Changes of Exhaled Volatile Organic Compounds in Postoperative Patients Undergoing Analgesic Treatment: A Prospective Observational Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics and Outcome
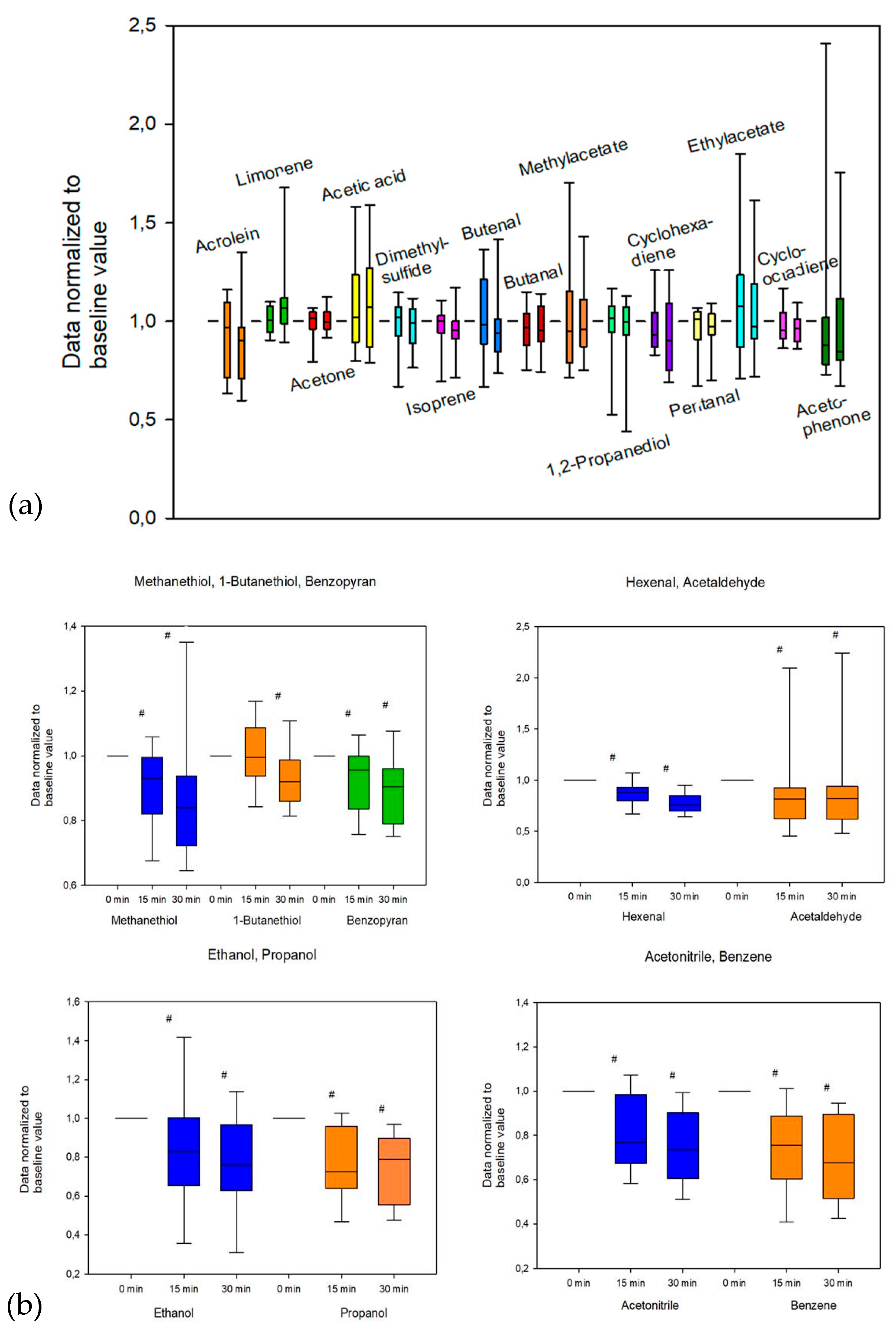
2.1.1. Changes in Exhaled VOCs
2.1.2. Changes in Cardiovascular Dynamics
2.1.3. Catecholamine Levels in Plasma
2.1.4. Correlation Analysis
2.1.5. Comparison of Patient Groups Using the NRS
3. Discussion
4. Materials and Methods
4.1. Design of the Study and Patients
4.2. General Anesthesia
4.3. Postoperative Care
4.4. Study Measurements of VOCs, Cardiovascular Variables, and Catecholamine Concentration in Plasma
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- McCaffery, M. Nursing Practice Theories Related to Cognition, Bodily Pain, and Man-Environment Interactions; University of California: Los Angeles, CA, USA, 1968. [Google Scholar]
- Harper, P. Postoperative pain: Why are patients’ self-reports so unreliable? Br. J. Nurs. 2007, 16, 1375. [Google Scholar] [CrossRef] [PubMed]
- Bechert, K.; Abraham, S.E. Pain management and wound care. J. Am. Col. Certif. Wound Spec. 2009, 1, 65–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiser, T.G.; Regenbogen, S.E.; Thompson, K.D.; Haynes, A.B.; Lipsitz, S.R.; Berry, W.R.; Gawande, A.A. An estimation of the global volume of surgery: A modelling strategy based on available data. Lancet 2008, 372, 139–144. [Google Scholar] [CrossRef]
- Fletcher, D.; Fermanian, C.; Mardaye, A.; Aegerter, P. A patient-based national survey on postoperative pain management in France reveals significant achievements and persistent challenges. Pain 2008, 137, 441–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, C.; Nestler, N.; Richter, H.; Hardinghaus, W.; Pogatzki-Zahn, E.; Zenz, M.; Osterbrink, J. The quality of pain management in German hospitals. Dtsch. Arztebl. Int. 2010, 107, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; Kaasa, S. Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: A systematic literature review. J. Pain Symptom Manag. 2011, 41, 1073–1093. [Google Scholar] [CrossRef]
- Miekisch, W.; Schubert, J.K.; Noeldge-Schomburg, G.F.E. Diagnostic potential of breath analysis--focus on volatile organic compounds. Clin. Chim. Acta 2004, 347, 25–39. [Google Scholar] [CrossRef]
- Amann, A.; Miekisch, W.; Schubert, J.; Buszewski, B.; Ligor, T.; Jezierski, T.; Pleil, J.; Risby, T. Analysis of exhaled breath for disease detection. Annu. Rev. Anal. Chem. 2014, 7, 455–482. [Google Scholar] [CrossRef]
