
Primary Melanoma of the Cervix Uteri: A Systematic Review and Meta-Analysis of the Reported Cases

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
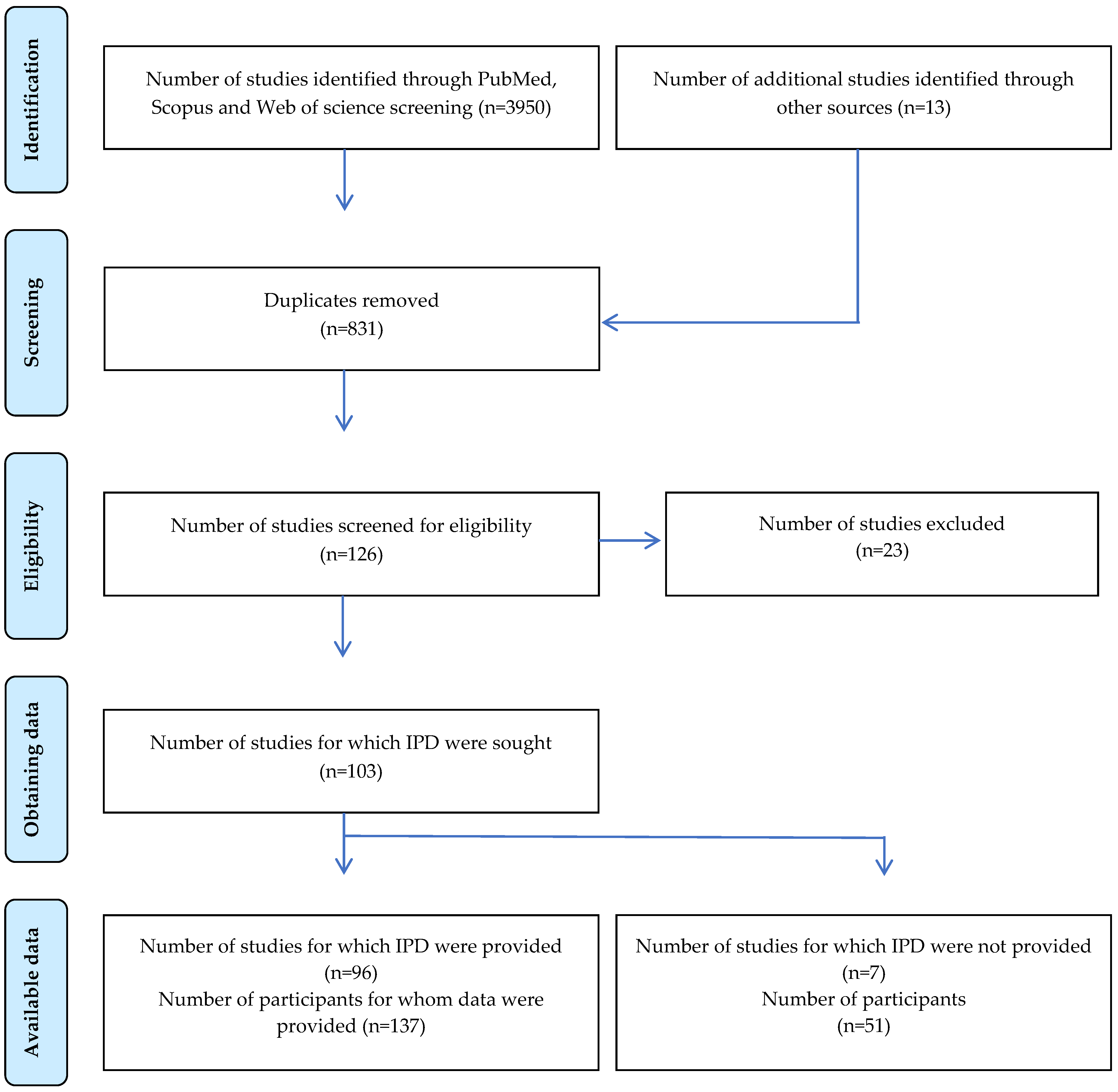
2. Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Extraction and Handling
2.4. Quality Assessment
2.5. Data Synthesis
3. Results
3.1. Study Characteristics
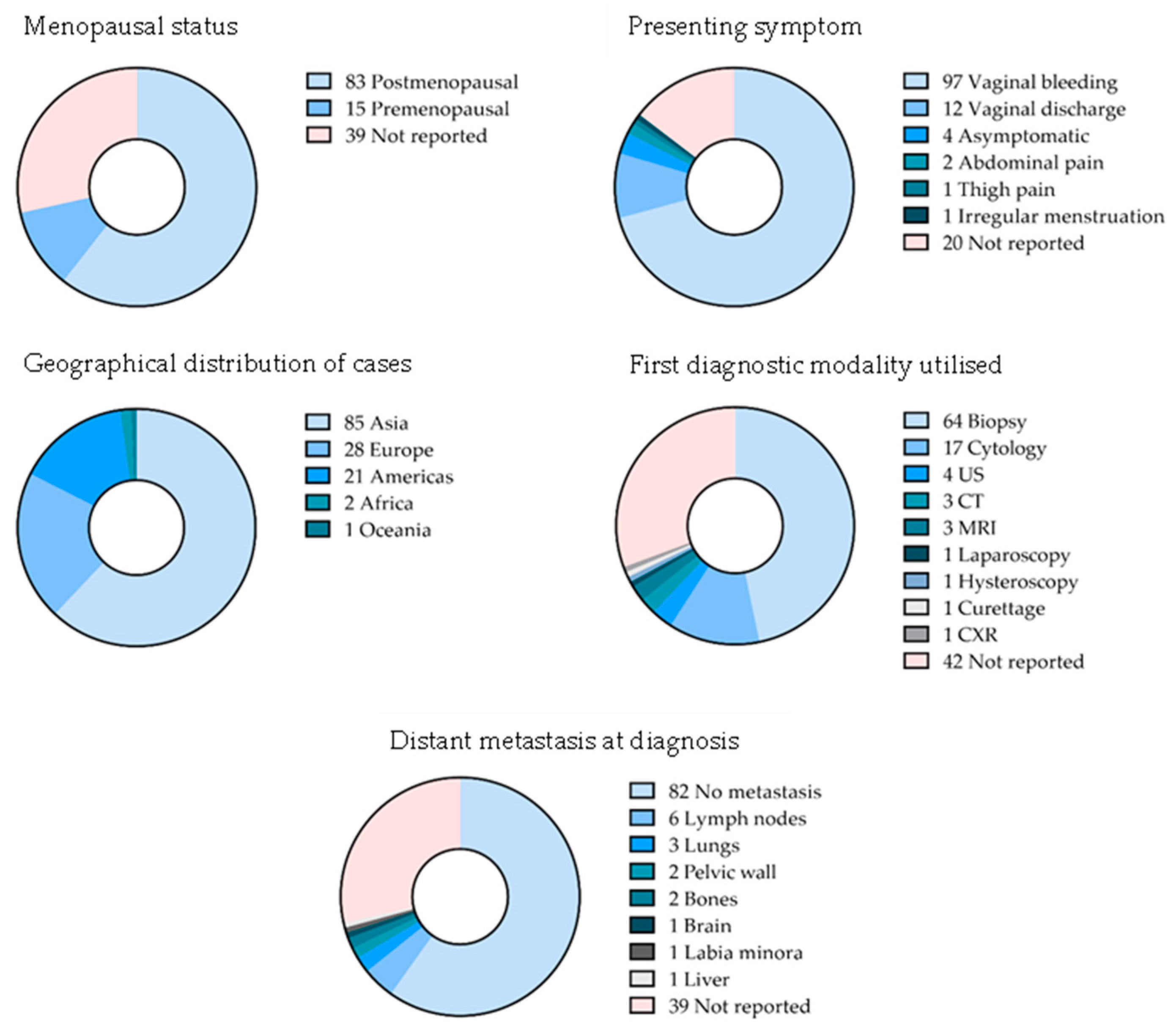
3.2. Patient Characteristics
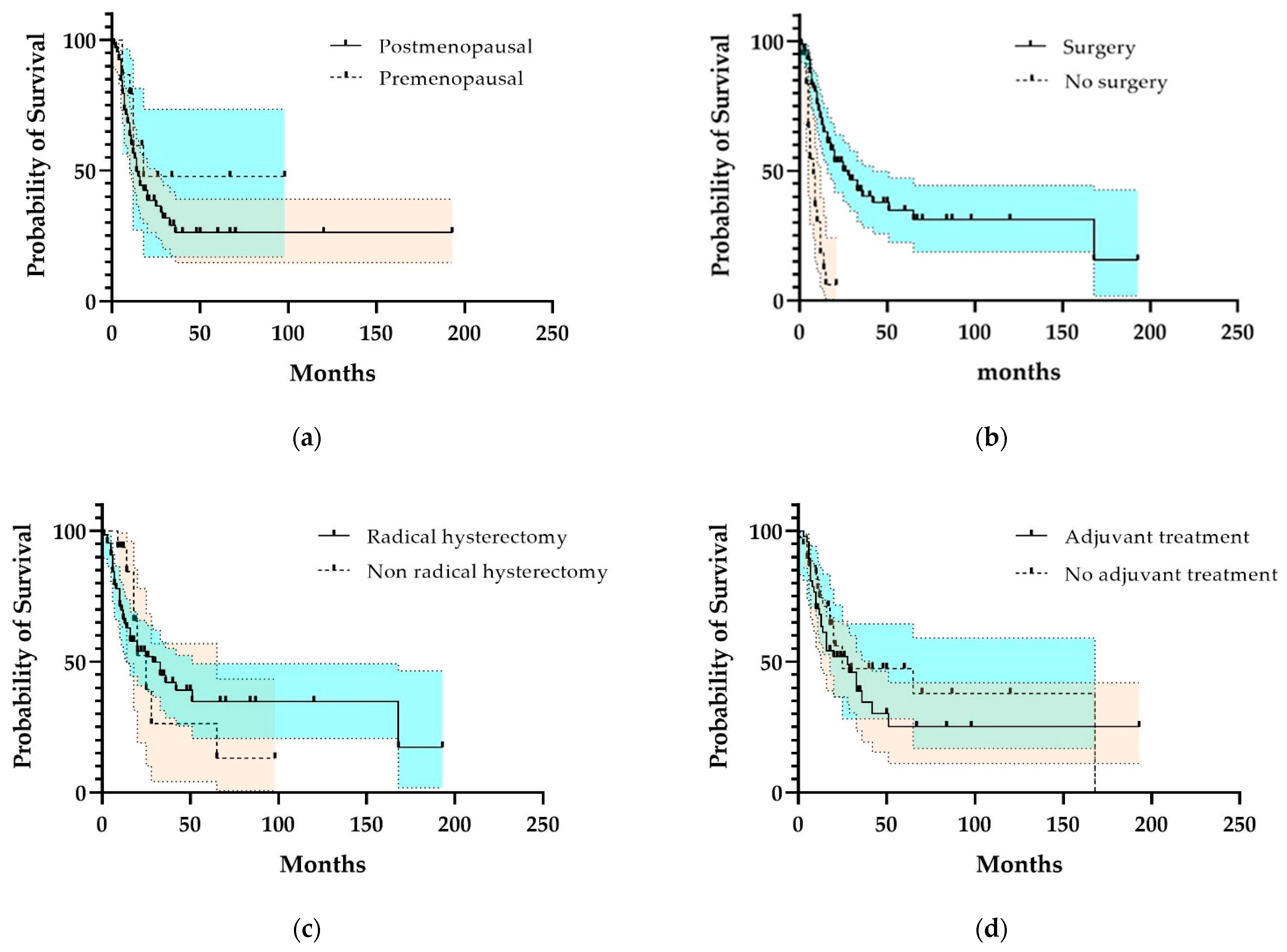
3.3. Outcome and Survival Rates
3.4. Quality of the Studies
4. Discussion
4.1. Results in the Context of the Literature
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mihajlovic, M.; Vlajkovic, S.; Jovanovic, P.; Stefanovic, V. Primary mucosal melanomas: A comprehensive review. Int. J. Clin. Exp. Pathol. 2012, 5, 739–753. [Google Scholar] [PubMed]
- Patrick, R.J.; Fenske, N.A.; Messina, J.L. Primary mucosal melanoma. J. Am. Acad. Derm. 2007, 56, 828–834. [Google Scholar] [CrossRef]
- Schadendorf, D.; Fisher, D.E.; Garbe, C.; Gershenwald, J.E.; Grob, J.J.; Halpern, A.; Herlyn, M.; Marchetti, M.A.; McArthur, G.; Ribas, A.; et al. Melanoma. Nat. Rev. Dis. Prim. 2015, 1, 15003. [Google Scholar] [CrossRef] [PubMed]
- Das, P.; Kumar, N.; Ahuja, A.; Jain, A.; Ray, R.; Sarkar, C.; Gupta, S.D. Primary malignant melanoma at unusual sites: An institutional experience with review of literature. Melanoma Res. 2010, 20, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Tranoulis, A.; Laios, A.; Munot, S.; Theophilou, G.; Pathak, D.; Nugent, D. Multidisciplinary Approach in the Management of Primary Malignant Melanoma of the Uterine Cervix: Diagnostic and Management Challenges. J. Gynecol. Surg. 2018, 34, 209–213. [Google Scholar] [CrossRef]
- Udager, A.M.; Frisch, N.K.; Hong, L.J.; Stasenko, M.; Johnston, C.M.; Liu, J.R.; Chan, M.P.; Harms, P.W.; Fullen, D.R.; Orsini, A.; et al. Gynecologic melanomas: A clinicopathologic and molecular analysis. Gynecol. Oncol. 2017, 147, 351–357. [Google Scholar] [CrossRef]
- Min, K.J.; Kim, Y.S.; Hong, J.H.; Lee, J.K.; Yang, D.S. Primary malignant melanoma of uterine cervix: A suggestion of new scheme of treatment combination. Chin. J. Cancer Res. 2014, 26, 351–354. [Google Scholar] [CrossRef]
- Piura, B. Management of primary melanoma of the female urogenital tract. Lancet Oncol. 2008, 9, 973–981. [Google Scholar] [CrossRef]
- Min, A.; Fu, A.; Huang, M.; Wang, H.; Chen, H. Primary Malignant Melanoma of the Cervix: An Integrated Analysis of Case Reports and Series. Front. Oncol. 2022, 12, 913964. [Google Scholar] [CrossRef]
- Indini, A.; Di Guardo, L.; Cimminiello, C.; Lorusso, D.; Raspagliesi, F.; Del Vecchio, M. Investigating the role of immunotherapy in advanced/recurrent female genital tract melanoma: A preliminary experience. J. Gynecol. Oncol. 2019, 30, e94. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sone, K.; Kukita, A.; Masui, Y.; Yamada, D.; Shinozaki-Ushiku, A.; Kawata, A.; Taguchi, A.; Miyamoto, Y.; Tanikawa, M.; Iriyama, T.; et al. Recurrent malignant melanoma of the uterine cervix treated with anti-PD-1 antibodies and anti-CTLA-4 antibodies: A case report. Mol. Clin. Oncol. 2022, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.K.M.; Li, J.J.X.; Lee, J.H.S. Smear detected cervicovaginal melanoma following negative screening-a cautionary tale of rapidly developing malignancy of the lower female genital tract. Cytopathology 2021, 32, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Endo, H.; Sasaki, T.; Nakamura, T.; Yamanaka, H.; Hosonuma, S.; Kuji, S.; Deura, I.; Ohara, T.; Kondo, H.; et al. Primary malignant melanoma of uterine cervix treated with pembrolizumab as adjuvant immunotherapy. Int. Cancer Conf. J. 2021, 10, 254–258. [Google Scholar] [CrossRef]
