
Exploring the Connection between Porphyromonas gingivalis and Neurodegenerative Diseases: A Pilot Quantitative Study on the Bacterium Abundance in Oral Cavity and the Amount of Antibodies in Serum

 , , ,
, , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Oral Examination
2.3. Collection of the Samples
2.4. Evaluation of Comorbidities in Patients
2.5. DNA Isolation and Bacterial DNA Quantification on Brushing
2.6. Antibody Assay of Serum
2.7. Statistical Analyses
3. Results
3.1. Clinical and Oral Outcomes
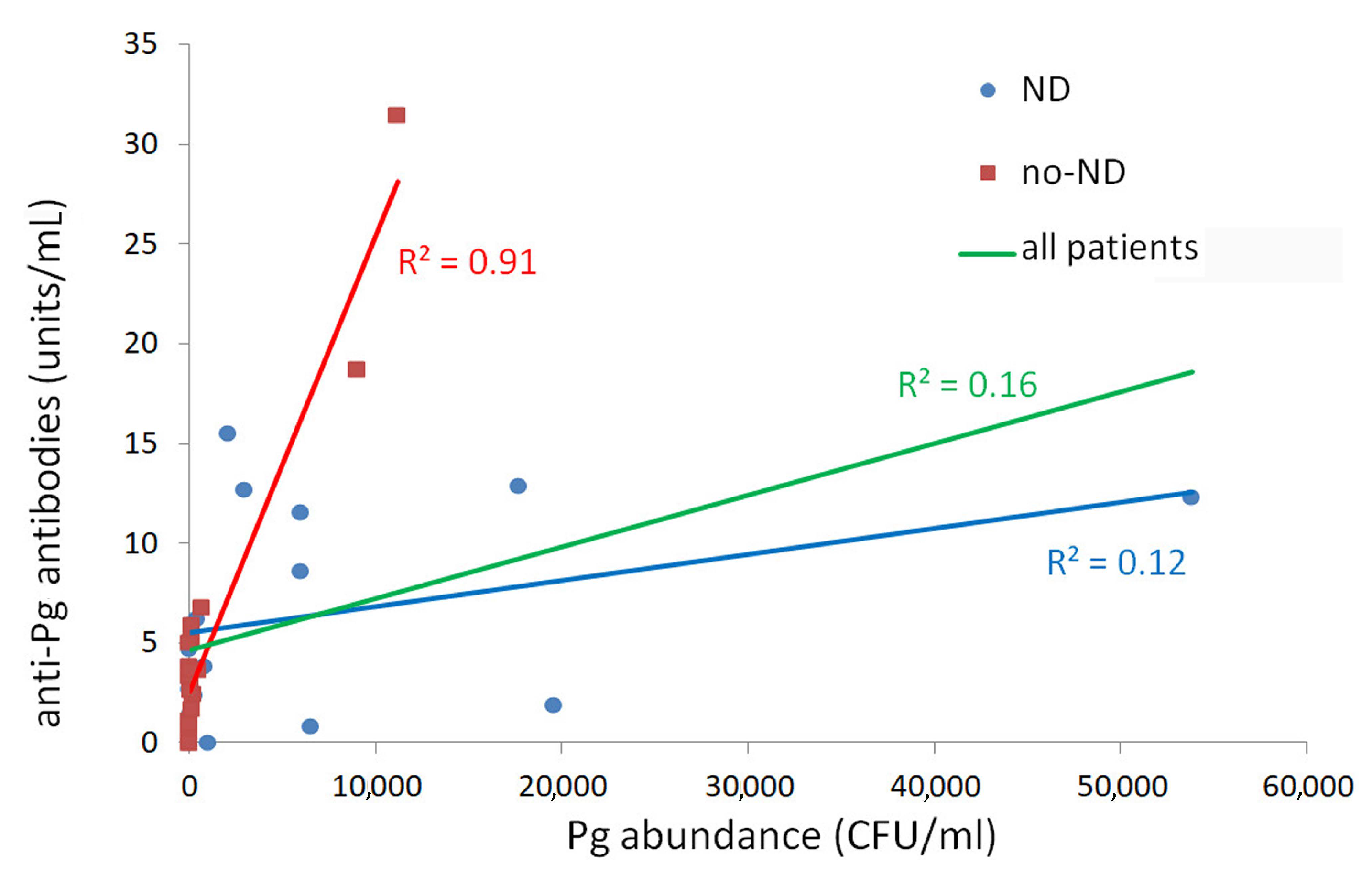
3.2. Pg Bacteria and Antibody Quantification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Miklossy, J. Emerging Roles of Pathogens in Alzheimer Disease. Expert. Rev. Mol. Med. 2011, 13, e30. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharjee, S.; Lukiw, W.J. Alzheimer’s Disease and the Microbiome. Front. Cell Neurosci. 2013, 7, 153. [Google Scholar] [CrossRef] [Green Version]
- Poole, S.; Singhrao, S.K.; Kesavalu, L.; Curtis, M.A.; Crean, S. Determining the Presence of Periodontopathic Virulence Factors in Short-Term Postmortem Alzheimer’s Disease Brain Tissue. J. Alzheimers Dis. 2013, 36, 665–677. [Google Scholar] [CrossRef]
- Kumar, D.K.V.; Choi, S.H.; Washicosky, K.J.; Eimer, W.A.; Tucker, S.; Ghofrani, J.; Lefkowitz, A.; McColl, G.; Goldstein, L.E.; Tanzi, R.E.; et al. Amyloid-β Peptide Protects against Microbial Infection in Mouse and Worm Models of Alzheimer’s Disease. Sci. Trans.l Med. 2016, 8, 340ra72. [Google Scholar] [CrossRef] [Green Version]
- Kinney, J.W.; Bemiller, S.M.; Murtishaw, A.S.; Leisgang, A.M.; Salazar, A.M.; Lamb, B.T. Inflammation as a Central Mechanism in Alzheimer’s Disease. Alzheimers Dement. 2018, 4, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Toldi, J.; Vécsei, L. Exploring the Etiological Links behind Neurodegenerative Diseases: Inflammatory Cytokines and Bioactive Kynurenines. Int. J. Mol. Sci. 2020, 21, 2431. [Google Scholar] [CrossRef] [Green Version]
- Cho, I.; Blaser, M.J. The Human Microbiome: At the Interface of Health and Disease. Nat. Rev. Genet. 2012, 13, 260–270. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.-S.; Jeon, Y.-S.; Chun, J. Current Status and Future Promise of the Human Microbiome. Pediatr. Gastroenterol. Hepatol. Nutr. 2013, 16, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Heintz, C.; Mair, W. You Are What You Host: Microbiome Modulation of the Aging Process. Cell 2014, 156, 408–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancuso, R.; Baglio, F.; Cabinio, M.; Calabrese, E.; Hernis, A.; Nemni, R.; Clerici, M. Titers of Herpes Simplex Virus Type 1 Antibodies Positively Correlate with Grey Matter Volumes in Alzheimer’s Disease. J. Alzheimers Dis. 2014, 38, 741–745. [Google Scholar] [CrossRef]
