
Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment


Abstract
:1. Introduction
2. Vitamin D Sources and Metabolism
2.1. Sources
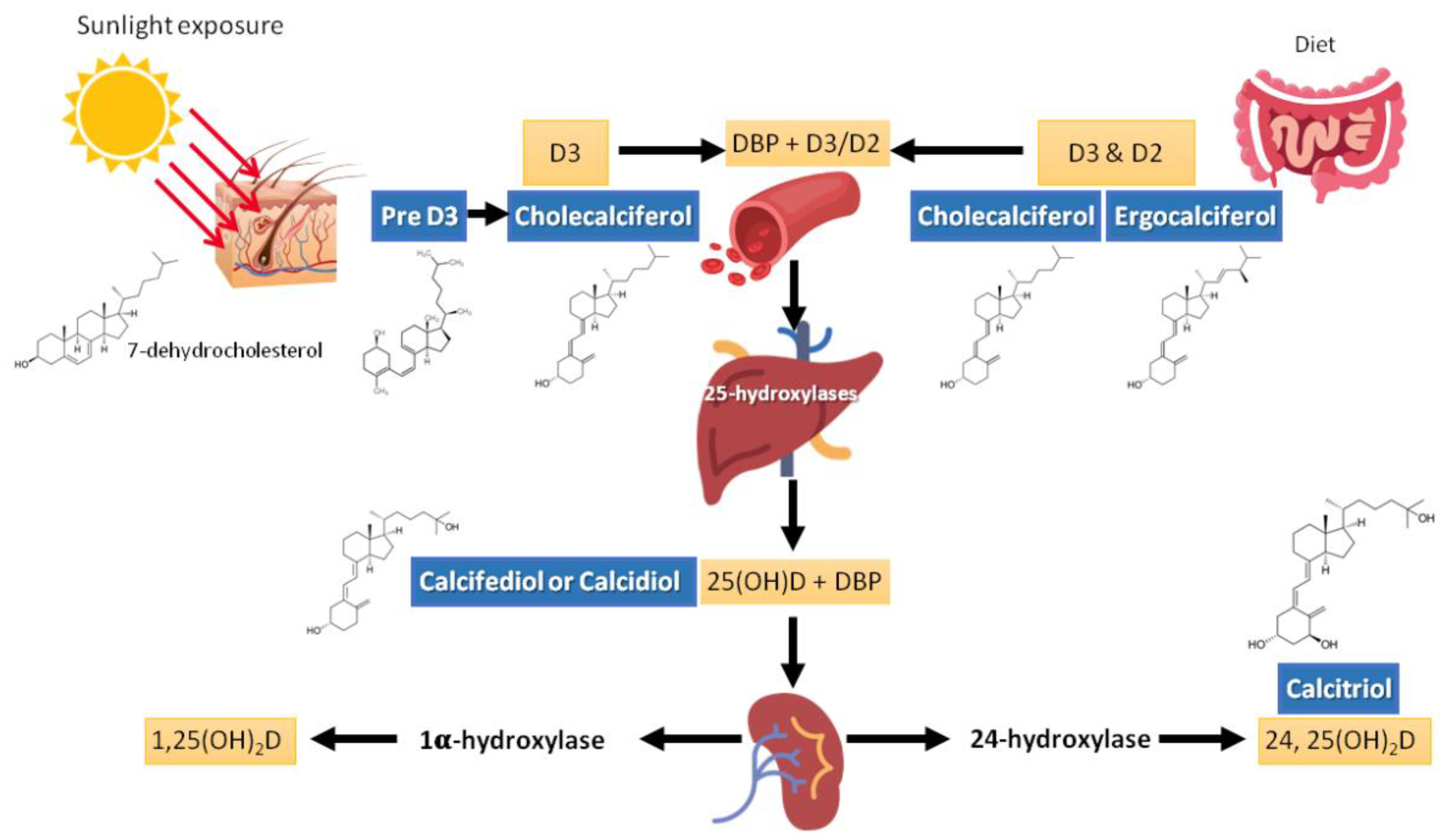
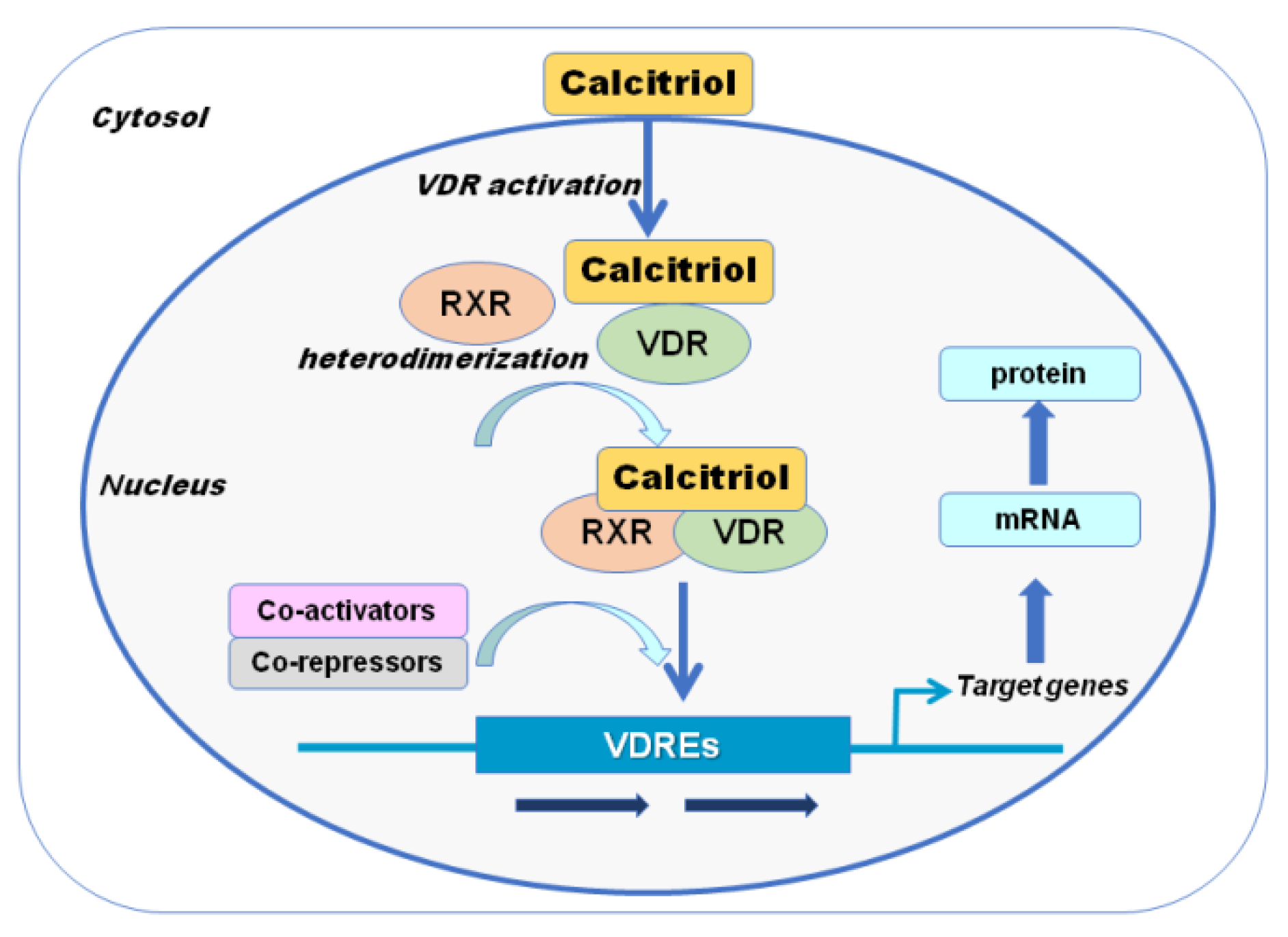
2.2. Metabolism
2.3. Pharmacokinetics
2.4. Measurements
2.5. Optimal Values
3. Vitamin D Actions
3.1. Calcium, Phosphate, and Bone Metabolism
3.2. Other Non-Skeletal or Mineral Actions
4. Vitamin D Deficiency
4.1. Dimension of the Problem—Epidemiology
4.2. Clinical Characteristics
4.3. Management of Vitamin D Deficiency
5. Vitamin D Excess/Toxicity
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rosen, C.J.; Adams, J.S.; Bikle, D.D.; Black, D.M.; DeMay, M.B.; Manson, J.E.; Murad, M.H.; Kovacs, C.S. The Nonskeletal Effects of Vitamin D: An Endocrine Society Scientific Statement. Endocr. Rev. 2012, 33, 456–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Pike, J.W.; Christakos, S. Biology and Mechanisms of Action of the Vitamin D Hormone. Endocrinol. Metab. Clin. N. Am. 2017, 46, 815–843. [Google Scholar] [CrossRef] [PubMed]
- Sanders, K.M.; Stuart, A.L.; Williamson, E.J.; Simpson, J.A.; Kotowicz, M.A.; Young, D.; Nicholson, G.C. Annual high-dose oral vitamin D and falls and fractures in older women: A randomized controlled trial. JAMA 2010, 303, 1815–1822. [Google Scholar] [CrossRef] [Green Version]
- Glendenning, P.; Zhu, K.; Inderjeeth, C.; Howat, P.; Lewis, J.R.; Prince, R.L. Effects of three-monthly oral 150,000 IU cholecalciferol supplementation on falls, mobility, and muscle strength in older postmenopausal women: A randomized controlled trial. J. Bone Miner. Res. 2011, 27, 170–176. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Grossman, D.C.; Curry, S.J.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; Krist, A.H.; et al. Vitamin D, Calcium, or Combined Supplementation for the Primary Prevention of Fractures in Community-Dwelling Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1592–1599. [Google Scholar]
- Reid, I.R.; Bolland, M.J. Calcium and/or Vitamin D Supplementation for the Prevention of Fragility Fractures: Who Needs It? Nutrients 2020, 12, 1011. [Google Scholar] [CrossRef] [Green Version]
- Carmel, A.S.; Shieh, A.; Bang, H.; Bockman, R.S. The 25(OH)D level needed to maintain a favorable bisphosphonate response is >/=33 ng/mL. Osteoporos. Int. 2012, 23, 2479–2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peris, P.; Martínez-Ferrer, A.; Monegal, A.; de Osaba, M.J.M.; Muxi, A.; Guañabens, N. 25 hydroxyvitamin D serum levels influence adequate response to bisphosphonate treatment in postmenopausal osteoporosis. Bone 2012, 51, 54–58. [Google Scholar] [CrossRef]
- Wolf, G. The Discovery of Vitamin D: The Contribution of Adolf Windaus. J. Nutr. 2004, 134, 1299–1302. [Google Scholar] [CrossRef]
- Blunt, J.W.; Tanaka, Y.; DeLuca, H.F. Biological activity of 25-hydroxycholecalciferol, a metabolite of vitamin D3. Proc. Natl. Acad. Sci. USA 1968, 61, 1503–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponchon, G.; Kennan, A.L.; DeLuca, H.F. “Activation” of vitamin D by the liver. J. Clin. Investig. 1969, 48, 2032–2037. [Google Scholar] [CrossRef] [PubMed]
- Norman, A.W.; Myrtle, J.F.; Midgett, R.J.; Nowicki, H.G.; Williams, V.; Popják, G.; Miogett, R.J.; Popjaak, G. 1,25-Dihydroxycholecalciferol: Identification of the Proposed Active Form of Vitamin D3 in the Intestine. Science 1971, 173, 51–54. [Google Scholar] [CrossRef]
- Holick, M.; Schnoes, H.K.; DeLuca, H.F. Identification of 1,25-Dihydroxycholecalciferol, a Form of Vitamin D3 Metabolically Active in the Intestine. Proc. Natl. Acad. Sci. USA 1971, 68, 803–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80, 1689S–1696S. [Google Scholar] [CrossRef] [Green Version]
- Dattola, A.; Silvestri, M.; Bennardo, L.; Passante, M.; Scali, E.; Patruno, C.; Nisticò, S.P. Role of Vitamins in Skin Health: A Systematic Review. Curr. Nutr. Rep. 2020, 9, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Engelsen, O. Calculated ultraviolet exposure levels for a healthy vitamin D status. Photochem. Photobiol. 2006, 82, 1697–1703. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: Importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am. J. Clin. Nutr. 2004, 79, 362–371. [Google Scholar] [CrossRef] [Green Version]
- Vieth, R. Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety. Am. J. Clin. Nutr. 1999, 69, 842–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, J.G. Vitamin D—Solar rays, the Milky Way, or both? N. Engl. J. Med. 1992, 326, 1213–1215. [Google Scholar] [CrossRef]
- Binkley, N.; Novotny, R.; Krueger, D.; Kawahara, T.; Daida, Y.G.; Lensmeyer, G.; Hollis, B.W.; Drezner, M.K. Low Vitamin D Status despite Abundant Sun Exposure. J. Clin. Endocrinol. Metab. 2007, 92, 2130–2135. [Google Scholar] [CrossRef] [Green Version]
- Neville, J.J.; Palmieri, T.; Young, A.R. Physical Determinants of Vitamin D Photosynthesis: A Review. JBMR Plus 2021, 5, e10460. [Google Scholar] [CrossRef]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef]
- Lucas, R.M.; Yazar, S.; Young, A.R.; Norval, M.; de Gruijl, F.R.; Takizawa, Y.; Rhodes, L.E.; Sinclair, C.A.; Neale, R.E. Human health in relation to exposure to solar ultraviolet radiation under changing stratospheric ozone and climate. Photochem. Photobiol. Sci. 2019, 18, 641–680. [Google Scholar] [CrossRef]
- Webb, A.R.; DeCosta, B.R.; Holick, M.F. Sunlight Regulates the Cutaneous Production of Vitamin D3 by Causing Its Photodegradation. J. Clin. Endocrinol. Metab. 1989, 68, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Kütting, B.; Drexler, H. Evaluation of Skin-Protective Means against Acute and Chronic Effects of Ultraviolet Radiation from Sunlight. Metab. Disord. Nutr. Correl. Skin 2007, 34, 87–97. [Google Scholar]
- Thompson, G.R.; Lewis, B.; Booth, C.C. Absorption of vitamin D3-3H in control subjects and patients with intestinal malabsorption. J. Clin. Investig. 1966, 45, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Maislos, M.; Silver, J.; Fainaru, M. Intestinal absorption of vitamin D sterols: Differential absorption into lymph and portal blood in the rat. Gastroenterology 1981, 80, 1528–1534. [Google Scholar] [CrossRef]
- Davies, M.; Mawer, E.B.; Krawitt, E.L. Comparative absorption of vitamin D3 and 25-hydroxyvitamin D3 in intestinal disease. Gut 1980, 21, 287–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitrin, M.D.; Bengoa, J.M. Intestinal absorption of cholecalciferol and 25-hydroxycholecalciferol in chronic cholestatic liver disease. Am. J. Clin. Nutr. 1987, 46, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Larson-Meyer, D.E.; Douglas, C.S.; Thomas, J.J.; Johnson, E.C.; Barcal, J.N.; Heller, J.E.; Hollis, B.W.; Halliday, T.M. Validation of a Vitamin D Specific Questionnaire to Determine Vitamin D Status in Athletes. Nutrients 2019, 11, 2732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruins, M.J.; Létinois, U. Adequate Vitamin D Intake Cannot Be Achieved within Carbon Emission Limits Unless Food Is Fortified: A Simulation Study. Nutrients 2021, 13, 592. [Google Scholar] [CrossRef]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef]
- Bikle, D.D. Vitamin D: An ancient hormone. Exp. Dermatol. 2011, 20, 7–13. [Google Scholar] [CrossRef]
- Haussler, M.R.; Norman, A.W. Chromosomal Receptor for a Vitamin D Metabolite. Proc. Natl. Acad. Sci. USA 1969, 62, 155–162. [Google Scholar] [CrossRef] [Green Version]