- Cai, Y.J.; Ke, L.F.; Zhang, W.W.; Lu, J.P.; Chen, Y.P. Recurrent KRAS, KIT and SF3B1 mutations in melanoma of the female genital tract. BMC Cancer 2021, 21, 677. [Google Scholar] [CrossRef]
- Diakosavvas, M.; Fasoulakis, Z.N.; Kouroupi, M.; Theodora, M.; Inagamova, L.; Tsatsaris, G.; Nikolaou, P.; Frangia-Tsivou, K.; Giatromanolaki, A.; Kontomanolis, E.N. Primary Malignant Melanoma of the Cervix: A Case Report and a Review of the Literature. Case Rep. Oncol. Med. 2020, 2020, 7206786. [Google Scholar] [CrossRef]
- Pumpure, E.; Drucka, E.; Kigitovica, D.; Meskauskas, R.; Isajevs, S.; Nemiro, I.; Rasa, A.; Olmane, E.; Zablocka, T.; Alberts, P.; et al. Management of a primary malignant melanoma of uterine cervix stage IVA patient with radical surgery and adjuvant oncolytic virus Rigvir((R)) therapy: A case report. Clin. Case Rep. 2020, 8, 1538–1543. [Google Scholar] [CrossRef]
- Anko, M.; Nakamura, M.; Kobayashi, Y.; Tsuji, K.; Nakada, S.; Nakamura, Y.; Funakoshi, T.; Banno, K.; Aoki, D. Primary malignant melanoma of the uterine cervix or vagina which were successfully treated with nivolumab. J. Obs. Gynaecol. Res. 2020, 46, 190–195. [Google Scholar] [CrossRef]
- Shakeel, O.; Ullah, F.; Khalid, N.; Ali, S.I.; Batool, S.; Amjad, A.; Anwer, A.W.; Ali, H.; Zafar, H.; Syed, A.A. Malignant Melanoma of the Female Genital Tract: Experience of an Oncology Center in Pakistan. Cureus 2020, 12, e8484. [Google Scholar] [CrossRef]
- Pang, Y.; Yuan, H.; Ren, A.; Zhang, S.; Liu, P. Primary malignant melanoma of the female genital tract synchronously involving the vulva and uterine cervix: A case report. Medicine 2019, 98, e16366. [Google Scholar] [CrossRef]
- Yin, C.; Yang, A.; Zhang, Y.; Tao, L.; Zou, H.; Ren, Y.; Liang, W.; Jiang, J.; Zhao, J.; Zhang, W.; et al. Primary Cervical Malignant Melanoma: 2 Cases and a Literature Review. Int. J. Gynecol. Pathol. 2019, 38, 196–203. [Google Scholar] [CrossRef]
- Eniu, D.T.; Staicu, A.; Somcutian, O.; Buiga, R.; Albu, C.; Goidescu, I.G.; Chiorean, A.R.; Nistor-Ciurba, C.C. Blue nevus-like melanoma of the uterine cervix. Case report and review of the literature. Rom. J. Morphol. Embryol. 2019, 60, 1317–1321. [Google Scholar] [PubMed]
- Srivastava, P.; Rath, S.; Hadi, R.; Husain, N. Primary amelanotic malignant melanoma of cervix masquerading as squamous cell carcinoma presenting with extensive metastases. BMJ Case Rep. 2018, 2018, 224723. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Chen, Y.; Chen, Y.; Liu, D.; Yan, Z.; Bin, M.; Zhao, G.; Pan, Z.; Li, Q. Primary malignant melanoma of the cervix: 14 cases and literature overview. Melanoma Res. 2018, 28, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Choi, C.H.; Kim, T.J.; Lee, J.W.; Lee, J.; Bae, D.S.; Kim, B.G. Primary malignant melanoma of the uterine cervix treated with pembrolizumab after radical surgery: A case report and literature review. Obs. Gynecol. Sci. 2018, 61, 524–528. [Google Scholar] [CrossRef]