- González-Sanmiguel, J.; Schuh, C.M.; Muñoz-Montesino, C.; Contreras-Kallens, P.; Aguayo, L.G.; Aguayo, S. Complex Interaction between Resident Microbiota and Misfolded Proteins: Role in Neuroinflammation and Neurodegeneration. Cells 2020, 9, 2476. [Google Scholar] [CrossRef] [PubMed]
- Török, N.; Tanaka, M.; Vécsei, L. Searching for Peripheral Biomarkers in Neurodegenerative Diseases: The Tryptophan-Kynurenine Metabolic Pathway. Int. J. Mol. Sci. 2020, 21, 9338. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.J.; Paskett, K.T.; Cheever, V.J.; Lipsky, M.S. Periodontitis: A Global Disease and the Primary Care Provider’s Role. Postgrad. Med. J. 2017, 93, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Holmer, J.; Aho, V.; Eriksdotter, M.; Paulin, L.; Pietiäinen, M.; Auvinen, P.; Schultzberg, M.; Pussinen, P.J.; Buhlin, K. Subgingival Microbiota in a Population with and without Cognitive Dysfunction. J. Oral. Microbiol. 2021, 13, 1854552. [Google Scholar] [CrossRef]
- Kato, H.; Takahashi, Y.; Iseki, C.; Igari, R.; Sato, H.; Sato, H.; Koyama, S.; Tobita, M.; Kawanami, T.; Iino, M.; et al. Tooth Loss-Associated Cognitive Impairment in the Elderly: A Community-Based Study in Japan. Intern. Med. 2019, 58, 1411–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pussinen, P.J.; Alfthan, G.; Rissanen, H.; Reunanen, A.; Asikainen, S.; Knekt, P. Antibodies to Periodontal Pathogens and Stroke Risk. Stroke 2004, 35, 2020–2023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoyama, N.; Kure, K.; Minabe, M.; Izumi, Y. Increased Heart Failure Prevalence in Patients with a High Antibody Level Against Periodontal Pathogen. Int. Heart J. 2019, 60, 1142–1146. [Google Scholar] [CrossRef] [Green Version]
- Aoki, S.; Hosomi, N.; Nishi, H.; Nakamori, M.; Nezu, T.; Shiga, Y.; Kinoshita, N.; Ueno, H.; Ishikawa, K.; Imamura, E.; et al. Serum IgG Titers to Periodontal Pathogens Predict 3-Month Outcome in Ischemic Stroke Patients. PLoS ONE 2020, 15, e0237185. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Darveau, R.P.; Curtis, M.A. The Keystone-Pathogen Hypothesis. Nat. Rev. Microbiol. 2012, 10, 717–725. [Google Scholar] [CrossRef]
- Chopra, A.; Radhakrishnan, R.; Sharma, M. Porphyromonas Gingivalis and Adverse Pregnancy Outcomes: A Review on Its Intricate Pathogenic Mechanisms. Crit. Rev. Microbiol. 2020, 46, 213–236. [Google Scholar] [CrossRef]
- Perricone, C.; Ceccarelli, F.; Saccucci, M.; Di Carlo, G.; Bogdanos, D.P.; Lucchetti, R.; Pilloni, A.; Valesini, G.; Polimeni, A.; Conti, F. Porphyromonas Gingivalis and Rheumatoid Arthritis. Curr. Opin. Rheumatol. 2019, 31, 517–524. [Google Scholar] [CrossRef]