- McDonnell, D.P.; Mangelsdorf, D.J.; Pike, J.W.; Haussler, M.R.; O’Malley, B.W. Molecular cloning of complementary DNA encoding the avian receptor for vitamin D. Science 1987, 235, 1214–1217. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.R.; McDonnell, D.P.; Hughes, M.; Crisp, T.M.; Mangelsdorf, D.J.; Haussler, M.R.; Pike, J.W.; Shine, J.; O’Malley, B.W. Cloning and expression of full-length cDNA encoding human vitamin D receptor. Proc. Natl. Acad. Sci. USA 1988, 85, 3294–3298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshizawa, T.; Handa, Y.; Uematsu, Y.; Takeda, S.; Sekine, K.; Yoshihara, Y.; Kawakami, T.; Arioka, K.; Sato, H.; Uchiyama, Y.; et al. Mice lacking the vitamin D receptor exhibit impaired bone formation, uterine hypoplasia and growth retardation after weaning. Nat. Genet. 1997, 16, 391–396. [Google Scholar] [CrossRef]
- Walters, M.R. Newly identified actions of the vitamin D endocrine system. Endocr. Rev. 1992, 13, 719–764. [Google Scholar] [PubMed]
- Smith, J.E.; Goodman, D.S. The turnover and transport of vitamin D and of a polar metabolite with the properties of 25-hydroxycholecalciferol in human plasma. J. Clin. Investig. 1971, 50, 2159–2167. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.J. Regulation of vitamin D action. Nephrol. Dial. Transplant. 1999, 14, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Driel, M.; Koedam, M.; Buurman, C.J.; Roelse, M.; Weyts, F.; Chiba, H.; Uitterlinden, A.G.; Pols, H.A.P.; van Leeuwen, J.P.T.M. Evidence that both 1alpha,25-dihydroxyvitamin D3 and 24-hydroxylated D3 enhance human osteoblast differentiation and mineralization. J. Cell Biochem. 2006, 99, 922–935. [Google Scholar] [CrossRef]
- Takeyama, K.; Kitanaka, S.; Sato, T.; Kobori, M.; Yanagisawa, J.; Kato, S. 25-Hydroxyvitamin D3 1alpha-hydroxylase and vitamin D synthesis. Science 1997, 277, 1827–1830. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Guerrero-Romero, F.; Barbagallo, M. Magnesium in Infectious Diseases in Older People. Nutrients 2021, 13, 180. [Google Scholar] [CrossRef]
- Anast, C.S.; Mohs, J.M.; Kaplan, S.L.; Burns, T.W. Evidence for Parathyroid Failure in Magnesium Deficiency. Science 1972, 177, 606–608. [Google Scholar] [CrossRef] [PubMed]
- Medalle, R.; Waterhouse, C.; Hahn, T.J. Vitamin D resistance in magnesium deficiency. Am. J. Clin. Nutr. 1976, 29, 854–858. [Google Scholar] [CrossRef]
- Rude, R.K.; Oldham, S.B.; Sharp, C.F., Jr.; Singer, F.R. Parathyroid hormone secretion in magnesium deficiency. J. Clin. Endocrinol. Metab. 1978, 47, 800–806. [Google Scholar] [CrossRef]
- Mutnuri, S.; Fernandez, I.; Kochar, T. Suppression of Parathyroid Hormone in a Patient with Severe Magnesium Depletion. Case Rep. Nephrol. 2016, 2016, 2608538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, M.M.; Deluccia, R.; Ramadoss, R.K.; Aljahdali, A.; Volpe, S.L.; Shewokis, P.A.; Sukumar, D. Low dietary magnesium intake alters vitamin D—parathyroid hormone relationship in adults who are overweight or obese. Nutr. Res. 2019, 69, 82–93. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Solmi, M.; Noale, M.; Vaona, A.; Demurtas, J.; Maggi, S. Dietary magnesium intake and fracture risk: Data from a large prospective study. Br. J. Nutr. 2017, 117, 1570–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, X.; Song, Y.; Manson, J.E.; Signorello, L.B.; Zhang, S.M.; Shrubsole, M.J.; Ness, R.M.; Seidner, D.L.; Dai, Q. Magnesium, vitamin D status and mortality: Results from US National Health and Nutrition Examination Survey (NHANES) 2001 to 2006 and NHANES III. BMC Med. 2013, 11, 187. [Google Scholar] [CrossRef] [Green Version]
- Dai, Q.; Zhu, X.; Manson, J.E.; Song, Y.; Li, X.; Franke, A.A.; Costello, R.B.; Rosanoff, A.; Nian, H.; Fan, L.; et al. Magnesium status and supplementation influence vitamin D status and metabolism: Results from a randomized trial. Am. J. Clin. Nutr. 2018, 108, 1249–1258. [Google Scholar] [CrossRef] [PubMed]
- Zehnder, D.; Bland, R.; Walker, E.A.; Bradwell, A.R.; Howie, A.J.; Hewison, M.; Stewart, P.M. Expression of 25-hydroxyvitamin D3-1alpha-hydroxylase in the human kidney. J. Am. Soc. Nephrol. 1999, 10, 2465–2473. [Google Scholar] [PubMed]
- Prié, D.; Friedlander, G. Reciprocal Control of 1,25-Dihydroxyvitamin D and FGF23 Formation Involving the FGF23/Klotho System. Clin. J. Am. Soc. Nephrol. 2010, 5, 1717–1722. [Google Scholar] [CrossRef]
- Liu, S.; Tang, W.; Zhou, J.; Stubbs, J.R.; Luo, Q.; Pi, M.; Quarles, L.D. Fibroblast growth factor 23 is a counter-regulatory phosphaturic hormone for vitamin D. J. Am. Soc. Nephrol. 2006, 17, 1305–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negri, A.L. Proximal tubule endocytic apparatus as the specific renal uptake mechanism for vitamin D-binding protein/25-(OH)D3 complex. Nephrology 2006, 11, 510–515. [Google Scholar] [CrossRef]
- Hewison, M.; Burke, F.; Evans, K.N.; Lammas, D.A.; Sansom, D.M.; Liu, P.; Modlin, R.L.; Adams, J.S. Extra-renal 25-hydroxyvitamin D3-1α-hydroxylase in human health and disease. J. Steroid Biochem. Mol. Biol. 2007, 103, 316–321. [Google Scholar] [CrossRef]
- Zhou, Y.; Lower, E.E. Balancing Altered Calcium Metabolism with Bone Health in Sarcoidosis. Semin. Respir. Crit. Care Med. 2020, 41, 618–625. [Google Scholar] [CrossRef]
- Aloia, J.F.; Patel, M.; Dimaano, R.; Li-Ng, M.; Talwar, S.A.; Mikhail, M.; Pollack, S.; Yeh, J.K. Vitamin D intake to attain a desired serum 25-hydroxyvitamin D concentration. Am. J. Clin. Nutr. 2008, 87, 1952–1958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deb, S.; Reeves, A.A.; LaFortune, S. Simulation of Physicochemical and Pharmacokinetic Properties of Vitamin D3 and Its Natural Derivatives. Pharmaceuticals 2020, 13, 160. [Google Scholar] [CrossRef] [PubMed]
- Foissac, F.; Treluyer, J.-M.; Souberbielle, J.-C.; Rostane, H.; Urien, S.; Viard, J.-P. Vitamin D3 supplementation scheme in HIV-infected patients based upon pharmacokinetic modelling of 25-hydroxycholecalciferol. Br. J. Clin. Pharmacol. 2013, 75, 1312–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawyer, M.E.; Tran, H.T.; Evans, M.V. A physiologically based pharmacokinetic model of vitamin D. J. Appl. Toxicol. 2017, 37, 1448–1454. [Google Scholar] [CrossRef]
- Sempos, C.T.; Heijboer, A.C.; Bikle, D.D.; Bollerslev, J.; Bouillon, R.; Brannon, P.M.; DeLuca, H.F.; Jones, G.; Munns, C.F.; Bilezikian, J.P.; et al. Vitamin D assays and the definition of hypovitaminosis D: Results from the First International Conference on Controversies in Vitamin D. Br. J. Clin. Pharmacol. 2018, 84, 2194–2207. [Google Scholar] [CrossRef]
- Vieth, R. What is the optimal vitamin D status for health? Prog. Biophys. Mol. Biol. 2006, 92, 26–32. [Google Scholar] [CrossRef]
- Bouillon, R. Free or Total 25OHD as Marker for Vitamin D Status? J. Bone Miner. Res. 2016, 31, 1124–1127. [Google Scholar] [CrossRef] [Green Version]
- Phinney, K.W.; Bedner, M.; Tai, S.S.C.; Vamathevan, V.V.; Sander, L.C.; Sharpless, K.E.; Wise, S.A.; Yen, J.H.; Schleicher, R.L.; Chaudhary-Webb, M.; et al. Development and certification of a standard reference material for vitamin D metabolites in human serum. Anal. Chem. 2012, 84, 956–962. [Google Scholar] [CrossRef] [Green Version]