- Nai, G.A.; Bazan, A.; Rocha, C.A.; Nagy, J.S.; Campos, I.T. Postpartum Genital Melanoma—A Case Report. Rev. Bras. Ginecol. Obs. 2018, 40, 163–167. [Google Scholar] [CrossRef] [Green Version]
- Yuan, G.; Wu, L.; Li, B.; An, J. Primary malignant melanoma of the cervix: Report of 14 cases and review of literature. Oncotarget 2017, 8, 73162–73167. [Google Scholar] [CrossRef]
- Juliao, I.; Carvalho, S.D.; Patricio, V.; Raimundo, A. Primary malignant melanoma of the cervix: A rare disease. BMJ Case Rep. 2017, 2017, 219361. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, T.; Ota, N.; Mabuchi, Y.; Yagi, S.; Minami, S.; Okuhira, H.; Yamamoto, Y.; Nakamura, Y.; Ino, K. A Case of Malignant Melanoma of the Uterine Cervix with Disseminated Metastases throughout the Vaginal Wall. Case Rep. Obs. Gynecol. 2017, 2017, 5656340. [Google Scholar] [CrossRef]
- Lim, K.H.; Tay, S.K.; Ng, A.X.; Mantoo, S. Primary Melanoma of the Uterine Cervix: A Case Report, With Key Points on Recognition and Pathological Diagnosis. J. Low Genit. Tract. Dis. 2017, 21, e1–e4. [Google Scholar] [CrossRef]
- Gupta, M. Malignant melanoma of cervix. BMJ Case Rep. 2016, 2016, 217970. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Yun, J.; Seo, J.W.; Bae, G.E.; Lee, J.W.; Kim, S.W. Primary malignant melanoma of cervix and vagina. Obs. Gynecol. Sci. 2016, 59, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Arik, D.; Oge, T.; Kabukcuoglu, S.; Yalcin, O.T.; Ozalp, S. Amelanotic malignant melanoma of the uterine cervix diagnosed by cervical smear. Diagn. Cytopathol. 2016, 44, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, D.; Lamblin, G.; Mathevet, P.; Hetu, J.; Berakdar, I.; Beurrier, F.; Chopin, N. Genital melanoma: Prognosis factors and treatment modality. Arch Gynecol. Obs. 2016, 294, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Schiavone, M.B.; Broach, V.; Shoushtari, A.N.; Carvajal, R.D.; Alektiar, K.; Kollmeier, M.A.; Abu-Rustum, N.R.; Leitao, M.M., Jr. Combined immunotherapy and radiation for treatment of mucosal melanomas of the lower genital tract. Gynecol. Oncol. Rep. 2016, 16, 42–46. [Google Scholar] [CrossRef] [Green Version]
- Berger, J.L.; Samrao, D.; Huang, M.; Olawaiye, A.B. Primary gynecologic melanoma: A report of two unusual cases. Gynecol. Oncol. Rep. 2015, 11, 31–33. [Google Scholar] [CrossRef] [Green Version]
- Geredeli, C.; Boruban, M.C.; Poyraz, N.; Artac, M.; Aribas, A.; Koral, L. Biatrial Cardiac Metastases in a Patient with Uterine Cervix Malignant Melanoma. Case Rep. Cardiol. 2015, 2015, 958756. [Google Scholar] [CrossRef] [Green Version]
- Cetinkaya, K.; Benzer, E.; Dervisoglu, H. Primary mucosal malignant melanoma of the cervix: Case report and review of the literature. Tumori 2015, 101, e147–e150. [Google Scholar] [CrossRef]
- Mihmanli, V.; Toprakci, G.; Cetinkaya, N.; Kilickaya, A.; Kamali, G. Primary malignant melanoma of the cervix: A case report. Eur. J. Gynaecol. Oncol. 2015, 36, 607–609. [Google Scholar]
- Bhargava, S.; Mogra, N.; Goyal, N. Primary malignant melanoma of uterine cervix. J. Obs. Gynaecol. India 2014, 64, 132–133. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Wang, H.; Zhang, X.; Xu, Q. Primary malignant melanoma of the cervix: A case report. Oncol. Lett. 2014, 8, 2661–2663. [Google Scholar] [CrossRef] [PubMed]