- Fuchs, P.; Loeseken, C.; Schubert, J.K.; Miekisch, W. Breath gas aldehydes as biomarkers of lung cancer. Int. J. Cancer 2010, 126, 2663–2670. [Google Scholar] [CrossRef]
- De Lacy Costello, B.; Amann, A.; Al-Kateb, H.; Flynn, C.; Filipiak, W.; Khalid, T.; Osborne, D.; Ratcliffe, N.M. A review of the volatiles from the healthy human body. J. Breath Res. 2014, 8, 14001. [Google Scholar] [CrossRef] [PubMed]
- Sehnert, S.S.; Jiang, L.; Burdick, J.F.; Risby, T.H. Breath biomarkers for detection of human liver diseases: Preliminary study. Biomarkers 2002, 7, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Trefz, P.; Schmidt, S.C.; Sukul, P.; Schubert, J.K.; Miekisch, W.; Fischer, D.C. Non-Invasive Assessment of Metabolic Adaptation in Paediatric Patients Suffering from Type 1 Diabetes Mellitus. J. Clin. Med. 2019, 8, 1797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinkman, P.; Ahmed, W.M.; Gómez, C.; Knobel, H.H.; Weda, H.; Vink, T.J.; Nijsen, T.M.; Wheelock, C.E.; Dahlen, S.E.; Montuschi, P.; et al. Exhaled volatile organic compounds as markers for medication use in asthma. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef] [PubMed]
- Pabst, F.; Miekisch, W.; Fuchs, P.; Kischkel, S.; Schubert, J.K. Monitoring of oxidative and metabolic stress during cardiac surgery by means of breath biomarkers: An observational study. J. Cardiothorac. Surg. 2007, 2, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, C.S.; McMillan, L.C.; Stevenson, K.; Radhakrishnan, K.; Shiels, P.G.; Padgett, M.J.; Skeldon, K.D. Dynamic study of oxidative stress in renal dialysis patients based on breath ethane measured by optical spectroscopy. J. Breath Res. 2007, 1, 26005. [Google Scholar] [CrossRef]
- Hlastala, M.P.; Powell, F.L.; Anderson, J.C. Airway exchange of highly soluble gases. J. Appl. Physiol. 2013, 114, 675–680. [Google Scholar] [CrossRef] [Green Version]
- De Barros Falcão Ferraz, A.; da Silva, J.; Deimlimg, L.I.; Santos-Mello, R.; Sharlau, A.; von Poser, G.L.; Picada, J.N. Genotoxicity evaluation of three benzopyrans from Hypericum polyanthemum. Planta Med. 2009, 75, 37–40. [Google Scholar] [CrossRef]
- Ragab, F.A.E.-F.; Eid, N.M.; Hassan, G.S.; Nissan, Y.M. Synthesis and anti-inflammatory activity of some benzofuran and benzopyran-4-one derivatives. Chem. Pharm. Bull. 2012, 60, 110–120. [Google Scholar] [CrossRef] [Green Version]
- Haas, J.S.; Viana, A.F.; Heckler, A.P.M.; von Poser, G.L.; Rates, S.M.K. The antinociceptive effect of a benzopyran (HP1) isolated from Hypericum polyanthemum in mice hot-plate test is blocked by naloxone. Planta Med. 2010, 76, 1419–1423. [Google Scholar] [CrossRef]
