
The Influence of Oxidative Stress on Neurological Outcomes in Spontaneous Intracerebral Hemorrhage

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Blood and CSF Samples
2.3. Analysis of Antioxidants and Oxidative Stress Markers
2.4. Evaluation of Clinical Data and Imaging
2.5. Statistical Analysis
2.6. Ethics Declarations
3. Results
3.1. Baseline Demographics and Follow-Up
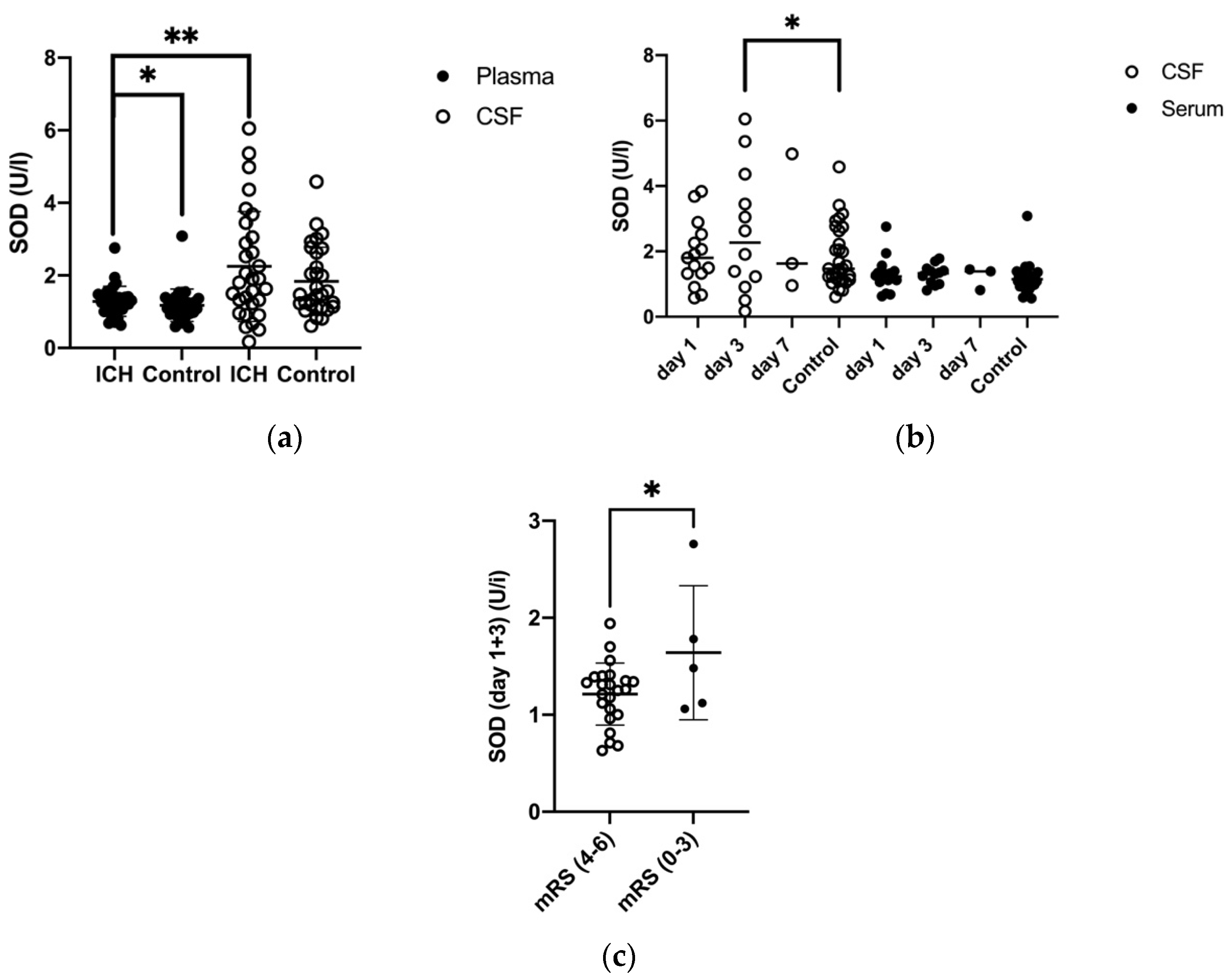
3.2. Superoxide Dismutase (SOD) in Plasma and CSF
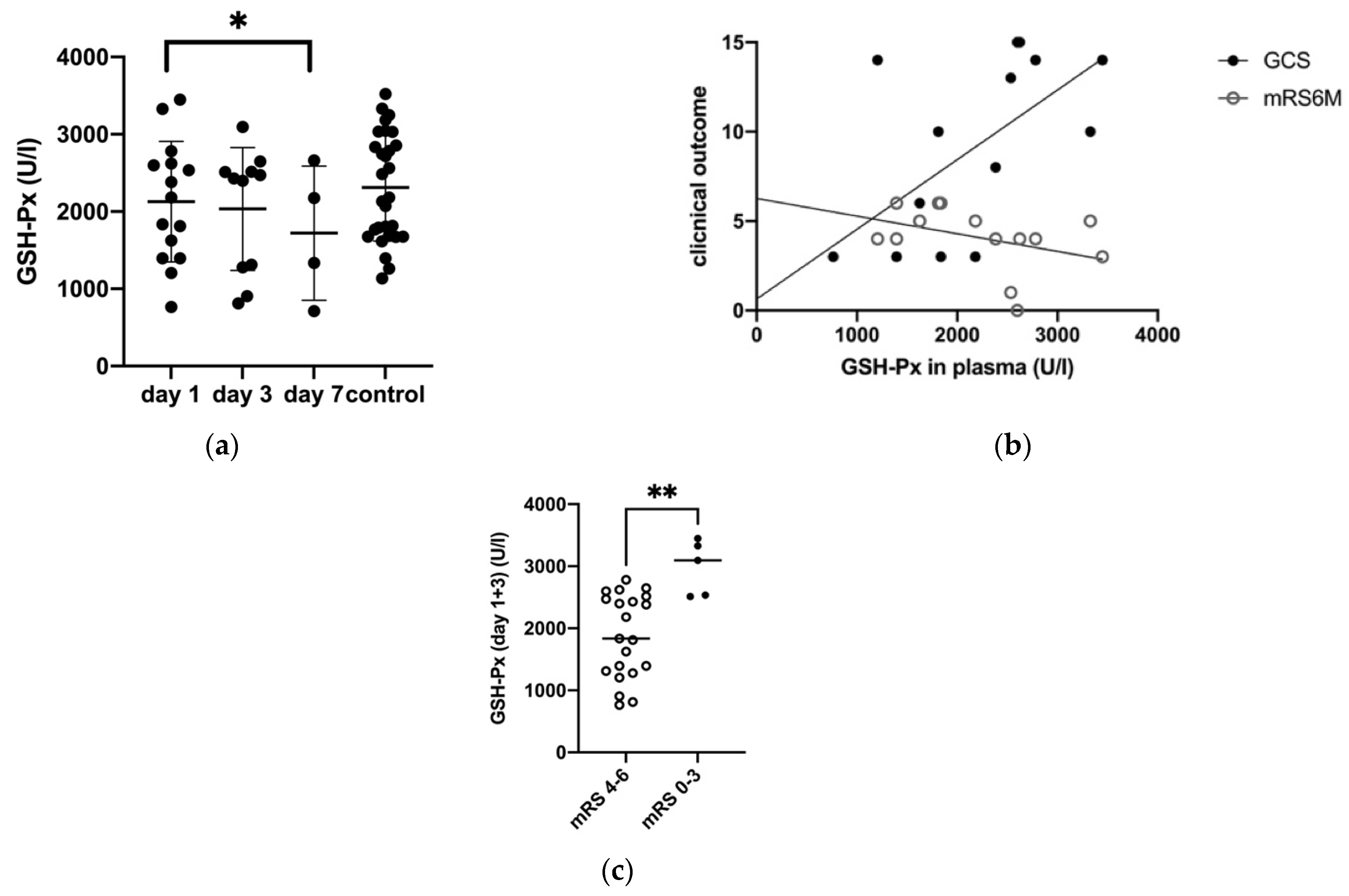
3.3. Glutathione Peroxidase (GSH-Px) in Plasma and CSF
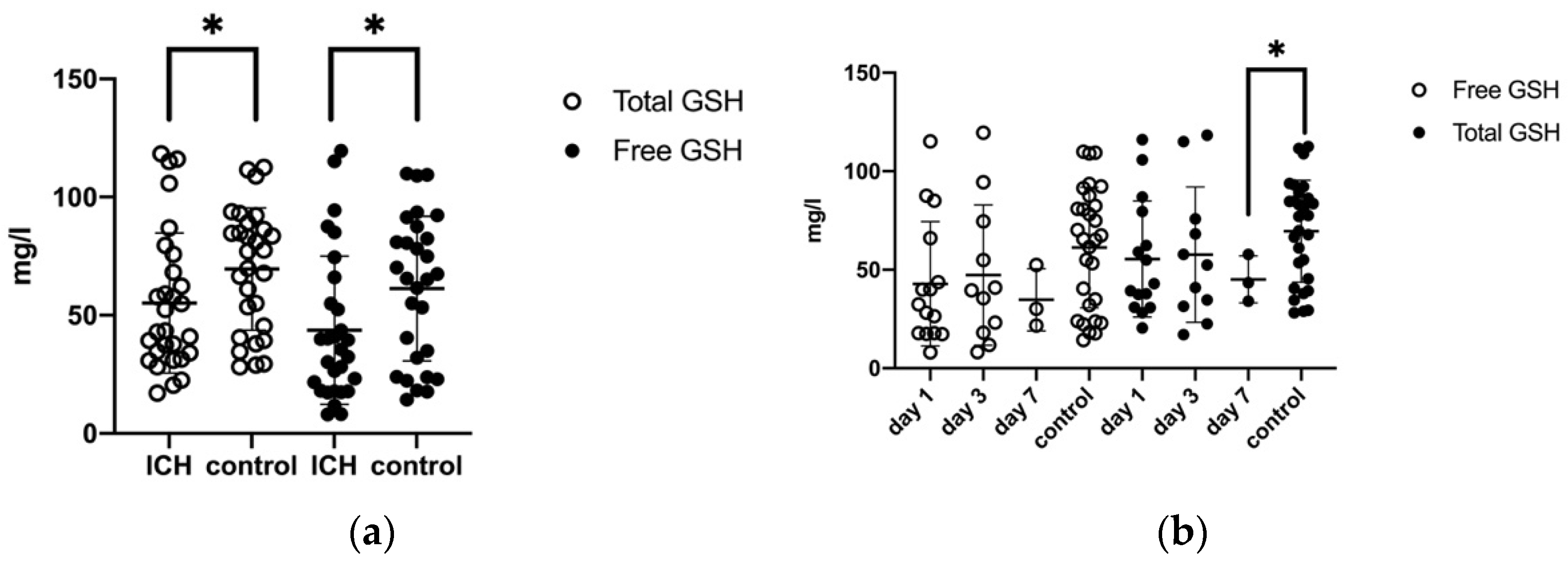
3.4. Glutathione-Sulfhydryl (GSH) in Plasma
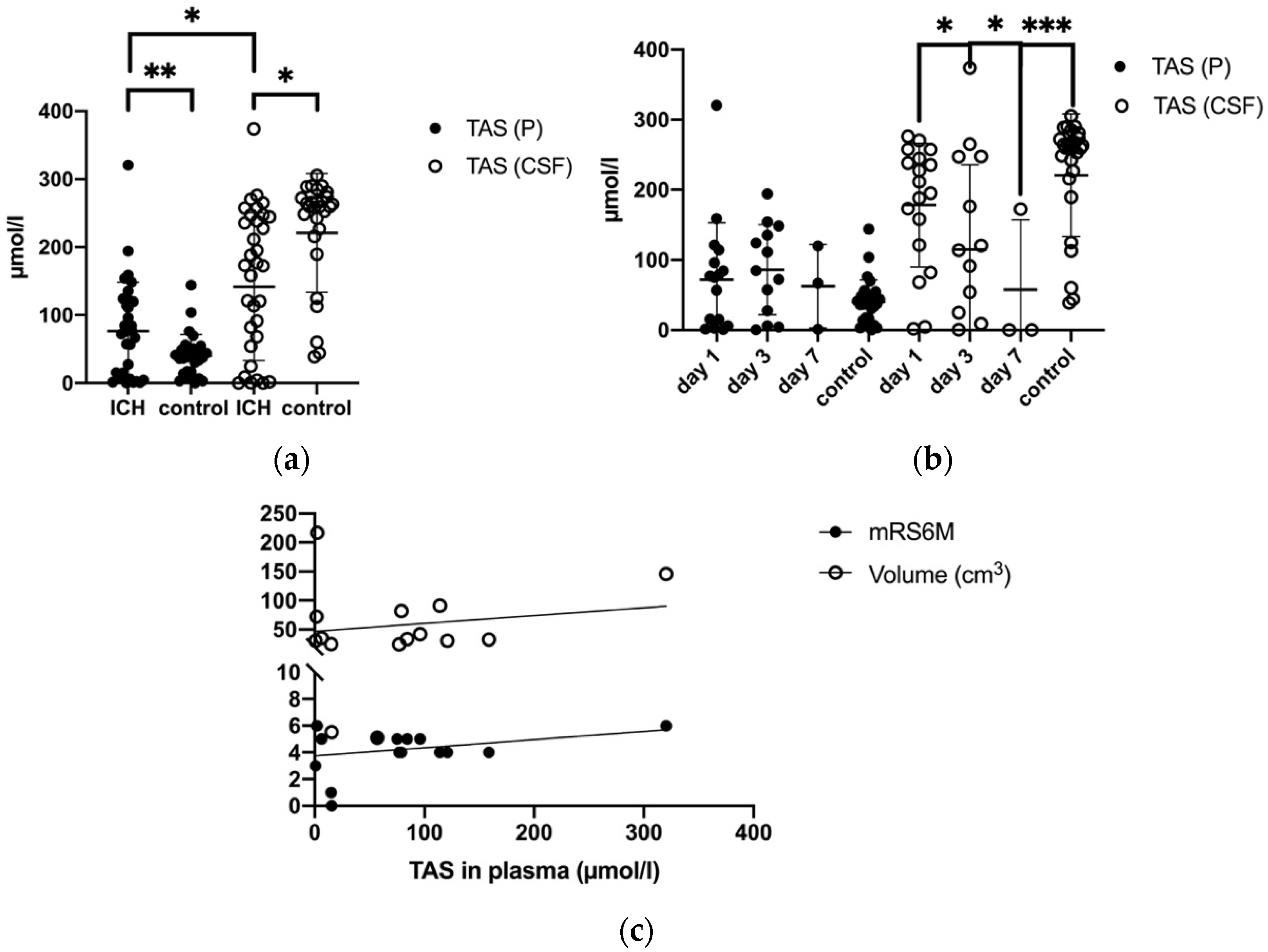
3.5. Total Antioxidant Status (TAS) in Plasma and CSF
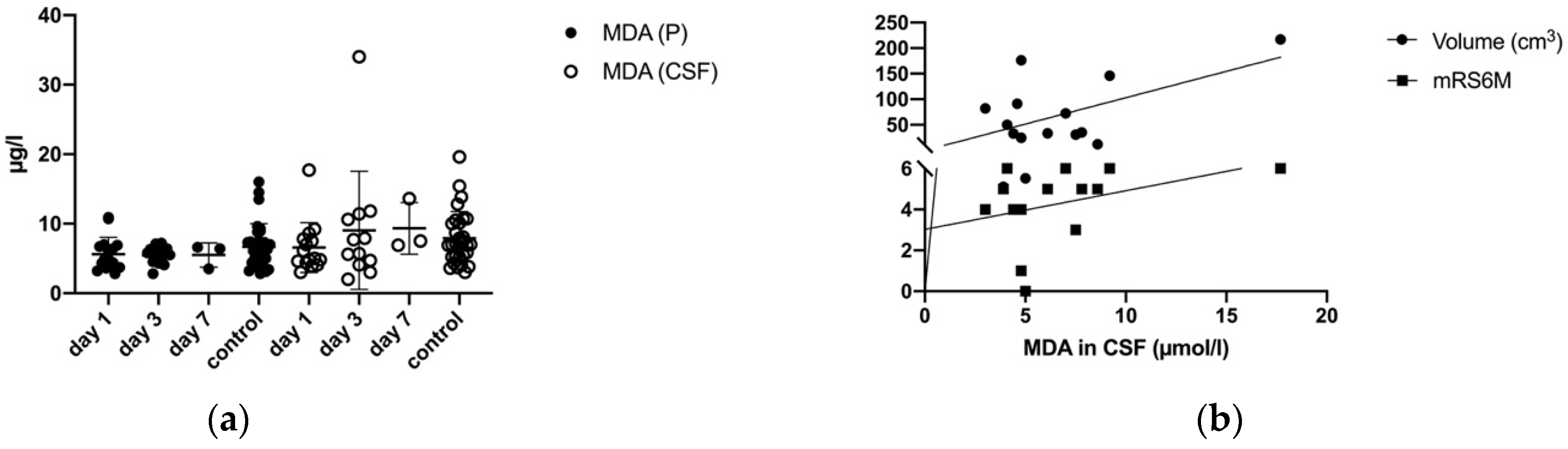
3.6. Malondialdehyde (MDA) in Plasma and CSF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qureshi, A.I.; Mendelow, A.D.; Hanley, D.F. Intracerebral Haemorrhage. Lancet 2009, 373, 1632–1644. [Google Scholar] [CrossRef] [Green Version]
- Krishnamurthi, R.V.; Feigin, V.L.; Forouzanfar, M.H.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.M.; Truelsen, T.; et al. Global and Regional Burden of First-Ever Ischaemic and Haemorrhagic Stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet Glob. Health 2013, 1, e259–e281. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira Manoel, A.L. Surgery for Spontaneous Intracerebral Hemorrhage. Crit. Care 2020, 24, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gildersleeve, K.L.; Hirzallah, M.I.; Esquenazi, Y.; Moomaw, C.J.; Sekar, P.; Cai, C.; Tandon, N.; Woo, D.; Gonzales, N.R. Hemicraniectomy for Supratentorial Primary Intracerebral Hemorrhage: A Retrospective, Propensity Score Matched Study. J. Stroke Cerebrovasc. Dis. 2019, 28, 104361. [Google Scholar] [CrossRef]
