
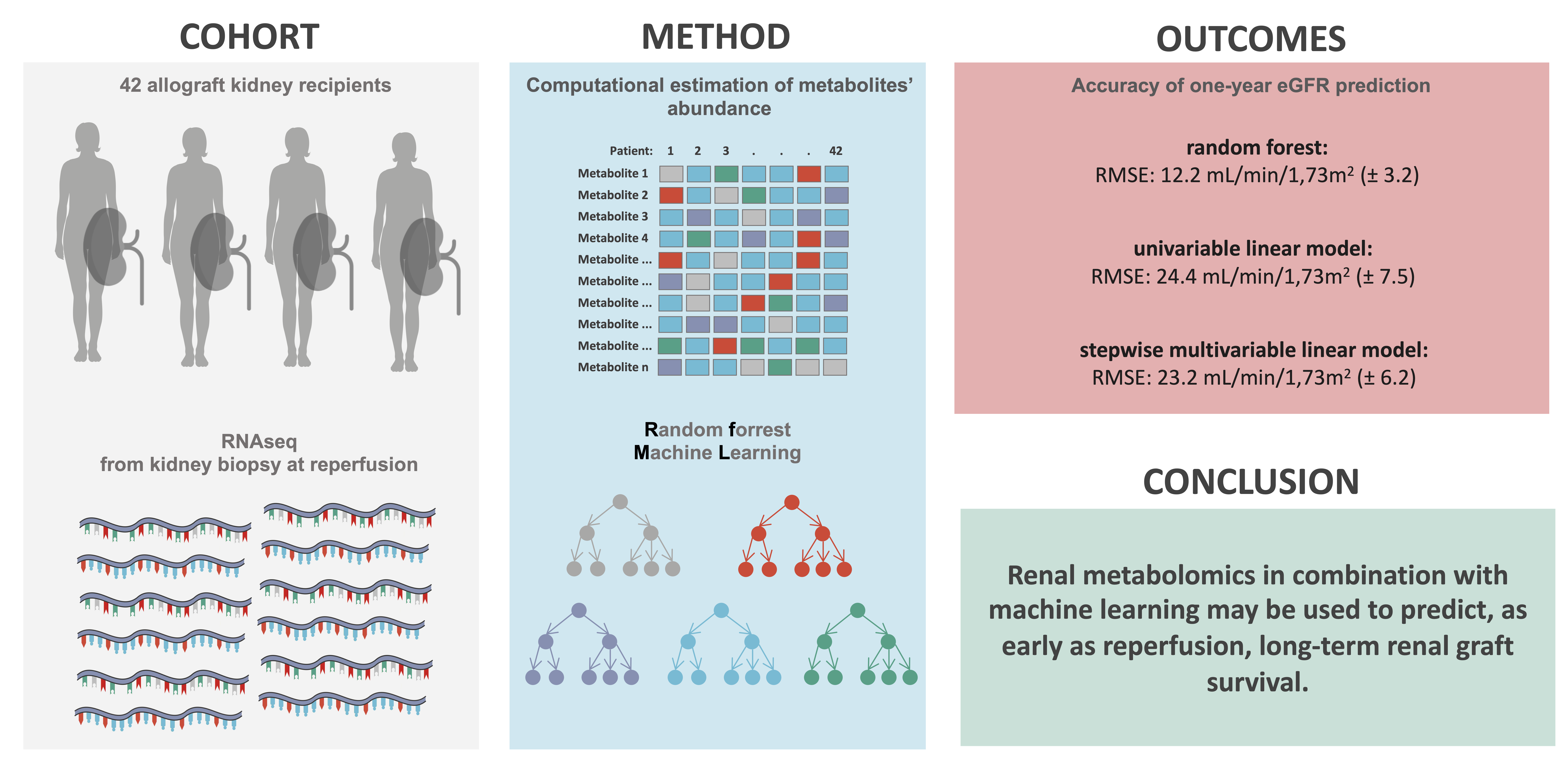
Estimated Renal Metabolomics at Reperfusion Predicts One-Year Kidney Graft Function

 ,
,
Abstract
:
1. Introduction
2. Results
2.1. Description of the Cohort
2.2. Machine Learning on Estimated Metabolomic Predicts One-Year eGFR
2.3. ML Approach Outperforms Classic Statisical Method
3. Discussion
4. Materials and Methods
4.1. Inclusion of Patients
4.2. Estimation of Metabolomics
4.3. Relation between One-Year eGFR and Each Metabolite Abundance Estimation
4.4. Random Forrest Model
- We only kept the final product (i.e., AMP, Dolichyl-phosphate-D-mannose, d-UTMP and Succinate).
