1. Introduction
Primary and secondary education students spend about a third of their life attending school, which suggests that the school environment impacts significantly on their lives. Therefore, schools are expected to be places of promoting emotional well-being, and where early signs of changes to students’ behaviour and of mental distress can be spotted [
1]. Schools are well placed to perform an essential role to safeguard children. For example, they are expected to develop robust practices to identify and act on signs of abuse (and neglect), have a good vetting process in place for adults working with children, and train members of staff to keep their knowledge up to date on regulations and safeguarding policy. Another aspect is to establish trust with children to feel confident to seek advice and report to members of the team should they have a worry.
In relation to children and young people, the promotion of welfare in schools is regularly inspected. For instance, the Office for Standards in Education (Ofsted) in the UK publishes safeguarding and inspectors’ responsibilities including essential requirements such as enforcing the Department for Education (DfE) statuary guidance for schools [
2]. It also makes references to other guidelines, including “keeping children safe in education,” “working together to safeguard children,” and “prevent duty guidance for England and Wales” [
2]. Consequences from regular inspections affect schools’ ratings at a national level and trigger follow-up processes to promote compliance and adequate safeguarding.
Safeguarding action plans aim to protect young people from problems ranging from neglect to abuse (sexual, emotional, physical). In this study, we focus on bullying and physical abuse targeting young people with disabilities and chronic conditions. Recent studies show that the impact of bullying can be severe, with health implications on these vulnerable groups [
3,
4]. Moreover, there is evidence suggesting they were victimised due to their visible signs of disabilities, as discussed in refs. [
5,
6]. Bullying is a fixated behaviour targeting a victim; it is defined as an aggressive act carried out by an individual or by a group repeatedly. It includes threats and abuse to intimidate or dominate the victims. This dangerous behaviour has an essential characteristic around the perception of power imbalance, which can either be physical or social [
7]. Bullying can have a devastating impact on victims’ psychological well-being and psychosocial functioning. It can be persistent and include a stalking behaviour, which is an abnormal behaviour characterised by persistence, fixated threats and intrusions by the “offender” towards the “victim” resulting in fear and distress.
Current intervention mechanisms are still problematic with an area for improvement. Despite increased awareness of the impact of bullying, recent studies report a high prevalence in schools. A systematic review [
8] and meta-analysis to estimate prevalence among Australian children reported the 12-month prevalence of physical bullying victimisation at 15.17% with a lifetime prevalence of 25.27%. The content of 463 student surveys representing middle schools across the Southern United States shows 37% of students were bullied either physically or online [
9]. In China, the incidents of bullying reported were 26.10% [
10]. In the UK, a survey by the Organisation for Economic Co-operation and Development (OECD) (Teachers and School Leaders 2018 survey) covering around 250,000 teachers from 48 industrialised countries showed that in 2018 [
2] 29% of English secondary schools received reports of bullying, 29.4% in Finland, 27.0% in Sweden, 27.2% in France, and 25.6% in Bulgaria.
In this study we offer a two-fold contribution. Firstly, we design a new layer of protection for medically vulnerable students by exploiting the characteristics of Internet of Medical Things (IoMT) data from medical sensors and wearable devices already attached to students due to chronic conditions to add a new layer of protection. IoMT data can be used to detect stress and incidents of victimisation. In this regard, we propose and discuss how a private permission blockchain deployment in established IoMT infrastructures can support safeguarding with timely reporting of incidents (near real time) while regulating data sharing between stakeholders (e.g., schools and medical centres). The role of blockchain is inevitable to keep a track record of changes that is also trusted (e.g., complies with the rules of digital evidence). We argue that this novel approach to supporting the well-being of vulnerable victims of bullying and physical abuse is a key enabled to support fundamental safeguarding principles, namely, empowerment, prevention, proportionality, protection, partnership, and accountability.
Secondly, we appreciate that stakeholders with no existing infrastructure require feasibility studies. Therefore, the second contribution is manifested through the development of an emulator to demonstrate the performance and capabilities of the proposed architecture given different loads of sensor-generated data. We argue to the suitability of this emulator for schools to conduct feasibility studies to address sensor data with disruptive data processing and management technologies. The emulator takes under consideration organisational and functional characteristics of the IoMT sensors, network-related metrics, and data attributes to better visualise inhibitors to the successful integration of these environments with disruptive technologies such as blockchain. The emulator acts as a standalone tool that can be utilised to test and verify the scalability and interoperability of sensors with distributed data management and processing structures.
In the remaining part of this paper, we cover background and related work in
Section 2 and propose a blockchain-based safeguarding model for schools in
Section 3. The integration of blockchain with IoMT data for the model is fully investigated in
Section 4, including challenges and consensus mechanisms. In
Section 5, we present the design requirements of our experiments and emulator. We also test different consensus mechanisms to investigate the efficacy of a private permissioned blockchain in the management and processing of data generated by medical sensors.
Section 5 discusses the main results and analysis from our experiments, and
Section 6 concludes our work.
2. Background and Related Work
2.1. Bullying and Its Impact on People with Disabilities and Chronic Conditions
Bullying is an aggressive intentional act that is verbally, physically, or socially hurtful and is repeated over time directly or indirectly [
11,
12,
13]. In bullying experiences, there is a perceived power imbalance between the bully and the victim, thus, it can also be described as using power to control others and cause distress [
13]. Bullying is a local and international issue that is consistently associated with a negative impact on the victims [
3,
14,
15]. In Sweden, a study of 5248 schoolchildren reported that 14% experienced bullying in the past two months. The reported impact was severe, such as poor general health, physical health problems (headache, migraine, stomach ache, tinnitus, musculoskeletal pain), mental health problems (insomnia, anxiety, worry, depression), and self-injurious behaviour [
13].
The impact of bullying is potentially more severe on vulnerable groups such as people with disabilities and chronic conditions [
3,
4]. In Canada, individuals who have epilepsy were victimised compared to their peers in schools. Likewise, young people with chronic kidney disease were victimised [
5]. Sentenac et al. [
6] studied 12,048 cases of victimization targeting students aged between 11 and 14 years old in France and Ireland. Findings showed that young people living with diabetes, arthritis, cerebral palsy, and allergies were frequently targeted by other children. The prevalence in Ireland was 20.6% and 16.6% in France [
6]. Other documented targeted conditions include attention deficit hyperactivity disorder (ADHD) [
16], autism [
17], hearing impairment or deafness [
18], and chronic tic disorders [
19]. The underlying causes were “being different” [
20,
21] or having a different lifestyle as part of the self-management in conditions such as diabetes and asthma [
22]. Nonetheless, the impact of such conditions is potentially devastating and has immediate and long-term medical manifestation [
3].
Furthermore, cyberbullying is a form of bullying that occurs when such experiences take place partially or fully in cyberspace, such as bullying through email, instant messaging, chatrooms, or webpages, or by receiving digital images or messages to a phone [
3,
11]. Cyberbullying could take the form of offensive messages sent to a target (harassment), an online fight between two people, posting personal data of the target online without permission, blocking a person from a social list, impersonation, stalking, or sexting (sending nude pictures of the target without their knowledge or consent) [
23]. Cyberbullying is increasingly reported with a reported prevalence of up to 41% among children with long-term conditions [
24]. It causes no less impact compared to its offline counterpart, such as subjective health complaints [
24], which include a group of general symptoms indicating health status, including headache, feeling low, being irritable, nervousness, sleep, or dizziness. These symptoms were significantly higher in cases of online harassment, especially among female victims [
24,
25]. Other impacts include post-traumatic stress symptoms [
26], depression and anxiety [
27], and suicidality and self-harm [
28]. Hence, often cyberbullying and bullying are researched together [
13].
2.2. IoMT Applications
The Internet of Medical Things (IoMT) has infiltrated almost every field of modern healthcare that seamlessly integrates with large-scale automation systems and parallel computation platforms. Sensors and actuators in these environments have naturally evolved into highly distributed applications that computerise processes in e-health services offered and general supply-chain management. At the same time, they proved to better link physical properties with digital controls [
29]. They are provided with unique identifiers and the ability to sense, process, and make decisions based on a data stream externally or internally processed. This decision-making capability is often underpinned by the complete absence of human interference or interaction. Mohammed et al. [
30] suggested a smart healthcare monitoring system (SW-SHMS) to collect data through wearable sensors, which are collected and stored in the cloud for further analysis. In this way, phycological disorders may be spotted and transmitted to a user’s doctor. Zualkernan et al. [
31] proposed the use of a mobile phone keyboard to monitor emotions and moods. This is done by testing users’ typing styles, texting speeds, the time lapses between presses, and even their physical shaking; it is then measured using an accelerometer and a multi-response linear regression machine learning algorithm. Lane et al. [
32] and Hicks et al. [
33] developed applications called “BeWell” and “AndWellness” for use in android smartphones to promote better health by tracking social and mental activities, including the quality of sleep and social interactions and by providing intelligent feedback.
