
Examination of the Fractalkine and Fractalkine Receptor Expression in Fallopian Adenocarcinoma Reveals Differences When Compared to Ovarian Carcinoma

Abstract
:1. Introduction
2. Results
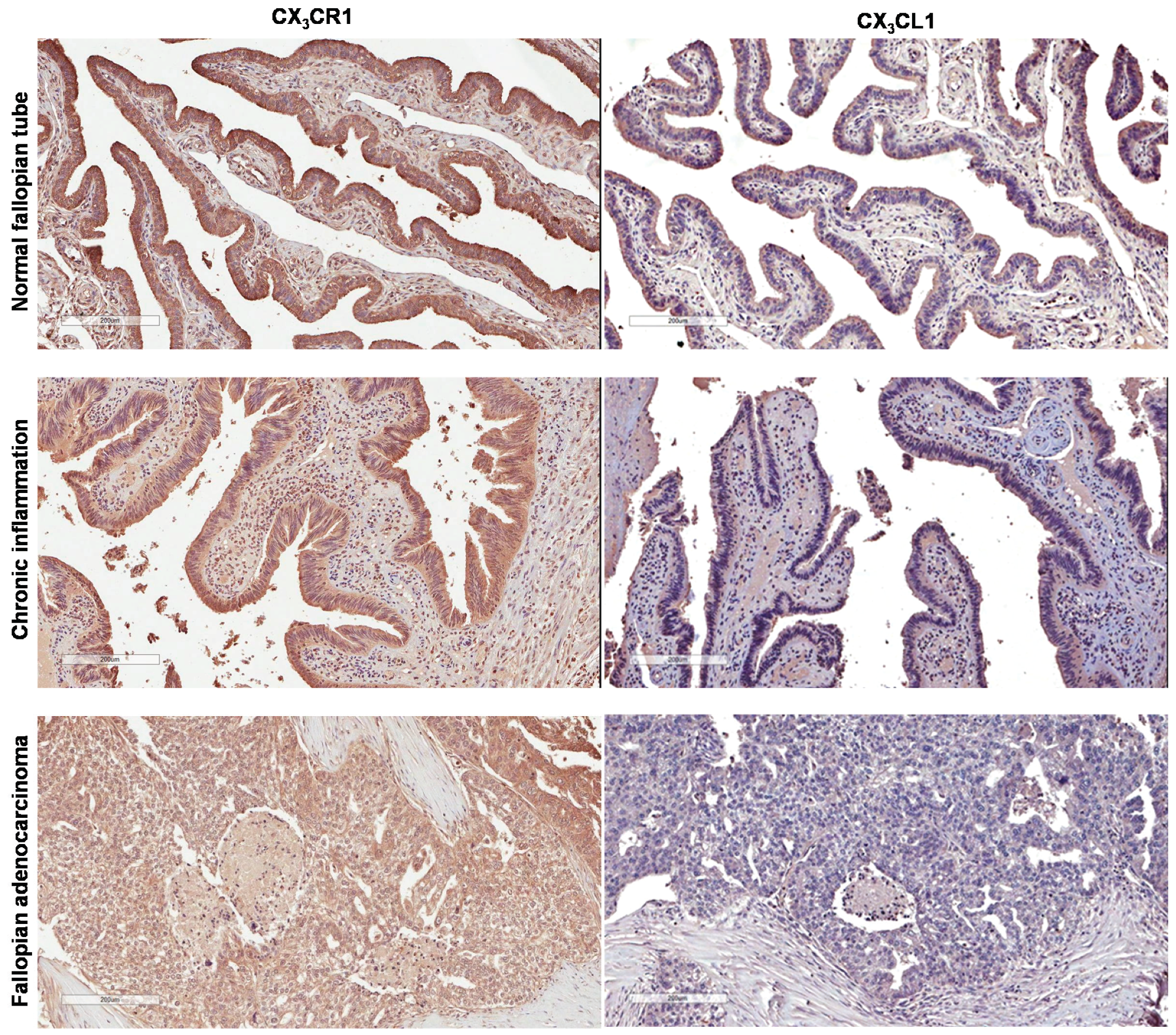
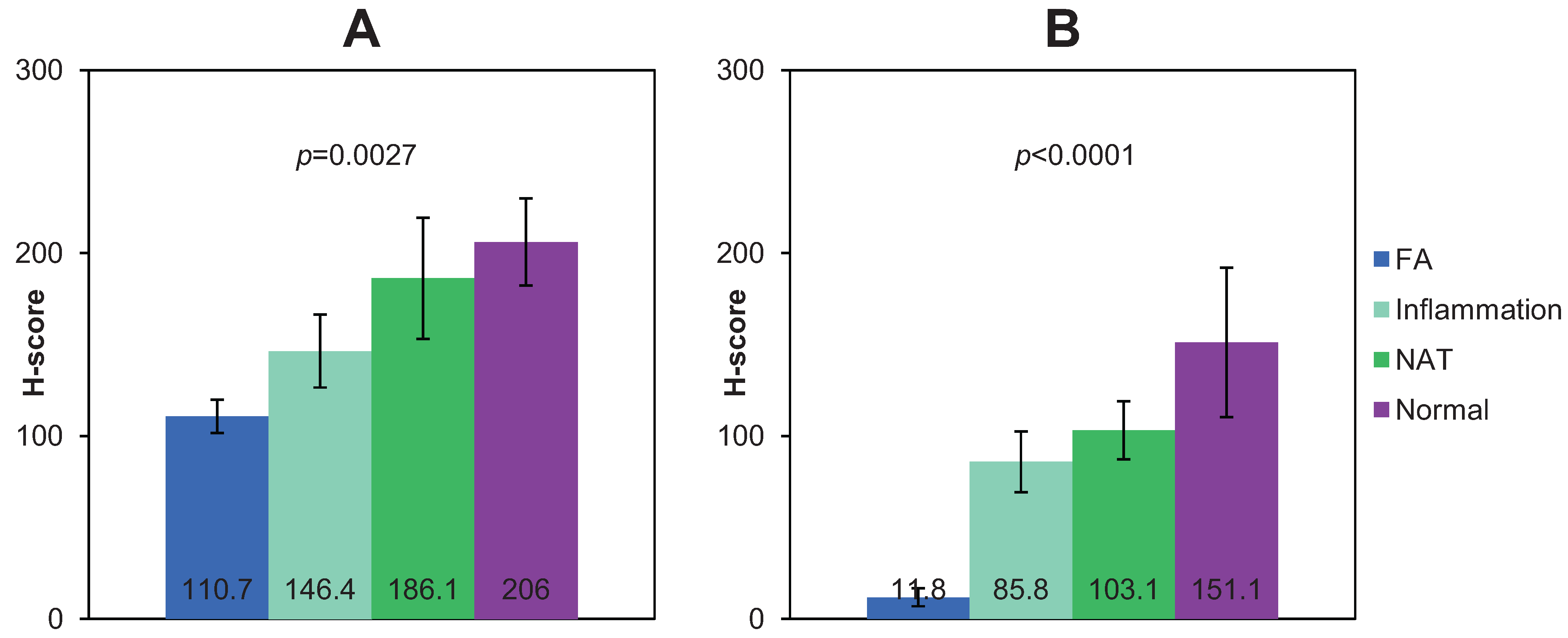
2.1. Expression of CX3CR1 in Normal and Pathologic Fallopian Epithelium and Fallopian Carcinoma


2.2. Expression of CX3CL1 in Normal and Pathologic Fallopian Epithelium and Fallopian Carcinoma
2.3. Patterns of CX3CL1 and CX3CR1 Expression Are Different between Normal Cells of Origin and Cancerous Cells in Ovarian and Fallopian Carcinomas

{kind=link}
{kind=link}
| Organ Site | Normal Epithelium | Fallopian Epithelium with Chronic Inflammation | Cancer |
|---|---|---|---|
| Expression of CX3CR1 | |||
| Fallopian tube | Positive ([38] and present study) Average h-score = 206 | Positive (present study) Average h-score = 146.1 | Positive (present study) Average h-score = 110.7 |
| Ovary | Negative [33] | Positive [33] | |
| Expression of CX3CL1 | |||
| Fallopian tube | Positive ([34,38] and present study) Average h-score = 151.1 | Negative (present study) Average h-score = 85.6 | Negative (present study) Average h-score = 11.8 |
| Ovary | Positive [34] | Positive [34] | |
3. Discussion
4. Experimental Section
4.1. Materials
4.2. Immunohistochemistry
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kalampokas, E.; Kalampokas, T.; Tourountous, I. Primary fallopian tube carcinoma. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 169, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Koo, Y.J.; Im, K.S.; Kwon, Y.S.; Lee, I.H.; Kim, T.J.; Lim, K.T.; Lee, K.H.; Shim, J.U.; Mok, J.E. Primary fallopian tube carcinoma: A clinicopathological analysis of a rare entity. Int. J. Clin. Oncol. 2011, 16, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Pectasides, D.; Pectasides, E.; Economopoulos, T. Fallopian tube carcinoma: A review. Oncologist 2006, 11, 902–912. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.L.; Wike, J.M.; Foster, S.L.; Michaud, F. The incidence of primary fallopian tube cancer in the United States. Gynecol. Oncol. 2007, 107, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Fathalla, M.F. Incessant ovulation—A factor in ovarian neoplasia? Lancet 1971. [Google Scholar] [CrossRef]
- Gondos, B. Surface epithelium of the developing ovary. Possible correlation with ovarian neoplasia. Am. J. Pathol. 1975, 81, 303–321. [Google Scholar] [PubMed]
