
Influence of an Upper Limb Isometric Task in Perceived and Performance Fatigability of Elderly Subjects: A Quasi-Experimental Study

 , ,
, ,  ,
,  , , ,
, , ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Sample
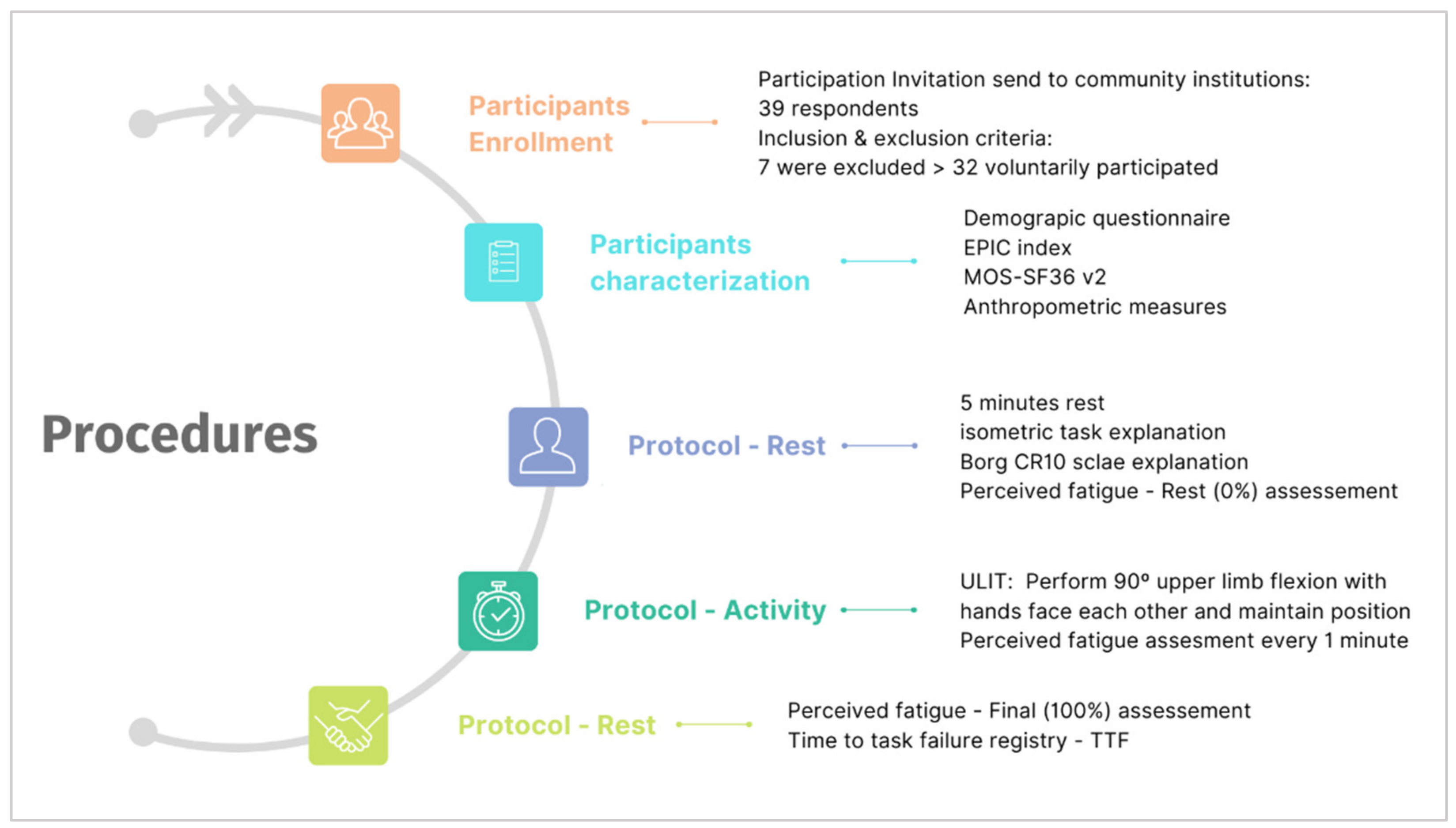
2.2. Procedure
2.3. Outcome Measures
2.4. Ethical Considerations
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
3.1. Sample Demographic, Anthropometric, Physical Activity, and Clinical Characteristics
3.2. Perceived Fatigability and Performance Variables Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vestergaard, S.; Nayfield, S.G.; Patel, K.V.; Eldadah, B.; Cesari, M.; Ferrucci, L.; Ceresini, G.; Guralnik, J.M. Fatigue in a Representative Population of Older Persons and Its Association with Functional Impairment, Functional Limitation, and Disability. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2009, 64, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lasorda, K.R.; Gmelin, T.; Kuipers, A.L.; Boudreau, R.M.; Santanasto, A.J.; Christensen, K.; Renner, S.W.; Wojczynski, M.K.; Andersen, S.L.; Cosentino, S.; et al. Epidemiology of Perceived Physical Fatigability in Older Adults: The Long Life Family Study. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2020, 75, e81–e88. [Google Scholar] [CrossRef] [PubMed]
- Santos-Eggimann, B.; Cuénoud, P.; Spagnoli, J.; Junod, J. Prevalence of Frailty in Middle-Aged and Older Community-Dwelling Europeans Living in 10 Countries. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2009, 64, 675–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manfredi, G.; Midão, L.; Paúl, C.; Cena, C.; Duarte, M.; Costa, E. Prevalence of Frailty Status among the European Elderly Population: Findings from the Survey of Health, Aging and Retirement in Europe. Geriatr. Gerontol. Int. 2019, 19, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.M.; Desai, M.M.; Gahbauer, E.A.; Holford, T.R.; Williams, C.S. Restricted Activity among Community-Living Older Persons: Incidence, Precipitants, and Health Care Utilization. Ann. Intern. Med. 2001, 135, 313–321. [Google Scholar] [CrossRef]
- Schrack, J.A.; Simonsick, E.M.; Glynn, N.W. Fatigability: A Prognostic Indicator of Phenotypic Aging. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2020, 75, e63–e66. [Google Scholar] [CrossRef]
- Kluger, B.M.; Krupp, L.B.; Enoka, R.M. Fatigue and Fatigability in Neurologic Inllnesses. Neurology 2013, 80, 409–416. [Google Scholar] [CrossRef]