The main objectives of the referred applications are to sense, acquire, and analyse (process) data, which can be used to detect in time the students who need further support. Then the main issue that arises is the secured storage of the sensitive collected health data. The answers to the above questions are (i) the IoMT, which allows smartphones or other devices to use and manage the connection to the Internet; (ii) the cloud services that provide an efficient and effective framework for storing and processing big amounts of data, providing Infrastructure as a Service; and (iii) blockchain technology, which allows the security hardening of sensitive and heavy volumes of data. Applying blockchain technologies to protect data from healthcare applications is getting increasing research focus.
2.3. Blockchain Technology for Healthcare Information
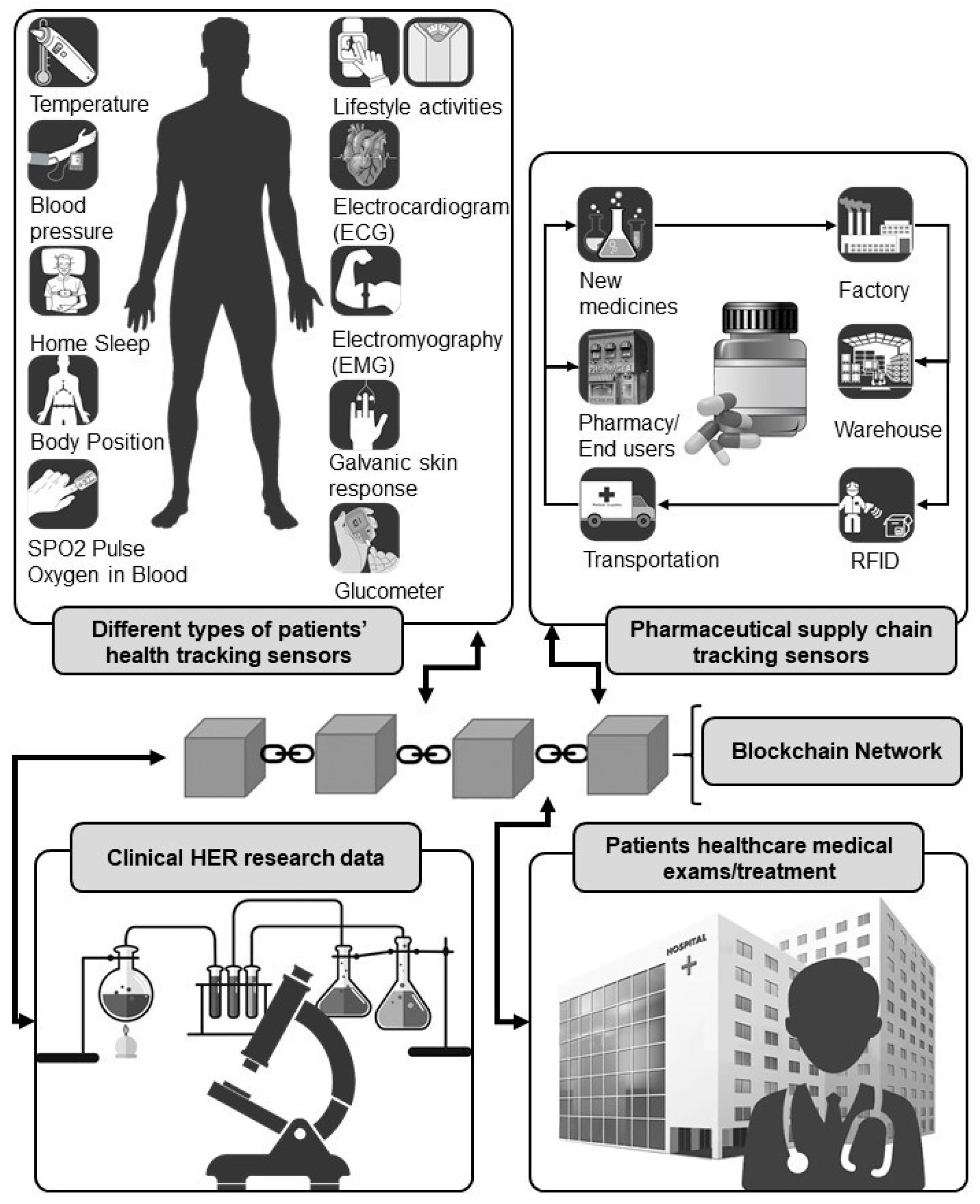
Specific properties of blockchain technology have already been used to address, efficiently and with interoperability, healthcare information and product transactions [
34]. These areas include pharmaceuticals, e-health, and clinical research. For instance, pharmaceutical companies can track drug journeys more swiftly and securely, and medical equipment supply chains can be more streamlined, enabling buyers to acquire them more efficiently and securely. In addition, patients, doctors, clinical researchers, and healthcare providers can share electronic health records both quickly and with significant advantages in privacy, security, safety, transparency, and data integrity. Thus, in contrast to conventional data-management technologies, where the patients’ data are placed under direct control by a central server, a blockchain decentralised system firmly establishes patient ownership by putting them “in the driving seat” for managing and controlling their own data (see
Figure 1). This “smart” and “citizen-based” interoperability approach for health records enables health data exchange among health information systems and patients. It also offers inherent provenance and integrity of the data, as well as great traceability and support for seamless data sharing that can eliminate duplication, errors, and inconsistencies compared to traditional centralised data storage.
2.4. Blockchain for Sharing Electronic Health Records (EHR)
Electronic health records (EHR), which are created and maintained throughout a patient’s lifetime by all providers, are vital sources of intelligence, the sharing of which is essential for operating a quality service [
35]. However, in their current, fragmentary form, they are not easily accessed by patients. Blockchain, on the other hand, based on a combination of telemedicine and precision medicine, would make collaborative decision-making between professionals and patients possible. Using a private blockchain Ethereum platform with a Practical Byzantine Fault Tolerance (PBFT) consensus mechanism, ref.[
36] created a system where patients can store their lifestyle data derived from their mobile sensors as new events in the database. This Health Insurance Portability and Accountability Act (HIPAA)—compliant system records and monitors real-time interventions, notifies patients and professionals, and identifies initiators. The authors believe this resolves many remote monitoring security vulnerabilities. In contrast, ref. [
37] proposed a public blockchain network based on Proof-of-Importance (PoI) protocol to ensure that medical records exist and have not been tampered with and that an off-chain cloud storage-based framework exists to manage, share, and record patients’ data, which is subject to a hashing algorithm to ensure integrity. Thereafter, the data is available to the patient and cannot be accessed by unauthorised parties. Ref. [
38] also developed a public blockchain platform named BlockChain platform for Healthcare Information Exchange (BloCHIE) that supports two Proof of Work (PoW) algorithms—the first incorporates an electronic medical record from the relevant institution signed by both institution and patient, and the second consists of personal data derived from the patient’s sensors. To meet both authenticity and privacy requirements, the authors reinforced the platform with on-chain and off-chain verification procedures.
2.5. Blockchain Applications in Healthcare
Other examples of blockchain applications in healthcare include clinical research and pharmaceuticals. Blockchain offers the pharmaceutical supply chain the ability to preserve the authenticity and condition of drugs and mitigate against counterfeiting by tracing and tracking pharmaceutical products throughout their life cycle [
39]. Information such as temperature and humidity conditions of the medicines are also monitored and stored on the blockchain platform. Ref. [
40] also proposed a pharmaceutical turnover control system for monitoring the transportation of the drugs based on a private blockchain network administered by a state-controlled agency. As it is a Hyperledger Fabric-based network, all nodes have different roles in the system. Not all “endorser peers” nodes, though, are directly involved in the execution of smart contracts. While the end-user “client peers” place their orders, “Endorser peers” validate and execute them; however, special “nodes-guarantors” are required to execute the code of smart contracts. Credibility risks in collecting clinical trial data can be eliminated with the use of blockchain technology. It thus ensures that its analysis of clinical research complies with the pre-specified plans. Furthermore, threats to privacy, integrity, sharing, record keeping, and patient enrolment can be avoided [
41].
Ref. [
42] developed a pubic blockchain using a Proof of Capacity (PoC) web-based interface named BlockTrial, which allows users to run trial-related “smart contracts.” The patients grant access to their health data collected from the sensors, and researchers may request data stored off-chain, while a durable and transparent log of all transactions is created in the form of a distributable ledger. BlockTrial is beneficial as it both allows patients better access and control over their data and encourages researchers to adhere to reporting requirements.