- Mougeot, J.-L.C.; Stevens, C.B.; Paster, B.J.; Brennan, M.T.; Lockhart, P.B.; Mougeot, F.K.B. Porphyromonas Gingivalis Is the Most Abundant Species Detected in Coronary and Femoral Arteries. J. Oral. Microbiol. 2017, 9, 1281562. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, L.; Cervino, G.; Laino, L.; D’Amico, C.; Mauceri, R.; Tozum, T.F.; Gaeta, M.; Cicciù, M. Porphyromonas Gingivalis, Periodontal and Systemic Implications: A Systematic Review. Dent. J. 2019, 7, 114. [Google Scholar] [CrossRef] [Green Version]
- Sung, C.-E.; Huang, R.-Y.; Cheng, W.-C.; Kao, T.-W.; Chen, W.-L. Association between Periodontitis and Cognitive Impairment: Analysis of National Health and Nutrition Examination Survey (NHANES) III. J. Clin. Periodontol. 2019, 46, 790–798. [Google Scholar] [CrossRef]
- Tzeng, N.-S.; Chung, C.-H.; Yeh, C.-B.; Huang, R.-Y.; Yuh, D.-Y.; Huang, S.-Y.; Lu, R.-B.; Chang, H.-A.; Kao, Y.-C.; Chiang, W.-S.; et al. Are Chronic Periodontitis and Gingivitis Associated with Dementia? A Nationwide, Retrospective, Matched-Cohort Study in Taiwan. Neuroepidemiology 2016, 47, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Peng, Y.; Yu, J.; Chen, T.; Wu, Y.; Shi, L.; Li, Q.; Wu, J.; Fu, X. Invasive Fusobacterium Nucleatum Activates Beta-Catenin Signaling in Colorectal Cancer via a TLR4/P-PAK1 Cascade. Oncotarget 2017, 8, 31802–31814. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Lindahl, C.; Marín, M.J.; Renvert, S.; Herrera, D.; Ohlsson, O.; Wetterling, T.; Sanz, M. Quantification of Periodontal Pathogens in Vascular, Blood, and Subgingival Samples from Patients with Peripheral Arterial Disease or Abdominal Aortic Aneurysms. J. Periodontol. 2014, 85, 1182–1193. [Google Scholar] [CrossRef] [PubMed]
- Kannosh, I.; Staletovic, D.; Toljic, B.; Radunovic, M.; Pucar, A.; Matic Petrovic, S.; Grubisa, I.; Lazarevic, M.; Brkic, Z.; Knezevic Vukcevic, J.; et al. The Presence of Periopathogenic Bacteria in Subgingival and Atherosclerotic Plaques—An Age Related Comparative Analysis. J. Infect. Dev. Ctries. 2018, 12, 1088–1095. [Google Scholar] [CrossRef] [Green Version]
- Madianos, P.N.; Bobetsis, Y.A.; Offenbacher, S. Adverse Pregnancy Outcomes (APOs) and Periodontal Disease: Pathogenic Mechanisms. J. Clin. Periodontol. 2013, 40 (Suppl. 14) (Suppl. 14), S170–S180. [Google Scholar] [CrossRef]
- Noble, J.M.; Borrell, L.N.; Papapanou, P.N.; Elkind, M.S.V.; Scarmeas, N.; Wright, C.B. Periodontitis Is Associated with Cognitive Impairment among Older Adults: Analysis of NHANES-III. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1206–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamer, A.R.; Craig, R.G.; Pirraglia, E.; Dasanayake, A.P.; Norman, R.G.; Boylan, R.J.; Nehorayoff, A.; Glodzik, L.; Brys, M.; de Leon, M.J. TNF-Alpha and Antibodies to Periodontal Bacteria Discriminate between Alzheimer’s Disease Patients and Normal Subjects. J. Neuroimmunol. 2009, 216, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Sparks Stein, P.; Steffen, M.J.; Smith, C.; Jicha, G.; Ebersole, J.L.; Abner, E.; Dawson, D. Serum Antibodies to Periodontal Pathogens Are a Risk Factor for Alzheimer’s Disease. Alzheimers Dement. 