- Jia, Z.; Patra, A.; Kutty, V.K.; Venkatesan, T. Critical Review of Volatile Organic Compound Analysis in Breath and In Vitro Cell Culture for Detection of Lung Cancer. Metabolites 2019, 9, 52. [Google Scholar] [CrossRef] [Green Version]
- Jordan, A.; Hansel, A.; Holzinger, R.; Lindinger, W. Acetonitrile and benzene in the breath of smokers and non-smokers investigated by proton transfer reaction mass spectrometry (PTR-MS). Int. J. Mass Spectrom. Ion Process. 1995, 148, L1–L3. [Google Scholar] [CrossRef]
- Tangerman, A. Measurement and biological significance of the volatile sulfur compounds hydrogen sulfide, methanethiol and dimethyl sulfide in various biological matrices. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2009, 877, 3366–3377. [Google Scholar] [CrossRef]
- Pellock, S.J.; Creekmore, B.C.; Walton, W.G.; Mehta, N.; Biernat, K.A.; Cesmat, A.P.; Ariyarathna, Y.; Dunn, Z.D.; Li, B.; Jin, J.; et al. Gut Microbial β-Glucuronidase Inhibition via Catalytic Cycle Interception. ACS Cent. Sci. 2018, 4, 868–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, M.A.M.; Aronoff, D.M. The influence of non-steroidal anti-inflammatory drugs on the gut microbiome. Clin. Microbiol. Infect. 2016, 22, 178.e1–178.e9. [Google Scholar] [CrossRef] [PubMed]
- Lötsch, J.; Geisslinger, G. Morphine-6-glucuronide: An analgesic of the future? Clin. Pharmacokinet. 2001, 40, 485–499. [Google Scholar] [CrossRef] [PubMed]
- Sukul, P.; Schubert, J.K.; Trefz, P.; Miekisch, W. Natural menstrual rhythm and oral contraception diversely affect exhaled breath compositions. Sci. Rep. 2018, 8, 10838. [Google Scholar] [CrossRef]
- Francino, M.P. Antibiotics and the Human Gut Microbiome: Dysbioses and Accumulation of Resistances. Front. Microbiol. 2015, 6, 1543. [Google Scholar] [CrossRef] [Green Version]
- Wickramasinghe, S.N.; Bond, A.N.; Sloviter, H.A.; Saunders, J.E. Metabolism of ethanol by human bone marrow cells. Acta Haematol. 1981, 66, 238–243. [Google Scholar] [CrossRef]
- Trefz, P.; Kamysek, S.; Fuchs, P.; Sukul, P.; Schubert, J.K.; Miekisch, W. Drug detection in breath: Non-invasive assessment of illicit or pharmaceutical drugs. J. Breath Res. 2017, 11, 24001. [Google Scholar] [CrossRef]
- Bond, A.N.; Wickramasinghe, S.N. Investigations into the production of acetate from ethanol by human blood and bone marrow cells in vitro. Acta Haematol. 1983, 69, 303–313. [Google Scholar] [CrossRef]
- Shin, H.W.; Umber, B.J.; Meinardi, S.; Leu, S.Y. Gas Signatures from Cultured Neutrophils and Peripheral Blood Mononuclear Cells Obtained from Healthy Humans. J. Mol. Biomark. Diagn. 2011, 2, 2. [Google Scholar] [CrossRef]