- Marcora, S.M.; Staiano, W. The Limit to Exercise Tolerance in Humans: Mind over Muscle? Eur. J. Appl. Physiol. 2010, 109, 763–770. [Google Scholar] [CrossRef]
- Drouin, P.J.; Kohoko, Z.I.N.N.; Mew, O.K.; Lynn, M.J.T.T.; Fenuta, A.M.; Tschakovsky, M.E. Fatigue-Independent Alterations in Muscle Activation and Effort Perception during Forearm Exercise: Role of Local Oxygen Delivery. J. Appl. Physiol. 2019, 127, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.L.; Amann, M.; Duchateau, J.; Meeusen, R.; Rice, C.L. Neural Contributions to Muscle Fatigue: From the Brain to the Muscle and Back Again. Med. Sci. Sports Exerc. 2016, 48, 2294–2306. [Google Scholar] [CrossRef] [Green Version]
- Wan, J.-J.J.; Qin, Z.; Wang, P.-Y.Y.; Sun, Y.; Liu, X. Muscle Fatigue: General Understanding and Treatment. Exp. Mol. Med. 2017, 49, e384-11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheel, A.W.; Boushel, R.; Dempsey, J.A. Competition for Blood Flow Distribution between Respiratory and Locomotor Muscles: Implications for Muscle Fatigue. J. Appl. Physiol. 2018, 125, 820–831. [Google Scholar] [CrossRef] [PubMed]
- Velloso, M.; do Nascimento, N.H.; Gazzotti, M.R.; Jardim, J.R. Evaluation of Effects of Shoulder Girdle Training on Strength and Performance of Activities of Daily Living in Patients with Chronic Obstructive Pulmonary Disease. Int. J. COPD 2013, 8, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Panka, G.F.L.; Oliveira, M.M.; França, D.C.; Parreira, V.F.; Britto, R.R.; Velloso, M. Ventilatory and Muscular Assessment in Healthy Subjects during an Activity of Daily Living with Unsupported Arm Elevation. Rev. Bras. Fisioter. 2010, 14, 337–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical Activity in Older Age: Perspectives for Healthy Ageing and Frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Avlund, K.; Trab Damsgaard, M.; Scient Soc, M.; Schroll, M. Tiredness as Determinant of Subsequent Use of Health and Social Services Among Nondisabled Elderly People. J. Aging Health 2001, 13, 267–286. [Google Scholar] [CrossRef]
- Glynn, N.W.; Gmelin, T.; Renner, S.W.; Qiao, Y.; Boudreau, R.M.; Feitosa, M.F.; Wojczynski, M.K.; Cosentino, S.; Andersen, S.L.; Christensen, K.; et al. Perceived Physical Fatigability Predicts All-Cause Mortality in Older Adults. J. Gerontol. Ser. A 2022, 77, 837–841. [Google Scholar] [CrossRef]
