
Acute Cardiorespiratory and Metabolic Responses to Incremental Cycling Exercise in Endurance- and Strength-Trained Athletes


 , , ,
, , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Eligibility Criteria
2.2. Ethical Approval
2.3. Design and Procedures
2.4. Pre-Test Preparation
2.5. Anthropometry
2.6. Incremental Cycling Test
2.7. Cardiorespiratory Measurements
2.8. Biochemical Analysis
2.9. Statistical Analysis
3. Results
4. Discussion
4.1. Acute Respiratory Responses
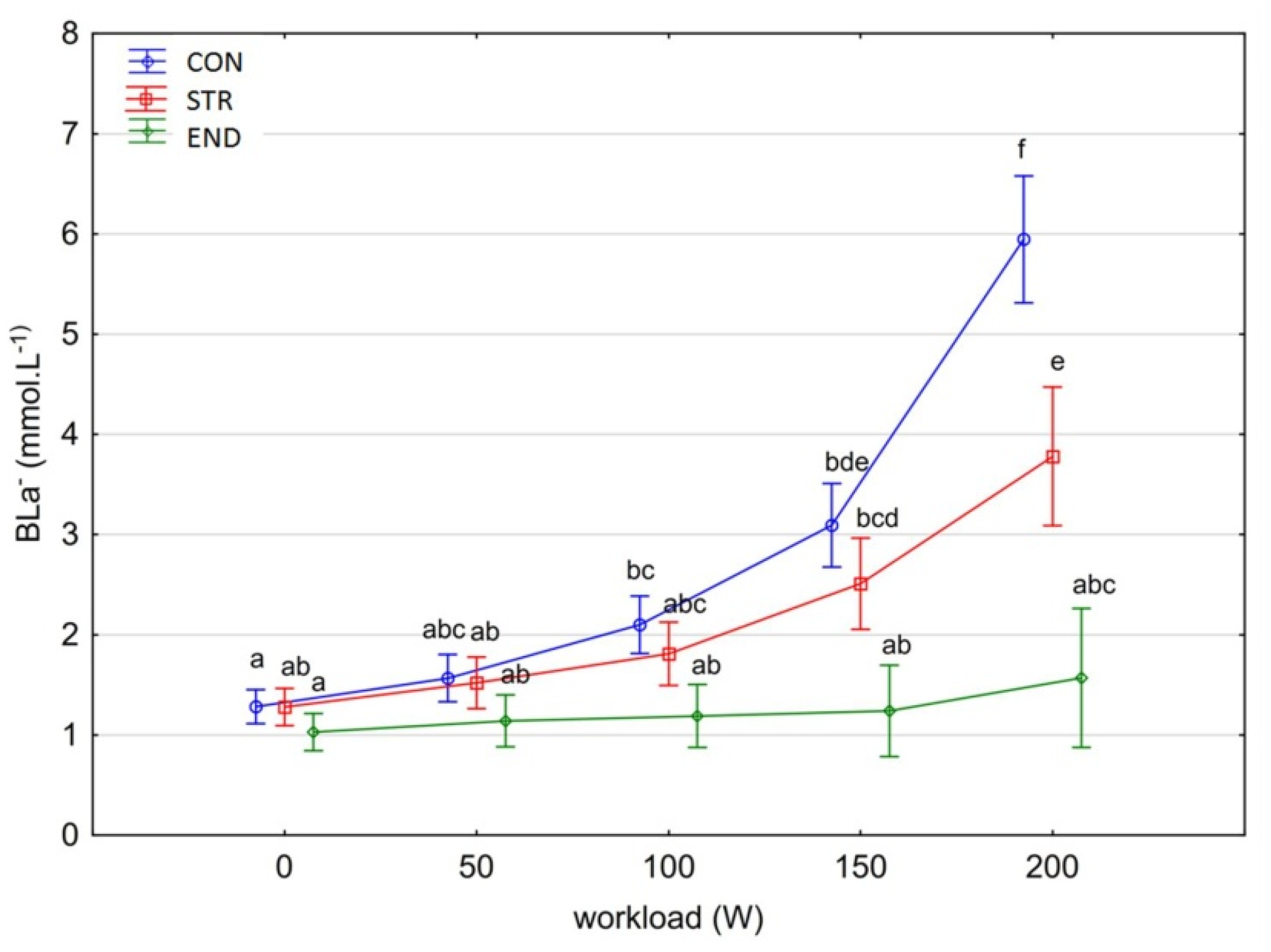
4.2. Acute Metabolic Responses (RER and BLa–)
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bohm, P.; Schneider, G.; Linneweber, L.; Rentzsch, A.; Krämer, N.; Abdul-Khaliq, H.; Kindermann, W.; Meyer, T.; Scharhag, J. Right and left ventricular function and mass in male elite master athletes: A controlled contrast-enhanced cardiovascular magnetic resonance study. Circulation 2016, 133, 1927–1935. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.A.; Oh, D.J. The effects of long-term aerobic exercise on cardiac structure, stroke volume of the left ventricle, and cardiac output. J. Exerc. Rehabil. 2016, 12, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Trachsel, L.D.; Ryffel, C.P.; De Marchi, S.; Seiler, C.; Brugger, N.; Eser, P.; Wilhelm, M. Exercise-induced cardiac remodeling in non-elite endurance athletes: Comparison of 2-tiered and 4-tiered classification of left ventricular hypertrophy. PLoS ONE 2018, 13, e0193203. [Google Scholar] [CrossRef]
- Aubry, A.; Hausswirth, C.; Louis, J.; Coutts, A.J.; Buchheit, M.; Le Meur, Y. The development of functional overreaching is associated with a faster heart rate recovery in endurance athletes. PLoS ONE 2015, 10, e0139754. [Google Scholar] [CrossRef] [Green Version]
- Horn, P.; Ostadal, P.; Ostadal, B. Rowing increases stroke volume and cardiac output to a greater extent than cycling. Physiol. Res. 2015, 64, 203–207. [Google Scholar] [CrossRef]
- Bolger, R.; Lyons, M.; Harrison, A.J.; Kenny, I.C. Sprinting performance and resistance-based training interventions: A systematic review. J. Strength Cond. Res. 2015, 29, 1146–1156. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Contreras, B.; Krieger, J.; Grgic, J.; Delcastillo, K.; Belliard, R.; Alto, A. Resistance training volume enhances muscle hypertrophy but not strength in trained men. Med. Sci. Sports Exerc. 2019, 51, 94–103. [Google Scholar] [CrossRef]
- Roberts, M.D.; Haun, C.T.; Mobley, C.B.; Mumford, P.W.; Romero, M.A.; Roberson, P.A.; Vann, C.G.; McCarthy, J.J. Physiological differences between low versus high skeletal muscle hypertrophic responders to resistance exercise training: Current perspectives and future research directions. Front. Physiol. 2018, 9, 834. [Google Scholar] [CrossRef]
- Gotshalk, L.A.; Berger, R.A.; Kraemer, W.J. Cardiovascular responses to a high-volume continuous circuit resistance training protocol. J. Strength Cond. Res. 2004, 18, 760–764. [Google Scholar]
- Santoro, A.; Alvino, F.; Antonelli, G.; Caputo, M.; Padeletti, M.; Lisi, M.; Mondillo, S. Endurance and Strength Athlete’s Heart: Analysis of Myocardial Deformation by Speckle Tracking Echocardiography. J. Cardiovasc. Ultrasound 2014, 22, 196–204. [Google Scholar] [CrossRef] [Green Version]