- Carter, G.; Berry, J.; Durazo-Arvizu, R.; Gunter, E.; Jones, G.; Jones, J.; Makin, H.; Pattni, P.; Sempos, C.; Twomey, P.; et al. Hydroxyvitamin D assays: An historical perspective from DEQAS. J. Steroid Biochem. Mol. Biol. 2018, 177, 30–35. [Google Scholar] [CrossRef]
- Binkley, N.C.; Wiebe, D.A. It’s Time to Stop Prescribing Ergocalciferol. Endocr. Pract. 2018, 24, 1099–1102. [Google Scholar] [CrossRef]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bouillon, R.; Ebeling, P.R.; Lazaretti-Castro, M.; Marcocci, C.; Rizzoli, R.; Sempos, C.T.; Bilezikian, J.P. Controversies in Vitamin D: Summary Statement From an International Conference. J. Clin. Endocrinol. Metab. 2019, 104, 234–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergwitz, C.; Jüppner, H. Regulation of Phosphate Homeostasis by PTH, Vitamin D, and FGF23. Annu. Rev. Med. 2010, 61, 91–104. [Google Scholar] [CrossRef] [Green Version]
- Boucher, B.J. Why do so many trials of vitamin D supplementation fail? Endocr. Connect. 2020, 9, R195–R206. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Sluyter, J.D. Is There Proof of Extraskeletal Benefits From Vitamin D Supplementation From Recent Mega Trials of Vitamin D? JBMR Plus 2021, 5, e10459. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knechtle, B.; Nikolaidis, P.T. Vitamin D and Sport Performance. Nutrients 2020, 12, 841. [Google Scholar] [CrossRef] [Green Version]
- Wiciński, M.; Adamkiewicz, D.; Adamkiewicz, M.; Śniegocki, M.; Podhorecka, M.; Szychta, P.; Malinowski, B. Impact of Vitamin D on Physical Efficiency and Exercise Performance-A Review. Nutrients 2019, 11, 2826. [Google Scholar] [CrossRef] [Green Version]
- Bischoff, H.; Borchers, M.; Gudat, F.; Duermueller, U.; Theiler, R.; Stähelin, H.; Dick, W. In Situ Detection of 1,25-dihydroxyvitamin D Receptor in human Skeletal Muscle Tissue. J. Mol. Histol. 2001, 33, 19–24. [Google Scholar]
- Wang, Y.; DeLuca, H.F. Is the Vitamin D Receptor Found in Muscle? Endocrinology 2010, 152, 354–363. [Google Scholar] [CrossRef] [Green Version]
- Srikuea, R.; Zhang, X.; Park-Sarge, O.-K.; Esser, K.A. VDR and CYP27B1 are expressed in C2C12 cells and regenerating skeletal muscle: Potential role in suppression of myoblast proliferation. Am. J. Physiol. Cell Physiol. 2012, 303, C396–C405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceglia, L. Vitamin D and skeletal muscle tissue and function. Mol. Asp. Med. 2008, 29, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Koundourakis, N.E.; Avgoustinaki, P.D.; Malliaraki, N.; Margioris, A.N. Muscular effects of vitamin D in young athletes and non-athletes and in the elderly. Hormones 2016, 15, 471–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Książek, A.; Zagrodna, A.; Słowińska-Lisowska, M. Vitamin D, Skeletal Muscle Function and Athletic Performance in Athletes-A Narrative Review. Nutrients 2019, 11, 1800. [Google Scholar] [CrossRef] [Green Version]
- Lips, P. Worldwide status of vitamin D nutrition. J. Steroid Biochem. Mol. Biol. 2010, 121, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef] [Green Version]
- Ayadi, I.D.; Nouaili, E.B.; Talbi, E.; Ghdemssi, A.; Rached, C.; Bahlous, A.; Gammoudi, A.; Ben Hamouda, S.; Bouguerra, B.; Bouzid, K.; et al. Prevalence of vitamin D deficiency in mothers and their newborns in a Tunisian population. Int. J. Gynecol. Obstet. 2016, 133, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Feleke, Y.; Abdulkadir, J.; Mshana, R.; Mekbib, T.A.; Brunvand, L.; Berg, J.P.; Falch, J.A. Low levels of serum calcidiol in an African population compared to a North European population. Eur. J. Endocrinol. 1999, 141, 358–360. [Google Scholar] [CrossRef] [PubMed]
- El Maghraoui, A.; Ouzzif, Z.; Mounach, A.; Rezqi, A.; Achemlal, L.; Bezza, A.; Tellal, S.; Dehhaoui, M.; Ghozlani, I. Hypovitaminosis D and prevalent asymptomatic vertebral fractures in Moroccan postmenopausal women. BMC Womens Health 2012, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Botros, R.M.; Sabry, I.M.; Abdelbaky, R.S.; Eid, Y.M.; Nasr, M.S.; Hendawy, L.M. Vitamin D deficiency among healthy Egyptian females. Endocrinol. Nutr. 2015, 62, 314–321. [Google Scholar] [CrossRef]
- Arabi, A.; El Rassi, R.; Fuleihan, G.E.-H. Hypovitaminosis D in developing countries—Prevalence, risk factors and outcomes. Nat. Rev. Endocrinol. 2010, 6, 550–561. [Google Scholar] [CrossRef]
- Fraser, W.D.; Milan, A.M. Vitamin D Assays: Past and Present Debates, Difficulties, and Developments. Calcif. Tissue Int. 2013, 92, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Pourshahidi, L.K. Vitamin D and obesity: Current perspectives and future directions. Proc. Nutr. Soc. 2014, 74, 115–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gröber, U.; Kisters, K. Influence of drugs on vitamin D and calcium metabolism. Derm. Endocrinol. 2012, 4, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borel, P.; Caillaud, D.; Cano, N.J. Vitamin D Bioavailability: State of the Art. Crit. Rev. Food Sci. Nutr. 2013, 55, 1193–1205. [Google Scholar] [CrossRef] [PubMed]
- Ben-Porat, T.; Weiss, R.; Sherf-Dagan, S.; Nabulsi, N.; Maayani, A.; Khalaileh, A.; Abed, S.; Brodie, R.; Harari, R.; Mintz, Y.; et al. Nutritional Deficiencies in Patients with Severe Obesity before Bariatric Surgery: What Should Be the Focus During the Preoperative Assessment? J. Acad. Nutr. Diet. 2020, 120, 874–884. [Google Scholar] [CrossRef]
- Schafer, A.L. Vitamin D and intestinal calcium transport after bariatric surgery. J. Steroid Biochem. Mol. Biol. 2017, 173, 202–210. [Google Scholar] [CrossRef]
- Borges, J.L.C.; Miranda, I.S.D.M.; Sarquis, M.M.; Borba, V.; Maeda, S.S.; Lazaretti-Castro, M.; Blinkey, N. Obesity, Bariatric Surgery, and Vitamin D. J. Clin. Densitom. 2018, 21, 157–162. [Google Scholar] [CrossRef]
- Peterson, L.A.; Zeng, X.; Caufield-Noll, C.P.; Schweitzer, M.A.; Magnuson, T.H.; Steele, K.E. Vitamin D status and supplementation before and after bariatric surgery: A comprehensive literature review. Surg. Obes. Relat. Dis. 2016, 12, 693–702. [Google Scholar] [CrossRef]
- Amrein, K.; Venkatesh, B. Vitamin D and the critically ill patient. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 188–193. [Google Scholar] [CrossRef]
- Christopher, K.B. Vitamin D and critical illness outcomes. Curr. Opin. Crit. Care 2016, 22, 332–338. [Google Scholar] [CrossRef]
- Al-Dujaili, E.A.S.; Munir, N.; Iniesta, R.R. Effect of vitamin D supplementation on cardiovascular disease risk factors and exercise performance in healthy participants: A randomized placebo-controlled preliminary study. Ther. Adv. Endocrinol. Metab. 2016, 7, 153–165. [Google Scholar] [CrossRef] [Green Version]
- de La Puente Yagüe, M.; Collado Yurrita, L.; Cuadrado Cenzual, M.A. Role of Vitamin D in Athletes and Their Performance: Current Concepts and New Trends. Nutrients 2020, 12, 579. [Google Scholar] [CrossRef] [Green Version]
- Mehran, N.; Schulz, B.M.; Neri, B.R.; Robertson, W.J.; Limpisvasti, O. Prevalence of Vitamin D Insufficiency in Professional Hockey Players. Orthop. J. Sports Med. 2016, 4, 2325967116677512. [Google Scholar] [CrossRef] [PubMed]
- Engelsen, O. The Relationship between Ultraviolet Radiation Exposure and Vitamin D Status. Nutrients 2010, 2, 482–495. [Google Scholar] [CrossRef] [Green Version]
