (IQR), y | 62 (50–73) | 63 (53–73) | 57 (42–69) | 61 (50–69) | 61 (52–72) | 59 (51–69) | 65 (38–76) | 64 (52–75) |
| Birth cohort | ||||||||
| 1920–1929, n (%) | 28 (1.3) | 3 (1.6) | 1 (0.3) | 1 (0.5) | 1 (0.9) | 1 (0.7) | 3 (2.7) | 18 (2) |
| 1930–1939, n (%) | 181 (8.5) | 16 (8.4) | 18 (4.6) | 10 (5) | 13 (7.3) | 7 (5.1) | 11 (10.1) | 106 (11.5) |
| 1940–1949, n (%) | 425 (20) | 39 (20.4) | 64 (16.4) | 35 (17.4) | 36 (20.1) | 19 (13.8) | 30 (27.5) | 202 (22) |
| 1950–1959, n (%) | 459 (21.6) | 46 (24.1) | 76 (19.5) | 58 (28.9) | 40 (22.3) | 37 (26.8) | 17 (15.6) | 185 (20.1) |
| 1960–1969, n (%) | 482 (22.7) | 51 (26.7) | 89 (22.8) | 47 (23.4) | 48 (26.8) | 39 (28.3) | 11 (10.1) | 197 (21.5) |
| 1970–1979, n (%) | 254 (11.9) | 22 (11.5) | 51 (13.1) | 30 (15.9) | 23 (12.8) | 25 (18.1) | 7 (6.4) | 96 (10.5) |
| 1980–1989, n (%) | 166 (7.8) | 10 (5.2) | 56 (14.4) | 9 (4.5) | 15 (8.4) | 9 (6.5) | 14 (12.8) | 53 (5.8) |
| 1990–2002, n (%) | 131 (6.2) | 4 (2.1) | 35 (9) | 11 (5.5) | 3 (1.7) | 1 (0.7) | 16 (14.7) | 61 (6.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nevola, R.; Messina, V.; Marrone, A.; Coppola, N.; Rescigno, C.; Esposito, V.; Sangiovanni, V.; Claar, E.; Pisaturo, M.; Fusco, F.M.; et al. Epidemiology of HCV and HBV in a High Endemic Area of Southern Italy: Opportunities from the COVID-19 Pandemic—Standardized National Screening or One Tailored to Local Epidemiology? Biology 2022, 11, 609. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11040609
Nevola R, Messina V, Marrone A, Coppola N, Rescigno C, Esposito V, Sangiovanni V, Claar E, Pisaturo M, Fusco FM, et al. Epidemiology of HCV and HBV in a High Endemic Area of Southern Italy: Opportunities from the COVID-19 Pandemic—Standardized National Screening or One Tailored to Local Epidemiology? Biology. 2022; 11(4):609. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11040609
Chicago/Turabian StyleNevola, Riccardo, Vincenzo Messina, Aldo Marrone, Nicola Coppola, Carolina Rescigno, Vincenzo Esposito, Vincenzo Sangiovanni, Ernesto Claar, Mariantonietta Pisaturo, Francesco Maria Fusco, and et al. 2022. "Epidemiology of HCV and HBV in a High Endemic Area of Southern Italy: Opportunities from the COVID-19 Pandemic—Standardized National Screening or One Tailored to Local Epidemiology?" Biology 11, no. 4: 609. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11040609