Similarly, ref. [
43] developed SCoDES, a Hyperledger blockchain framework based on PoC to improve the procedures for managing patient consent, with confidentiality, to share their health data with clinicians. The collected data from the sensors is shared between medical platforms using appropriate software (e.g., React, REpresentational State Transfer (REST) Server, and Research Electronic Data Capture (REDCap)).
3. Proposed Architecture and Emulator Environment
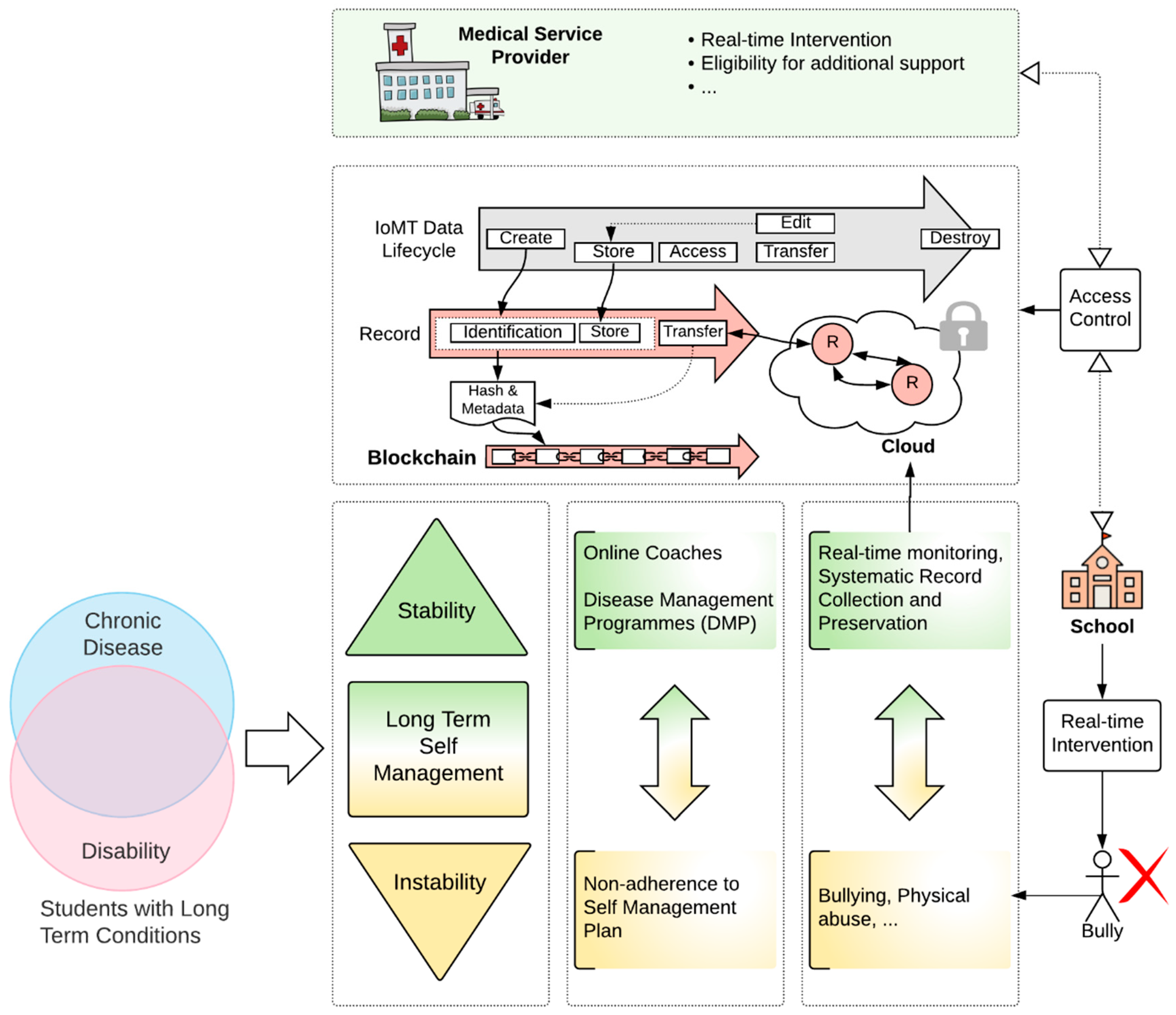
A high-level demonstration of the solution is shown in
Figure 2 and the emulator’s architecture is shared in
Figure 3. The proposal was designed to establish collaboration between the IoMT service provider (e.g., hospital, medical centre) and a participating school attended by the patient. In our case study, the scenario focuses on bullying at schools due to the size of the problem, as evidenced by published studies.
Figure 2 illustrates how students with long-term conditions (which can be a disability, chronic disease, or both) are supported by disease management programmes (DMPs) to support the stability of their day-to-day lives. However, several factors could introduce risk through instability. Bullying and physical abuse are one of the key reasons a life’s routine can be affected. Furthermore, a bullying experience, in this case, can be life-threatening and require urgent intervention (e.g., by security officers on campus).
The IoMT data is typically shared with the medical service provider without the added value of blockchain immunity and data management. We propose an access control module responsible for permitting the required access to IoMT data to trigger the required intervention. Several principles govern the model. These are:
Segregation of duties between stakeholders;
Principle of least privilege; and
Forensic readiness enabled by an automated process where the chain of custody is blockchain-based and updated in real time.
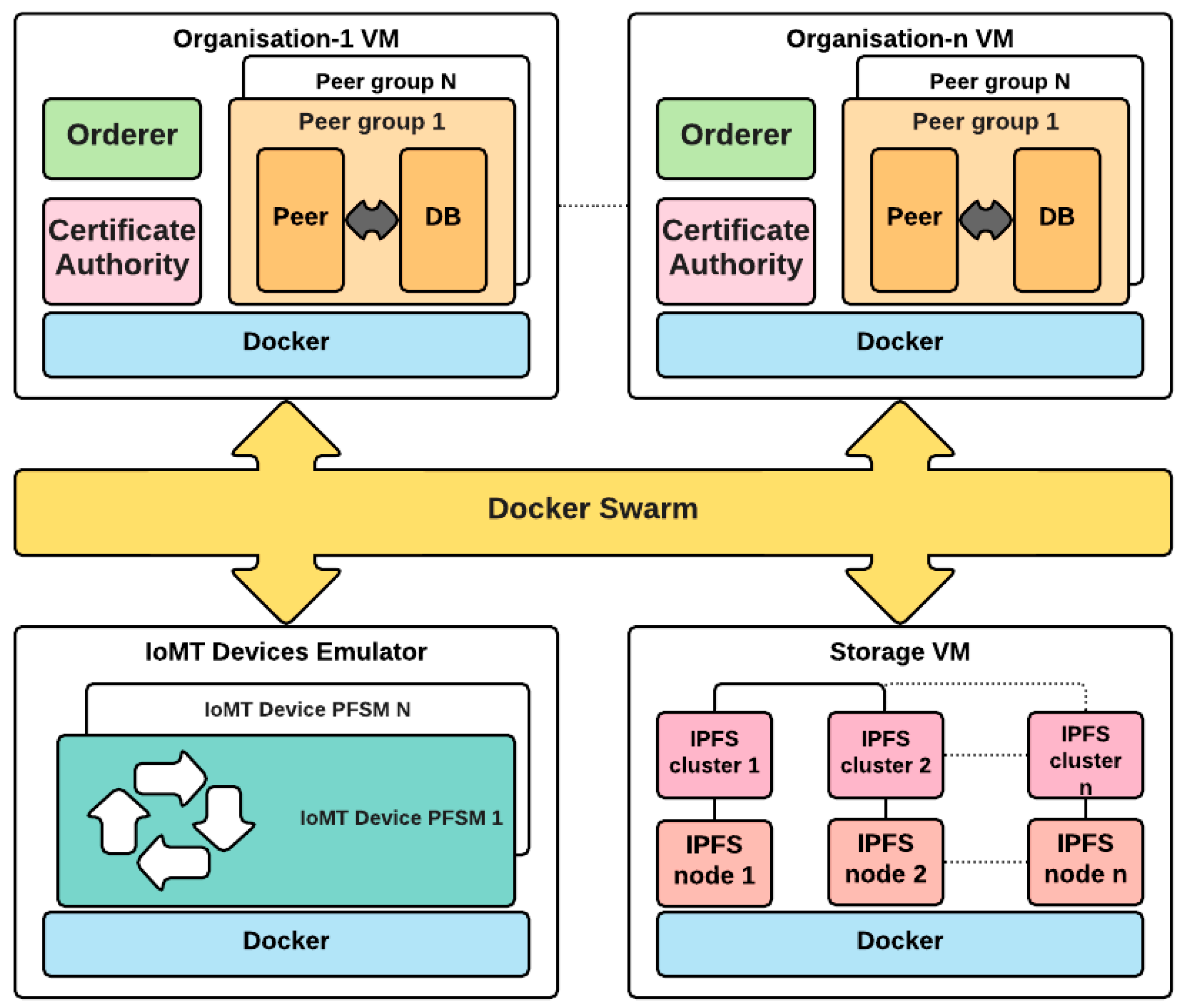
To evaluate the performance of the blockchain-based model in a hypothetical IoMT scenario,
Figure 3 presents the architectural components of our IoMT–blockchain emulator, namely, the main design requirements and the reference architecture. It consists of several virtual machines, each containing different elements encapsulated and isolated in containers. These containers communicate with the rest of the system via a Docker Swarm network, which orchestrates local docker installations. The use of containers is justified by their substantial lightness, portability, and a corresponding reduction in management overhead since they share the same operating system. The use of virtual machines has not been completely excluded but considered to logically group components that are geographically located remotely in a production scenario, such as organisations and storage.