- Zhou, H.; Zhang, Y.; Liu, L.; Han, X.; Tao, Y.; Tang, Y.; Hua, W.; Xue, J.; Dong, Q. A Prospective Controlled Study: Minimally Invasive Stereotactic Puncture Therapy versus Conventional Craniotomy in the Treatment of Acute Intracerebral Hemorrhage. BMC Neurol. 2011, 11, 76. [Google Scholar] [CrossRef] [Green Version]
- Mendelow, A.D.; Gregson, B.A.; Fernandes, H.M.; Murray, G.D.; Teasdale, G.M.; Hope, D.T.; Karimi, A.; Shaw, M.D.M.; Barer, D.H. Early Surgery versus Initial Conservative Treatment in Patients with Spontaneous Supratentorial Intracerebral Haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): A Randomised Trial. Lancet 2005, 365, 387–397. [Google Scholar] [CrossRef]
- Mendelow, A.D.; Gregson, B.A.; Rowan, E.N.; Murray, G.D.; Gholkar, A.; Mitchell, P.M.; STICH II Investigators. Early Surgery versus Initial Conservative Treatment in Patients with Spontaneous Supratentorial Lobar Intracerebral Haematomas (STICH II): A Randomised Trial. Lancet 2013, 382, 397–408. [Google Scholar] [CrossRef] [Green Version]
- Fiorella, D.; Gutman, F.; Woo, H.; Arthur, A.; Aranguren, R.; Davis, R. Minimally Invasive Evacuation of Parenchymal and Ventricular Hemorrhage Using the Apollo System with Simultaneous Neuronavigation, Neuroendoscopy and Active Monitoring with Cone Beam CT. J. Neurointerv. Surg. 2015, 7, 752–757. [Google Scholar] [CrossRef]
- Hanley, D.F.; Thompson, R.E.; Rosenblum, M.; Yenokyan, G.; Lane, K.; McBee, N.; Mayo, S.W.; Bistran-Hall, A.J.; Gandhi, D.; Mould, W.A.; et al. Minimally Invasive Surgery with Thrombolysis in Intracerebral Haemorrhage Evacuation (MISTIE III): A Randomised, Controlled, Open-Label Phase 3 Trial with Blinded Endpoint. Lancet 2019, 393, 1021–1032. [Google Scholar] [CrossRef] [Green Version]