- When two metabolites were correlated with a third one, we removed the third to maximize the number of predictors (Arginosuccinate, 3PD and Propanoyl-CoA).
- The number of predictors randomly sampled as candidates for each split (mtry), were the square root and the log2 of the number of predictors, and a sequential vector of integer from 1 to the total number of predictors.
- The minimum sizes of terminal node (nodesize) tried were 2, 4 and 8.
- The numbers of trees to grow tried were 25, 50, 100, 150, 300, 500, 1000 and 2000.
- The optimal model was selected to maximize the RMSE.
4.5. Statistical Models
4.6. TRIPOD Guidelines
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levey, A.S.; Coresh, J.; Greene, T.; Marsh, J.; Stevens, L.A.; Kusek, J.W.; Van Lente, F. Chronic Kidney Disease Epidemiology Collaboration Expressing the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate with Standardized Serum Creatinine Values. Clin. Chem. 2007, 53, 766–772. [Google Scholar] [CrossRef] [Green Version]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. GBD Chronic Kidney Disease Collaboration Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Tonelli, M.; Wiebe, N.; Culleton, B.; House, A.; Rabbat, C.; Fok, M.; McAlister, F.; Garg, A.X. Chronic Kidney Disease and Mortality Risk: A Systematic Review. J. Am. Soc. Nephrol. 2006, 17, 2034–2047. [Google Scholar] [CrossRef] [Green Version]
- Liyanage, T.; Ninomiya, T.; Jha, V.; Neal, B.; Patrice, H.M.; Okpechi, I.; Zhao, M.; Lv, J.; Garg, A.X.; Knight, J.; et al. Worldwide Access to Treatment for End-Stage Kidney Disease: A Systematic Review. Lancet 2015, 385, 1975–1982. [Google Scholar] [CrossRef]
- Abecassis, M.; Bartlett, S.T.; Collins, A.J.; Davis, C.L.; Delmonico, F.L.; Friedewald, J.J.; Hays, R.; Howard, A.; Jones, E.; Leichtman, A.B.; et al. Kidney Transplantation as Primary Therapy for End-Stage Renal Disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) Conference. Clin. J. Am. Soc. Nephrol. 2008, 3, 471–480. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [Green Version]
- Hariharan, S.; Johnson, C.P.; Bresnahan, B.A.; Taranto, S.E.; McIntosh, M.J.; Stablein, D. Improved Graft Survival after Renal Transplantation in the United States, 1988 to 1996. N. Engl. J. Med. 2000, 342, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Hart, A. Global Perspective on Kidney Transplantation: United States. Kidney360 2021, 2, 1836–1839. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Zeier, M.G.; Chapman, J.R.; Craig, J.C.; Ekberg, H.; Garvey, C.A.; Green, M.D.; Jha, V.; Josephson, M.A.; Kiberd, B.A.; et al. KDIGO Clinical Practice Guideline for the Care of Kidney Transplant Recipients: A Summary. Kidney Int. 2010, 77, 299–311. [Google Scholar] [CrossRef] [Green Version]
- Hariharan, S.; Mcbride, M.A.; Cherikh, W.S.; Tolleris, C.B.; Bresnahan, B.A.; Johnson, C.P. Post-Transplant Renal Function in the First Year Predicts Long-Term Kidney Transplant Survival. Kidney Int. 2002, 62, 311–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvadori, M.; Rosati, A.; Bock, A.; Chapman, J.; Dussol, B.; Fritsche, L.; Kliem, V.; Lebranchu, Y.; Oppenheimer, F.; Pohanka, E.; et al. Estimated One-Year Glomerular Filtration Rate Is the Best Predictor of Long-Term Graft Function Following Renal Transplant. Transplantation 2006, 81, 202–206. [Google Scholar] [CrossRef]
- Faivre, A.; Verissimo, T.; Auwerx, H.; Legouis, D.; de Seigneux, S. Tubular Cell Glucose Metabolism Shift during Acute and Chronic Injuries. Front. Med. 2021, 8, 742072. [Google Scholar] [CrossRef]