The description starts with the introduction of an abstract model of IoMT sensors based on the elementary interactions performed on the blockchain platform and modelled through a probabilistic finite-state machine (PFSM). This model provides the opportunity to define a test environment as close as possible to a real scenario without the need to introduce unnecessary complexities, which are not relevant in the performance evaluation of the platform itself. In the corresponding virtual machine (VM), the emulator spawns several entities that access the blockchain platform, each of which can have independent and unique behaviour according to its status and functionalities. At the same time, the impact on the platform is continuously monitored to discover and measure possible constraints and bottlenecks of the system.
One or more VMs contain the organisations that participate in the blockchain. Each organisation includes a CA (certificate authority) server that manages the certificates and credentials regulating the access to the blockchain. The peers have distributed replicas of the ledger, being the sources and the destinations of all transactions. The choice of the number of peers is influenced by many factors, including the need to provide high availability and data distribution to reduce access latency. It is not unusual for an organisation to have multiple peers distributed across different geographic areas. Each peer is associated with a support database, which contains the last value for each key entered and updated by the transactions, hence the name “world state database.” Its presence is crucial for the performance of the system: Access to the last state of an asset (for example, the last version of the patient’s health record) becomes immediate without having to traverse all the blocks of the chain. Finally, each organisation also contains an orderer node that participates in a Raft cluster. Orderers are the key players in the consensus mechanism, as they reach an agreement on validating the new block of transactions added to the ledger.
Although it is possible to save patients’ information directly in the transaction payload, this possibility must be evaluated by considering the data size and rate. All the data stored in the transactions will be replicated on each peer and cannot be removed, directly resulting from the immutability property of the blockchain. To tackle this scalability issue, we considered the solution of storing data off-chain in additional VM storage, which contains a network of nodes implementing an InterPlanetary File System (IPFS). IPFS is a protocol very often associated with the blockchain, as it shares its distributed nature. Furthermore, in IPFS the address of a document coincides with the hash of its content, avoiding unnecessary storage of future identical files and at the same time, reducing the space required in the case of files with common sub-parts. Such a hash is then stored in a blockchain transaction, inheriting its properties of immutability and integrity. In our approach, the storage is composed of a configurable number of IPFS nodes, each one connected to a cluster service to provide a fail-safe environment by guaranteeing a minimum number of replicas. Access to IPFS functionalities is implemented via RESTful Application Programming Interfaces (APIs), which are exported by the nodes themselves.
4. Integration of Blockchain Types and Associated Consensus Mechanisms in IoMT
Blockchains consist of multiple blocks containing transactions records strung together. The four requirements for adding a block are (i) it must be a transaction, (ii) it must be verified, (iii) it must be stored, and (iv) it must receive a hash. For a more detailed classification, a blockchain requires a distributed ledger, a consensus mechanism, and associated cryptographic means [
44].
A distributed ledger is a consensually shared database synchronised across multiple nodes that allows transactions to have public witnesses [
45]. To that aspect, all nodes are permitted to retrieve and store a copy of the recorded transactions. Once added to the ledger, data cannot be removed or edited. To achieve a consensus regarding a transaction’s legitimacy, the nodes must adhere to a predefined mechanism protocol. Without consensus, all stored transaction blocks are at risk of various attacks known as Byzantine manners [
46].
Public or permissionless blockchains, such as those used for Bitcoin [
47] and Ethereum [
48] algorithms, hold the transactions’ information in the public domain and can be read and contributed to without requiring permission. They are decentralised, immutable, accessible to all, and no individual participant can control the network. In such a system, medical data, including treatment and institutional costs, once validated, could be inserted by professionals and patients, making them transparent. In an open public blockchain, the more popular the network is, the more time a transaction will require to be validated. As new transactions entries would require a consensus from all the nodes’ multiple transactions would clog the network. Lastly, consensus mechanisms running on public open blockchain networks such as Proof-of-Work (PoW), Proof-of-Authority (PoAu), ByzCoin, Proof-of-Stake (PoS), Delegated Proof-of-Stake (DPoS), Leased Proof-of-Stake (LPoS), Casper, Proof-of-Burn (PoB), Elastico, and OmniLedger consume considerable amounts of electricity. Such drawbacks mean that open public blockchains in their current state cannot compete with traditional systems [
49].
Alternatively, in a private or permissioned blockchain, based on Practical Byzantine Fault Tolerance (PBFT), Delegated Practical Byzantine Fault Tolerance (DPBFT), Proof-of-Elapsed-Time (PoET), RSCoin, Tendermint, Pore, or Raft consensus protocols, membership is by invitation only. A single entity and the participants governing it require permission to read, contribute to, or audit its multiple layers of often confidential information, some of which requires higher levels of security and privacy that can only be accessed by authorised parties. They are also highly scalable, and since only a few nodes are capable of managing data, the network can process more transactions more quickly than a public blockchain. These characteristics of private blockchain platforms make them optimal for an IoMT network [
49]. Due to the sensitivity and the size of data, privacy, trust, speed, and scalability are key criteria that are better met by the private blockchain [
50]. However, its disadvantages are that (i) being private makes it centralised, (ii) trust becomes an important issue since transactions cannot be independently validated, and (iii) its security is compromised since its fewer nodes make it easier to exploit. The right selection of consensus mechanisms addresses these disadvantages. Both public and private blockchains are competitors. However, there is plenty of room for them both to be developed, as they each have their individual advantages. Indeed, creating a hybrid network based on either Ripple or Aergo consensus protocols could be a viable solution for a decentralised structure with centralised elements. There are numerous benefits of using a hybrid blockchain as it combines a private blockchain speed of generating the transactions’ hash combined with the verification security procedure benefits provided by the public blockchain [
51].
The consensus mechanisms define the verification process, validation time, processing cost, and thus, the security and efficiency of the network [
52]. Four main categories of consensus mechanisms can be discriminated based on their characteristics, i.e., (i) PoW, (ii) PoS, (iii) a hybrid that is a combination of both PoW and PoS, and (iv) Byzantine Fault Tolerance.
Table 1 presents a comparison of the consensus mechanisms, evaluating specific performance parameters.
The Proof-of-Work (PoW) is the most popular resource-intensive consensus protocol and requires great computation power and advanced hardware for the fastest node to solve complex computational algorithms and be selected to validate and generate a new block (mining process) [
53]. Similar to the PoW mechanism is the Proof-of-Capacity (PoC), which allows nodes to use the available hard drive space instead of the device’s computing processing power. The disadvantages, though, include lower adoption rates and possible malware, which may affect the mining process. Both PoW and PoC protocols are susceptible to scalability issues [
54].
Table 1.
Comparison of consensus mechanisms [
46,
54,
55,
56].
Table 1.