- Omranipour, R.; Mahmoodzadeh, H.; Jalaeefar, A.; Abdirad, A.; Parsaei, R.; Ebrahimi, R. Primary malignant melanoma of uterine cervix. J. Obs. Gynaecol. 2014, 34, 111. [Google Scholar] [CrossRef] [PubMed]
- Shenjere, P.; Fisher, C.; Rajab, R.; Patnaik, L.; Hazell, S.; Thway, K. Melanoma with rhabdomyosarcomatous differentiation: Two further cases of a rare pathologic pitfall. Int. J. Surg. Pathol. 2014, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.; Barmon, D.; Deka, P.; Ch Kataki, A.; Choudhary, B.K. Sarcomatoid carcinoma of the cervix with foci of malignant melanoma. J. Midlife Health 2014, 5, 41–44. [Google Scholar] [CrossRef]
- Myriokefalitaki, E.; Babbel, B.; Smith, M.; Ahmed, A.S. Primary malignant melanoma of uterine cervix FIGO IIa1: A case report with 40 months ongoing survival and literature review. Gynecol. Oncol. Case Rep. 2013, 5, 52–54. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Tripathi, R.; Mala, Y.M. Primary malignant melanoma of uterine cervix with probable origin from benign cervical melanosis. BMJ Case Rep. 2013, 2013, bcr2013010042. [Google Scholar] [CrossRef] [Green Version]
- Bennani, A.; el Fatemi, H.; Erraghay, S.; Mobakir, H.; Ameurtess, H.; Souuaf, I.; Moumna, K.; Idrissi, K.; Zriouel, A.; Squalli, N.; et al. The primary melanoma of the female genital tract: Report of three cases and review of literature. Pan. Afr. Med. J. 2013, 16, 58. [Google Scholar] [CrossRef]
- Parada, D.; Pena, K.B.; Riu, F. Coexisting malignant melanoma and blue nevus of the uterine cervix: An unusual combination. Case Rep. Pathol. 2012, 2012, 986542. [Google Scholar] [CrossRef]
- Tsai, Y.J.; Shueng, P.W.; Chan, S.C.; Chuang, W.Y.; Shiau, Y.C.; Hsu, C.H. Uterine cervical melanoma presenting with rapid progression detected by PET/CT. Acta Radiol. Short Rep. 2012, 1, 120026. [Google Scholar] [CrossRef]
- Calderon-Salazar, L.; Cantu de Leon, D.; Perez Montiel, D.; Almogabar-Villagran, E.; Villavicencio, V.; Cetina, L. Primary malignant melanoma of the uterine cervix treated with ultraradical surgery: A case report. ISRN Obs. Gynecol. 2011, 2011, 683020. [Google Scholar] [CrossRef]
- Zhang, J.; Cao, Y.; Xiao, L.; Tang, J.; Tang, L. A peculiar site: Melanoma of the cervix. Am. J. Obs. Gynecol. 2011, 205, 508.e1–508.e3. [Google Scholar] [CrossRef] [PubMed]
- Simoes, M.; Cunha, V.; Nabais, H.; Riscado, I.; Jorge, A.F. Primary malignant melanoma of the uterine cervix--case report and review. Eur. J. Gynaecol. Oncol. 2011, 32, 448–451. [Google Scholar] [PubMed]
- Setia, N.; Goulart, R.A.; Leiman, G.; Otis, C.N.; Modem, R.; Pantanowtiz, L. Cytomorphology of cervicovaginal melanoma: ThinPrep versus conventional Papanicolaou tests. Cytojournal 2010, 7, 25. [Google Scholar] [CrossRef]
- Duggal, R.; Srinivasan, R. Primary amelanotic melanoma of the cervix: Case report with review of literature. J. Gynecol. Oncol. 2010, 21, 199–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurana, A.; Jalpota, Y. Primary malignant melanoma of the uterine cervix. Indian J. Pathol. Microbiol. 2009, 52, 575–576. [Google Scholar] [CrossRef]
- An, J.; Li, B.; Wu, L.; Lu, H.; Li, N. Primary malignant amelanotic melanoma of the female genital tract: Report of two cases and review of literature. Melanoma Res. 2009, 19, 267–270. [Google Scholar] [CrossRef]