- Legouis, D.; Ricksten, S.-E.; Faivre, A.; Verissimo, T.; Gariani, K.; Verney, C.; Galichon, P.; Berchtold, L.; Feraille, E.; Fernandez, M.; et al. Altered Proximal Tubular Cell Glucose Metabolism during Acute Kidney Injury Is Associated with Mortality. Nat. Metab. 2020, 2, 732–743. [Google Scholar] [CrossRef]
- Tran, M.T.; Zsengeller, Z.K.; Berg, A.H.; Khankin, E.V.; Bhasin, M.K.; Kim, W.; Clish, C.B.; Stillman, I.E.; Karumanchi, S.A.; Rhee, E.P.; et al. PGC1α Drives NAD Biosynthesis Linking Oxidative Metabolism to Renal Protection. Nature 2016, 531, 528–532. [Google Scholar] [CrossRef] [Green Version]
- Tran, M.; Tam, D.; Bardia, A.; Bhasin, M.; Rowe, G.C.; Kher, A.; Zsengeller, Z.K.; Akhavan-Sharif, M.R.; Khankin, E.V.; Saintgeniez, M.; et al. PGC-1α Promotes Recovery after Acute Kidney Injury during Systemic Inflammation in Mice. J. Clin. Investig. 2011, 121, 4003–4014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsyuba, E.; Mottis, A.; Zietak, M.; De Franco, F.; van der Velpen, V.; Gariani, K.; Ryu, D.; Cialabrini, L.; Matilainen, O.; Liscio, P.; et al. De Novo NAD+ Synthesis Enhances Mitochondrial Function and Improves Health. Nature 2018, 563, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Faivre, A.; Katsyuba, E.; Verissimo, T.; Lindenmeyer, M.; Rajaram, R.D.; Naesens, M.; Heckenmeyer, C.; Mottis, A.; Feraille, E.; Cippà, P.; et al. Differential Role of Nicotinamide Adenine Dinucleotide Deficiency in Acute and Chronic Kidney Disease. Nephrol. Dial. Transplant. 2021, 36, 60–68. [Google Scholar] [CrossRef]
- Kang, H.M.; Ahn, S.H.; Choi, P.; Ko, Y.-A.; Han, S.H.; Chinga, F.; Park, A.S.D.; Tao, J.; Sharma, K.; Pullman, J.; et al. Defective Fatty Acid Oxidation in Renal Tubular Epithelial Cells Plays a Key Role in Kidney Fibrosis Development. Nat. Med. 2015, 21, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Grams, M.E.; Shafi, T.; Rhee, E.P. Metabolomics Research in Chronic Kidney Disease. JASN 2018, 29, 1588–1590. [Google Scholar] [CrossRef] [Green Version]
- Wijermars, L.G.M.; Schaapherder, A.F.; de Vries, D.K.; Verschuren, L.; Wüst, R.C.I.; Kostidis, S.; Mayboroda, O.A.; Prins, F.; Ringers, J.; Bierau, J.; et al. Defective Postreperfusion Metabolic Recovery Directly Associates with Incident Delayed Graft Function. Kidney Int. 2016, 90, 181–191. [Google Scholar] [CrossRef]
- Stenlund, H.; Madsen, R.; Vivi, A.; Calderisi, M.; Lundstedt, T.; Tassini, M.; Carmellini, M.; Trygg, J. Monitoring Kidney-Transplant Patients Using Metabolomics and Dynamic Modeling. Chemom. Intell. Lab. Syst. 2009, 98, 45–50. [Google Scholar] [CrossRef]
- Suhre, K.; Schwartz, J.E.; Sharma, V.K.; Chen, Q.; Lee, J.R.; Muthukumar, T.; Dadhania, D.M.; Ding, R.; Ikle, D.N.; Bridges, N.D.; et al. Urine Metabolite Profiles Predictive of Human Kidney Allograft Status. J. Am. Soc. Nephrol. 2016, 27, 626–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goek, O.-N.; Döring, A.; Gieger, C.; Heier, M.; Koenig, W.; Prehn, C.; Römisch-Margl, W.; Wang-Sattler, R.; Illig, T.; Suhre, K.; et al. Serum Metabolite Concentrations and Decreased GFR in the General Population. Am. J. Kidney Dis. 2012, 60, 197–206. [Google Scholar] [CrossRef]