- Newell, D.W.; Shah, M.M.; Wilcox, R.; Hansmann, D.R.; Melnychuk, E.; Muschelli, J.; Hanley, D.F. Minimally Invasive Evacuation of Spontaneous Intracerebral Hemorrhage Using Sonothrombolysis. J. Neurosurg. 2011, 115, 592–601. [Google Scholar] [CrossRef]
- Duan, X.; Wen, Z.; Shen, H.; Shen, M.; Chen, G. Intracerebral Hemorrhage, Oxidative Stress, and Antioxidant Therapy. Oxid. Med. Cell. Longev. 2016, 2016, 1203285. [Google Scholar] [CrossRef] [Green Version]
- Zheng, J.; Shi, L.; Liang, F.; Xu, W.; Li, T.; Gao, L.; Sun, Z.; Yu, J.; Zhang, J. Sirt3 Ameliorates Oxidative Stress and Mitochondrial Dysfunction After Intracerebral Hemorrhage in Diabetic Rats. Front. Neurosci. 2018, 12, 414. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, B.; Whiteman, M. Measuring Reactive Species and Oxidative Damage in Vivo and in Cell Culture: How Should You Do It and What Do the Results Mean? Br. J. Pharmacol. 2004, 142, 231–255. [Google Scholar] [CrossRef] [Green Version]
- Fiers, W.; Beyaert, R.; Declercq, W.; Vandenabeele, P. More than One Way to Die: Apoptosis, Necrosis and Reactive Oxygen Damage. Oncogene 1999, 18, 7719–7730. [Google Scholar] [CrossRef] [Green Version]
- Aygul, R.; Demircan, B.; Erdem, F.; Ulvi, H.; Yildirim, A.; Demirbas, F. Plasma Values of Oxidants and Antioxidants in Acute Brain Hemorrhage: Role of Free Radicals in the Development of Brain Injury. Biol. Trace Elem. Res. 2005, 108, 43–52. [Google Scholar] [CrossRef]
- Davis, S.M.; Pennypacker, K.R. Targeting Antioxidant Enzyme Expression as a Therapeutic Strategy for Ischemic Stroke. Neurochem. Int. 2017, 107, 23–32. [Google Scholar] [CrossRef]