- Lehtonen-Veromaa, M.; Möttönen, T.; Irjala, K.; Kärkkäinen, M.; Lamberg-Allardt, C.; Hakola, P.; Viikari, J. Vitamin D intake is low and hypovitaminosis D common in healthy 9- to 15-year-old Finnish girls. Eur. J. Clin. Nutr. 1999, 53, 746–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bezuglov, E.; Tikhonova, A.; Zueva, A.; Khaitin, V.; Waśkiewicz, Z.; Gerasimuk, D.; Żebrowska, A.; Rosemann, T.; Nikolaidis, P.; Knechtle, B. Prevalence and Treatment of Vitamin D Deficiency in Young Male Russian Soccer Players in Winter. Nutrients 2019, 11, 2405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrokhyar, F.; Tabasinejad, R.; Dao, D.; Peterson, D.; Ayeni, O.R.; Hadioonzadeh, R.; Bhandari, M. Prevalence of Vitamin D Inadequacy in Athletes: A Systematic-Review and Meta-Analysis. Sports Med. 2014, 45, 365–378. [Google Scholar] [CrossRef]
- Farrokhyar, F.; Sivakumar, G.; Savage, K.; Koziarz, A.; Jamshidi, S.; Ayeni, O.R.; Peterson, D.; Bhandari, M. Effects of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Concentrations and Physical Performance in Athletes: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sports Med. 2017, 47, 2323–2339. [Google Scholar] [CrossRef]
- Lappe, J.; Cullen, D.; Haynatzki, G.; Recker, R.; Ahlf, R.; Thompson, K. Calcium and Vitamin D Supplementation Decreases Incidence of Stress Fractures in Female Navy Recruits. J. Bone Miner. Res. 2008, 23, 741–749. [Google Scholar] [CrossRef]
- Davey, T.; Lanham-New, S.A.; Shaw, A.M.; Hale, B.; Cobley, R.; Berry, J.L.; Roch, M.; Allsopp, A.J.; Fallowfield, J.L. Low serum 25-hydroxyvitamin D is associated with increased risk of stress fracture during Royal Marine recruit training. Osteoporos. Int. 2015, 27, 171–179. [Google Scholar] [CrossRef]
- Richards, T.; Wright, C. British Army recruits with low serum vitamin D take longer to recover from stress fractures. BMJ Mil Health 2020, 166, 240–242. [Google Scholar] [CrossRef]
- Scragg, R.; Holdaway, I.; Jackson, R.; Lim, T. Plasma 25-hydroxyvitamin D3 and its relation to physical activity and other heart disease risk factors in the general population. Ann. Epidemiol. 1992, 2, 697–703. [Google Scholar] [CrossRef]
- Kluczynski, M.A.; LaMonte, M.J.; Mares, J.A.; Wactawski-Wende, J.; Smith, A.W.; Engelman, C.D.; Andrews, C.A.; Snetselaar, L.G.; Sarto, G.E.; Millen, A.E. Duration of Physical Activity and Serum 25-hydroxyvitamin D Status of Postmenopausal Women. Ann. Epidemiol. 2011, 21, 440–449. [Google Scholar] [CrossRef] [Green Version]
- Brock, K.; Cant, R.; Clemson, L.; Mason, R.; Fraser, D. Effects of diet and exercise on plasma vitamin D (25(OH)D) levels in Vietnamese immigrant elderly in Sydney, Australia. J. Steroid Biochem. Mol. Biol. 2007, 103, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Camargo, C.A. Frequency of Leisure-Time Physical Activity and Serum 25-Hydroxyvitamin D Levels in the US Population: Results from the Third National Health and Nutrition Examination Survey. Am. J. Epidemiol. 2008, 168, 577–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.; Cao, Z.-B.; Taniguchi, H.; Tanisawa, K.; Higuchi, M. Effect of an Acute Bout of Endurance Exercise on Serum 25(OH)D Concentrations in Young Adults. J. Clin. Endocrinol. Metab. 2017, 102, 3937–3944. [Google Scholar] [CrossRef] [PubMed]
- Barker, T.; Henriksen, V.T.; Martins, T.B.; Hill, H.R.; Kjeldsberg, C.R.; Schneider, E.D.; Dixon, B.M.; Weaver, L.K. Higher Serum 25-Hydroxyvitamin D Concentrations Associate with a Faster Recovery of Skeletal Muscle Strength after Muscular Injury. Nutrients 2013, 5, 1253–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maïmoun, L.; Manetta, J.; Couret, I.; Dupuy, A.M.; Mariano-Goulart, D.; Micallef, J.P.; Peruchon, E.; Rossi, M. The intensity level of physical exercise and the bone metabolism response. Int. J. Sports Med. 2006, 27, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Maïmoun, L.; Simar, D.; Caillaud, C.; Coste, O.; Barbotte, E.; Peruchon, E.; Rossi, M.; Mariano-Goulart, D. Response of calciotropic hormones and bone turnover to brisk walking according to age and fitness level. J. Sci. Med. Sport 2009, 12, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R. Vitamin D status in Africa is worse than in other continents. Lancet Glob. Health 2020, 8, e20–e21. [Google Scholar] [CrossRef] [Green Version]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Forrest, K.Y.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Schleicher, R.L.; Sternberg, M.R.; Lacher, D.A.; Sempos, C.T.; Looker, A.C.; Durazo-Arvizu, R.A.; Yetley, E.A.; Chaudhary-Webb, M.; Maw, K.L.; Pfeiffer, C.M.; et al. The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases. Am. J. Clin. Nutr. 2016, 104, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [Green Version]
- Hyppönen, E.; Power, C. Hypovitaminosis D in British adults at age 45 y: Nationwide cohort study of dietary and lifestyle predictors. Am. J. Clin. Nutr. 2007, 85, 860–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calame, W.; Street, L.; Hulshof, T. Vitamin D Serum Levels in the UK Population, including a Mathematical Approach to Evaluate the Impact of Vitamin D Fortified Ready-to-Eat Breakfast Cereals: Application of the NDNS Database. Nutrients 2020, 12, 1868. [Google Scholar] [CrossRef]
- Darling, A.L.; Blackbourn, D.J.; Ahmadi, K.R.; Lanham-New, S.A. Very high prevalence of 25-hydroxyvitamin D deficiency in 6433 UK South Asian adults: Analysis of the UK Biobank Cohort. Br. J. Nutr. 2021, 125, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Malacova, E.; Cheang, P.; Dunlop, E.; Sherriff, J.L.; Lucas, R.M.; Daly, R.M.; Nowson, C.A.; Black, L.J. Prevalence and predictors of vitamin D deficiency in a nationally representative sample of adults participating in the 2011–2013 Australian Health Survey. Br. J. Nutr. 2019, 121, 894–904. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Stoecklin, E.; Eggersdorfer, M. A glimpse of vitamin D status in Mainland China. Nutrition 2013, 29, 953–957. [Google Scholar] [CrossRef]
- Wheeler, B.J.; Snoddy, A.M.E.; Munns, C.; Simm, P.; Siafarikas, A.; Jefferies, C. A Brief History of Nutritional Rickets. Front. Endocrinol. 2019, 10, 795. [Google Scholar] [CrossRef]
- Minisola, S.; Colangelo, L.; Pepe, J.; Diacinti, D.; Cipriani, C.; Rao, S.D. Osteomalacia and Vitamin D Status: A Clinical Update 2020. JBMR Plus 2021, 5, e10447. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Antonio, L. Nutritional rickets: Historic overview and plan for worldwide eradication. J. Steroid Biochem. Mol. Biol. 2020, 198, 105563. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Pacaud, D.; Petryk, A.; Collett-Solberg, P.F.; Kappy, M. Vitamin D Deficiency in Children and Its Management: Review of Current Knowledge and Recommendations. Pediatrics 2008, 122, 398–417. [Google Scholar] [CrossRef] [Green Version]
- Balk, E.M.; Adam, G.P.; Langberg, V.N.; Earley, A.; Clark, P.; Ebeling, P.R.; Mithal, A.; Rizzoli, R.; Zerbini, C.A.F.; Pierroz, D.D.; et al. Global dietary calcium intake among adults: A systematic review. Osteoporos. Int. 2017, 28, 3315–3324. [Google Scholar] [CrossRef] [Green Version]
- Bhan, A.; Qiu, S.; Rao, S.D. Bone histomorphometry in the evaluation of osteomalacia. Bone Rep. 2018, 8, 125–134. [Google Scholar] [CrossRef]