- Otsuki, T.; Maeda, S.; Iemitsu, M.; Saito, Y.; Tanimura, Y.; Sugawara, J.; Ajisaka, R.; Miyauchi, T. Postexercise heart rate recovery accelerates in strength-trained athletes. Med. Sci. Sports Exerc. 2007, 39, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Barbier, J.; Ville, N.; Kervio, G.; Walther, G.; Carré, F. Sports-specific features of athlete’s heart and their relation to echocardiographic parameters. Herz 2006, 31, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Bloomer, R.J. Energy cost of moderate-duration resistance and aerobic exercise. J. Strength Cond. Res. 2005, 19, 878–882. [Google Scholar] [PubMed]
- Jung, A.P. The impact of resistance training on distance running performance. Sports Med. 2003, 33, 539–552. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, P.; Andersen, J.L. Effects of strength training on endurance capacity in top-level endurance athletes. Scand. J. Med. Sci. 2010, 20, 39–47. [Google Scholar] [CrossRef]
- Carter, H.; Jones, A.M.; Barstow, T.J.; Burnley, M.; Williams, C.; Doust, J.H. Effect of endurance training on oxygen uptake kinetics during treadmill running. J. Appl. Physiol. 2000, 89, 1744–1752. [Google Scholar] [CrossRef]
- Schroeder, E.C.; Franke, W.D.; Sharp, R.L.; Lee, D.C. Comparative effectiveness of aerobic, resistance, and combined training on cardiovascular disease risk factors: A randomized controlled trial. PLoS ONE 2019, 14, e0210292. [Google Scholar] [CrossRef] [Green Version]
- García-Pallarés, J.; Sánchez-Medina, L.; Carrasco, L.; Díaz, A.; Izquierdo, M. Endurance and neuromuscular changes in world-class level kayakers during a periodized training cycle. Eur.J. Appl. Physiol. 2009, 106, 629–638. [Google Scholar] [CrossRef]
- Steele, J.; Fisher, J.; Bruce-Low, S. Resistance training to momentary muscular failure improves cardiovascular fitness in humans: A review of acute physiological responses and chronic physiological adaptations. J. Exerc. Physiol. Online 2012, 15, 53–80. [Google Scholar]
- Dufour, S.P.; Lampert, E.; Doutreleau, S.T.; Lonsdorfer-Wolf, E.; Billat, V.L.; Piquard, F.R.; Richard, R.U. Eccentric cycle exercise: Training application of specific circulatory adjustments. Med. Sci. Sports Exerc. 2004, 36, 1900–1906. [Google Scholar] [CrossRef]
- Prieur, F.; Benoit, H.; Busso, T.; Castells, J.; Geyssant, A.; Denis, C. Effects of moderate hyperoxia on oxygen consumption during submaximal and maximal exercise. Eur. J. Appl. Physiol. 2002, 88, 235–242. [Google Scholar] [PubMed]
- Gutmann, I.; Wahlefeld, A.W. L-(−)-malate. Determination with malate dehydrogenase and NAD. In Methods of Enzymatic Analysis; Bergmeyer, H.U., Ed.; Academic Press: London, UK, 1974; pp. 1585–1589. [Google Scholar]
- TIBCO Software Inc. Statistica (Data Analysis Software System), Version 13. 2017. Available online: http://statistica.io.
- IBM. IBM Manuals. IBM® SPSS® Statistics Algorithms; IBM Corporation: Armonk, NY, USA, 2020. [Google Scholar]
- Sokal, R.R.; Rohlf, E.J. Biometry, 3rd ed.; W. H. Freeman and Company: San Francisco, CA, USA, 1995. [Google Scholar]