- Moored, K.D.; Qiao, Y.S.; Boudreau, R.M.; Roe, L.S.; Cawthon, P.M.; Cauley, J.A.; Glynn, N.W. Prospective Associations Between Physical Activity and Perceived Fatigability in Older Men: Differences by Activity Type and Baseline Marital Status. J. Gerontol. Ser. A 2022, glac030. [Google Scholar] [CrossRef]
- Engberg, I.; Segerstedt, J.; Waller, G.; Wennberg, P.; Eliasson, M. Fatigue in the General Population- Associations to Age, Sex, Socioeconomic Status, Physical Activity, Sitting Time and Self-Rated Health: The Northern Sweden MONICA Study 2014. BMC Public Health 2017, 17, 654. [Google Scholar] [CrossRef] [Green Version]
- Avlund, K. Fatigue in Older Adults: An Early Indicator of the Aging Process? Aging Clin. Exp. Res. 2010, 22, 100–115. [Google Scholar] [CrossRef] [Green Version]
- Enoka, R.M.; Duchateau, J. Translating Fatigue to Human Performance. Med. Sci. Sports Exerc. 2016, 48, 2228–2238. [Google Scholar] [CrossRef] [Green Version]
- Simonsick, E.M.; Schrack, J.A.; Glynn, N.W.; Ferrucci, L. Assessing fatigability in mobility-intact older adults. J. Am. Geriatr. Soc. 2014, 62, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Gruet, M. Fatigue in Chronic Respiratory Diseases: Theoretical Framework and Implications for Real-Life Performance and Rehabilitation. Front. Physiol. 2018, 9, 1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loy, B.D.; Taylor, R.L.; Fling, B.W.; Horak, F.B. Relationship between Perceived Fatigue and Performance Fatigability in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. J. Psychosom. Res. 2017, 100, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.K. Performance Fatigability: Mechanisms and Task Specificity. Cold Spring Harb. Perspect. Med. 2018, 8, a029728. [Google Scholar] [CrossRef] [Green Version]
- Salerno, E.A.; Wanigatunga, A.A.; An, Y.; Urbanek, J.K.; Simonsick, E.M.; Ferrucci, L.; Resnick, S.M.; Schrack, J.A.; Newman, A. Longitudinal Association between Perceived Fatigability and Cognitive Function in Older Adults: Results from the Baltimore Longitudinal Study of Aging. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2020, 75, e67–e73. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 5 May 2022).
- World Health Organization (WHO). UN Decade of Healthy Ageing (2021–2030). Available online: https://www.who.int/initiatives/decade-of-healthy-ageing (accessed on 21 April 2022).