- Baruah, J.; Roy, K.K.; Kumar, S.; Kumar, L. A rare case of primary malignant melanoma of cervix. Arch Gynecol. Obs. 2009, 280, 453–456. [Google Scholar] [CrossRef]
- Yucesoy, G.; Kus, E.; Cakiroglu, Y.; Muezzinoglu, B.; Yildiz, K.; Yucesoy, I. Primary malignant melanoma of the cervix: Report of a case. Arch Gynecol. Obs. 2009, 279, 573–575. [Google Scholar] [CrossRef]
- Mandato, V.D.; Kobal, B.; Di Stefano, A.; Sinkovec, J.; Levicnik, A.; Rakar, S.; Costagliola, L. Amelanotic malignant melanoma of the uterine cervix with ten-year follow-up. Eur. J. Gynaecol. Oncol. 2009, 30, 106–109. [Google Scholar]
- Pusceddu, S.; Bajetta, E.; Buzzoni, R.; Carcangiu, M.L.; Platania, M.; Del Vecchio, M.; Ditto, A. Primary uterine cervix melanoma resembling malignant peripheral nerve sheath tumor: A case report. Int. J. Gynecol. Pathol. 2008, 27, 596–600. [Google Scholar] [CrossRef]
- Jin, B.; Goldsmith, A.; Budev, H.; Al-Abbadi, M. Primary melanoma of the uterine cervix after supracervical hysterectomy. A case report. Acta Cytol. 2007, 51, 86–88. [Google Scholar] [CrossRef]
- Mousavi, A.S.; Fakor, F.; Nazari, Z.; Ghaemmaghami, F.; Hashemi, F.A.; Jamali, M. Primary malignant melanoma of the uterine cervix: Case report and review of the literature. J. Low Genit. Tract. Dis. 2006, 10, 258–263. [Google Scholar] [CrossRef]
- Wydra, D.; Sawicki, S.; Ciach, K.; Emerich, J. Malignant melanoma of the uterine cervix. Eur. J. Obs. Gynecol. Reprod. Biol. 2006, 124, 257–258. [Google Scholar] [CrossRef]
- Ma, S.Q.; Bai, C.M.; Zhong, S.; Yu, X.H.; Lang, J.H. Clinical analysis of primary malignant melanoma of the cervix. Chin. Med. Sci. J. 2005, 20, 257–260. [Google Scholar]
- Gupta, R.; Singh, S.; Mandal, A.K. Primary malignant melanoma of cervix—A case report. Indian J. Cancer 2005, 42, 201–204. [Google Scholar]
- Siozos, C.; Bhat, A.; Lonsdale, R.; Nieto, J.J.; Crocker, S.G. Malignant melanoma of the uterine cervix. J. Obs. Gynaecol. 2005, 25, 826–827. [Google Scholar] [CrossRef]
- Kudrimoti, J.; Bindu, R.; Hayatnagarkar, N.; Bhople, K. Primary malignant melanoma of cervix: A case report. Indian J. Pathol. Microbiol. 2004, 47, 257–258. [Google Scholar]
- Makovitzky, J.; Schmitz, C.; Vogt-Weber, B.; Nizze, H. Primary malignant melanoma of the cervix uteri: A case report of a rare tumor. Anticancer Res. 2003, 23, 1063–1067. [Google Scholar]
- Boldt, C.; Lehmann, R.; Osmers, R.; Burrig, K.F. Primary malignant melanoma of the uterine cervix. Report of two cases and review of the literature. Pathologe 2003, 24, 226–235. [Google Scholar] [CrossRef]
- Gupta, S.; Sodhani, P.; Jain, S. Primary malignant melanoma of uterine cervix: A rare entity diagnosed on fine needle aspiration cytology--report of a case. Cytopathology 2003, 14, 153–156. [Google Scholar] [CrossRef]
- Deshpande, A.H.; Munshi, M.M. Primary malignant melanoma of the uterine cervix: Report of a case diagnosed by cervical scrape cytology and review of the literature. Diagn. Cytopathol. 2001, 25, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Zamiati, S.; Sahraoui, S.; Jabri, L.; Louahlia, S.; Sqalli, S.; Kahlain, A. Primary malignant melanoma of the cervix uteri: Apropos of 1 case with review of the literature. Gynecol. Obs. Fertil. 2001, 29, 381–385. [Google Scholar] [CrossRef]