- Shin, H.W.; Umber, B.J.; Meinardi, S.; Leu, S.Y.; Zaldivar, F.; Blake, D.R.; Cooper, D.M. Acetaldehyde and hexanaldehyde from cultured white cells. J. Transl. Med. 2009, 7, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Moore, P.K. An overview of the biological significance of endogenous gases: New roles for old molecules. Biochem. Soc. Trans. 2007, 35, 1138–1141. [Google Scholar] [CrossRef] [PubMed]
- Chiba, S.; Tsukada, M. Potentiation of acetaldehyde-induced vasoconstrictions by cocaine in isolated and perfused arteries. Tohoku J. Exp. Med. 1991, 165, 63–65. [Google Scholar] [CrossRef] [Green Version]
- Saccò, M.; Meschi, M.; Regolisti, G.; Detrenis, S.; Bianchi, L.; Bertorelli, M.; Pioli, S.; Magnano, A.; Spagnoli, F.; Giuri, P.G.; et al. The relationship between blood pressure and pain. J. Clin. Hypertens. 2013, 15, 600–605. [Google Scholar] [CrossRef]
- McCartney, M.M.; Thompson, C.J.; Klein, L.R.; Ngo, J.H.; Seibel, J.D.; Fabia, F.; Simms, L.A.; Borras, E.; Young, B.S.; Lara, J.; et al. Breath carbonyl levels in a human population of seven hundred participants. J. Breath Res. 2020, 14, 46005. [Google Scholar] [CrossRef]
- Yamada, S.; Funada, T.; Shibata, N.; Kobayashi, M.; Kawai, Y.; Tatsuda, E.; Furuhata, A.; Uchida, K. Protein-bound 4-hydroxy-2-hexenal as a marker of oxidized n-3 polyunsaturated fatty acids. J. Lipid Res. 2004, 45, 626–634. [Google Scholar] [CrossRef] [Green Version]
- Yamauchi, Y.; Kunishima, M.; Mizutani, M.; Sugimoto, Y. Reactive short-chain leaf volatiles act as powerful inducers of abiotic stress-related gene expression. Sci. Rep. 2015, 5, 8030. [Google Scholar] [CrossRef] [Green Version]
- Mano, J.I.; Tokushige, K.; Mizoguchi, H.; Fujii, H.; Khorobrykh, S. Accumulation of lipid peroxide-derived, toxic α, β-unsaturated aldehydes (E)-2-pentenal, acrolein and (E)-2-hexenal in leaves under photoinhibitory illumination. Plant Biotechnol. 2010, 27, 193–197. [Google Scholar] [CrossRef] [Green Version]
- Ratcliffe, N.; Wieczorek, T.; Drabińska, N.; Gould, O.; Osborne, A.; de Lacy Costello, B. A mechanistic study and review of volatile products from peroxidation of unsaturated fatty acids: An aid to understanding the origins of volatile organic compounds from the human body. J. Breath Res. 2020, 14, 34001. [Google Scholar] [CrossRef]
- Hjemdahl, P. Plasma catecholamines—Analytical challenges and physiological limitations. Baillière’s Clin. Endocrinol. Metab. 1993, 7, 307–353. [Google Scholar] [CrossRef]