- Bahar-Shany, K.; Brand, H.; Sapoznik, S.; Jacob-Hirsch, J.; Yung, Y.; Korach, J.; Perri, T.; Cohen, Y.; Hourvitz, A.; Levanon, K. Exposure of fallopian tube epithelium to follicular fluid mimics carcinogenic changes in precursor lesions of serous papillary carcinoma. Gynecol. Oncol. 2014, 132, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Dubeau, L. The cell of origin of ovarian epithelial tumours. Lancet Oncol. 2008, 9, 1191–1197. [Google Scholar] [CrossRef]
- Dubeau, L.; Drapkin, R. Coming into focus: The nonovarian origins of ovarian cancer. Ann. Oncol. 2013, S24, viii28–viii35. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J. Origin and molecular pathogenesis of ovarian high-grade serous carcinoma. Ann. Oncol. 2013, S24, x16–x21. [Google Scholar] [CrossRef] [PubMed]
- Lengyel, E.; Fleming, S.; McEwen, K.A.; Montag, A.; Temkin, S.M. Serial sectioning of the fallopian tube allows for improved identification of primary fallopian tube carcinoma. Gynecol. Oncol. 2013, 129, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Perets, R.; Wyant, G.A.; Muto, K.W.; Bijron, J.G.; Poole, B.B.; Chin, K.T.; Chen, J.Y.; Ohman, A.W.; Stepule, C.D.; Kwak, S.; et al. Transformation of the fallopian tube secretory epithelium leads to high-grade serous ovarian cancer in Brca;Tp53;Pten models. Cancer Cell 2013, 24, 751–765. [Google Scholar] [CrossRef] [PubMed]
- Piek, J.M.; Verheijen, R.H.; Kenemans, P.; Massuger, L.F.; Bulten, H.; van Diest, P.J. BRCA1/2-related ovarian cancers are of tubal origin: A hypothesis. Gynecol. Oncol. 2003. [Google Scholar] [CrossRef]
- Vang, R.; Shih Ie, M.; Kurman, R.J. Fallopian tube precursors of ovarian low- and high-grade serous neoplasms. Histopathology 2013, 62, 44–58. [Google Scholar] [CrossRef] [PubMed]
- Hariprasad, P.; Hariprasad, S.; Srinivas, T.; Shetty, K.J. Primary bilateral fallopian tube carcinoma the report of a single case with review of the literature. J. Clin. Diagn. Res. 2013, 7, 930–932. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Xu, N.; Fang, W.; Zhao, P.; Mao, C.; Zheng, Y.; Mou, H. Complete remission of platinum-refractory primary Fallopian tube carcinoma with third-line gemcitabine plus cisplatin: A case report and review of the literature. Oncol. Lett. 2013, 5, 1601–1604. [Google Scholar] [PubMed]