- Yu, B.; Zheng, Y.; Nettleton, J.A.; Alexander, D.; Coresh, J.; Boerwinkle, E. Serum Metabolomic Profiling and Incident CKD among African Americans. Clin. J. Am. Soc. Nephrol. 2014, 9, 1410–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calderisi, M.; Vivi, A.; Mlynarz, P.; Tassin, M.; Banasik, M.; Dawiskiba, T.; Carmellini, M. Using Metabolomics to Monitor Kidney Transplantation Patients by Means of Clustering to Spot Anomalous Patient Behavior. Transplant. Proc. 2013, 45, 1511–1515. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Garcia-Tsao, G.; Reddy, K.R.; O’Leary, J.G.; Vargas, H.E.; Lai, J.C.; Kamath, P.S.; Tandon, P.; Subramanian, R.M.; Thuluvath, P.; et al. Admission Urinary and Serum Metabolites Predict Renal Outcomes in Hospitalized Patients with Cirrhosis. Hepatology 2021, 74, 2699–2713. [Google Scholar] [CrossRef]
- Huang, J.; Huth, C.; Covic, M.; Troll, M.; Adam, J.; Zukunft, S.; Prehn, C.; Wang, L.; Nano, J.; Scheerer, M.F.; et al. Machine Learning Approaches Reveal Metabolic Signatures of Incident Chronic Kidney Disease in Individuals with Prediabetes and Type 2 Diabetes. Diabetes 2020, 69, 2756–2765. [Google Scholar] [CrossRef]
- Chen, D.-Q.; Cao, G.; Chen, H.; Argyopoulos, C.P.; Yu, H.; Su, W.; Chen, L.; Samuels, D.C.; Zhuang, S.; Bayliss, G.P.; et al. Identification of Serum Metabolites Associating with Chronic Kidney Disease Progression and Anti-Fibrotic Effect of 5-Methoxytryptophan. Nat. Commun. 2019, 10, 1476. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.-L.; Qiu, X.-J.; Wang, W.-B.; Li, R.-M.; Wang, D.-S. NMR Metabolomics and Random Forests Models to Identify Potential Plasma Biomarkers of Blood Stasis Syndrome with Coronary Heart Disease Patients. Front. Physiol. 2019, 10, 1109. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, N.; Chang, W.; Dang, P.; Lu, X.; Wan, C.; Gampala, S.; Huang, Z.; Wang, J.; Ma, Q.; Zang, Y.; et al. A Graph Neural Network Model to Estimate Cell-Wise Metabolic Flux Using Single-Cell RNA-Seq Data. Genome Res. 2021, 31, 1867–1884. [Google Scholar] [CrossRef]
- Cippà, P.E.; Sun, B.; Liu, J.; Chen, L.; Naesens, M.; McMahon, A.P. Transcriptional Trajectories of Human Kidney Injury Progression. JCI Insight 2018, 3, e123151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhn, M. Building Predictive Models in R Using the Caret Package. J. Stat. Softw. 2008, 28, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, M. The Caret Package. Available online: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.150.2466&rep=rep1&type=pdf (accessed on 8 December 2021).
- Dash, J.; Verissimo, T.; Faivre, A.; Berchtold, L.; Berney, T.; Pugin, J.; de Seigneux, S.; Legouis, D. Kinetic GFR Outperforms CKD-EPI for Slow Graft Function Prediction in the Immediate Postoperative Period Following Kidney Transplantation. J. Clin. Med. 2020, 9, 4003. [Google Scholar] [CrossRef]
- Jäger, S.; Allhorn, A.; Bießmann, F. A Benchmark for Data Imputation Methods. Front. Big Data 2021, 4, 48. [Google Scholar] [CrossRef]
- Nicol, D.; MacDonald, A.S.; Lawen, J.; Belitsky, P. Early Prediction of Renal Allograft Loss beyond One Year. Transpl. Int. 1993, 6, 153–157. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Skeans, M.A. Patient Outcomes in Renal Transplantation (PORT) Investigators The Relationship between Kidney Function and Long-Term Graft Survival after Kidney Transplant. Am. J. Kidney Dis. 2011, 57, 466–475. [Google Scholar] [CrossRef]
- Giral, M.; Taddei, C.; Nguyen, J.M.; Dantal, J.; Hourmant, M.; Cantarovich, D.; Blancho, G.; Ancelet, D.; Soulillou, J.P. Single-Center Analysis of 468 First Cadaveric Kidney Allografts with a Uniform ATG-CsA Sequential Therapy. Clin. Transpl. 1996, 257–264. Available online: https://pubmed.ncbi.nlm.nih.gov/9286575/ (accessed on 8 December 2021).