- Fukumoto, S.; Ozono, K.; Michigami, T.; Minagawa, M.; Okazaki, R.; Sugimoto, T.; Takeuchi, Y.; Matsumoto, T. Pathogenesis and diagnostic criteria for rickets and osteomalacia—Proposal by an expert panel supported by the Ministry of Health, Labour and Welfare, Japan, the Japanese Society for Bone and Mineral Research, and the Japan Endocrine Society. J. Bone Miner. Metab. 2015, 33, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Potts, J.T., Jr. A short history of parathyroid hormone, its biological role, and pathophysiology of hormone excess. J. Clin. Densitom. 2013, 16, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Resurrection of vitamin D deficiency and rickets. J. Clin. Investig. 2006, 116, 2062–2072. [Google Scholar] [CrossRef] [Green Version]
- Rabelink, N.M.; Westgeest, H.M.; Bravenboer, N.; Jacobs, M.A.J.M.; Lips, P. Bone pain and extremely low bone mineral density due to severe vitamin D deficiency in celiac disease. Arch. Osteoporos. 2011, 6, 209–213. [Google Scholar] [CrossRef] [Green Version]
- Visser, M.; Deeg, D.J.H.; Lips, P. Low Vitamin D and High Parathyroid Hormone Levels as Determinants of Loss of Muscle Strength and Muscle Mass (Sarcopenia): The Longitudinal Aging Study Amsterdam. J. Clin. Endocrinol. Metab. 2003, 88, 5766–5772. [Google Scholar] [CrossRef]
- Rokan, Z.; Kealey, W.D. Osteomalacia: A forgotten cause of fractures in the elderly. Case Rep. 2015, bcr2014207184. [Google Scholar] [CrossRef] [Green Version]
- Remelli, F.; Vitali, A.; Zurlo, A.; Volpato, S. Vitamin D Deficiency and Sarcopenia in Older Persons. Nutrients 2019, 11, 2861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhan, A.; Rao, A.D.; Rao, D.S. Osteomalacia as a Result of Vitamin D Deficiency. Endocrinol. Metab. Clin. N. Am. 2010, 39, 321–331. [Google Scholar] [CrossRef]
- Häuser, W.; Perrot, S.; Sommer, C.; Shir, Y.; Fitzcharles, M.-A. Diagnostic confounders of chronic widespread pain: Not always fibromyalgia. Pain Rep. 2017, 2, e598. [Google Scholar] [CrossRef]
- Priemel, M.; von Domarus, C.; Klatte, T.O.; Kessler, S.; Schlie, J.; Meier, S.; Proksch, N.; Pastor, F.; Netter, C.; Streichert, T.; et al. Bone mineralization defects and vitamin D deficiency: Histomorphometric analysis of iliac crest bone biopsies and circulating 25-hydroxyvitamin D in 675 patients. J. Bone Miner. Res. 2009, 25, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Alamoudi, L.H.; Almuteeri, R.Z.; Al-Otaibi, M.E.; Alshaer, D.A.; Fatani, S.K.; Alghamdi, M.M.; Safdar, O.Y. Awareness of Vitamin D Deficiency among the General Population in Jeddah, Saudi Arabia. J. Nutr. Metab. 2019, 2019, 4138187. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. A Call to Action: Pregnant Women In-Deed Require Vitamin D Supplementation for Better Health Outcomes. J. Clin. Endocrinol. Metab. 2018, 104, 13–15. [Google Scholar] [CrossRef]
- Wagner, C.L.; Hollis, B.W. Early-Life Effects of Vitamin D: A Focus on Pregnancy and Lactation. Ann. Nutr. Metab. 2020, 76, 16–28. [Google Scholar] [CrossRef]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Hyppönen, E.; Berry, J.; Vieth, R.; et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef] [Green Version]
- Tripkovic, L.; Wilson, L.R.; Hart, K.; Johnsen, S.; de Lusignan, S.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Elliott, R.; et al. Daily supplementation with 15 mug vitamin D2 compared with vitamin D3 to increase wintertime 25-hydroxyvitamin D status in healthy South Asian and white European women: A 12-wk randomized, placebo-controlled food-fortification trial. Am. J. Clin. Nutr. 2017, 106, 481–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieth, R. Critique of the Considerations for Establishing the Tolerable Upper Intake Level for Vitamin D: Critical Need for Revision Upwards. J. Nutr. 2006, 136, 1117–1122. [Google Scholar] [CrossRef] [Green Version]
- Heaney, R.P.; Davies, K.M.; Chen, T.C.; Holick, M.F.; Barger-Lux, M.J. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am. J. Clin. Nutr. 2003, 77, 204–210. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, J.C.; Smith, L.M.; Yalamanchili, V. Incidence of hypercalciuria and hypercalcemia during vitamin D and calcium supplementation in older women. Menopause 2014, 21, 1173–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, S.S.; Dawson-Hughes, B. Plasma vitamin D and 25OHD responses of young and old men to supplementation with vitamin D3. J. Am. Coll. Nutr. 2002, 21, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Hill, T.R.; Lucey, A.J.; Taylor, N.; Seamans, K.M.; Muldowney, S.; Fitzgerald, A.P.; Flynn, A.; Barnes, M.S.; Horigan, G.; et al. Estimation of the dietary requirement for vitamin D in healthy adults. Am. J. Clin. Nutr. 2008, 88, 1535–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cashman, K.D.; Wallace, J.M.; Horigan, G.; Hill, T.R.; Barnes, M.S.; Lucey, A.J.; Bonham, M.P.; Taylor, N.; Duffy, E.M.; Seamans, K.; et al. Estimation of the dietary requirement for vitamin D in free-living adults ≥64 y of age. Am. J. Clin. Nutr. 2009, 89, 1366–1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ish-Shalom, S.; Segal, E.; Salganik, T.; Raz, B.; Bromberg, I.L.; Vieth, R. Comparison of Daily, Weekly, and Monthly Vitamin D3 in Ethanol Dosing Protocols for Two Months in Elderly Hip Fracture Patients. J. Clin. Endocrinol. Metab. 2008, 93, 3430–3435. [Google Scholar] [CrossRef] [Green Version]
- Dawson-Hughes, B.; Heaney, R.P.; Holick, M.F.; Lips, P.; Meunier, P.J.; Vieth, R. Estimates of optimal vitamin D status. Osteoporos. Int. 2005, 16, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Basha, B.; Rao, D.; Han, Z.-H.; Parfitt, A. Osteomalacia due to vitamin D depletion: A neglected consequence of intestinal malabsorption. Am. J. Med. 2000, 108, 296–300. [Google Scholar] [CrossRef]
- Heaney, R.P.; Horst, R.L.; Cullen, D.M.; Armas, L.A. Vitamin D3 distribution and status in the body. J. Am. Coll. Nutr. 2009, 28, 252–256. [Google Scholar] [CrossRef]
- Hollis, B.W. Comparison of equilibrium and disequilibrium assay conditions for ergocalciferol, cholecalciferol and their major metabolites. J. Steroid Biochem. 1984, 21, 81–86. [Google Scholar] [CrossRef]
- Christakos, S.; Ajibade, D.V.; Dhawan, P.; Fechner, A.J.; Mady, L.J. Vitamin D: Metabolism. Rheum. Dis. Clin. N. Am. 2012, 38, 1–11. [Google Scholar] [CrossRef]
- Minisola, S.; Cianferotti, L.; Biondi, P.; Cipriani, C.; Fossi, C.; Franceschelli, F.; Giusti, F.; Leoncini, G.; Pepe, J.; Bischoff-Ferrari, H.A.; et al. Correction of vitamin D status by calcidiol: Pharmacokinetic profile, safety, and biochemical effects on bone and mineral metabolism of daily and weekly dosage regimens. Osteoporos. Int. 2017, 28, 3239–3249. [Google Scholar] [CrossRef] [PubMed]