- Watts, M.E.; Pocock, R.; Claudianos, C. Brain Energy and Oxygen Metabolism: Emerging Role in Normal Function and Disease. Front. Mol. Neurosci. 2018, 11, 216. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Yang, Q.; Li, G.; Wang, L.; Hu, W.; Tang, Q.; Li, D.; Sun, Z. Time Course of Heme Oxygenase-1 and Oxidative Stress after Experimental Intracerebral Hemorrhage. Acta Neurochir. 2011, 153, 319–325. [Google Scholar] [CrossRef]
- Han, N.; Ding, S.-J.; Wu, T.; Zhu, Y.-L. Correlation of Free Radical Level and Apoptosis after Intracerebral Hemorrhage in Rats. Neurosci. Bull. 2008, 24, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Gonullu, H.; Aslan, M.; Karadas, S.; Kati, C.; Duran, L.; Milanlioglu, A.; Aydin, M.N.; Demir, H. Serum Prolidase Enzyme Activity and Oxidative Stress Levels in Patients with Acute Hemorrhagic Stroke. Scand. J. Clin. Lab. Investig. 2014, 74, 199–205. [Google Scholar] [CrossRef]
- Loeffler, D.A.; Klaver, A.C.; Coffey, M.P.; Aasly, J.O.; LeWitt, P.A. Increased Oxidative Stress Markers in Cerebrospinal Fluid from Healthy Subjects with Parkinson’s Disease-Associated LRRK2 Gene Mutations. Front. Aging Neurosci. 2017, 9, 89. [Google Scholar] [CrossRef] [Green Version]
- Okabe, T.; Hamaguchi, K.; Inafuku, T.; Hara, M. Aging and Superoxide Dismutase Activity in Cerebrospinal Fluid. J. Neurol. Sci. 1996, 141, 100–104. [Google Scholar] [CrossRef]
- Gregson, B.A.; Broderick, J.P.; Auer, L.M.; Batjer, H.; Chen, X.-C.; Juvela, S.; Morgenstern, L.B.; Pantazis, G.C.; Teernstra, O.P.M.; Wang, W.-Z.; et al. Individual Patient Data Subgroup Meta-Analysis of Surgery for Spontaneous Supratentorial Intracerebral Hemorrhage. Stroke 2012, 43, 1496–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaggiante, J.; Zhang, X.; Mocco, J.; Kellner, C.P. Minimally Invasive Surgery for Intracerebral Hemorrhage. Stroke 2018, 49, 2612–2620. [Google Scholar] [CrossRef]