Comparison of consensus mechanisms [
46,
54,
55,
56].
| Consensus Mechanisms | Network Type | Decentralisation | Scalability | Throughput | Latency | Tolerance | Power Consumption | Network Resources | Storage Resources | Consensus Type |
|---|
| PoW | Public | High | High | Low | High | Low | High | Low | High | Competitive |
| PoC | Public | High | High | Low | High | N/A | Low | Low | Very High | Collaborative |
| PoET | Both | Med | High | High | Low | N/A | Low | Low | High | Competitive |
| PoS | Both | High | High | Low | Med | High | Med | Low | High | Competitive |
| DPoS | Public | Med | High | High | Med | High | Med | N/A | High | Collaborative |
| DPoW | Public | High | High | Low | High | High | Med | N/A | High | Collaborative |
| PoR | Private | High | High | N/A | High | High | Low | Low | Low | Collaborative |
| LPoS | Public | High | High | Low | Med | High | Med | Low | High | Competitive |
| PoI | Public | High | High | High | Med | High | Low | Low | High | N/A |
| PoA | Public | High | High | Low | Med | High | High | Low | High | Collaborative |
| Casper | Public | High | High | Med | Med | High | Med | Low | High | N/A |
| PoB | Public | High | High | Low | High | Low | Med | Low | High | N/A |
| PBFT | Private | Med | Low | High | Low | Med | Low | High | High | N/A |
| DPBFT | Private | Med | High | High | Med | Med | Low | High | High | N/A |
| Stellar | Public | High | High | High | Med | Variable | Low | Med | High | N/A |
| Ripple | Public | High | High | High | Med | Low | Low | Med | High | N/A |
| Tendermint | Private | Med | High | High | Low | Med | Low | High | High | N/A |
| ByzCoin | Public | High | High | High | Med | Med | High | Med | High | N/A |
| Algorand | Public | High | High | Med | Med | Med | Low | High | High | N/A |
| Dfinity | Both | High | High | N/A | Med | N/A | Low | N/A | N/A | N/A |
| RSCoin | Private | Low | High | High | Low | N/A | Low | Med | High | N/A |
| Elastico | Public | High | High | Low | High | Low | Med | High | High | N/A |
| OmniLedger | Public | High | High | High | Med | Low | Med | Med | Low | N/A |
| RapidChain | Public | High | High | High | Med | Med | Med | Low | Low | N/A |
| Raft | Private | Med | High | High | Low | High | Low | N/A | High | N/A |
| Tangle | Public | Med | High | High | Low | Med | Low | Low | Low | N/A |
| Pore | Private | Low | High | N/A | Low | N/A | N/A | N/A | N/A | Collaborative |
As a solution, PoS is more environmentally friendly and does not require computational power as it chooses a node to be the validator based on a pseudo-random selection process. However, to commit to the process, nodes must stake their own coins [
57]. In addition, although it eliminates the excessive PoW computational requirement, the blockchain becomes centralised because of its dependence on nodes with the highest amount of stake. The DPoS protocol is more efficient, faster, and democratic than PoS, as the generation and validation of new blocks is based on a voting system among a team of elected delegates. The voting power of each node increases based on the number of coins it holds, which makes it more centralised but also more scalable as it can process more transactions per second (Tps) than PoW and PoS. More variations of the PoS that partially solve the centralisation problem are the LPoS and the Proof-of-Importance (PoI). LPoS allows wealthy nodes to lease funds to low balance nodes, thereby increasing their selection chances to verify transactions [
54]. In the PoI the node’s reputation is also taken into account in the selection process.
The PBFT protocol, based on a voting consensus approach for validating transactions, assumes nodes are authenticated, thereby improving robustness and performance. However, it is beneficial only for small consensus groups since the scale of transactions is large and outcomes are few. PBFT has been used in IoMT for sharing clinical data between healthcare providers [
58] because it can provide integrity and value of the collected data from the vital sensors and monitors, and assurance and transparency of the data management [
59].
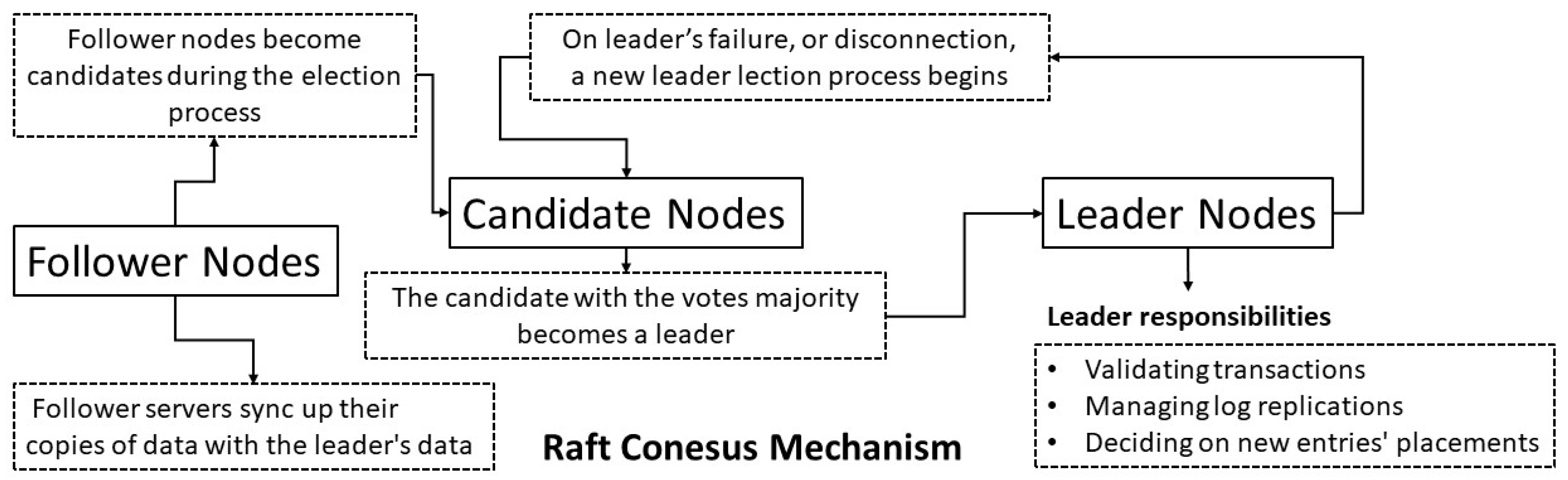
The consensus mechanism that was selected to achieve the necessary agreement among the distributed processes was the Raft. It was chosen because it has PBFT characteristics, is designed for a private blockchain network, has been proven to be safe, and is a modern, reliable, and relatively less complicated distributed consensus algorithm. The nodes fall into three categories: (i) leader, (ii) follower, and (iii) candidate (see
Figure 4). The “leader” is responsible for validating transactions, monitoring and controlling the log replications on the cluster’s servers, deciding on new entries’ placements, and assuring data flow between all servers without needing to consult any of them. If a malfunction is spotted on the leader’s activities, then a new leader is elected. The “follower” servers, whose responsibilities up to that moment are to sync up their copies of data with the leader’s data at regular time intervals [
60], become candidates if they cannot establish communication with the leader for a specific period—called an election timeout. A leader election then begins. The candidate server increases the term counter by voting for itself to become a new leader. It will also send a message to all other servers canvassing their votes; it must be stated that any node in the cluster can become a leader. The candidate gets defeated when it receives a message with a term number equal to or bigger than its current term. In that case, it becomes a follower. The candidate receiving the most votes becomes the leader. If there is a split vote, a new term must start, and a new election takes place. The democratic voting system for electing a new leader and the operational sustainability can remain operational even if a minority of servers, i.e., two out of five, fail. The high performance and the low latency characteristics were also considered for selecting this consensus mechanism protocol to run our IoMT dedicated emulator.
5. Experiments
An extensive series of experiments was conducted to analyse the feasibility and performance of the proposed architecture. The choice of the specific blockchain implementation was made according to the maturity and modularity levels of the solution. Hyperledger Fabric [
61] was demonstrated to be the best option, considering the expressiveness of its smart contracts, created with GOLang and Javascript programming languages, and the availability of ready-made and tested side projects that significantly extend its functionalities.
The evaluation metrics that were used during the tests were the transaction latency, Central Processing Unit (CPU) utilisation, memory consumption, and disk throughput. These metrics were analysed based on three different directions: the rate at which transactions were accessed, the size of the corresponding payloads, and finally, the specific type of access. To monitor these Key Performance Indicators (KPIs), we introduced a separate virtual machine hosting a tool called Hyperledger Explorer. The latter provided a web frontend and a layer of APIs to consult the blockchain platform. More specifically, these APIs were used to monitor the status of the system and the system’s nodes, to inspect the transactions’ contents, and to provide coarse indicators, as the number of transactions and blocks per hour. More accurate data was provided by a second tool, named Hyperledger Caliper, which was used to monitor all containers deployed in our testbed. During its execution, Hyperledger Caliper spawned a predefined number of client components, written in Javascript, which connected to the blockchain platform, invoking the smart contracts through a callback mechanism.
5.1. Archetypes of Data-Aware Smart Contracts and PFSM Composition
In its standard implementation, Hyperledger Caliper is only able to invoke a single smart contract in each test. Although this procedure is simple and effective, it is not sufficient for the evaluation of real scenarios, where the interaction between an IoMT sensor and the blockchain involves the invocation of multiple smart contracts. To obtain results that can be generalised to different contexts, we first categorised the fundamental read–write interactions between IoMT sensors and the blockchain platform, and we developed them in the form of smart contracts:
- -
The smart contracts writeOnchainData and readOnchainData store and retrieve data directly to and from the transactions saved in the blockchain. The data size must be limited as these payloads can never be removed and are automatically replicated in all peers. Possible examples are sensors that store the acquired values with low frequency and small payloads, such as humidity sensors.