- Michaud, J.; Naud, J.; Ouimet, D.; Demers, C.; Petit, J.-L.; Leblond, F.A.; Bonnardeaux, A.; Gascon-Barré, M.; Pichette, V. Reduced Hepatic Synthesis of Calcidiol in Uremia. J. Am. Soc. Nephrol. 2010, 21, 1488–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrado, A.; Rotondo, C.; Cici, D.; Berardi, S.; Cantatore, F.P. Effects of Different Vitamin D Supplementation Schemes in Post-Menopausal Women: A Monocentric Open-Label Randomized Study. Nutrients 2021, 13, 380. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, C.; Baroni, M.; Bini, V.; Brozzetti, A.; Parretti, L.; Zengarini, E.; Lapenna, M.; Antinolfi, P.; Falorni, A.; Mecocci, P.; et al. Effects of Weekly Supplementation of Cholecalciferol and Calcifediol Among the Oldest-Old People: Findings From a Randomized Pragmatic Clinical Trial. Nutrients 2019, 11, 2778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaes, A.M.; Tieland, M.; de Regt, M.F.; Wittwer, J.; van Loon, L.J.; de Groot, L.C. Dose-response effects of supplementation with calcifediol on serum 25-hydroxyvitamin D status and its metabolites: A randomized controlled trial in older adults. Clin. Nutr. 2018, 37, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Shieh, A.; Ma, C.; Chun, R.F.; Witzel, S.; Rafison, B.; Contreras, H.T.M.; Wittwer-Schegg, J.; Swinkels, L.; Huijs, T.; Hewison, M.; et al. Effects of Cholecalciferol vs. Calcifediol on Total and Free 25-Hydroxyvitamin D and Parathyroid Hormone. J. Clin. Endocrinol. Metab. 2017, 102, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Orav, E.J.; Staehelin, H.B.; Meyer, O.W.; Theiler, R.; Dick, W.; Willett, W.C.; Egli, A. Monthly High-Dose Vitamin D Treatment for the Prevention of Functional Decline: A Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 175–183. [Google Scholar] [CrossRef]
- Navarro-Valverde, C.; Sosa-Henríquez, M.; Alhambra-Expósito, M.R.; Quesada-Gómez, J.M. Vitamin D3 and calcidiol are not equipotent. J. Steroid Biochem. Mol. Biol. 2016, 164, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Meyer, O.; Dawson-Hughes, B.; Sidelnikov, E.; Egli, A.; Grob, D.; Staehelin, H.B.; Theiler, G.; Kressig, R.W.; Simmen, H.P.; Theiler, R.; et al. Calcifediol versus vitamin D3 effects on gait speed and trunk sway in young postmenopausal women: A double-blind randomized controlled trial. Osteoporos. Int. 2015, 26, 373–381. [Google Scholar] [CrossRef]
- Catalano, A.; Morabito, N.; Basile, G.; Cucinotta, M.; Lasco, A. Calcifediol improves lipid profile in osteopenicatorvastatin-treated postmenopausal women. Eur. J. Clin. Investig. 2015, 45, 144–149. [Google Scholar] [CrossRef]
- Jetter, A.; Egli, A.; Dawson-Hughes, B.; Staehelin, H.B.; Stoecklin, E.; Goessl, R.; Henschkowski, J.; Bischoff-Ferrari, H.A. Pharmacokinetics of oral vitamin D3 and calcifediol. Bone 2014, 59, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Stöcklin, E.; Sidelnikov, E.; Willett, W.C.; Edel, J.O.; Stähelin, H.B.; Wolfram, S.; Jetter, A.; Schwager, J.; et al. Oral supplementation with 25(OH)D3 versus vitamin D3: Effects on 25(OH)D levels, lower extremity function, blood pressure, and markers of innate immunity. J. Bone Miner. Res. 2012, 27, 160–169. [Google Scholar] [CrossRef]
- Cashman, K.D.; Seamans, K.M.; Lucey, A.J.; Stöcklin, E.; Weber, P.; Kiely, M.; Hill, T.R. Relative effectiveness of oral 25-hydroxyvitamin D3 and vitamin D3 in raising wintertime serum 25-hydroxyvitamin D in older adults. Am. J. Clin. Nutr. 2012, 95, 1350–1356. [Google Scholar] [CrossRef] [Green Version]
- Barger-Lux, M.J.; Heaney, R.P.; Dowell, S.; Chen, T.C.; Holick, M.F. Vitamin D and its Major Metabolites: Serum Levels after Graded Oral Dosing in Healthy Men. Osteoporos. Int. 1998, 8, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Stamp, T.; Haddad, J.; Twigg, C. Comparison of oral 25-hydroxycholecalciferol, vitamin D, and ultraviolet light as determinants of circulating 25-hydroxyvitamin D. Lancet 1977, 309, 1341–1343. [Google Scholar] [CrossRef]
- Rossini, M.; Viapiana, O.; Gatti, D.; James, G.; Girardello, S.; Adami, S. The long term correction of vitamin D deficiency: Comparison between different treatments with vitamin D in clinical practice. Minerva Med. 2005, 96, 1–7. [Google Scholar]
- Cipriani, C.; Romagnoli, E.; Pepe, J.; Russo, S.; Carlucci, L.; Piemonte, S.; Nieddu, L.; McMahon, N.J.; Singh, R.; Minisola, S. Long-Term Bioavailability After a Single Oral or Intramuscular Administration of 600,000 IU of Ergocalciferol or Cholecalciferol: Implications for Treatment and Prophylaxis. J. Clin. Endocrinol. Metab. 2013, 98, 2709–2715. [Google Scholar] [CrossRef] [Green Version]
- Bischoff-Ferrari, H.A.; Shao, A.; Dawson-Hughes, B.; Hathcock, J.; Giovannucci, E.; Willett, W.C. Benefit—Risk assessment of vitamin D supplementation. Osteoporos. Int. 2009, 21, 1121–1132. [Google Scholar] [CrossRef] [Green Version]
- Rossini, M.; Adami, S.; Viapiana, O.; Fracassi, E.; Idolazzi, L.; Povino, M.R.; Gatti, D. Dose-Dependent Short-Term Effects of Single High Doses of Oral Vitamin D3 on Bone Turnover Markers. Calcif. Tissue Int. 2012, 91, 365–369. [Google Scholar] [CrossRef]
- Rossini, M.; Gatti, D.; Viapiana, O.; Fracassi, E.; Idolazzi, L.; Zanoni, S.; Adami, S. Short-Term Effects on Bone Turnover Markers of a Single High Dose of Oral Vitamin D3. J. Clin. Endocrinol. Metab. 2012, 97, E622–E626. [Google Scholar] [CrossRef] [Green Version]
- Levine, M.A. Diagnosis and Management of Vitamin D Dependent Rickets. Front. Pediatr. 2020, 8, 315. [Google Scholar] [CrossRef]
- Bertoli, M.; Luisetto, G.; Ruffatti, A.; Urso, M.; Romagnoli, G. Renal function during calcitriol therapy in chronic renal failure. Clin. Nephrol. 1990, 33, 98–102. [Google Scholar] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Hossein-Nezhad, A.; Holick, M.F. Vitamin D for Health: A Global Perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, A.R.; Kift, R.; Berry, J.L.; Rhodes, L.E. The Vitamin D Debate: Translating Controlled Experiments into Reality for Human Sun Exposure Times. Photochem. Photobiol. 2011, 87, 741–745. [Google Scholar] [CrossRef]
- Dudenkov, D.V.; Yawn, B.P.; Oberhelman, S.S.; Fischer, P.R.; Singh, R.J.; Cha, S.S.; Maxson, J.A.; Quigg, S.M.; Thacher, T.D. Changing Incidence of Serum 25-Hydroxyvitamin D Values Above 50 ng/mL: A 10-Year Population-Based Study. Mayo Clin. Proc. 2015, 90, 577–586. [Google Scholar] [CrossRef] [Green Version]
- Genzen, J.R.; Gosselin, J.T.; Wilson, T.C.; Racila, E.; Krasowski, M.D. Analysis of vitamin D status at two academic medical centers and a national reference laboratory: Result patterns vary by age, gender, season, and patient location. BMC Endocr. Disord. 2013, 13, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.H.; Majid, H.; Iqbal, R. Shifting of vitamin D deficiency to hypervitaminosis and toxicity. J. Coll. Physicians Surg. Pak. 2014, 24, 536. [Google Scholar] [PubMed]
- Spiller, H.A.; Good, T.F.; Spiller, N.E.; Aleguas, A. Vitamin D exposures reported to US poison centers 2000-2014: Temporal trends and outcomes. Hum. Exp. Toxicol. 2016, 35, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J.; Gallagher, J.C. The 2011 IOM Report on Vitamin D and Calcium Requirements for North America: Clinical Implications for Providers Treating Patients with Low Bone Mineral Density. J. Clin. Densitom. 2011, 14, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Khaw, K.T.; Toop, L.; Sluyter, J.; Lawes, C.M.; Waayer, D.; Giovannucci, E.; Camargo, C.A., Jr. Effect of monthly high-dose vitamin D supplementation on falls and non-vertebral fractures: Secondary and post-hoc outcomes from the randomised, double-blind, placebo-controlled ViDA trial. Lancet Diabetes Endocrinol. 2017, 5, 438–447. [Google Scholar]
- Burt, L.A.; Billington, E.O.; Rose, M.S.; Raymond, D.A.; Hanley, D.A.; Boyd, S.K. Effect of High-Dose Vitamin D Supplementation on Volumetric Bone Density and Bone Strength: A Randomized Clinical Trial. JAMA 2019, 322, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.M.; Gallagher, J.C.; Suiter, C. Medium doses of daily vitamin D decrease falls and higher doses of daily vitamin D3 increase falls: A randomized clinical trial. J. Steroid Biochem. Mol. Biol. 2017, 173, 317–322. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Food | mcg per Serving | IU per Serving |