- Lippitz, B.E.; Mayfrank, L.; Spetzger, U.; Warnke, J.P.; Bertalanffy, H.; Gilsbach, J.M. Lysis of Basal Ganglia Haematoma with Recombinant Tissue Plasminogen Activator (RtPA) after Stereotactic Aspiration: Initial Results. Acta Neurochir. 1994, 127, 157–160. [Google Scholar] [CrossRef]
- Abdu, E.; Hanley, D.F.; Newell, D.W. Minimally Invasive Treatment for Intracerebral Hemorrhage. Neurosurg. Focus 2012, 32, E3. [Google Scholar] [CrossRef] [PubMed]
- Hegde, A.; Menon, G.; Kumar, V.; Lakshmi Prasad, G.; Kongwad, L.I.; Nair, R.; Nayak, R. Clinical Profile and Predictors of Outcome in Spontaneous Intracerebral Hemorrhage from a Tertiary Care Centre in South India. Stroke Res. Treat. 2020, 2020, 2192709. [Google Scholar] [CrossRef] [PubMed]
- Aronowski, J.; Zhao, X. Molecular Pathophysiology of Cerebral Hemorrhage: Secondary Brain Injury. Stroke 2011, 42, 1781–1786. [Google Scholar] [CrossRef]
- Yu, Y.; Chi, X.; Liu, L. A Hypothesis: Hydrogen Sulfide Might Be Neuroprotective against Subarachnoid Hemorrhage Induced Brain Injury. Sci. World J. 2014, 2014, 432318. [Google Scholar] [CrossRef]
- Yu, Y.; Zhao, W.; Zhu, C.; Kong, Z.; Xu, Y.; Liu, G.; Gao, X. The Clinical Effect of Deferoxamine Mesylate on Edema after Intracerebral Hemorrhage. PLoS ONE 2015, 10, e0122371. [Google Scholar] [CrossRef]
- Klatzo, I. Neuropathological Aspects of Brain Edema. J. Neuropathol. Exp. Neurol. 1967, 26, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Qin, Z.; Yin, X. Classification Mechanism and Clinical Analysis of Perihematomal Edema in Intracerebral Hemorrhage. Brain Hemorrhages 2020, 1, 141–145. [Google Scholar] [CrossRef]