- Furuya, M.; Shimizu, M.; Nishihara, H.; Ito, T.; Sakuragi, N.; Ishikura, H.; Yoshiki, T. Clear cell variant of malignant melanoma of the uterine cervix: A case report and review of the literature. Gynecol. Oncol. 2001, 80, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Benson, R.J.; Tan, L.T. Radiation-induced malignant melanoma of the cervix. Clin. Oncol. (R Coll Radiol.) 2000, 12, 234–237. [Google Scholar] [CrossRef] [PubMed]
- Wasef, W.R.; Roberts, J.K.; Dixon, G.R. Primary malignant melanoma of the cervix uteri. J. Obs. Gynaecol. 1999, 19, 673–674. [Google Scholar] [CrossRef]
- Clark, K.C.; Butz, W.R.; Hapke, M.R. Primary malignant melanoma of the uterine cervix: Case report with world literature review. Int. J. Gynecol. Pathol. 1999, 18, 265–273. [Google Scholar] [CrossRef]
- Cantuaria, G.; Angioli, R.; Nahmias, J.; Estape, R.; Penalver, M. Primary malignant melanoma of the uterine cervix: Case report and review of the literature. Gynecol. Oncol. 1999, 75, 170–174. [Google Scholar] [CrossRef]
- Takehara, M.; Ito, E.; Saito, T.; Nishioka, Y.; Kudo, R. Primary malignant melanoma of the uterine cervix: A case report. J. Obs. Gynaecol. Res. 1999, 25, 129–132. [Google Scholar] [CrossRef]
- Schlosshauer, P.W.; Heller, D.S.; Koulos, J.P. Malignant melanoma of the uterine cervix diagnosed on a cervical cytologic smear. Acta Cytol. 1998, 42, 1043–1045. [Google Scholar]
- Teixeira, J.C.; Salina, J.R.; Teixeira, L.C.; Andrade, L.A. Primary melanoma of the uterine cervix figo stage III B. Sao Paulo Med. J. 1998, 116, 1778–1780. [Google Scholar] [CrossRef] [Green Version]
- Ishikura, H.; Kojo, T.; Ichimura, H.; Yoshiki, T. Desmoplastic malignant melanoma of the uterine cervix: A rare primary malignancy in the uterus mimicking a sarcoma. Histopathology 1998, 33, 93–94. [Google Scholar] [CrossRef] [PubMed]
- Miyagi, Y.; Yamada, S.; Miyagi, Y.; Yamamoto, J.; Kawanishi, K.; Yoshinouchi, M.; Kodama, J.; Kamimura, S.; Takamoto, N.; Kudo, T.; et al. Malignant melanoma of the uterine cervix: A case report. J. Obs. Gynaecol. Res. 1997, 23, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.; Roberts, D.L.; Calvert, J.P.; Williams, S. Primary malignant melanomas of cervix uteri and vulva. Br. J. Derm. 1996, 135, 858–859. [Google Scholar] [CrossRef]
- Fleming, H.; Mein, P. Primary melanoma of the cervix. A case report. Acta Cytol. 1994, 38, 65–69. [Google Scholar] [PubMed]
- Moon, W.K.; Kim, S.H.; Han, M.C. MR findings of malignant melanoma of the vagina. Clin. Radiol. 1993, 48, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Joura, E.; Gitsch, G.; Kainz, C.; Berger, E.; Breitenecker, G. Case report of primary irradiated melanoma of the cervix uteri. Gynakol. Geburtshilfliche Rundsch 1992, 32 (Suppl. 1), 134. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, S.B.; Anderson, R.; Cohen, D.M. Primary malignant melanoma of the cervix and review of the literature. Gynecol. Oncol. 1992, 47, 398–403. [Google Scholar] [CrossRef]
- Khoo, U.S.; Collins, R.J.; Ngan, H.Y. Malignant melanoma of the female genital tract. A report of nine cases in the Chinese of Hong Kong. Pathology 1991, 23, 312–317. [Google Scholar] [CrossRef]