- Mauchly, J.W. Significance test for sphericity of a normal n-variate distribution. Ann. Math. Statist. 1940, 11, 204–209. [Google Scholar] [CrossRef]
- Shingala, M.C.; Rajyaguru, A. Comparison of Post Hoc Tests for Unequal Variance. Int. J. New Technol. Sci. Eng. 2015, 2, 22–33. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using MultivariateStatistics, 7th ed.; Pearson Allyn & Bacon: Upper Saddle River, NJ, USA, 2019. [Google Scholar]
- Koutlianos, N.; Dimitros, E.; Metaxas, T.; Cansiz, M.; Deligiannis, A.; Kouidi, E. Indirect estimation of VO2max in athletes by ACSM’s equation: Valid or not? Hippokratia 2013, 17, 136–140. [Google Scholar] [PubMed]
- Iellamo, F.; Lucini, D.; Volterrani, M.; Casasco, M.; Salvati, A.; Gianfelici, A.; Gianfrancesco, A.D.; Urso, A.; Manzi, V. Autonomic nervous system responses to strength training in top-level weightlifters. Physiol. Rep. 2019, 7, e14233. [Google Scholar] [CrossRef]
- O’Toole, M.L.; Douglas, P.S.; Hiller, W.D. Lactate, oxygen uptake, and cycling performance in triathletes. Int. J. Sports Med. 1989, 10, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.; Claxton, D.; Fysh, M. A comparison of two time-domain analysis procedures in the determination of VO2 kinetics by pseudorandom binary sequence exercise testing. Eur. J. Appl. Physiol. 2003, 88, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Hackett, D.A.; Johnson, N.; Chow, C. Respiratory muscle adaptations: A comparison between bodybuilders and endurance athletes. J. Sports Med. Phys. Fit. 2013, 53, 139–145. [Google Scholar]
- Caputo, F.; Denadai, B.S. Exercise mode affects the time to achieve VO2max without influencing maximal exercise time at the intensity associated with VO2max in triathletes. Int. J. Sports Med. 2006, 27, 798–803. [Google Scholar] [CrossRef]
- do Nascimento Salvador, P.C.; Dal Pupo, J.; De Lucas, R.D.; de Aguiar, R.A.; Arins, F.B.; Guglielmo, L.G. The VO2 kinetics of maximal and supramaximal running exercises in sprinters and middle-distance runners. J. Strength Cond. Res. 2016, 30, 2857–2863. [Google Scholar] [CrossRef]
- Aagaard, P.; Magnusson, P.S.; Larsson, B.; Kjaer, M.; Krustrup, P. Mechanical muscle function, morphology, and fiber type in lifelong trained elderly. Med. Sci. Sports Exerc. 2007, 39, 1989–1996. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, P.; Andersen, J.L.; Bennekou, M.; Larsson, B.; Olesen, J.L.; Crameri, R.; Magnusson, S.P.; Kjaer, M. Effects of resistance training on endurance capacity and muscle fiber composition in young top-level cyclists. Scand. J. Med. Sci. Sports 2011, 21, e298–e307. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.L.; Frandsen, U.; Jensen, K.Y.; Prokhorova, T.A.; Dalgaard, L.B.; Bech, R.D.; Nygaard, T.; Suetta, C.; Aagaard, P. Skeletal Muscle Microvascular Changes in Response to Short-Term Blood Flow Restricted Training-Exercise-Induced Adaptations and Signs of Perivascular Stress. Front. Physiol. 2020, 11, 556. [Google Scholar] [CrossRef] [PubMed]
- Richard, N.A.; Hodges, L.; Koehle, M.S. Elevated peak systolic blood pressure in endurance-trained athletes: Physiology or pathology? Scand. J. Med. Sci. Sports 2021, 31, 956–966. [Google Scholar] [CrossRef]