- Yokoyama, Y.; Futagami, M.; Fujimoto, T.; Terada, Y.; Takatori, E.; Sugiyama, T.; Otsuki, T.; Yaegashi, N.; Kojimahara, T.; Kurachi, H.; et al. Investigation of the clinicopathological features of fallopian tube malignancy. Oncol. Rep. 2013, 30, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Baekelandt, M.; Jorunn Nesbakken, A.; Kristensen, G.B.; Trope, C.G.; Abeler, V.M. Carcinoma of the fallopian tube. Cancer 2000, 89, 2076–2084. [Google Scholar] [CrossRef]
- Gurney, H.; Murphy, D.; Crowther, D. The management of primary fallopian tube carcinoma. Br. J. Obstet. Gynaecol. 1990, 97, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Pectasides, D.; Pectasides, E.; Papaxoinis, G.; Andreadis, C.; Papatsibas, G.; Fountzilas, G.; Pliarchopoulou, K.; Macheras, A.; Aravantinos, G.; Economopoulos, T. Primary fallopian tube carcinoma: Results of a retrospective analysis of 64 patients. Gynecol. Oncol. 2009, 115, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Piura, B.; Rabinovich, A. Primary carcinoma of the fallopian tube: Study of 11 cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 91, 169–175. [Google Scholar] [CrossRef]
- Sama, A.R.; Schilder, R.J. Refractory fallopian tube carcinoma—Current perspectives in pathogenesis and management. Int. J. Womens Health 2014, 6, 149–157. [Google Scholar] [PubMed]
- Takeshima, N.; Hasumi, K. Treatment of fallopian tube cancer. Review of the literature. Arch. Gynecol. Obstet. 2000, 264, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.N.; Moxley, K.M.; Fader, A.N.; Axtell, A.E.; Rocconi, R.P.; Abaid, L.N.; Cass, I.A.; Rose, P.G.; Leath, C.A., 3rd; Rutledge, T.; et al. Serous fallopian tube carcinoma: A retrospective, multi-institutional case-control comparison to serous adenocarcinoma of the ovary. Gynecol. Oncol. 2007, 107, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Abaid, L.N.; Micha, J.P.; Rettenmaier, M.A.; Brown, J.V.; Mendivil, A.A.; Lopez, K.L.; Goldstein, B.H. A phase II study of modified dose-dense paclitaxel and every 4-week carboplatin for the treatment of advanced-stage primary epithelial ovarian, fallopian tube, or peritoneal carcinoma. Cancer Chemother. Pharmacol. 2013, 72, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, M.; Leblanc, E.; Filleron, T.; Morice, P.; Darai, E.; Classe, J.M.; Ferron, G.; Stoeckle, E.; Pomel, C.; Vinet, B.; et al. Maximal cytoreduction in patients with FIGO stage IIIC to stage IV ovarian, fallopian, and peritoneal cancer in day-to-day practice: A Retrospective French Multicentric Study. Int. J. Gynecol. Cancer 2012, 22, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.P.; Sill, M.; Shahin, M.S.; Powell, M.; DiSilvestro, P.; Landrum, L.M.; Gaillard, S.L.; Goodheart, M.J.; Hoffman, J.; Schilder, R.J. A phase II evaluation of AMG 102 (rilotumumab) in the treatment of persistent or recurrent epithelial ovarian, fallopian tube or primary peritoneal carcinoma: A Gynecologic Oncology Group study. Gynecol. Oncol. 2014, 132, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Mendivil, A.A.; Micha, J.P.; Brown, J.V., 3rd; Rettenmaier, M.A.; Abaid, L.N.; Lopez, K.L.; Goldstein, B.H. Increased incidence of severe gastrointestinal events with first-line paclitaxel, carboplatin, and vorinostat chemotherapy for advanced-stage epithelial ovarian, primary peritoneal, and fallopian tube cancer. Int. J. Gynecol. Cancer 2013, 23, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Safra, T.; Berman, T.; Yachnin, A.; Bruchim, I.; Meirovitz, M.; Barak, F.; Atlas, I.; Levy, T.; Rosengarten, O.S. Weekly topotecan for recurrent ovarian, fallopian tube and primary peritoneal carcinoma: Tolerability and efficacy study--the Israeli experience. Int. J. Gynecol. Cancer 2013, 23, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Schilder, R.J.; Sill, M.W.; Lankes, H.A.; Gold, M.A.; Mannel, R.S.; Modesitt, S.C.; Hanjani, P.; Bonebrake, A.J.; Sood, A.K.; Godwin, A.K.; et al. A phase II evaluation of motesanib (AMG 706) in the treatment of persistent or recurrent ovarian, fallopian tube and primary peritoneal carcinomas: A Gynecologic Oncology Group study. Gynecol. Oncol. 2013, 129, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F. Cancer and the chemokine network. Nat. Rev. Cancer 2004, 4, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Muralidhar, G.G.; Barbolina, M.V. Chemokine receptors in epithelial ovarian cancer. Int. J. Mol. Sci. 2013, 15, 361–376. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Rooper, L.; Xie, J.; Kajdacsy-Balla, A.A.; Barbolina, M.V. Fractalkine receptor CX(3)CR1 is expressed in epithelial ovarian carcinoma cells and required for motility and adhesion to peritoneal mesothelial cells. Mol. Cancer Res. 2012, 10, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Gaudin, F.; Nasreddine, S.; Donnadieu, A.C.; Emilie, D.; Combadiere, C.; Prevot, S.; Machelon, V.; Balabanian, K. Identification of the chemokine CX3CL1 as a new regulator of malignant cell proliferation in epithelial ovarian cancer. PLoS ONE 2011, 6, e21546. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Bacon, K.B.; Li, L.; Garcia, G.E.; Xia, Y.; Lo, D.; Thompson, D.A.; Yamamoto, T.; Siani, M.A.; Harrison, J.K.; et al. In vivo inhibition of CC and CX3C chemokine-induced leukocyte infiltration and attenuation of glomerulonephritis in Wistar-Kyoto (WKY) rats by vMIP-II. J. Exp. Med. 1998, 188, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.N.; Zujovic, V.; Harrison, J.K. Viral macrophage inflammatory protein-II and fractalkine (CX3CL1) chimeras identify molecular determinants of affinity, efficacy, and selectivity at CX3CR1. Mol. Pharmacol. 2004, 66, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Dorgham, K.; Ghadiri, A.; Hermand, P.; Rodero, M.; Poupel, L.; Iga, M.; Hartley, O.; Gorochov, G.; Combadiere, C.; Deterre, P. An engineered CX3CR1 antagonist endowed with anti-inflammatory activity. J. Leukoc. Biol. 2009, 86, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Shimoya, K.; Temma, K.; Kimura, T.; Tsujie, T.; Shioji, M.; Wasada, K.; Fukui, O.; Hayashi, S.; Kanagawa, T.; et al. Expression of fractalkine in the Fallopian tube and of CX3CR1 in sperm. Hum. Reprod. 2004, 19, 409–414. [Google Scholar] [CrossRef] [PubMed]
- McCarty, K.S., Jr.; Szabo, E.; Flowers, J.L.; Cox, E.B.; Leight, G.S.; Miller, L.; Konrath, J.; Soper, J.T.; Budwit, D.A.; Creasman, W.T.; et al. Use of a monoclonal anti-estrogen receptor antibody in the immunohistochemical evaluation of human tumors. Cancer Res. 1986, 46, 4244S–4248S. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gurler, H.; Macias, V.; Kajdacsy-Balla, A.A.; Barbolina, M.V. Examination of the Fractalkine and Fractalkine Receptor Expression in Fallopian Adenocarcinoma Reveals Differences When Compared to Ovarian Carcinoma. Biomolecules 2015, 5, 3438-3447. https://0-doi-org.brum.beds.ac.uk/10.3390/biom5043438
Gurler H, Macias V, Kajdacsy-Balla AA, Barbolina MV. Examination of the Fractalkine and Fractalkine Receptor Expression in Fallopian Adenocarcinoma Reveals Differences When Compared to Ovarian Carcinoma. Biomolecules. 2015; 5(4):3438-3447. https://0-doi-org.brum.beds.ac.uk/10.3390/biom5043438
Chicago/Turabian StyleGurler, Hilal, Virgilia Macias, Andre A. Kajdacsy-Balla, and Maria V. Barbolina. 2015. "Examination of the Fractalkine and Fractalkine Receptor Expression in Fallopian Adenocarcinoma Reveals Differences When Compared to Ovarian Carcinoma" Biomolecules 5, no. 4: 3438-3447. https://0-doi-org.brum.beds.ac.uk/10.3390/biom5043438