|---|---|---|
| Cod liver oil, 1 tablespoon | 34.0 | 1360 |
| Trout (rainbow), cooked, 3 ounces | 16.2 | 645 |
| Salmon (sockeye), cooked, 3 ounces | 14.2 | 570 |
| Mushrooms, raw, exposed to UV light, ½ cup | 9.2 | 366 |
| Sardines, canned in oil, drained, 2 sardines | 1.2 | 46 |
| Egg, 1 large, scrambled * | 1.1 | 44 |
| Liver, beef, braised, 3 ounces | 1.0 | 42 |
| Tuna fish, canned in water, drained, 3 ounces | 1.0 | 40 |
| Cheese, cheddar, 1 ounce | 0.3 | 12 |
| Mushrooms, portabella, raw, diced, ½ cup | 0.1 | 4 |
| Chicken breast, roasted, 3 ounces | 0.1 | 4 |
| Beef, ground, 90% lean, broiled, 3 ounces | traces | 1.7 |
| Broccoli, raw, chopped, ½ cup | 0 | 0 |
| Carrots, raw, chopped, ½ cup | 0 | 0 |
| Almonds, dry roasted, 1 ounce | 0 | 0 |
| Apple, large | 0 | 0 |
| Banana, large | 0 | 0 |
| Rice, brown, long-grain, cooked, 1 cup | 0 | 0 |
| Whole wheat bread, 1 slice | 0 | 0 |
| Lentils, boiled, ½ cup | 0 | 0 |
| Sunflower seeds, roasted, ½ cup | 0 | 0 |
| Edamame, shelled, cooked, ½ cup | 0 | 0 |
| Fortified Foods | ||
| Milk, 2% milkfat, vitamin D fortified, 1 cup | 2.9 | 120 |
| Soy, almond, and oat milks, vitamin D fortified, various brands, 1 cup | 2.5–3.6 | 100–144 |
|
|
| 25(OH)D ng/mL | NAM/NIH | ES | NOS | SACN | AGS * | ESE |
|---|---|---|---|---|---|---|
| <10 | deficiency | deficiency | deficiency | deficiency | deficiency | deficiency |
| 10–20 | inadequacy risk | deficiency | inadequacy risk | sufficient | deficiency | deficiency |
| 20–30 | sufficiency | insufficiency | sufficiency | sufficient | deficiency risk | insufficiency |
| 30–50 | sufficiency | desirable concentration | sufficiency | sufficient | minimal acceptable concentration | sufficiency |
| 50–100 | possible excess adverse events | desirable concentration | possible onset of toxicity | |||
| 100–150 | possible excess adverse events | possible onset of toxicity | ||||
| >150 | toxicity |
| 25(OH)D ng/mL | NAM/NIH | ES | NOS | SACN-PHE | AGS 4 |
|---|---|---|---|---|---|
| Initial Dose 1—Maintenance 2 | Initial Dose 3—Maintenance 2 | ||||
| <10 | 600 IU 5 | 400,000 IU 1500–2000 IU 6,7 | 300,000 IU 800–2000 IU | – | 4000 IU 11 |
| 10–20 | 600 IU 5 | 400,000 IU 1500–2000 IU 6,7 | 400 IU | 400 IU 10 | 4000 IU 11 |
| 20–30 | 600 IU 5 | 1500–2000 IU 6,8,9 | 400 IU | 400 IU 10 | 4000 IU 11 |
| 30–50 | 600 IU 5 | 1500–2000 IU 8,9 | 400 IU | 400 IU 10 | 4000 IU 11 |
| 50–100 | – | 1500–2000 IU 8,9 | – | – | – |
| >100 | – | – | – | – | – |
| Ergocalciferol | Cholecalciferol | Calcifediol (or Calcidiol) | Calcitriol | |
|---|---|---|---|---|
| Chemical Structure |  |  |  |  |
| Absorption | Intestine (bile required) | Intestine (bile required) | Intestine, readily absorbed * | Intestine, readily absorbed * |
| DBP dissociation constant | 10−7 | 10−7 | 10−9 | 10−7 |
| Volume of distribution | very limited in plasma compartment; rapidly stored in fat tissue | very limited in plasma compartment; rapidly stored in fat tissue | larger than plasma volume | plasma compartment |
| Tissue distribution for long-term | adipose tissue, muscle | adipose tissue, muscle | blood, adipose tissue, muscle | blood and tissues |
| Circulating half-life | 2 days | 2 days | 3 weeks | 4–8 h |
| Functional half-life | 2–3 months | ≤2 months | 2–3 months | 4–8 h |
| Authors/Country | Year | Number and Type of Participants | Study Design | Cholecalciferol/Calcifediol Dose | Duration | Summary of Results |
|---|---|---|---|---|---|---|
| Corrado et al. Italy [165] | 2021 | 107 postmenopausal women (mean age 60.8 ± 6.5 y) | Open-label RCT | –cholecalciferol: 100,000 IU single dose or 100,000 IU/month or 7000 IU/week –calcifediol: 7000 IU/week | 6 months | Weekly calcifediol and cholecalciferol induced a greater and faster increase of serum 25(OH)D vs. monthly or single-dose cholecalciferol administration; 25(OH)D increase was associated with improved lower limbs muscle function. Supplementation with calcifediol was more effective and faster vs. cholecalciferol in increasing 25(OH)D serum levels and was associated with a greater improvement of muscular function. |
| Ruggiero et al. Italy [166] | 2019 | 67 community-dwelling women and men, aged >75 y | Open-label RCT | –calcifediol: 150 μg/week –cholecalciferol: 150 μg/week | 7 months | Supplementation with calcifediol and cholecalciferol were associated with significant increasing serum levels of 25(OH)D and 1,25(OH)2D in oldest–old persons, with a steeper rise and faster recovery of acceptable iPTH levels for those on calcifediol; after adjustment for iPTH levels the differences disappeared. Both supplementations were associated with a decreasing trend of iPTH and CRP. Polypharmacy and low muscle strength weaken the recovery of adequate 25(OH)D serum levels. |
| Vaes et al. Netherlands [167] | 2018 | 59 men and women aged >65 y | Double-blind RCT | –calcifediol: 5, 10 or 15 μg/day –cholecalciferol: 20 μg/day | 24 weeks | Supplementation with 20 μg/day of cholecalciferol increased 25(OH)D3 concentrations towards 28 ng/mL within 16 weeks. Supplementation with 10 or 15 μg/day of calcifediol increased 25(OH)D3 levels >28 ng/mL/L in 8 and 4 weeks, respectively. Steady state was achieved from week 12 onwards with serum 25(OH)D3 levels stabilizing between 84 and 89 nmol/L (33.6 and 35.6 ng/mL) in the 10 μg/day calcifediol group. No cases of hypercalcemia occurred in any treatment during the study period. |
| Shieh et al. USA [168] | 2017 | 35 aged ≥18 y with 25(OH)D <20 ng/mL, from a multiethnic cohort | Open-label RCT | –calcifediol: 20 μg/day –cholecalciferol: 60 μg/day | 16 weeks | Significant higher and faster increment of total and free 25(OH)D with calcifediol vs. cholecaciferol (total: +25.5 vs. +13.8 ng/mL; free: +6.6 vs. +3.5 pg/mL). By 4 weeks, 87.5% of calcifediol treated participants had total 25(OH)D levels ≥30 ng/mL, vs. 23.1% of cholecalciferol treated participants. Conclusions: calcifediol increased total and free 25(OH)D levels more rapidly than cholecalciferol, regardless of race/ethnicity. Free and total 25(OH)D were similarly associated with change in PTH. |
| Bischoff-Ferrari et al. Switzerland [169] | 2016 | 200 community-dwelling men and women (67%) aged ≥70 y with a prior fall; 58% were vitamin D deficient (<20 ng/mL) at baseline | Double-blind RCT | –Group 1: cholecalciferol 24,000 IU/month –Group 2: cholecalciferol 60,000 IU/month –Group 3: cholecalciferol 24,000 IU/month plus calcifediol 300 μg/month | 12 months | Participants in Group 3 vs. Group 1 were significantly more likely to achieve 25(OH)D levels of at least 30 ng/mL. Lower extremity function did not differ among the treatment groups. The incidence of falls was higher for Groups 2 and 3 vs. Group 1. |
| Navarro-Valverde et al. Spain [170] | 2016 | 40 post-menopausal women (in 4 groups), mean age 67 ± y, deficient in vitamin D [mean 25(OH)D <15 ng/mL] | Open-label RCT | –Group 1: cholecalciferol 20 μg/day –Group 2: calcifediol 20 μg/day –Group 3: calcifediol 0.266 μg/week –Group 4: calcifediol 0.266 μg/two weeks | 12 months | Calcifediol was significantly faster and 3–6 times more potent to obtain serum levels of 25(OH)D in the medium to long term. The authors concluded that both metabolites are not equipotent and that the therapeutic prescription guidelines should consider the differences to avoid over-dosage of calcifediol. |