- Murofushi, K.; Yamaguchi, D.; Hirohata, K.; Furuya, H.; Mitomo, S. Variations in Upper Limb and Trunk Muscles Activation during Isometric Exercises with or without Exertion of Control. Isokinet. Exerc. Sci. 2022, 30, 251–258. [Google Scholar] [CrossRef]
- De Oliveira Sarmento, A.; da Cruz Santos, A.; Trombetta, I.C.; Dantas, M.M.; Marques, A.C.O.; do Nascimento, L.S.; Barbosa, B.T.; Dos Santos, M.R.; do Amparo Andrade, M.; Jaguaribe-Lima, A.M.; et al. Regular Physical Exercise Improves Cardiac Autonomic and Muscle Vasodilatory Responses to Isometric Exercise in Healthy Elderly. Clin. Interv. Aging 2017, 12, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Lemley, K.J.; Drewek, B.; Hunter, S.K.; Hoeger Bement, M.K. Pain Relief after Isometric Exercise Is Not Task-Dependent in Older Men and Women. Med. Sci. Sports Exerc. 2014, 46, 185–191. [Google Scholar] [CrossRef]
- Enoka, R.M.; Baudry, S.; Rudroff, T.; Farina, D.; Klass, M.; Duchateau, J. Unraveling the Neurophysiology of Muscle Fatigue. J. Electromyogr. Kinesiol. 2011, 21, 208–219. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998; pp. 1–120. [Google Scholar]
- Ferreira, P.L.; Noronha Ferreira, L.; Nobre Pereira, L. Medidas Sumário Física e Mental de Estado de Saúde Para a População Portuguesa. Rev. Port. Saude Publica 2012, 30, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Lopes Ferreira, P. Creation of the Portuguese Version of MOS SF-36 Part II—Validation Tests. Acta Med. Port. 2000, 13, 119–127. [Google Scholar] [CrossRef]
- Ferreira, P.L. Creation of Portuguese Version of the MOS SF-36 Part I, Cultural and Linguistic Adaptation. Acta Med. Port. 2000, 13, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, P.L.; Santana, P. Percepção de Estado de Saúde e de Qualidade de Vida Da População Activa: Contributo Para a Definição de Normas Portuguesas. Rev. Port. Saúde Pública 2003, 21, 15–30. [Google Scholar]
- Camões, M.; Severo, M.; Santos, A.C.; Barros, H.; Lopes, C. Testing an Adaptation of the EPIC Physical Activity Questionnaire in Portuguese Adults: A Validation Study That Assesses the Seasonal Bias of Self-Report. Ann. Hum. Biol. 2010, 37, 186–198. [Google Scholar] [CrossRef]
- Review, C.; Communication, S.; Principles, G. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Ansdell, P.; Brownstein, C.G.; Škarabot, J.; Hicks, K.M.; Howatson, G.; Thomas, K.; Hunter, S.K.; Goodall, S. Sex Differences in Fatigability and Recovery Relative to the Intensity–Duration Relationship. J. Physiol. 2019, 597, 5577–5595. [Google Scholar] [CrossRef]