2012, 8, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Yu, C.; Zhang, X.; Chen, H.; Dong, J.; Lu, W.; Song, Z.; Zhou, W. Porphyromonas Gingivalis Lipopolysaccharide Induces Cognitive Dysfunction, Mediated by Neuronal Inflammation via Activation of the TLR4 Signaling Pathway in C57BL/6 Mice. J. Neuroinflamm. 2018, 15, 37. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The Diagnosis of Dementia Due to Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rascovsky, K.; Hodges, J.R.; Knopman, D.; Mendez, M.F.; Kramer, J.H.; Neuhaus, J.; van Swieten, J.C.; Seelaar, H.; Dopper, E.G.P.; Onyike, C.U.; et al. Sensitivity of Revised Diagnostic Criteria for the Behavioural Variant of Frontotemporal Dementia. Brain 2011, 134, 2456–2477. [Google Scholar] [CrossRef] [PubMed]
- Strong, M.J.; Abrahams, S.; Goldstein, L.H.; Woolley, S.; Mclaughlin, P.; Snowden, J.; Mioshi, E.; Roberts-South, A.; Benatar, M.; HortobáGyi, T.; et al. Amyotrophic Lateral Sclerosis—Frontotemporal Spectrum Disorder (ALS-FTSD): Revised Diagnostic Criteria. Amyotroph. Lateral Scler. Front. Degener. 2017, 18, 153–174. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Litvan, I.; Lang, A.E.; Bak, T.H.; Bhatia, K.P.; Borroni, B.; Boxer, A.L.; Dickson, D.W.; Grossman, M.; Hallett, M.; et al. Criteria for the Diagnosis of Corticobasal Degeneration. Neurology 2013, 80, 496–503. [Google Scholar] [CrossRef] [Green Version]
- Höglinger, G.U.; Respondek, G.; Stamelou, M.; Kurz, C.; Josephs, K.A.; Lang, A.E.; Mollenhauer, B.; Müller, U.; Nilsson, C.; Whitwell, J.L.; et al. Clinical Diagnosis of Progressive Supranuclear Palsy: The Movement Disorder Society Criteria. Mov. Disord. 2017, 32, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS Clinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Emre, M.; Aarsland, D.; Brown, R.; Burn, D.J.; Duyckaerts, C.; Mizuno, Y.; Broe, G.A.; Cummings, J.; Dickson, D.W.; Gauthier, S.; et al. Clinical Diagnostic Criteria for Dementia Associated with Parkinson’s Disease. Mov. Disord. 2007, 22, 1689–1707. [Google Scholar] [CrossRef]
- McKeith, I.G.; Boeve, B.F.; Dickson, D.W.; Halliday, G.; Taylor, J.-P.; Weintraub, D.; Aarsland, D.; Galvin, J.; Attems, J.; Ballard, C.G.; et al. Diagnosis and Management of Dementia with Lewy Bodies: Fourth Consensus Report of the DLB Consortium. Neurology 2017, 89, 88–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of Multiple Sclerosis: 2017 Revisions of the McDonald Criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Reilmann, R.; Leavitt, B.R.; Ross, C.A. Diagnostic Criteria for Huntington’s Disease Based on Natural History. Mov. Disord. 2014, 29, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Löe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Pignatelli, P.; Iezzi, L.; Pennese, M.; Raimondi, P.; Cichella, A.; Bondi, D.; Grande, R.; Cotellese, R.; Di Bartolomeo, N.; Innocenti, P.; et al. The Potential of Colonic Tumor Tissue Fusobacterium Nucleatum to Predict Staging and Its Interplay with Oral Abundance in Colon Cancer Patients. Cancers 2021, 13, 1032. [Google Scholar] [CrossRef] [PubMed]