| Meyer et al. Switzerland [171] | 2015 | 20 post-menopausal women, mean age 61.5 ± 7.2 y, 25(OH)D between 8 and 24 ng/mL [mean 25(OH)D 13.2 ng/mL] | Double-blind RCT | –calcifediol: 20 μg/day –cholecalciferol: 20 μg/day | 4 months | Increase in 25(OH)D levels was significantly higher in the calcifediol group vs. cholecalciferol group (to a mean of 69.3 ± 9.5 ng/mL vs. 30.5 ± 5.0 ng/mL, respectively). Calcifediol vs. cholecalciferol improved gait speed by 18% among these young postmenopausal women, after adjustments for baseline gait speed, age, and BMI. Changes in 25(OH)D blood levels over time were significantly correlated with improvement in gait speed. No effect could be demonstrated for trunk sway. |
| Catalano et al. Italy [172] | 2015 | 57 postmenopausal women at low risk of fracture, on atorvastatin treatment, mean age 59 ± 6.7 y, 25(OH)D <30 ng/mL [mean 25(OH)D 13.2 ng/mL] | Open-label RCT | –calcifediol: 140 μg/week –cholecalciferol: 140 μg/week | 24 weeks | 25(OH)D increased significantly in both groups with higher levels in participants receiving calcifediol vs. cholecalciferol. Only in the calcifediol group, a significant reduction of LDL-C and an increase of HDL-C were observed, after adjustment for age, and baseline BMI, 25(OH)D and lipid levels. The percent changes in 25(OH)D levels were significantly associated with the variations of LDL-C but not with HDL-C levels. |
| Jetter et al. Switzerland [173] | 2014 | 35 healthy females aged 50–70 y, 25(OH)D between 8 and 24 ng/mL | Double-blind RCT | –calcifediol: 20 μg/day or 140 μg/week or both for 15 weeks or a single bolus of 140 μg –cholecalciferol: 20 μg/day or 140 μg/week or both for 15 weeks or a single bolus of 140 μg –calcifediol single bolus of 140 μg plus cholecalciferol single bolus of 140 μg | 15 weeks or single bolus | All women in the daily and weekly calcifediol groups achieved 25(OH)D3 concentrations >30 ng/mL (mean, 16.8 days), but only 70% in the cholecalciferol daily or weekly groups reached this concentration (mean, 68.4 days). A single dose of 140 μg calcifediol led to 117% higher 25(OH)D3 AUC0-96h values than 140 μg vitamin D3, while the simultaneous intake of both did not further increase exposure. The authors concluded that calcifediol given daily, weekly, or as a single bolus is about 2–3 times more potent in increasing plasma 25(OH)D3 concentrations vs. cholecalciferol, and concentrations of 30 ng/mL were reached more rapidly with calcifediol. |
| Bischoff-Ferrari et al. Switzerland [174] | 2012 | 20 healthy postmenopausal women, with a mean 25(OH)D level of 13.2 ± 3.9 ng/mL and a mean age of 61.5 ± 7.2 y | Double-blind RCT | –calcifediol: 20 μg/day –cholecalciferol: 20 μg/day | 4 months | Mean 25(OH)D levels increased rapidly to 69.5 ng/mL in the calcifediol group and to 31.0 ng/mL with a slow increase in the cholecalciferol group. All analyses were adjusted for baseline measurement, age, and BMI. Therapy with calcifediol vs. cholecalciferol had a significant 2.8-fold increased odds of maintained or improved lower extremity function, and a 5.7-mmHg significant decrease in SBP. Both types of vitamin D contributed to a decrease in five out of seven markers of innate immunity, significantly more pronounced with calcifediol for eotaxin, IL-12, MCP-1, and MIP-1 beta. There were no cases of hypercalcemia at any time point. |
| Cashman et al. Ireland [175] | 2012 | 56 healthy, free-living adults aged ≥50 y | Double-blind RCT | –calcifediol: 7 or 20 μg/day –cholecalciferol: 20 μg/day | 10 weeks | The mean increases (per μg of vitamin D compound) in serum 25(OH)D concentrations were 0.96 ± 0.62, 4.02 ± 1.27, and 4.77 ± 1.04 nmol/L for 20 μg/day of cholecalciferol and 7- and 20 μg/day of calcifediol, respectively. A comparison of the 7- and 20-μg of calcifediol groups with the 20 μg of cholecalciferol group yielded conversion factors of 4.2 and 5, respectively. There was no effect on serum calcium concentrations and no incidence of hypercalcemia. The authors concluded that each μg of calcifediol was about 5 times more effective in raising serum 25(OH)D in older adults in winter than an equivalent amount of cholecalciferol. |
| Rossini et al. Italy [178] | 2005 | 271 postmenopausal women with osteopenia or osteoporosis with hypovitaminosis D | Open-label RCT | –calcifediol: 100 μg/week –cholecalciferol: 20–22 μg/day | 12 months | The compliance to the weekly calcifediol was over 90% and led to serum levels of 25(OH)D, similar to those obtained with daily cholecalciferol. The potency of calcifediol vs. cholecalciferol in increasing 25(OH)D was 1.66 fold, but the study aimed to evaluate compliance, not efficacy. |
| Barger-Lux et al. USA [176] | 1998 | 116 healthy men with usual milk consumption of ≤0.47 L/day, mean age of 28 ± 4 y, mean serum 25(OH)D of 26.8 ± 10 ng/mL from January to April | Open-label RCT | –Cholecalciferol 25, 250 or 1250 μg/day –Calcifediol 10, 20 or 50 μg/day –Calcitriol 0.5, 1.0 or 2.0 μg/day | 8 weeks (group 1) 4 weeks (group 2) 2 weeks (group 3) | In participants treated with cholecalciferol serum 25(OH)D increased by 11.6, 58.4, and 257.2 ng/mL for the three dosage groups, respectively. Treatment with calcifediol increased circulating 25(OH)D by 16, 30.4, and 82.4 ng/mL, respectively. Treatment with calcitriol increased circulating 1,25(OH)2D by 10, 46, and 60 pmol/L, respectively. Slopes calculated from these data allowed the following estimates of mean treatment effects for typical dosage units in healthy 70-kg adults: an 8-week course of cholecalciferol at 10 μg/day would raise serum 25(OH)D by 4.4 ng/mL and a 4-week course of calcifediol at 20 μg/day would raise serum 25(OH)D by 37.6 ng/mL (potency of calcifediol vs. cholecalciferol in increasing 25(OH)D was 3.3–3.5 fold at a low dose and 7–8 fold for the highest dose of both compounds). |
| Stamp et al. UK [177] | 1977 | 200 participants | Clinical practice | 5 years | Ten times more cholecalciferol/ergocalciferol than calcifediol was required to produce equivalent plasma 25(OH)D concentration. The authors conclude that these data indirectly measure the superior therapeutic potency of calcifediol and the possible usefulness in patients with reduced 25-hydroxylation of vitamin D, or reduced solar exposure. Limitations of this study include: inclusion of patients with metabolic bone diseases; lack of homogeneity among the groups; use of ergocalciferol and cholecalciferol interchangeably without separating the results obtained by each of them; differences in duration of treatments of the diverse compounds. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dominguez, L.J.; Farruggia, M.; Veronese, N.; Barbagallo, M. Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment. Metabolites 2021, 11, 255. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11040255
Dominguez LJ, Farruggia M, Veronese N, Barbagallo M. Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment. Metabolites. 2021; 11(4):255. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11040255
Chicago/Turabian StyleDominguez, Ligia J., Mario Farruggia, Nicola Veronese, and Mario Barbagallo. 2021. "Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment" Metabolites 11, no. 4: 255. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11040255