- Kratz, A.L.; Murphy, S.L.; Braley, T.J.; Basu, N.; Kulkarni, S.; Russell, J.; Carlozzi, N.E. Development of a Person-Centered Conceptual Model of Perceived Fatigability. Qual. Life Res. 2019, 28, 1337–1347. [Google Scholar] [CrossRef]
- Bonett, D.G.; Wright, T.A. Sample Size Requirements for Estimating Pearson, Kendall and Spearman Correlations. Psychometrika 2000, 65, 23–28. [Google Scholar] [CrossRef]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenhouse-Tucknott, A.; Butterworth, J.B.; Wrightson, J.G.; Harrison, N.A.; Dekerle, J. Effect of the Subjective Intensity of Fatigue and Interoception on Perceptual Regulation and Performance during Sustained Physical Activity. PLoS ONE 2022, 17, e262303. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.K. The Relevance of Sex Differences in Performance Fatigability. Med. Sci. Sports Exerc. 2016, 48, 2247–2256. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Amezcua, P.; Simonsick, E.M.; Wanigatunga, A.A.; Urbanek, J.K.; Chiles Shaffer, N.; Ferrucci, L.; Schrack, J.A. Association between Adiposity and Perceived Physical Fatigability in Mid- to Late Life. Obesity 2019, 27, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.K.; Cavuoto, L.A. Relationship between BMI and Fatigability Is Task Dependent. Hum. Factors 2017, 59, 722–733. [Google Scholar] [CrossRef]
- Cooper, R.; Popham, M.; Santanasto, A.J.; Hardy, R.; Glynn, N.W.; Kuh, D. Are BMI and Inflammatory Markers Independently Associated with Physical Fatigability in Old Age? Int. J. Obes. 2019, 43, 832–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malak, M.Z.; Abu Adas, M.; Al-Amer, R.; Yousef, N.N.; Ali, R.M. Evaluation of Fatigue among Older Population in Jordan. Exp. Aging Res. 2021, 47, 464–477. [Google Scholar] [CrossRef] [PubMed]
- Salter, A.; Fox, R.J.; Tyry, T.; Cutter, G.; Marrie, R.A. The Association of Fatigue and Social Participation in Multiple Sclerosis as Assessed Using Two Different Instruments. Mult. Scler. Relat. Disord. 2019, 31, 165–172. [Google Scholar] [CrossRef]
- Schrack, J.A.; Wanigatunga, A.A.; Zipunnikov, V.; Kuo, P.L.; Simonsick, E.M.; Ferrucci, L.; Newman, A. Longitudinal Association between Energy Regulation and Fatigability in Mid-to-Late Life. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2020, 75, e74–e80. [Google Scholar] [CrossRef]
- Eldadah, B.A. Fatigue and Fatigability in Older Adults. PM&R 2010, 2, 406–413. [Google Scholar] [CrossRef]