- Salvadori, M.; Rosati, A.; Bock, A.; Chapman, J.; Dussol, B.; Fritsche, L.; Jeffery, J.; Kliem, V.; Lebranchu, Y.; Oppenheimer, F.; et al. One-Year Posttransplant Renal Function Is a Strong Predictor of Long-Term Kidney Function: Results from the Neoral-MOST Observational Study. Transplant. Proc. 2003, 35, 2863–2867. [Google Scholar] [CrossRef]
- Humar, A.; Kerr, S.; Gillingham, K.J.; Matas, A.J. Features of Acute Rejection That Increase Risk for Chronic Rejection. Transplantation 1999, 68, 1200–1203. [Google Scholar] [CrossRef]
- Lenihan, C.R.; OLKelly, P.; Mohan, P. Correction to: Lenihan, et al., MDRD-Estimated GFR at One Year Post-Renal Transplant Is a Predictor of Long-Term Graft Function. Ren. Fail. 2018, 40, 119. [Google Scholar] [CrossRef]
- Resende, L.; Guerra, J.; Santana, A.; Mil-Homens, C.; Abreu, F.; da Costa, A.G. First Year Renal Function as a Predictor of Kidney Allograft Outcome. Transplant. Proc. 2009, 41, 846–848. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Skeans, M.A.; Peng, Y.; Weinhandl, E.D. A Simple Tool to Predict Outcomes after Kidney Transplant. Am. J. Kidney Dis. 2010, 56, 947–960. [Google Scholar] [CrossRef]
- Ibrahim, A.; Garg, A.X.; Knoll, G.A.; Akbari, A.; White, C.A. Kidney Function Endpoints in Kidney Transplant Trials: A Struggle for Power. Am. J. Transplant. 2013, 13, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Schley, G.; Klanke, B.; Schödel, J.; Forstreuter, F.; Shukla, D.; Kurtz, A.; Amann, K.; Wiesener, M.S.; Rosen, S.; Eckardt, K.-U.; et al. Hypoxia-Inducible Transcription Factors Stabilization in the Thick Ascending Limb Protects against Ischemic Acute Kidney Injury. J. Am. Soc. Nephrol. 2011, 22, 2004–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Biju, M.P.; Wang, M.-H.; Haase, V.H.; Dong, Z. Cytoprotective Effects of Hypoxia against Cisplatin-Induced Tubular Cell Apoptosis: Involvement of Mitochondrial Inhibition and P53 Suppression. JASN 2006, 17, 1875–1885. [Google Scholar] [CrossRef] [Green Version]
- Shu, S.; Wang, Y.; Zheng, M.; Liu, Z.; Cai, J.; Tang, C.; Dong, Z. Hypoxia and Hypoxia-Inducible Factors in Kidney Injury and Repair. Cells 2019, 8, 207. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Devalaraja-Narashimha, K.; Padanilam, B.J. TIGAR Regulates Glycolysis in Ischemic Kidney Proximal Tubules. Am. J. Physiol. Ren. Physiol. 2015, 308, F298–F308. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-T.; Coleman, R.A.; Scheinman, J.I.; Kolbeck, P.C.; Sidbury, J.B. Renal Disease in Type I Glycogen Storage Disease. N. Engl. J. Med. 1988, 318, 7–11. [Google Scholar] [CrossRef]
- Gjorgjieva, M.; Raffin, M.; Duchampt, A.; Perry, A.; Stefanutti, A.; Brevet, M.; Tortereau, A.; Dubourg, L.; Hubert-Buron, A.; Mabille, M.; et al. Progressive Development of Renal Cysts in Glycogen Storage Disease Type I. Hum. Mol. Genet. 2016, 25, 3784–3797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallan, S.; Afkarian, M.; Zelnick, L.R.; Kestenbaum, B.; Sharma, S.; Saito, R.; Darshi, M.; Barding, G.; Raftery, D.; Ju, W.; et al. Metabolomics and Gene Expression Analysis Reveal Down-Regulation of the Citric Acid (TCA) Cycle in Non-Diabetic CKD Patients. EBioMedicine 2017, 26, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Uribe, A.P.; Hernández-Cruz, E.Y.; Ramírez-Magaña, K.J.; Pedraza-Chaverri, J. Involvement of Tricarboxylic Acid Cycle Metabolites in Kidney Diseases. Biomolecules 2021, 11, 1259. [Google Scholar] [CrossRef]