- Waritani, T.; Chang, J.; McKinney, B.; Terato, K. An ELISA Protocol to Improve the Accuracy and Reliability of Serological Antibody Assays. MethodsX 2017, 4, 153–165. [Google Scholar] [CrossRef]
- Maruyama, H.; Masago, A.; Nambu, T.; Mashimo, C.; Takahashi, K.; Okinaga, T. Inter-Site and Interpersonal Diversity of Salivary and Tongue Microbiomes, and the Effect of Oral Care Tablets. F1000Research 2020, 9, 1477. [Google Scholar] [CrossRef]
- Yu, X.-L.; Chan, Y.; Zhuang, L.; Lai, H.-C.; Lang, N.P.; Keung Leung, W.; Watt, R.M. Intra-Oral Single-Site Comparisons of Periodontal and Peri-Implant Microbiota in Health and Disease. Clin. Oral. Implants Res. 2019, 30, 760–776. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Yeh, Y.-M.; Yu, H.-Y.; Chin, C.-Y.; Hsu, C.-W.; Liu, H.; Huang, P.-J.; Hu, S.-N.; Liao, C.-T.; Chang, K.-P.; et al. Oral Microbiota Community Dynamics Associated With Oral Squamous Cell Carcinoma Staging. Front. Microbiol. 2018, 9, 862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Aiuto, F.; Nibali, L.; Parkar, M.; Suvan, J.; Tonetti, M.S. Short-Term Effects of Intensive Periodontal Therapy on Serum Inflammatory Markers and Cholesterol. J. Dent. Res. 2005, 84, 269–273. [Google Scholar] [CrossRef]
- Almabadi, E.S.; Seymour, G.J.; Akhter, R.; Bauman, A.; Cullinan, M.P.; Eberhard, J. Reduction of HsCRP Levels Following an Oral Health Education Program Combined with Routine Dental Treatment. J. Dent. 2021, 110, 103686. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.J.; de Araújo, I.D.; da Rocha Alves, L.; da Silva, R.L.; Dos Santos Calderon, P.; Borges, B.C.; de Aquino Martins, A.R.; de Vasconcelos Gurgel, B.C.; Lins, R.D. Relationship of Porphyromonas Gingivalis and Alzheimer’s Disease: A Systematic Review of Pre-Clinical Studies. Clin. Oral. Investig. 2021, 25, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.-Q.; Richmond, R.C.; Chen, Y.; Mai, X.-M. Mixed Evidence for the Relationship between Periodontitis and Alzheimer’s Disease: A Bidirectional Mendelian Randomization Study. PLoS ONE 2020, 15, e0228206. [Google Scholar] [CrossRef]