- Qiao, Y.S.; Gmelin, T.; Renner, S.W.; Boudreau, R.M.; Martin, S.; Wojczynski, M.K.; Christensen, K.; Andersen, S.L.; Cosentino, S.; Santanasto, A.J.; et al. Evaluation of the Bidirectional Relations of Perceived Physical Fatigability and Physical Activity on Slower Gait Speed. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2021, 76, E237–E244. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sample Characteristics | Total Sample Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p-Values | Effect Size Cohen’s d |
|---|---|---|---|---|---|
| Age (years) | 72.50 ± 5.18 (65–85) | 70.00 ± 1.00 (65–85) | 73.00 ± 1.00 (65–82) | 0.641 † | 3.000 |
| Weight (kg) | 73.34 ± 12.83 (48–100) | 68.25 ± 12.25 (48–86.5) | 78.44 ± 11.61 (57.90–100) | 0.022 † | 0.854 |
| Height (m) | 1.59 ± 0.08 (1.48–1.76) | 1.54 ± 0.50 (1.48–1.65) | 1.65 ± 0.06 (1.57–1.76) | <0.001 † | 0,199 |
| BMI (kg/m2) | 28.72 ± 4.58 (21.56–37.94) | 28.7 ± 1.28 (21.56–37.94) | 28.74 ± 1.04 (23.42–35.61) | 0.982 † | 0.034 |
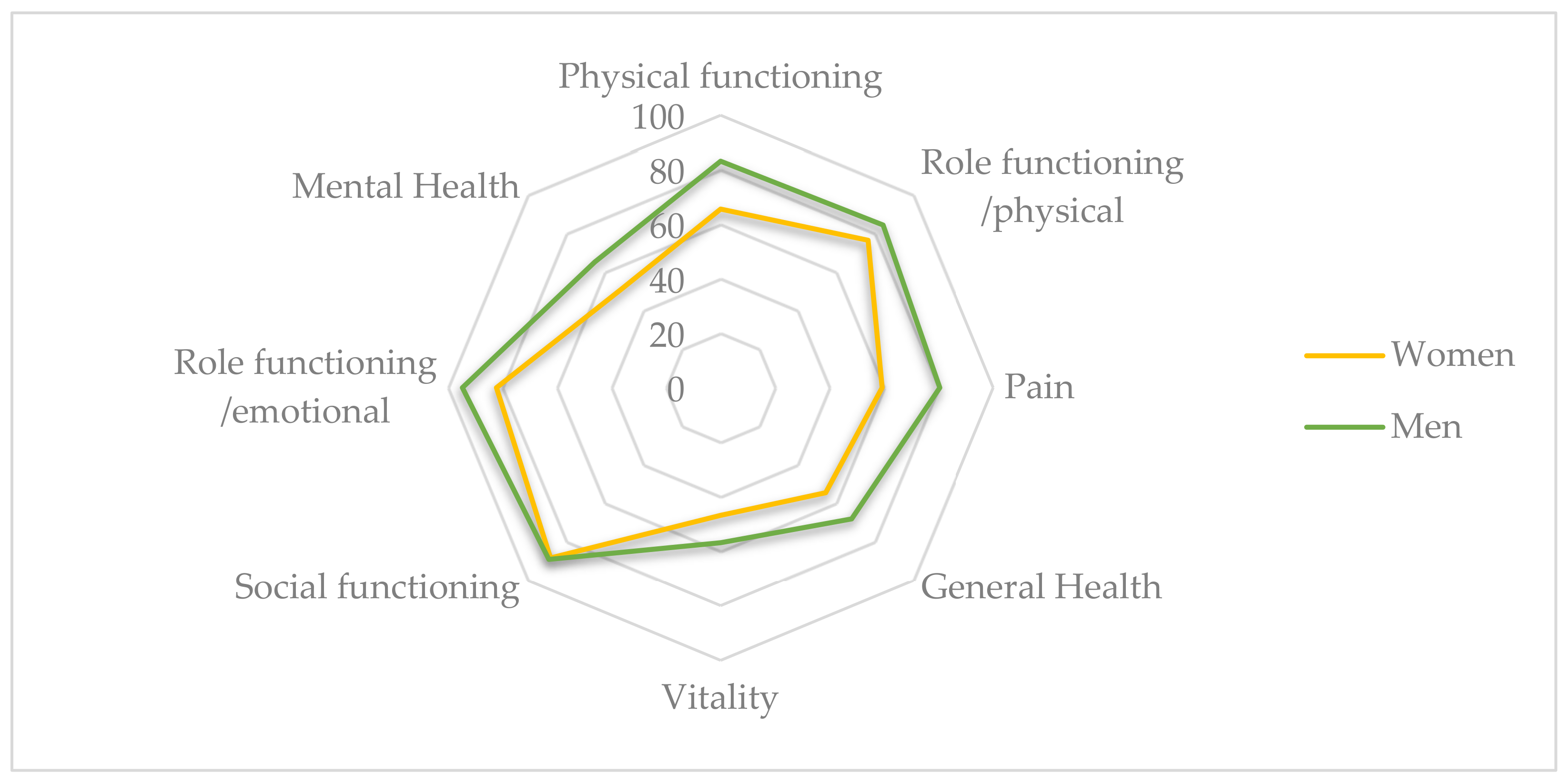
| Health-Related Quality of Life Dimensions | Total Sample Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p-Value | Effect Size Cohen’s d |
|---|---|---|---|---|---|
| SF36 Physical functioning | 74.38 ± 19.62 (30–100) | 66.00 ± 5.00 (30–100) | 83.00 ± 4.00 (40–100) | <0.001 † | 3.75 |
| SF36 Role functioning/physical | 80.47 ± 23.64 (31–100) | 77.00 ± 6.00 (31–100) | 84.00 ± 6.00 (31–100) | 0.254 ‡ | 0.216 |
| SF36 Pain | 69.81 ± 25.32 (22–100) | 59.00 ± 6.00 (22–100) | 80.00 ± 6.00 (41–100) | 0.023 ‡ | 0.40 |
| SF36 General health | 61.28 ± 19.82 (30–100) | 55.00 ± 5.00 (30–92) | 68.00 ± 5.00 (45–100) | 0.051 † | 2.60 |
| SF36 Vitality | 51.88 ± 15.75 (25–80) | 47.00 ± 4.00 (25–80) | 57.00 ± 4.00 (35–80) | 0.072 † | 2.50 |
| SF36 Social functioning | 88.67 ± 15.99 (38–100) | 88.00 ± 4.00 (38–100) | 89.00 ± 4.00 (50–100) | 0.867 ‡ | 0.036 |
| SF3 Role functioning/emotional | 88.54 ± 18.54 (42–100) | 82.00 ± 6.00 (42–100) | 95.00 ± 2.00 (67–100) | 0.270 ‡ | 0.215 |
| SF36 Mental health | 58.25 ± 17.97 (16–80) | 51.00 ± 4.00 (16–80) | 65.00 ± 4.00 (32–80) | 0.039 ‡ | 0.37 |
| Physical Activity | Total Sample Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p-Value | Effect Size Cohen’s d |
|---|---|---|---|---|---|
| Physical activity total time | 646.53 ± 701.66 (0–2520) | 668.00 ± 173.00 (0–2520) | 625.00 ± 183.00 (0–2520) | 0.669 ‡ | 0.078 |
| Moderate physical activity time | 479.44 ± 586.18 (0–2520) | 696.00 ± 180.00 (0–2520) | 263.00 ± 75.00 (0–840) | 0.035 ‡ | 0.380 |