- Toda, N.; Ayajiki, K.; Okamura, T. Cerebral Blood Flow Regulation by Nitric Oxide: Recent Advances. Pharmacol. Rev. 2009, 61, 62–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, R.L.; Weir, B.K.; Runzer, T.D.; Grace, M.G. Malondialdehyde, Glutathione Peroxidase, and Superoxide Dismutase in Cerebrospinal Fluid during Cerebral Vasospasm in Monkeys. Can. J. Neurol. Sci. 1992, 19, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakai, T.; Sakata, H.; Narasimhan, P.; Yoshioko, H.; Kinouchi, H.; Chan, P. Transplantation of Neural Stem Cells That Overexpress SOD1 Enhances Amelioration of Intracerebral Hemorrhage in Mice. J. Cereb. Blood Flow Metab. 2014, 34, 441–449. [Google Scholar] [CrossRef] [Green Version]
- Spranger, M.; Krempien, S.; Schwab, S.; Donneberg, S.; Hacke, W. Superoxide Dismutase Activity in Serum of Patients with Acute Cerebral Ischemic Injury. Correlation with Clinical Course and Infarct Size. Stroke 1997, 28, 2425–2428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaetani, P.; Cafe, C.; Rodriguez y Baena, R.; Tancioni, F.; Torri, C.; Tartara, F.; Marzatico, F. Superoxide Dismutase Activity in Cisternal Cerebrospinal Fluid after Aneurysmal Subarachnoid Haemorrhage. Acta Neurochir. 1997, 139, 1033–1037. [Google Scholar] [CrossRef]
- Zhang, Z.; Wu, Y.; Yuan, S.; Zhang, P.; Zhang, J.; Li, H.; Li, X.; Shen, H.; Wang, Z.; Chen, G. Glutathione Peroxidase 4 Participates in Secondary Brain Injury through Mediating Ferroptosis in a Rat Model of Intracerebral Hemorrhage. Brain Res. 2018, 1701, 112–125. [Google Scholar] [CrossRef]
- Diao, X.; Zhou, Z.; Xiang, W.; Jiang, Y.; Tian, N.; Tang, X.; Chen, S.; Wen, J.; Chen, M.; Liu, K.; et al. Glutathione Alleviates Acute Intracerebral Hemorrhage Injury via Reversing Mitochondrial Dysfunction. Brain Res. 2020, 1727, 146514. [Google Scholar] [CrossRef]