- Wu, Z.; Nakanishi, H. Connection between Periodontitis and Alzheimer’s Disease: Possible Roles of Microglia and Leptomeningeal Cells. J. Pharmacol. Sci. 2014, 126, 8–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbayya, K.; Puthanakar, N.Y.; Naduwinmani, S.; Chidambar, Y.S. Association between Periodontitis and Alzheimer’s Disease. N Am. J. Med. Sci. 2015, 7, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Singhrao, S.K.; Olsen, I. Assessing the Role of Porphyromonas Gingivalis in Periodontitis to Determine a Causative Relationship with Alzheimer’s Disease. J. Oral. Microbiol. 2019, 11, 1563405. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, F.B.; Saito, M.T.; Matheus, F.C.; Prediger, R.D.; Yamada, E.S.; Maia, C.S.F.; Lima, R.R. Periodontitis and Alzheimer’s Disease: A Possible Comorbidity between Oral Chronic Inflammatory Condition and Neuroinflammation. Front. Aging Neurosci. 2017, 9, 327. [Google Scholar] [CrossRef] [PubMed]
- Olsen, I.; Singhrao, S.K. Is There a Link between Genetic Defects in the Complement Cascade and Porphyromonas Gingivalis in Alzheimer’s Disease? J. Oral. Microbiol. 2020, 12, 1676486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannarkat, G.T.; Boss, J.M.; Tansey, M.G. The Role of Innate and Adaptive Immunity in Parkinson’s Disease. J. Parkinsons Dis. 2013, 3, 493–514. [Google Scholar] [CrossRef] [Green Version]
- Dominy, S.S.; Lynch, C.; Ermini, F.; Benedyk, M.; Marczyk, A.; Konradi, A.; Nguyen, M.; Haditsch, U.; Raha, D.; Griffin, C.; et al. Porphyromonas Gingivalis in Alzheimer’s Disease Brains: Evidence for Disease Causation and Treatment with Small-Molecule Inhibitors. Sci. Adv. 2019, 5, eaau3333. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.-L.; Jiang, M.-J.; Gu, B.-B.; Wei, Y.-M.; Fan, S.-N.; Liao, W.; Zheng, Y.-Q.; Liao, S.-W.; Xiong, Y.; Li, Y.; et al. Tooth Loss as a Risk Factor for Dementia: Systematic Review and Meta-Analysis of 21 Observational Studies. BMC Psychiatry 2018, 18, 345. [Google Scholar] [CrossRef] [Green Version]
- Paganini-Hill, A.; White, S.C.; Atchison, K.A. Dentition, Dental Health Habits, and Dementia: The Leisure World Cohort Study. J. Am. Geriatr. Soc. 2012, 60, 1556–1563. [Google Scholar] [CrossRef]
- Abusleme, L.; Dupuy, A.K.; Dutzan, N.; Silva, N.; Burleson, J.A.; Strausbaugh, L.D.; Gamonal, J.; Diaz, P.I. The Subgingival Microbiome in Health and Periodontitis and Its Relationship with Community Biomass and Inflammation. ISME J. 2013, 7, 1016–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haffajee, A.D.; Cugini, M.A.; Tanner, A.; Pollack, R.P.; Smith, C.; Kent, R.L.; Socransky, S.S. Subgingival Microbiota in Healthy, Well-Maintained Elder and Periodontitis Subjects. J. Clin. Periodontol. 1998, 25, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Faveri, M.; Feres, M.; Shibli, J.A.; Hayacibara, R.F.; Hayacibara, M.M.; de Figueiredo, L.C. Microbiota of the Dorsum of the Tongue after Plaque Accumulation: An Experimental Study in Humans. J. Periodontol. 2006, 77, 1539–1546. [Google Scholar] [CrossRef]