- Pinedo, F.; Ingelmo, J.M.; Miranda, P.; Garzon, A.; Lopez, J.I. Primary malignant melanoma of the uterine cervix: Case report and review of the literature. Gynecol. Obs. Invest. 1991, 31, 121–124. [Google Scholar] [CrossRef]
- Santoso, J.T.; Kucera, P.R.; Ray, J. Primary malignant melanoma of the uterine cervix: Two case reports and a century’s review. Obs. Gynecol. Surv. 1990, 45, 733–740. [Google Scholar] [CrossRef]
- Vleugels, M.P.; Brolmann, H.A.; van Beek, M. Primary melanoma of the cervix uteri, an avis rara? A review of the literature. Acta Obs. Gynecol. Scand. 1990, 69, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Podczaski, E.; Abt, A.; Kaminski, P.; Larson, J.; Sorosky, J.; DeGeest, K.; Mortel, R. A patient with multiple, malignant melanomas of the lower genital tract. Gynecol. Oncol. 1990, 37, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Chua, S.; Viegas, O.A.; Wee, A.; Ratnam, S.S. Malignant melanoma of the cervix. Gynecol. Obs. Invest. 1989, 27, 107–109. [Google Scholar] [CrossRef]
- Holmquist, N.D.; Torres, J. Malignant melanoma of the cervix. Report of a case. Acta Cytol. 1988, 32, 252–256. [Google Scholar]
- Owens, O.J.; Pollard, K.; Khoury, G.G.; Dyson, J.E.; Jarvis, G.J.; Joslin, C.A. Primary malignant melanoma of the uterine cervix. Clin. Radiol. 1988, 39, 336–338. [Google Scholar] [CrossRef]
- Yu, H.C.; Ketabchi, M. Detection of malignant melanoma of the uterine cervix from Papanicolaou smears. A case report. Acta Cytol. 1987, 31, 73–76. [Google Scholar] [PubMed]
- Krishnamoorthy, A.; Desai, M.; Simanowitz, M. Primary malignant melanoma of the cervix. Case report. Br. J. Obs. Gynaecol. 1986, 93, 84–86. [Google Scholar] [CrossRef]
- Ramsey, H.E.; Smith, H.B. Primary melanoma of the cervix: Report of a case. J. Natl. Med. Assoc. 1981, 73, 1149–1151. [Google Scholar]
- Mudge, T.J.; Johnson, J.; MacFarlane, A. Primary malignant melanoma of the cervix. Case report. Br. J. Obs. Gynaecol. 1981, 88, 1257–1259. [Google Scholar] [CrossRef]
- Genton, C.Y.; Kunz, J.; Schreiner, W.E. Primary malignant melanoma of the vagina and cervix uteri. Report of a case with ultrastructural study. Virchows Arch. A Pathol. Anat. Histol. 1981, 393, 245–250. [Google Scholar] [CrossRef]
- Hall, D.J.; Schneider, V.; Goplerud, D.R. Primary malignant melanoma of the uterine cervix. Obs. Gynecol. 1980, 56, 525–529. [Google Scholar]
- Puri, S.; Yoonessi, M.; Romney, S.L. Malignant melanoma of the cervix uteri. Obs. Gynecol. 1976, 47, 459–462. [Google Scholar]
- Jones, H.W., 3rd; Droegemueller, W.; Makowski, E.L. A primary melanocarcinoma of the cervix. Am. J. Obs. Gynecol. 1971, 111, 959–963. [Google Scholar] [CrossRef]
- Evers, H.H. A case of melanoma of the cervix. J. Obs. Gynaecol. Br. Emp. 1950, 57, 257–258. [Google Scholar]
- Cid, J.M. Melanoid pigmentation of the endocervix: A neurogenic visceral argument. Ann. Anat. Pathol. (Paris) 1959, 4, 617–628. [Google Scholar]
- Patel, D.S.; Bhagavan, B.S. Blue nevus of the uterine cervix. Hum. Pathol. 1985, 16, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Pusceddu, S.; Bajetta, E.; Carcangiu, M.L.; Formisano, B.; Ducceschi, M.; Buzzoni, R. A literature overview of primary cervical malignant melanoma: An exceedingly rare cancer. Crit. Rev. Oncol. Hematol. 2012, 81, 185–195. [Google Scholar] [CrossRef]