| Vigorous physical activity time | 234.03 ± 491.08 (0–2100) | 107.00 ± 72.00 (0–840) | 361.00 ± 155.00 (0–2100) | 0.323 ‡ | 0.227 |
| Fatigability Variables | Total Sample Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p-Value | Effect Size Cohen’s d | Repeated Measures | |||
|---|---|---|---|---|---|---|---|---|---|
| p-Value | Effect Size Cohen’s d | p-Value | Effect Size Cohen’s d | ||||||
| PcFat 0% | 0.47 ± 0.88 | 0.38 ± 0.89 | 0.56 ± 0.89 | 0.445 ‡ | 0.177 | <0.001 Ξ | 0.76 | ||
| (0.00–3.00) | (0.00–3.00) | (0.00–3.00) | |||||||
| PcFat 25% | 2.00 ± 1.48 | 1.69 ± 1.11 | 2.31 ± 1.75 | 0.237 † | 0.423 | <0.001 § | 0.93 | ||
| (0.00–6.00) | (0.00–3.00) | (0.00–6.00) | |||||||
| PcFat 50% | 3.67 ± 2.00 | 3.03 ± 1.45 | 4.31 ± 2.29 | 0.069 † | 0.668 | <0.001 Ξ | 0.88 | ||
| (0.00–8.00) | (0.00–5.00) | (0.00–8.00) | |||||||
| PcFat 75% | 6.11 ± 2.18 | 5.5 ± 1.81 | 6.72 ± 2.41 | 0.094 ‡ | 0.299 | <0.001 Ξ | 0.87 | ||
| (2.00–9.00) | (2.00–8.00) | (2.00–9.00) | |||||||
| PcFat 100% | 8.25 ± 2.29 | 7.75 ± 2.46 | 8.75 ± 2.05 | 0.210 ‡ | 0.243 | ||||
| (3.00–10.00) | (3.00–10.00) | (4.00–10.00) | |||||||
| VPcFat 0–25% | 1.53 ± 1.41 | 1.31 ± 0.98 | 1.75 ± 1.74 | 0.752 ‡ | 0.061 | 0.674 | 0.075 | ||
| (0.00–5.00) | (0.00–3.00) | (0.00–5.00) | |||||||
| VPcFat 25–50% | 1.67 ± 1.18 | 1.34 ± 0.87 | 2.00 ± 1.38 | 0.118 † | 0.572 | 0.0054 | 0.5 | ||
| (0.00–4.00) | (0.00–3.50) | (0.00–4.00) | |||||||
| VPcFat 50–75% | 2.44 ± 1.16 | 2.47 ± 1.22 | 2.41 ± 1.13 | 0.876 ‡ | 0.034 | 0.154 | 0.713 | ||
| (0.50–4.50) | 0.50–4.00) | (1.00–4.50) | |||||||
| VPcFat 75–100% | 2.14 ± 1.34 | 2.25 ± 1.34 | 2.03 ± 1.37 | 0.669 ‡ | 0.079 | ||||
| (0.00–6.00) | (0.50–5.50) | (0.00–6.00) | |||||||
| VPcFat 0–50% | 3.20 ± 2.12 | 2.66 ± 1.41 | 3.75 ± 2.59 | 0.151 † | 0.521 | 0.0113 | 0.66 | ||
| (0.00–8.00) | (0.00–5.00) | (0.00–8.00) | |||||||
| VPcFat 50–100% | 4.58 ± 1.97 | 4.72 ± 2.23 | 4.44 ± 1.74 | 0.694 † | 0.140 | ||||
| (1.00–9.50) | (1.00–9.50) | (1.00–7.00) | |||||||
| VPcFat 25–75% | 4.11 ± 1.86 | 3.81 ± 1.64 | 4.41 ± 2.07 | 0.375 † | 0.321 | ||||
| (1.00–8.00) | (1.50–6.50) | (1.00–8.00) | |||||||
| TTF (sec) | 472.25 ± 296.79 | 371.63 ± 221.18 | 572.88 ± 333.94 | 0.043 ‡ | 0.360 | ||||
| (128–1443) | (128–1012) | (286–1443) | |||||||
| Time to Task Failure (TTF) | |||
|---|---|---|---|
| Total Sample | Women | Men | |
| Perceived fatigability (PcFat) | PcFat 75% | PcFat 75% | PcFat 25% |
| (ρ = 0.544 **, 95% CI [0.22, 0.76] | (ρ = 0.615 *, 95% CI [0.12, 0.86]) | (ρ = 0.568 *, 95% CI [0.06, 0.84]) | |
| PcFat 100% | PcFat 100% | PcFat 75% | |