- -
The smart contracts writeOnchainBatch and readOnchainBatch manage batch data, directly saved inside a single blockchain’s transaction. Typical examples are time series. Batch operations avoid the generation of various transactions and the corresponding number of consensus agreements.
- -
The smart contracts writeOffchainData and readOffchainData store and retrieve files and big data to and from off-chain storage. The writing process starts with the upload to the IPFS endpoint and the creation of a blockchain transaction that includes the obtained hash value and eventual metadata. On the other hand, the reading process begins by reading the blockchain hash, which is used as the file path for the download by the storage service.
To properly model the complex interaction between IoMT devices and the blockchain’s smart contracts, we extensively used PFSMs. The latter was composed of a set of transitions, each one starting from and ending with a state with a specific probability of occurring. Each transition was bound to a smart contract that was executed at the same time the transition was fired. The probability of making a transition allowed the closer approximation of devices’ logic, distinguishing between standard and special operations. Furthermore, smart contracts’ parameters, such as the size of the payload or the batch length, could be configured independently in each step of the machine, aiming for even more accurate modelling.
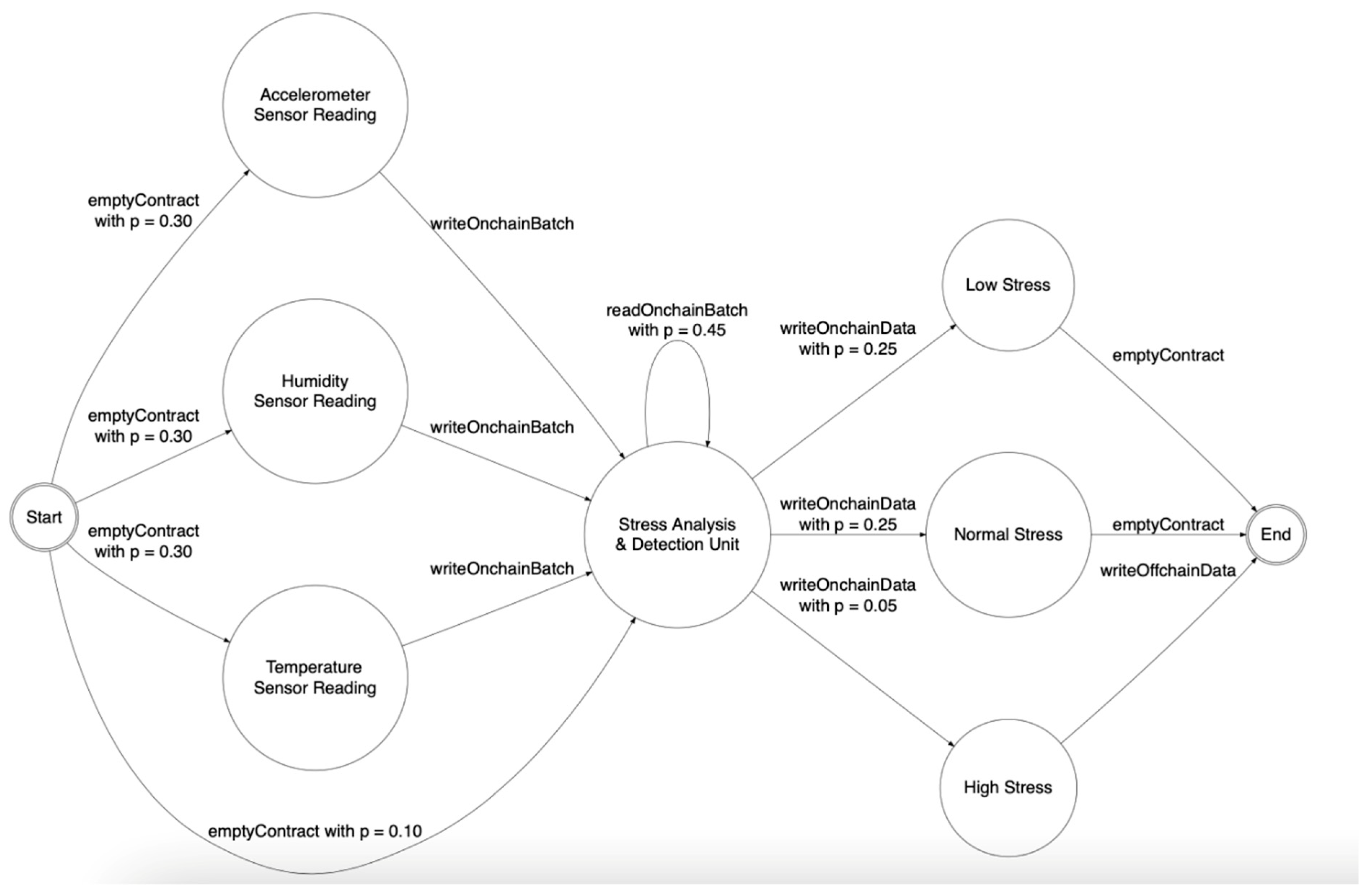
Figure 5. A possible representation of IoMT device iStress using a PFSM presents a possible representation of the stress-detection device named iStress proposed in ref. [
62] using a PFSM: The operation of the device was considered as the continuous iteration of the diagram shown. In the start node, it was very likely (
p = 0.90) that the data from the three primary sensors were read, namely the accelerometer, the humidity, and the temperature sensors. Each of these reads invocated the
writeOnchainData smart contract, which saved the values in the blockchain. Furthermore, it was possible to execute an empty transaction (with probability
p = 0.10) that simulated the unavailability of new data from those sensors. In the “Stress Analysis and Detection Unit” node, data analysis took place, which included a variable number of readings (smart contract
readOnchainBatch with
p = 0.45) and the following choice of one of the three possible outcomes: “Low Stress,” “Normal Stress,” or “High Stress.” Each of these was written on the blockchain via the
writeOnchainData smart contract. We deliberately assigned a low incidence to the “High Stress” outcome (
p = 0.05), however, due to its severity, it was likely to generate an event outside the system, for example to the healthcare facility, which was simulated through the
writeOffchainData smart contract.
Our testbed allowed for the definition of multiple PFSMs, each one representing a device or a class of sensors interacting with the blockchain platform. In doing so, an architect could recreate various scenarios, thus evaluating and predicting the impact of IoMT sensors on the blockchain even before the availability of physical devices. The emulation process led to a two-fold benefit: Firstly, by knowing the characteristics of an existing blockchain infrastructure, it was possible to estimate the number of devices that could be connected while maintaining the minimum quality of service, as in the case of maximum transaction latency. Secondly, by knowing the amount and type of devices and the expected number of patients, it was possible to predict the computational resources that should be acquired, either on-premises or in the cloud, as a part of a feasibility analysis and the estimation of the implementation costs.
5.2. Experiment Procedure
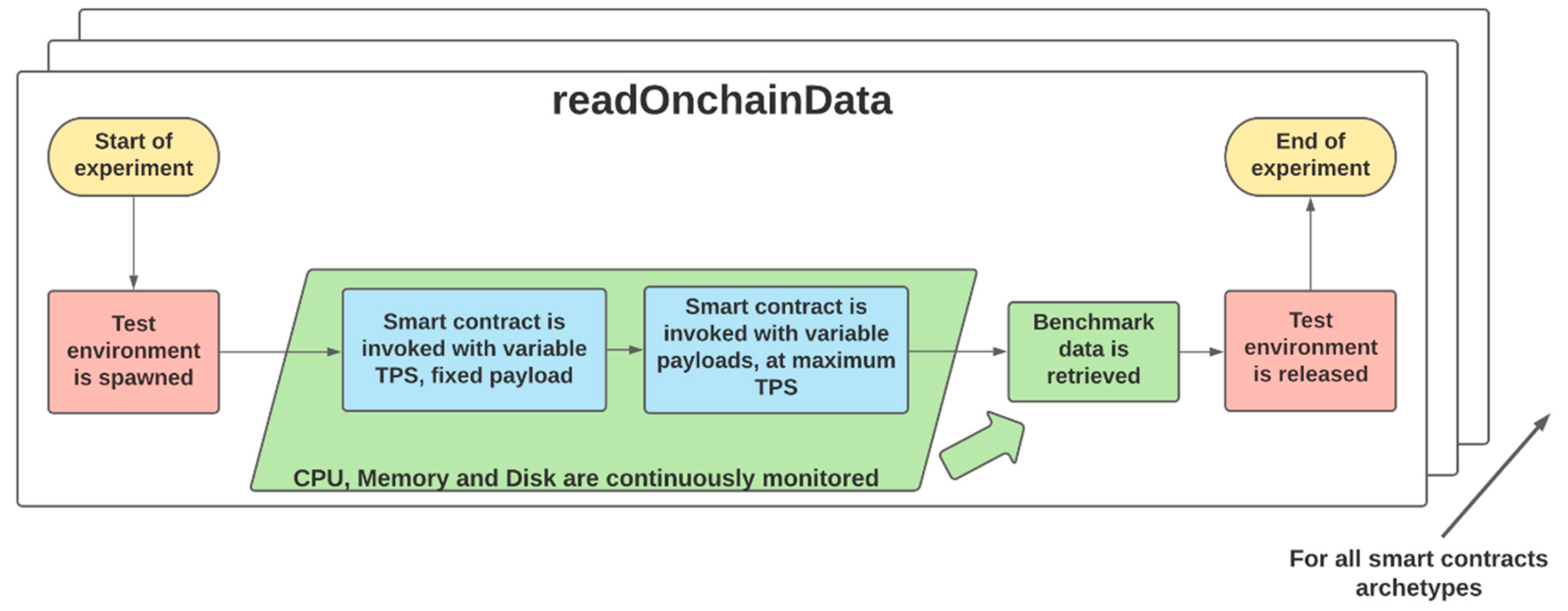
Figure 6 shows the flow chart representing the procedure used during the experiments. For each smart contract archetype, an independent testbed environment was allocated, each one having the same hardware characteristics and computational resources. In this environment, the Hyperledger Explorer and Hyperledger Caliper tools were used to monitor the KPIs. Furthermore, in each test, Hyperledger Caliper was associated with a bespoke callback module for interacting with the specific contract in the blockchain.