- Mihl, C.; Dassen, W.R.M.; Kuipers, H. Cardiac remodeling: Concentric versus eccentric hypertrophy in strength and endurance athletes. Neth. Heart J. 2008, 16, 129–133. [Google Scholar] [CrossRef] [Green Version]
- MacDougall, J.D.; Tuxen, D.; Sale, D.G.; Moroz, J.R. Arterial blood pressure response to heavy resistance exercise. J. Appl. Physiol. 1985, 58, 785–790. [Google Scholar] [CrossRef] [Green Version]
- Caselli, S.; Serdoz, A.; Mango, F.; Lemme, E.; VaquerSeguì, A.; Milan, A.; AttenhoferJost, C.; Schmied, C.; Spataro, A.; Pelliccia, A. High blood pressure response to exercise predicts future development of hypertension in young athletes. Eur. Heart J. 2019, 40, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Schultz, M.G.; Otahal, P.; Cleland, V.J.; Blizzard, L.; Marwick, T.H.; Sharman, J.E. Exercise-induced hypertension, cardiovascular events, and mortality in patients undergoing exercise stress testing: A systematic review and meta-analysis. Am. J. Hypertens. 2013, 26, 357–366. [Google Scholar] [CrossRef] [Green Version]
- Caselli, S.; Segui, A.V.; Quattrini, F.; Di Gacinto, B.; Milan, A.; Assorgi, R.; Verdile, L.; Spataro, A.; Pelliccia, A. Upper normal values of blood pressure response to exercise in Olympic athletes. Am. Heart J. 2016, 177, 120–128. [Google Scholar] [CrossRef]
- Colliander, E.B.; Tesch, P.A. Blood pressure in resistance-trained athletes. Can. J. Sport Sci. 1988, 13, 31–34. [Google Scholar]
- Ramos-Jiménez, A.; Hernández-Torres, R.P.; Torres-Durán, P.V.; Romero-Gonzalez, J.; Mascher, D.; Posadas-Romero, C.; Juárez-Oropeza, M.A. The respiratory exchange ratio is associated with fitness indicators both in trained and untrained men: A possible application for people with reduced exercise tolerance. Clin. Med. Circ. Respir. Pulm. Med. 2008, 2, CCRPM-S449. [Google Scholar] [CrossRef] [PubMed]
- Gavin, J.P.; Myers, S.; Willems, M.E.T. The accumulative effect of concentric-biased and eccentric-biased exercise on cardiorespiratory and metabolic responses to subsequent low-intensity exercise: A preliminary study. J. Hum. Kinet 2015, 49, 131–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goedecke, J.H.; Gibson, A.S.C.; Grobler, L.; Collins, M.; Noakes, T.D.; Lambert, E.V. Determinants of the variability in respiratory exchange ratio at rest and during exercise in trained athletes. Am. J. Physiol. Endocrinol. Metab. 2000, 279, E1325–E1334. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.J.; Marbut, M.M.; Round, J.M. Muscle fibre type and aetiology of obesity. Lancet 1990, 335, 805–808. [Google Scholar] [CrossRef]
- Lucía, A.; Hoyos, J.; Pardo, J.; Chicharro, J.L. Metabolic and neuromuscular adaptations to endurance training in professional cyclists: A longitudinal study. Jpn. J. Physiol. 2000, 50, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Jeukendrup, A.E.; Mensink, M.; Saris, W.H.M.; Wagenmakers, A.J.M. Exogenous glucose oxidation during exercise in endurance-trained and untrained subjects. J. Appl. Physiol. 1997, 82, 835–840. [Google Scholar] [CrossRef] [Green Version]