- Toyohara, T.; Akiyama, Y.; Suzuki, T.; Takeuchi, Y.; Mishima, E.; Tanemoto, M.; Momose, A.; Toki, N.; Sato, H.; Nakayama, M.; et al. Metabolomic Profiling of Uremic Solutes in CKD Patients. Hypertens. Res. 2010, 33, 944–952. [Google Scholar] [CrossRef]
- Chen, D.-Q.; Cao, G.; Chen, H.; Liu, D.; Su, W.; Yu, X.-Y.; Vaziri, N.D.; Liu, X.-H.; Bai, X.; Zhang, L.; et al. Gene and Protein Expressions and Metabolomics Exhibit Activated Redox Signaling and Wnt/β-Catenin Pathway Are Associated with Metabolite Dysfunction in Patients with Chronic Kidney Disease. Redox Biol. 2017, 12, 505–521. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-N.; Ma, S.-X.; Chen, Y.-Y.; Chen, L.; Liu, B.-L.; Liu, Q.-Q.; Zhao, Y.-Y. Chronic Kidney Disease: Biomarker Diagnosis to Therapeutic Targets. Clin. Chim. Acta 2019, 499, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.-Y. Metabolomics in Chronic Kidney Disease. Clin. Chim. Acta 2013, 422, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Miao, H.; Wu, X.-Q.; Wang, Y.-N.; Chen, D.-Q.; Chen, L.; Vaziri, N.D.; Zhuang, S.; Guo, Y.; Su, W.; Ma, S.-X.; et al. 1-Hydroxypyrene Mediates Renal Fibrosis through Aryl Hydrocarbon Receptor Signalling Pathway. Br. J. Pharmacol. 2022, 179, 103–124. [Google Scholar] [CrossRef] [PubMed]
- Miao, H.; Cao, G.; Wu, X.-Q.; Chen, Y.-Y.; Chen, D.-Q.; Chen, L.; Vaziri, N.D.; Feng, Y.-L.; Su, W.; Gao, Y.; et al. Identification of Endogenous 1-Aminopyrene as a Novel Mediator of Progressive Chronic Kidney Disease via Aryl Hydrocarbon Receptor Activation. Br. J. Pharmacol. 2020, 177, 3415–3435. [Google Scholar] [CrossRef]
- Kim, J. Spermidine Rescues Proximal Tubular Cells from Oxidative Stress and Necrosis after Ischemic Acute Kidney Injury. Arch. Pharm. Res. 2017, 40, 1197–1208. [Google Scholar] [CrossRef]
- Zahedi, K.; Barone, S.; Wang, Y.; Murray-Stewart, T.; Roy-Chaudhury, P.; Smith, R.D.; Casero, R.A.; Soleimani, M. Proximal Tubule Epithelial Cell Specific Ablation of the Spermidine/Spermine N1-Acetyltransferase Gene Reduces the Severity of Renal Ischemia/Reperfusion Injury. PLoS ONE 2014, 9, e110161. [Google Scholar] [CrossRef]
- Feng, Y.-L.; Cao, G.; Chen, D.-Q.; Vaziri, N.D.; Chen, L.; Zhang, J.; Wang, M.; Guo, Y.; Zhao, Y.-Y. Microbiome-Metabolomics Reveals Gut Microbiota Associated with Glycine-Conjugated Metabolites and Polyamine Metabolism in Chronic Kidney Disease. Cell. Mol. Life Sci. CMLS 2019, 76, 4961–4978. [Google Scholar] [CrossRef] [Green Version]
- Cuperlovic-Culf, M. Machine Learning Methods for Analysis of Metabolic Data and Metabolic Pathway Modeling. Metabolites 2018, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Bravo-Merodio, L.; Williams, J.A.; Gkoutos, G.V.; Acharjee, A. -Omics Biomarker Identification Pipeline for Translational Medicine. J. Transl. Med. 2019, 17, 155. [Google Scholar] [CrossRef] [Green Version]