In the first phase of the experiments, a smart contract at increasing frequencies (Transaction per second or Tps) was invoked with a fixed payload in order to analyse the latency. The latency measurement included the time needed for the transfer of the payload between the various nodes of the network, the duration of the chosen consensus method, and the creation time of a new block that would contain the transaction itself. The reciprocal of the minimum latency was the maximum frequency with which transactions could be created in the system and determined an upper bound of the rate of interactions between the IoMT sensors and the blockchain. In the second phase, the same smart contract was invoked under different payload sizes to investigate the corresponding maximum achievable frequency of invocation. These sizes were powers of two, from 256 to 32,768 bytes for on-chain operations and above that limit for the off-chain storage. The maximum Tps was determined by a fixed-length backlog-based technique, where the smart contract was invoked only if the backlog had a free slot. When the smart contract was fired, the call was inserted in the backlog and removed as soon as the transaction was completed. If the backlog was full, no new smart contract was executed until an ongoing one was completed. In this way, the emulated device could dynamically adapt its data rate to the instantaneous workload of the blockchain.
For the entire duration of the experiment, the environment was continuously monitored in order to collect detailed information regarding CPU utilisation, memory consumption, and disk throughput. This information was retrieved directly from each component of the architecture, namely, the peers (Pe), the databases (Db), the orderers (Or), the off-chain storage (St), and the certificate authority (CA). By doing so, the components and the subsystems more likely to limit the scalability of our proposed solution get identified.
6. Results and Discussion
The results in this section emerged from a case study including two organisations. The testbed included virtual machines hosted in Amazon AWS EC2 (Amazon, Seattle, WA, USA), each equipped with 2 vCPU, 8 Gb of RAM, and 30 Gb of Solid-State Drive (SSD) storage. Tests lasted 120 s, during which the performance of system components was monitored.
The maximum rate of transaction creation (transactions per second, or Tps), although dependant on payload’s size, was 120, which constituted the upper limit in rate-related tests.
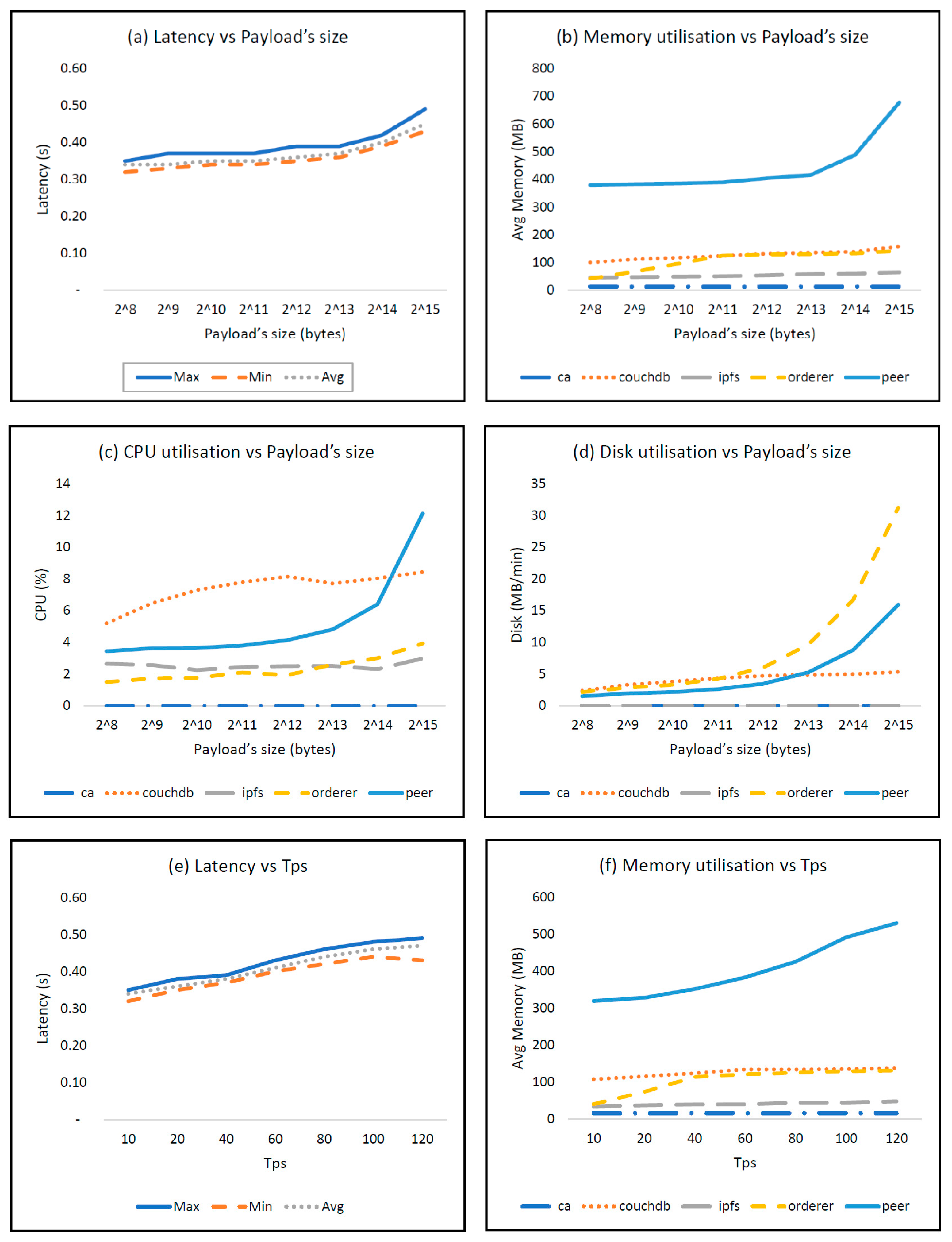
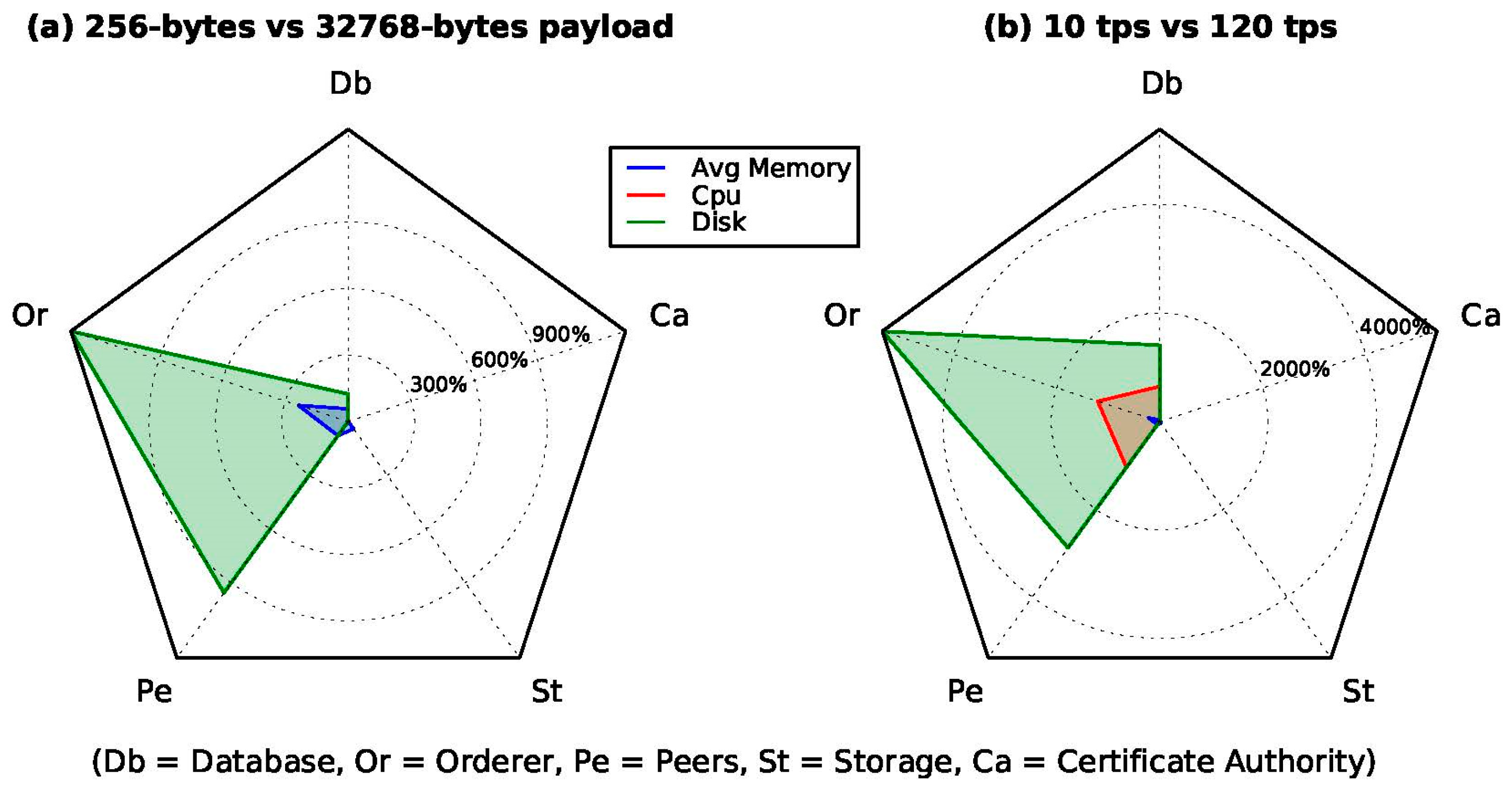
Figure 7 shows the results of the test for writeOnchainData as an example. Moreover, since the absolute performances were correlated to the specific hardware infrastructure, we opted for the normalisation of the worst-condition results (i.e., 32,768-byte payload and 120 Tps) with the ones corresponding to the most favourable conditions (i.e., 256-byte payload and 10 Tps).