- Bergman, B.C.; Wolfel, E.E.; Butterfield, G.E.; Lopaschuk, G.D.; Casazza, G.A.; Horning, M.A.; Brooks, G.A. Active muscle and whole-body lactate kinetics after endurance training in men. J. Appl. Physiol. 1999, 87, 1684–1696. [Google Scholar] [CrossRef] [Green Version]
- Gollnick, P.; Bayly, W.; Hodgson, D. Exercise intensity, training, diet and lactate concentration in muscle and blood. Med. Sci. Sports Exerc. 1986, 18, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Messonnier, L.A.; Emhoff, C.A.W.; Fattor, J.A.; Horning, M.A.; Carlson, T.J.; Brooks, G.A. Lactate kinetics at the lactate threshold in trained and untrained men. J. Appl. Physiol. 2013, 114, 1593–1602. [Google Scholar] [CrossRef]
- Regan, W.F.; Potteiger, J.A. Isokinetic exercise velocities and blood lactate concentrations in strength/power and endurance athletes. J. Strength Cond. Res. 1999, 13, 157–161. [Google Scholar]
- San-Millán, I.; Brooks, G.A. Assessment of metabolic flexibility by means of measuring blood lactate, fat, and carbohydrate oxidation responses to exercise in professional endurance athletes and less-fit individuals. Sports Med. 2018, 48, 467–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Variable | Mean ± SD | 95% CI | Median | Min | Max |
|---|---|---|---|---|---|---|
| END (n = 10) | Age (years) | 20.3 ± 0.62 | 18.9–21.7 | 19 | 19 | 24 |
| BH (cm) | 179.8 ± 2.08 | 175.1–184.5 | 181 | 165 | 190 | |
| BM (kg) | 75.06 ± 2.935 | 66.42–81.70 | 80.5 | 59.2 | 83.5 | |
| BMI (kg/m2) | 23.16 ± 0.644 | 21.70–24.62 | 23.3 | 18.9 | 25.9 | |
| STR (n = 10) | Age (years) | 22.4 ± 0.43 | 21.4–23.4 | 22 | 20 | 24 |
| BH (cm) | 181.9 ± 2.40 | 176.5–187.3 | 179 | 173 | 192 | |
| BM (kg) | 83.93 ± 2.704 | 77.81–90.05 | 82.6 | 75.0 | 103.7 | |
| BMI (kg/m2) | 25.37 ± 0.639 | 23.92–26.81 | 25.0 | 22.8 | 28.4 | |
| CON (n = 12) | Age (years) | 23.2 ± 0.41 | 22.3–24.2 | 24 | 21 | 25 |
| BH (cm) | 181.6 ± 1.82 | 177.6–185.6 | 184 | 173 | 189 | |
| BM (kg) | 78.23 ± 2.579 | 72.56–83.91 | 78.6 | 65.0 | 91.0 | |
| BMI (kg/m2) | 23.70 ± 0.635 | 22.30–25.10 | 23.6 | 20.6 | 28.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurasz, M.; Boraczyński, M.; Laskin, J.J.; Kamelska-Sadowska, A.M.; Podstawski, R.; Jaszczur-Nowicki, J.; Nowakowski, J.J.; Gronek, P. Acute Cardiorespiratory and Metabolic Responses to Incremental Cycling Exercise in Endurance- and Strength-Trained Athletes. Biology 2022, 11, 643. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11050643
Jurasz M, Boraczyński M, Laskin JJ, Kamelska-Sadowska AM, Podstawski R, Jaszczur-Nowicki J, Nowakowski JJ, Gronek P. Acute Cardiorespiratory and Metabolic Responses to Incremental Cycling Exercise in Endurance- and Strength-Trained Athletes. Biology. 2022; 11(5):643. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11050643
Chicago/Turabian StyleJurasz, Maciej, Michał Boraczyński, James J. Laskin, Anna M. Kamelska-Sadowska, Robert Podstawski, Jarosław Jaszczur-Nowicki, Jacek J. Nowakowski, and Piotr Gronek. 2022. "Acute Cardiorespiratory and Metabolic Responses to Incremental Cycling Exercise in Endurance- and Strength-Trained Athletes" Biology 11, no. 5: 643. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11050643