- Norms, H.J.; Taylor, H.B. Melanomas of the Vagina. Am. J. Clin. Pathol. 1966, 46, 420–426. [Google Scholar] [CrossRef] [Green Version]
- Kechagias, K.S.; Kalliala, I.; Bowden, S.J.; Athanasiou, A.; Paraskevaidi, M.; Paraskevaidis, E.; Dillner, J.; Nieminen, P.; Strander, B.; Sasieni, P.; et al. Role of human papillomavirus (HPV) vaccination on HPV infection and recurrence of HPV related disease after local surgical treatment: Systematic review and meta-analysis. BMJ 2022, 378, e070135. [Google Scholar] [CrossRef]
- Giannos, P.; Kechagias, K.S.; Bowden, S.; Tabassum, N.; Paraskevaidi, M.; Kyrgiou, M. PCNA in Cervical Intraepithelial Neoplasia and Cervical Cancer: An Interaction Network Analysis of Differentially Expressed Genes. Front. Oncol. 2021, 11, 4799. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Bowden, S.J.; Athanasiou, A.; Paraskevaidi, M.; Kechagias, K.; Zikopoulos, A.; Terzidou, V.; Martin-Hirsch, P.; Arbyn, M.; Bennett, P.; et al. Morbidity after local excision of the transformation zone for cervical intra-epithelial neoplasia and early cervical cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2021, 75, 10–22. [Google Scholar] [CrossRef]
- Doulgeraki, T.; Bowden, S.; Athanasiou, A.; Kechagias, K.; Lathouras, K.; Kalliala, I.; Kyrgiou, M. 280 Environmental and modifiable risk factors for cervical cancer: An umbrella review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 270, e83. [Google Scholar] [CrossRef]
- Ruer, J.B.; Pépin, L.; Gheit, T.; Vidal, C.; Kantelip, B.; Tommasino, M.; Prétet, J.L.; Mougin, C.; Aubin, F. Detection of alpha-and beta-human papillomavirus (HPV) in cutaneous melanoma: A matched and controlled study using specific multiplex PCR combined with DNA microarray primer extension. Exp. Dermatol. 2009, 18, 857–862. [Google Scholar] [CrossRef]
- Wang, D.; Xu, T.; Zhu, H.; Dong, J.; Fu, L. Primary malignant melanomas of the female lower genital tract: Clinicopathological characteristics and management. Am. J. Cancer Res. 2020, 10, 4017–4037. [Google Scholar]
- Borcoman, E.; Le Tourneau, C. Pembrolizumab in cervical cancer: Latest evidence and clinical usefulness. Ther. Adv. Med. Oncol. 2017, 9, 431–439. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kechagias, K.S.; Zafeiri, M.; Katsikas Triantafyllidis, K.; Kyrtsonis, G.; Geropoulos, G.; Lyons, D.; Burney Ellis, L.; Bowden, S.; Galani, A.; Paraskevaidi, M.; et al. Primary Melanoma of the Cervix Uteri: A Systematic Review and Meta-Analysis of the Reported Cases. Biology 2023, 12, 398. https://0-doi-org.brum.beds.ac.uk/10.3390/biology12030398
Kechagias KS, Zafeiri M, Katsikas Triantafyllidis K, Kyrtsonis G, Geropoulos G, Lyons D, Burney Ellis L, Bowden S, Galani A, Paraskevaidi M, et al. Primary Melanoma of the Cervix Uteri: A Systematic Review and Meta-Analysis of the Reported Cases. Biology. 2023; 12(3):398. https://0-doi-org.brum.beds.ac.uk/10.3390/biology12030398
Chicago/Turabian StyleKechagias, Konstantinos S., Marina Zafeiri, Konstantinos Katsikas Triantafyllidis, Georgios Kyrtsonis, Georgios Geropoulos, Deirdre Lyons, Laura Burney Ellis, Sarah Bowden, Apostolia Galani, Maria Paraskevaidi, and et al. 2023. "Primary Melanoma of the Cervix Uteri: A Systematic Review and Meta-Analysis of the Reported Cases" Biology 12, no. 3: 398. https://0-doi-org.brum.beds.ac.uk/10.3390/biology12030398