- Amaratunga, D.; Cabrera, J.; Lee, Y.-S. Enriched Random Forests. Bioinformatics 2008, 24, 2010–2014. [Google Scholar] [CrossRef] [Green Version]
- Svetnik, V.; Liaw, A.; Tong, C.; Culberson, J.C.; Sheridan, R.P.; Feuston, B.P. Random Forest: A Classification and Regression Tool for Compound Classification and QSAR Modeling. J. Chem. Inf. Comput. Sci. 2003, 43, 1947–1958. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Altman, N.; Krzywinski, M. Ensemble Methods: Bagging and Random Forests. Nat. Methods 2017, 14, 933–934. [Google Scholar] [CrossRef]
- Gampala, S.; Shah, F.; Lu, X.; Moon, H.-R.; Babb, O.; Umesh Ganesh, N.; Sandusky, G.; Hulsey, E.; Armstrong, L.; Mosely, A.L.; et al. Ref-1 Redox Activity Alters Cancer Cell Metabolism in Pancreatic Cancer: Exploiting This Novel Finding as a Potential Target. J. Exp. Clin. Cancer Res. 2021, 40, 251. [Google Scholar] [CrossRef]
- Abbiss, H.; Maker, G.L.; Trengove, R.D. Metabolomics Approaches for the Diagnosis and Understanding of Kidney Diseases. Metabolites 2019, 9, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, J.M. Glutathione and Glycine in Acute Renal Failure. Ren. Fail. 1992, 14, 311–319. [Google Scholar] [CrossRef]
- Santangelo, F.; Witko-Sarsat, V.; Drüeke, T.; Descamps-Latscha, B. Restoring Glutathione as a Therapeutic Strategy in Chronic Kidney Disease. Nephrol. Dial. Transplant. 2004, 19, 1951–1955. [Google Scholar] [CrossRef] [PubMed]
- Zuo, M.; Tang, J.; Xiang, M.; Long, Q.; Dai, J.; Yu, G.; Zhang, H.; Hu, H. Clinical Observation of the Reduced Glutathione in the Treatment of Diabetic Chronic Kidney Disease. J. Cell. Biochem. 2019, 120, 8483–8491. [Google Scholar] [CrossRef] [PubMed]
- Nakatsu, R.T. An Evaluation of Four Resampling Methods Used in Machine Learning Classification. IEEE Intell. Syst. 2021, 36, 51–57. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. BMC Med. 2015, 13, 214. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1-yr eGFR < 51 n = 21 | 1-yr eGFR > 51 n = 21 | Total n = 42 | p-Value | |
|---|---|---|---|---|
| Donor serum creatinine (mg/dL) | 0.8 (0.3) | 0.7 (0.2) | 0.7 (0.2) | 0.180 |
| Donor sex male | 9 (42.9%) | 10 (47.6%) | 19 (45.2%) | 1.000 |
| Donor age (years) | 39.3 (16.6) | 55.9 (6.7) | 47.8 (14.9) | 0.002 |
| Donor type | 1.000 | |||
| Donation after brain death | 12 (57.1%) | 13 (61.9%) | 25 (59.5%) | |
| Deceased cadaveric donor | 7 (33.3%) | 6 (28.6%) | 13 (31.0%) | |
| Living donor | 2 (9.5%) | 2 (9.5%) | 4 (9.5%) | |
| Donor weight (kg) | 71.5 (13.5) | 77.0 (13.6) | 74.2 (13.7) | 0.175 |
| Donor height (cm) | 172.9 (8.6) | 169.8 (8.6) | 171.3 (8.6) | 0.367 |
| Donor body mass index (kg/m2) | 23.9 (4.3) | 26.7 (4.6) | 25.3 (4.6) | 0.002 |
| Donor hypertension | 1 (4.8%) | 6 (28.6%) | 7 (16.7%) | 0.093 |
| Recipient age (years) | 50.0 (14.2) | 54.6 (11.6) | 52.3 (13.0) | 0.385 |
| Recipient sex male | 14 (66.7%) | 13 (61.9%) | 27 (64.3%) | 1.000 |
| Cold ischemia time (hours) | 11.4 (5.6) | 12.9 (5.2) | 12.2 (5.4) | 0.187 |