| (ρ = 0.645 **, 95% CI [0.35, 0.82]) | (ρ = 0.848 **, 95% CI [0.55, 0.95]) | (ρ = 0.522 *, 95% CI [0.00, 0.82]) | |
| Perceived Fatigability (PcFat) | |||
|---|---|---|---|
| Total Sample | Women | Men | |
| Sample characteristics | Age-PcFat 25% | ||
| (r = 0.660 **, 95% CI [0.24, 0.87]) | Vigorous-PcFat 100% | ||
| Vigorous - PcFat 75% | Age-PcFat 50% | (ρ = 0.560 *, 95% CI [0.05, 0.84]) | |
| (ρ = 0.363 *, 95% CI [0.00, 0.64]) | (r = 0.524 *, 95% CI [0.038, 0.81]) | ||
| BMI - PcFat 100% | SF36 Pain - PcFat 50% | ||
| (ρ = −0.507 *, 95% CI [−0.81, 0.02]) | (ρ = −0.543 *, 95% CI [−0.83, −0.03]) | ||
| SF36 Social functioning - PcFat 75% | SF36 Pain - PcFat 75% | ||
| (ρ = −0.411 *, 95% CI [0.06, 0.67]) | SF36 Vitality - PcFat 25% | (ρ = −0.556 *, 95% CI [−0.84, −0.04])) | |
| (r = −0.559 *, 95% CI [−0.83, −0.09]) | SF36 Vitality - PcFat 50% | ||
| (r = −0.533 *, 95% CI [−0.81, −0.05]) | |||
| Time to Task Failure (TTF) | |||
|---|---|---|---|
| Total Sample | Women | Men | |
| Sample characteristics | BMI (ρ = −0.471 **, 95% CI [−0.71, −0.13]) SF36 Physical functioning (ρ = 0.471 **, 95% CI [0.13, 0.71]) SF36 Role functioning/physical (ρ = 0.381 *, 95% CI [0.02, 0.65]) | BMI (ρ = −0.629 **, 95% CI −0.87, −0.14]) SF36 Physical functioning (ρ = 0.506 *, 95% CI [−0.02, 0.81]) | No significative correlation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Migueis, H.; Martínez-Jiménez, E.M.; Casado-Hernández, I.; Dias, A.; Monteiro, A.J.; Martins, R.B.; Romero-Morales, C.; López-López, D.; Gómez-Salgado, J. Influence of an Upper Limb Isometric Task in Perceived and Performance Fatigability of Elderly Subjects: A Quasi-Experimental Study. Biology 2022, 11, 1175. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11081175
Silva-Migueis H, Martínez-Jiménez EM, Casado-Hernández I, Dias A, Monteiro AJ, Martins RB, Romero-Morales C, López-López D, Gómez-Salgado J. Influence of an Upper Limb Isometric Task in Perceived and Performance Fatigability of Elderly Subjects: A Quasi-Experimental Study. Biology. 2022; 11(8):1175. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11081175
Chicago/Turabian StyleSilva-Migueis, Helena, Eva María Martínez-Jiménez, Israel Casado-Hernández, Adriano Dias, Ana Júlia Monteiro, Rodrigo B. Martins, Carlos Romero-Morales, Daniel López-López, and Juan Gómez-Salgado. 2022. "Influence of an Upper Limb Isometric Task in Perceived and Performance Fatigability of Elderly Subjects: A Quasi-Experimental Study" Biology 11, no. 8: 1175. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11081175