- Wagemakers, S.H.; van der Velden, J.M.; Gerlich, A.S.; Hindriks-Keegstra, A.W.; van Dijk, J.F.M.; Verhoeff, J.J.C. A Systematic Review of Devices and Techniques that Objectively Measure Patients’ Pain. Pain Physician 2019, 22, 1–13. [Google Scholar] [PubMed]
- Trefz, P.; Schmidt, M.; Oertel, P.; Obermeier, J.; Brock, B.; Kamysek, S.; Dunkl, J.; Zimmermann, R.; Schubert, J.K.; Miekisch, W. Continuous real time breath gas monitoring in the clinical environment by proton-transfer-reaction-time-of-flight-mass spectrometry. Anal. Chem. 2013, 85, 10321–10329. [Google Scholar] [CrossRef] [PubMed]
- Bikov, A.; Paschalaki, K.; Logan-Sinclair, R.; Horváth, I.; Kharitonov, S.A.; Barnes, P.J.; Usmani, O.S.; Paredi, P. Standardised exhaled breath collection for the measurement of exhaled volatile organic compounds by proton transfer reaction mass spectrometry. BMC Pulm. Med. 2013, 13, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boshier, P.R.; Priest, O.H.; Hanna, G.B.; Marczin, N. Influence of respiratory variables on the on-line detection of exhaled trace gases by PTR-MS. Thorax 2011, 66, 919–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukul, P.; Oertel, P.; Kamysek, S.; Trefz, P. Oral or nasal breathing? Real-time effects of switching sampling route onto exhaled VOC concentrations. J. Breath Res. 2017, 11, 27101. [Google Scholar] [CrossRef]
- Sukul, P.; Schubert, J.K.; Oertel, P.; Kamysek, S.; Taunk, K.; Trefz, P.; Miekisch, W. FEV manoeuvre induced changes in breath VOC compositions: An unconventional view on lung function tests. Sci. Rep. 2016, 6, 28029. [Google Scholar] [CrossRef]
- Sukul, P.; Schubert, J.K.; Kamysek, S.; Trefz, P.; Miekisch, W. Applied upper-airway resistance instantly affects breath components: A unique insight into pulmonary medicine. J. Breath Res. 2017, 11, 47108. [Google Scholar] [CrossRef]
- Trefz, P.; Pugliese, G.; Brock, B.; Schubert, J.K.; Miekisch, W. Effects of elevated oxygen levels on VOC analysis by means of PTR-ToF-MS. J. Breath Res. 2019, 13, 46004. [Google Scholar] [CrossRef]
- Pugliese, G.; Trefz, P.; Brock, B.; Schubert, J.K.; Miekisch, W. Extending PTR based breath analysis to real-time monitoring of reactive volatile organic compounds. Analyst 2019, 144, 7359–7367. [Google Scholar] [CrossRef]
- Trefz, P.; Schubert, J.K.; Miekisch, W. Effects of humidity, CO2 and O2 on real-time quantitation of breath biomarkers by means of PTR-ToF-MS. J. Breath Res. 2018, 12, 26016. [Google Scholar] [CrossRef] [PubMed]
- Brock, B.; Kamysek, S.; Silz, J.; Trefz, P.; Schubert, J.K.; Miekisch, W. Monitoring of breath VOCs and electrical impedance tomography under pulmonary recruitment in mechanically ventilated patients. J. Breath Res. 2017, 11, 16005. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographics | |
| sex (male/female) | 15/5 |
| age (year) | 60 (48;67) |
| height (cm) | 175 (172;182) |
| body weight (kg) | 88 (67.2;104.3) |
| body mass index | 29.5 (21.8;33.3) |
| body surface (m2) | 2.05 (1.8;2.26) |
| ASA Physical Status Classification (Grade) | |
| I | 15% (3/20) |
| II | 35% (7/20) |
| III | 50% (10/20) |
| Permanent Medication | |
| non-opioid analgesics | 40% (8/20) |
| opioids | 20% (4/20) |
| blood thinners | 35% (7/20) |
| statins | 25% (5/20) |
| antihypertensives | 45% (9/20) |
| diuretics | 35% (7/20) |
| thyroid hormones | 15% (3/20) |
| Pre-existing Medical Conditions | |
| lung diseases | 15% (3/20) |
| cardiovascular diseases | 70% (14/20) |
| renal failure | 15% (3/20) |
| diabetes mellitus | 5% (1/20) |
| history of smoking | 30% (6/20) |
| Type of Surgery | |
| general surgery/visceral surgery | 45% (9/20) |
| trauma surgery | 25% (5/20) |
| neurosurgery | 20% (4/20) |
| vascular surgery | 10% (2/20) |
| Tentative VOC | (A) Baseline (0 min) (ncps) | (B) 15 min (ncps) | (C) 30 Min. (ncps) | p Friedman Test | p A vs. B | p A vs. C | p B vs. C |
|---|---|---|---|---|---|---|---|
| acetonitrile | 353.0 (308.5;746.3) | 324.8 (219.1;690.6) | 282.2 (212.1;627.9) | <0.001 | <0.001 | <0.001 | 0.014 |
| acetaldehyde | 511.7 (341.9;1058.5) | 401.6 (289.7;908.8) | 386.5 (304.5;851.2) | 0.002 | 0.002 | 0.001 | 0.074 |
| ethanol | 73.9 (58.2;142.4) | 55.0 (42.8;130.4) | 52.0 (40.3;111.3) | 0.003 | <0.001 | 0.003 | 0.18 |
| methanethiol | 665.6 (71.1;4745.8) | 550.2 (49.1;4668.9) | 471.1 (47.2;4152.1) | <0.001 | 0.004 | <0.001 | <0.001 |
| acrolein | 81.4 (65.1;119.0) | 73.9 (54.4;101.5) | 68.1 (52.1;108.3) | 0.058 | n.a. | n.a. | n.a. |
| acetone (via isotope at m/z 60) | 2954.7 (1676.6;5929.1) | 2595.4 (1733.3;5612.3) | 2796.4 (1769.7;6038.5) | 0.819 | n.a. | n.a. | n.a. |
| acetic acid | 584.0 (327.4;1063.1) | 540.6 (323.4;713.0) | 554.5 (312.5;913.5) | 0.819 | n.a. | n.a. | n.a. |
| propanol | 641.5 (460.1;1397.1) | 555.0 (330.9;981.8) | 551.1 (301.4;888.4) | <0.001 | <0.001 | <0.001 | 0.655 |
| dimethyl-sulfide | 55.4 (35.1;115.0) | 49.7 (37.1;113.4) | 49.5 (38.3;110.5) | 0.951 | n.a. | n.a. | n.a. |
| isoprene | 2312.1 (1579.8;2910.0) | 2140.3 (1266.4;2736.5) | 2155,2 (1486.7;2508.1) | 0.142 | n.a. | n.a. | n.a. |
| butenal | 27.9 (20.4;55.6) | 25.2 (19.8;43.9) | 25.5 (18.8;47.0) | 0.212 | n.a. | n.a. | n.a. |
| butanal | 60.8 (47.3;89.6) | 61.6 (46.3;79.2) | 59.4 (44.9;83.3) | 0.387 | n.a. | n.a. | n.a. |
| methylacetate | 160.8 (105.7;266.8) | 150.3 (130.5;204.0) | 145.6 (110.3;228.3) | 0.247 | n.a. | n.a. | n.a. |