- Hakeem, F.F.; Bernabé, E.; Sabbah, W. Association between Oral Health and Frailty: A Systematic Review of Longitudinal Studies. Gerodontology 2019, 36, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Dibello, V.; Lozupone, M.; Manfredini, D.; Dibello, A.; Zupo, R.; Sardone, R.; Daniele, A.; Lobbezoo, F.; Panza, F. Oral Frailty and Neurodegeneration in Alzheimer’s Disease. Neural. Regen. Res. 2021, 16, 2149–2153. [Google Scholar] [CrossRef]
- Kim, M.-S.; Oh, B.; Yoo, J.W.; Han, D.-H. The Association between Mastication and Mild Cognitive Impairment in Korean Adults. Medicine 2020, 99, e20653. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.C.G.; Lan, S.-J.; Hirano, H.; Lin, L.-M.; Hori, K.; Lin, C.-S.; Zwetchkenbaum, S.; Minakuchi, S.; Teng, A.Y.-T. Update and Review of the Gerodontology Prospective for 2020′s: Linking the Interactions of Oral (Hypo)-Functions to Health vs. Systemic Diseases. J. Dent. Sci. 2021, 16, 757–773. [Google Scholar] [CrossRef]
- Olsen, I.; Singhrao, S.K. Can Oral Infection Be a Risk Factor for Alzheimer’s Disease? J. Oral. Microbiol. 2015, 7, 29143. [Google Scholar] [CrossRef] [Green Version]
- Poole, S.; Singhrao, S.K.; Chukkapalli, S.; Rivera, M.; Velsko, I.; Kesavalu, L.; Crean, S. Active Invasion of Porphyromonas Gingivalis and Infection-Induced Complement Activation in ApoE-/-Mice Brains. J. Alzheimers Dis. 2015, 43, 67–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Nguyen, K.-A.; Potempa, J. Dichotomy of Gingipains Action as Virulence Factors: From Cleaving Substrates with the Precision of a Surgeon’s Knife to a Meat Chopper-like Brutal Degradation of Proteins. Periodontol. 2000 2010, 54, 15–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajishengallis, G.; Krauss, J.L.; Liang, S.; McIntosh, M.L.; Lambris, J.D. Pathogenic Microbes and Community Service through Manipulation of Innate Immunity. Adv. Exp. Med. Biol. 2012, 946, 69–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Variables | ND Patients (n = 21) | No-ND Patients (n = 28) | HC (n = 29) |
|---|---|---|---|
| Age, years (mean ± SD) | 70.6 ± 13.4 | 67.6 ± 19.8 | 56.1 ± 12.8 |
| Sex (% male) | 66.7 | 28.6 | 44.8 |
| Teeth number (mean ± SD) | 15.8 ± 8.8 | 14.6 ± 10.2 | 22.5 ± 6.3 |
| Plaque index (mean ± SD) | 2.1 ± 0.9 (n = 8) | 2.0 ± 0.3 (n = 8) | 1.2 ± 0.6 |
| Gingival index (mean ± SD) | 1.5 ± 0.8 (n = 8) | 1.1 ± 0.5 (n = 8) | 0.6 ± 0.5 |
| Presence of gingivitis (% of pts) | 88 | 69 | 52 |
| Lingual patina index (mean ± SD) | 1.6 ± 1.3 (n = 16) | 0.8 ± 0.9 (n = 25) | 0.4 ± 0.5 (n = 14) |
| Presence of oral infection (% of pts) | 82.4 (n = 17) | 64 (n = 25) | 41.4 |
| Oral hygiene index (mean ± SD) | 0.2 ± 0.4 (n = 17) | 0.4 ± 0.6 (n = 25) | 1.2 ± 0.6 |
| Presence of fissured tongue (% of pts) | 5.9 (n = 17) | 7.7 (n = 26) | 1 |
| Number of fixed prosthesis (mean ± SD) | 0.3 ± 0.7 | 0.4 ± 0.7 | 0.4 ± 0.6 |
| Number of removable denture (mean ± SD) | 0.5 ± 0.7 | 0.5 ± 0.8 | 0.2 ±0.5 |