- Wang, J.-A.; Tong, M.-L.; Zhao, B.; Zhu, G.; Xi, D.-H.; Yang, J.-P. Parthenolide Ameliorates Intracerebral Hemorrhage-Induced Brain Injury in Rats. Phytother. Res. 2020, 34, 153–160. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Sabatel, R.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Riaño-Ruiz, M.; Jiménez, A.; García-Marín, V. Serum Malondialdehyde Levels and Mortality in Patients with Spontaneous Intracerebral Hemorrhage. World Neurosurg. 2018, 113, e542–e547. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; Almeida, T.; Abreu-González, P.; Ferreres, J.; Solé-Violán, J.; Labarta, L.; Díaz, C.; Jiménez, A. Association between Serum Total Antioxidant Capacity and Mortality in Severe Septic Patients. J. Crit. Care 2015, 30, 217.e7–217.e12. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Pérez-Cejas, A.; Abreu-González, P.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Jiménez, A. Association between Total Antioxidant Capacity and Mortality in Ischemic Stroke Patients. Ann. Intensive Care 2016, 6, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorente, L.; Martín, M.M.; Almeida, T.; Abreu-González, P.; Ramos, L.; Argueso, M.; Riaño-Ruiz, M.; Solé-Violán, J.; Jiménez, A. Total Antioxidant Capacity Is Associated with Mortality of Patients with Severe Traumatic Brain Injury. BMC Neurol. 2015, 15, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | ICH Group | Control Group |
|---|---|---|
| Number of patients | 19 | 29 |
| Sex, n [%] | ||
| Male | 12 (63%) | 14 (48%) |
| Female | 7 (37%) | 15 (52%) |
| Age [years] | ||
| Mean (SD) | 64.05 ± 10.99 | 57.52 ± 15.28 |
| Mean volume of hemorrhageat day 1 [cm3] | 69.75 ± 57.4 | - |
| Antioxidative/ Oxidative Parameters | ICH Group | Control Group | ||
|---|---|---|---|---|
| Day 1 | Day 3 | Day 7 | Day 1 | |
| SOD (P) | [U/I] | |||
| Mean (SD) | 1.18 ± 0.13 | 1.29 ± 0.26 | 1.22 ± 0.20 | 0.45 ± 0.49 |
| SOD (CSF) | [U/I] | |||
| Mean (SD) | 1.84 ± 0.25 | 2.58 ± 0.55 | 2.52 ± 1.67 | 0.94 ± 0.94 |