| 1,2-propanediol | 55.8 (21.6;147.2) | 47.2 (22.4;151.2) | 46.3 (23.9;154.5) | 0.951 | n.a. | n.a. | n.a. |
| benzene | 21.4 (14.8;48.2) | 18.7 (12.1;28.1) | 15.7 (10.7;29.0) | <0.001 | <0.001 | <0.001 | 0.044 |
| cyclohexadiene | 273.1 (71.7;1325.3) | 319.9 (74.7;1168.6) | 285.0 (88.8;1075.9) | 0.247 | n.a. | n.a. | n.a. |
| pentanal | 28.3 (18.6;44.8) | 23.8 (18.6;45.6) | 24.8 (18.5;46.5) | 0.819 | n.a. | n.a. | n.a. |
| ethylacetate | 36.9 (23.7;77.7) | 38.0 (23.9;78.1) | 45.5 (22.2;73.5) | 0.387 | n.a. | n.a. | n.a. |
| 1-butanethiol | 25.8 (17.3;150.2) | 25.6 (20.0;160.7) | 23.8 (18.2;159.9) | 0.004 | 0.655 | 0.008 | <0.001 |
| hexenal | 76.1 (42.0;1558.9.3) | 63.1 (37.4;1728.4) | 53.2 (36.0;1497.3) | <0.001 | <0.001 | <0.001 | <0.001 |
| cyclooctadiene | 63.5 (53.6;68.3) | 60.0 (50.3;70.5) | 57.3 (52.4;64.4) | 0.142 | n.a. | n.a. | n.a. |
| acetophenone | 77.8 (64.5;104.6) | 72.4 (55.7;153.4) | 70.4 (55.3;142.8) | 0.074 | n.a. | n.a. | n.a. |
| benzopyran | 57.0 (11.4;630.6) | 52.2 (12.1;600.6) | 43.6 (10.7;523.0) | 0.004 | 0.007 | 0.003 | 0.044 |
| limonene | 27.5 (21.0;38.8) | 27.1 (21.1;41.9) | 26.7 (22.2;49.6) | 0.116 | n.a. | n.a. | n.a. |
| Catecholamine | Prior to Analgesic Treatment (nmol/L) | 30 min after Analgesic Treatment (nmol/L) | p |
|---|---|---|---|
| epinephrine | 0.31 (0.10;1.02) | 0.51 (0.11;1.21) | 0.492 |
| norepinephrine | 1.94 (1.52;5.77) | 1.97 (1.37;3.66) | 0.044 |
| dopamine | 0.19 (0.04;0.52) | 0.28 (0.11;0.34) | 0.557 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Löser, B.; Grabenschröer, A.; Pugliese, G.; Sukul, P.; Trefz, P.; Schubert, J.K.; Miekisch, W. Changes of Exhaled Volatile Organic Compounds in Postoperative Patients Undergoing Analgesic Treatment: A Prospective Observational Study. Metabolites 2020, 10, 321. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo10080321
Löser B, Grabenschröer A, Pugliese G, Sukul P, Trefz P, Schubert JK, Miekisch W. Changes of Exhaled Volatile Organic Compounds in Postoperative Patients Undergoing Analgesic Treatment: A Prospective Observational Study. Metabolites. 2020; 10(8):321. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo10080321
Chicago/Turabian StyleLöser, Benjamin, Alina Grabenschröer, Giovanni Pugliese, Pritam Sukul, Phillip Trefz, Jochen K Schubert, and Wolfram Miekisch. 2020. "Changes of Exhaled Volatile Organic Compounds in Postoperative Patients Undergoing Analgesic Treatment: A Prospective Observational Study" Metabolites 10, no. 8: 321. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo10080321