| Warm ischemia time (min) | 49.5 (18.5) | 47.9 (13.6) | 48.7 (16.1) | 0.995 |
| Delayed graft function | 2 (9.5%) | 4 (19.0%) | 6 (14.3%) | 0.663 |
| Immunosuppression | 0.520 | |||
| TAC-MMF-CS | 9 (42.9%) | 6 (28.6%) | 15 (35.7%) | |
| Induction with Basiliximab | 12 (57.1%) | 15 (71.4%) | 27 (64.3%) | |
| 1-week Serum Creatinine (mg/dL) | 2.8 (3.0) | 4.0 (3.4) | 3.4 (3.3) | 0.110 |
| Cohort Test n = 8 | Cohort Train n = 34 | Total n = 42 | p-Value | |
|---|---|---|---|---|
| Donor serum creatinine (mg/dL) | 0.8 (0.2) | 0.7 (0.3) | 0.7 (0.2) | 0.352 |
| Donor sex male | 3 (37.5%) | 16 (47.1%) | 19 (45.2%) | 0.760 |
| Donor age (years) | 40.7 (18.0) | 49.4 (14.0) | 47.8 (14.9) | 0.227 |
| Donor type | 0.491 | |||
| Donation after brain death | 6 (75.0%) | 19 (55.9%) | 25 (59.5%) | |
| Deceased cadaveric donor | 1 (12.5%) | 12 (35.3%) | 13 (31.0%) | |
| Living donor | 1 (12.5%) | 3 (8.8%) | 4 (9.5%) | |
| Donor weight (kg) | 71.0 (7.9) | 75.0 (14.7) | 74.2 (13.7) | 0.508 |
| Donor height (cm) | 169.5 (10.0) | 171.8 (8.4) | 171.3 (8.6) | 0.759 |
| Donor Body Mass Index (kg/m2) | 24.8 (2.6) | 25.4 (5.0) | 25.3 (4.6) | 0.987 |
| Donor hypertension | 1 (12.5%) | 6 (17.6%) | 7 (16.7%) | 0.093 |
| Recipient age (years) | 56.5 (10.7) | 51.3 (13.5) | 52.3 (13.0) | 0.370 |
| Recipient sex male | 5 (62.5%) | 22 (64.7%) | 27 (64.3%) | 1.000 |
| Cold ischemia time (hours) | 12.8 (5.6) | 12.0 (5.4) | 12.2 (5.4) | 0.564 |
| Warm ischemia time (min) | 37.6 (8.5) | 51.2 (16.4) | 48.7 (16.1) | 0.034 |
| Delayed graft function | 1 (12.5%) | 5 (14.7%) | 6 (14.3%) | 1.000 |
| Immunosuppression | 0.425 | |||
| TAC-MMF-CS | 4 (50.0%) | 23 (67.6%) | 27 (64.3%) | |
| Induction with Basiliximab | 4 (50.0%) | 11 (32.4%) | 15 (35.7%) | |
| 1-week Serum Creatinine (mg/dL) | 3.8 (3.8) | 3.3 (3.2) | 3.4 (3.3) | 0.974 |
| 1-year Glomerular filtration rate (estimated, mL/min/1.73 m2) | 57.4 (19.3) | 52.2 (16.3) | 53.2 (16.8) | 0.586 |
| RMSE | MAE | R2 | |
|---|---|---|---|
| random forest | 12.2 ± 3.2 | 9.2 ± 2.9 | 0.5 ± 0.6 |
| univariable linear model | 24.4 ± 7.5 | 16.4 ± 6.68 | −0.8 ± 1.0 |
| stepwise linear model | 23.2 ± 6.2 | 18.0 ± 5.4 | −0.6 ± 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verissimo, T.; Faivre, A.; Sgardello, S.; Naesens, M.; de Seigneux, S.; Criton, G.; Legouis, D. Estimated Renal Metabolomics at Reperfusion Predicts One-Year Kidney Graft Function. Metabolites 2022, 12, 57. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo12010057
Verissimo T, Faivre A, Sgardello S, Naesens M, de Seigneux S, Criton G, Legouis D. Estimated Renal Metabolomics at Reperfusion Predicts One-Year Kidney Graft Function. Metabolites. 2022; 12(1):57. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo12010057
Chicago/Turabian StyleVerissimo, Thomas, Anna Faivre, Sebastian Sgardello, Maarten Naesens, Sophie de Seigneux, Gilles Criton, and David Legouis. 2022. "Estimated Renal Metabolomics at Reperfusion Predicts One-Year Kidney Graft Function" Metabolites 12, no. 1: 57. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo12010057