| GSH-Px (P) | [U/I] | |||
| Mean (SD) | 2127.23 ± 201.52 | 2033.84 ± 239.38 | 1720.0 ± 433.88 | 2312.72 ± 695.89 |
| Free GSH (P) | [mg/L] | |||
| Mean (SD) | 42.86 ± 8.15 | 47.33 ± 10.74 | 34.78 ± 9.14 | 61.34 ± 30.60 |
| Total GSH (P) | [mg/L] | |||
| Mean (SD) | 55.5 ± 7.59 | 57.65 ± 10.36 | 45.1 ± 6.9 | 69.57 ± 25.82 |
| TAS (P) | [μmol/L] | |||
| Mean (SD) | 80.25 ± 20.43 | 86.22 ± 17.82 | 62.60 ± 34.41 | 40.01 ± 31.4 |
| TAS (CSF) | [μmol/L] | |||
| Mean (SD) | 178.40 ± 20.80 | 114.87 ± 31.25 | 57.67 ± 57.37 | 220.99 ± 87.4 |
| MDA (P) | [mg/L] | |||
| Mean (SD) | 5.63 ± 2.43 | 5.44 ± 1.30 | 5.50 ± 1.73 | 6.67 ± 3.33 |
| MDA (CSF) | [mg/L] | |||
| Mean (SD) | 6.57 ± 3.60 | 9.04 ± 8.50 | 9.33 ± 3.71 | 7.92 ± 3.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masomi-Bornwasser, J.; Kurz, E.; Frenz, C.; Schmitt, J.; Wesp, D.M.A.; König, J.; Lotz, J.; Ringel, F.; Kerz, T.; Krenzlin, H.; et al. The Influence of Oxidative Stress on Neurological Outcomes in Spontaneous Intracerebral Hemorrhage. Biomolecules 2021, 11, 1615. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11111615
Masomi-Bornwasser J, Kurz E, Frenz C, Schmitt J, Wesp DMA, König J, Lotz J, Ringel F, Kerz T, Krenzlin H, et al. The Influence of Oxidative Stress on Neurological Outcomes in Spontaneous Intracerebral Hemorrhage. Biomolecules. 2021; 11(11):1615. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11111615
Chicago/Turabian StyleMasomi-Bornwasser, Julia, Elena Kurz, Christina Frenz, Jan Schmitt, Dominik M. A. Wesp, Jochem König, Johannes Lotz, Florian Ringel, Thomas Kerz, Harald Krenzlin, and et al. 2021. "The Influence of Oxidative Stress on Neurological Outcomes in Spontaneous Intracerebral Hemorrhage" Biomolecules 11, no. 11: 1615. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11111615