| Smoker (% of pts) | 0 | 11.1 (n = 27) | 20.7 |
| Former smoker (% of pts) | 28.6 | 11.1 (n = 27) | 20.7 |
| Main Effect | Post-Hoc ND vs. no-ND | Post-Hoc ND vs. HC | Post-Hoc No-ND vs. HC | |
|---|---|---|---|---|
| Age (mean ± st.dev.) | F = 6.200, p = 0.003 | p = 1 | p = 0.006 | p = 0.022 |
| Sex | p = 0.031 | p = 0.025 | p = 0.384 | p = 0.661 |
| Teeth number | F = 6.866, p = 0.002 | p = 1 | p = 0.022 | p = 0.003 |
| Plaque index | p = 0.001 | p = 1 | p = 0.013 | p = 0.004 |
| Gingival index | p = 0.005 | p = 1 | p = 0.008 | p = 0.155 |
| Presence of gingivitis | p = 0.040 | p = 0.598 | p = 0.035 | p = 0.516 |
| Lingual patina index | p = 0.015 | p = 0.131 | p = 0.016 | p = 0.607 |
| Presence of oral infection | p = 0.006 | p = 0.704 | p = 0.004 | p = 0.050 |
| Oral hygiene index | p = 0.001 | p = 0.967 | p = 0.001 | p = 0.001 |
| Presence of fissured tongue | p = 0.675 | |||
| Number of fixed prosthesis | p = 0.590 | |||
| Number of removable denture | p = 0.132 | |||
| Smoker | p = 0.082 | |||
| Former smoker | p = 0.315 |
| Patients (%) | ND (n = 21) | No-ND (n = 28) | Statistical Results |
|---|---|---|---|
| Systemic Inflammation | 56 | 52 | Χ2 = 0.06 p = 0.80 |
| Cholesterol ratio > cut-off | 20 | 44 | Χ2 = 1.53 p = 0.22 |
| High triglycerides | 20 | 38 | Χ2 = 0.89 p = 0.35 |
| Hypertension | 39 | 56 | Χ2 = 1.20 p = 0.27 |
| Diabetes | 22 | 26 | χ2 = 0.08 p = 0.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franciotti, R.; Pignatelli, P.; Carrarini, C.; Romei, F.M.; Mastrippolito, M.; Gentile, A.; Mancinelli, R.; Fulle, S.; Piattelli, A.; Onofrj, M.; et al. Exploring the Connection between Porphyromonas gingivalis and Neurodegenerative Diseases: A Pilot Quantitative Study on the Bacterium Abundance in Oral Cavity and the Amount of Antibodies in Serum. Biomolecules 2021, 11, 845. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11060845
Franciotti R, Pignatelli P, Carrarini C, Romei FM, Mastrippolito M, Gentile A, Mancinelli R, Fulle S, Piattelli A, Onofrj M, et al. Exploring the Connection between Porphyromonas gingivalis and Neurodegenerative Diseases: A Pilot Quantitative Study on the Bacterium Abundance in Oral Cavity and the Amount of Antibodies in Serum. Biomolecules. 2021; 11(6):845. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11060845
Chicago/Turabian StyleFranciotti, Raffaella, Pamela Pignatelli, Claudia Carrarini, Federica Maria Romei, Martina Mastrippolito, Antonella Gentile, Rosa Mancinelli, Stefania Fulle, Adriano Piattelli, Marco Onofrj, and et al. 2021. "Exploring the Connection between Porphyromonas gingivalis and Neurodegenerative Diseases: A Pilot Quantitative Study on the Bacterium Abundance in Oral Cavity and the Amount of Antibodies in Serum" Biomolecules 11, no. 6: 845. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11060845