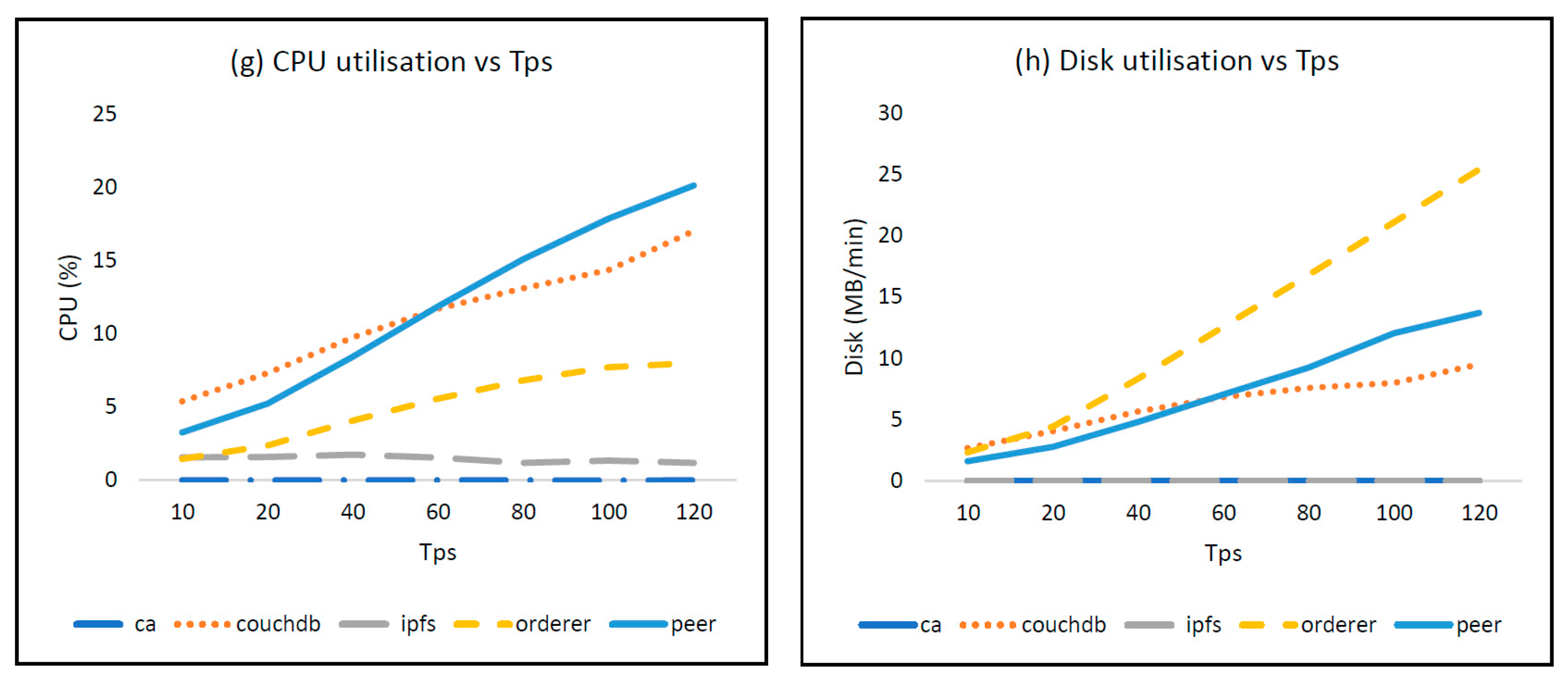
Figure 8 illustrates which resources were more influenced and could become potential bottlenecks of the system. Similar plots were produced for all other smart contracts as well.
According to
Figure 7a,e, the time required for the transaction’s creation grew slightly with larger data sizes and faster invocations but always remained under 1 s. Considering that the payload doubled in each test, the apparent exponential behaviour of peers’ memory, CPU, and disk utilisation increased linearly. An interesting observation arises by comparing peers with the underlying world state databases (CouchDB). At first sight, they should have been subjected to the same load, since the increasing payloads were equally stored in both components. Nonetheless, memory and disk utilisations were lower in databases, as a consequence of the inner compression method applied by the latter, which was also confirmed by the CPU usage. By disabling compression or by providing high-entropy payloads that can be hardly compressed, peers and databases showed similar resource usage. Orderer disk utilisation was also significant, as illustrated in
Figure 8a,b, where the disk subsystems emerged as the components most directly affected by the increase in both data size and data rate.
The tests carried out on the
readOnchainData smart contract showed that the average latency was stable at 0.01 s for all the payload’s sizes and Tps. Nonetheless, as the payload’s size increased, more orderer memory was used, concurrent with a slight increase in database CPU utilisation, plausibly due to data decompression. On the other hand, by increasing Tps, only peer CPU utilisation was affected, due to the higher number of smart contract invocations. Reading the data from the transactions was therefore a very efficient action because the consensus was avoided by querying the peer directly. Furthermore, it was possible to force the execution of the consensus method, giving the possibility to isolate the delay introduced by the consensus. The results in
Table 2. Latency of readOnchainData with
consensus enabled suggest that the Raft-based consensus’s overhead was approximately 0.30 s.
The writeOnchainBatch smart contract was tested to assess its limits. Considering a batch of fixed length equal to 10 elements, the maximum size of each element was 8192 bytes, for a total payload of 80 kbytes. Beyond this size, transactions were not completed fast enough to sustain the desired 10 Tps. The most utilised component was the orderer for both memories used and disk access, followed by CPU usage of the peers. Considering a fixed batch of 10 elements of 256 bytes each, the maximum invocation frequency was 53 Tps, which emerged from the use of the backlog. Finally, considering a 256-byte payload, a maximum batch length of 75 was reached before the resulting latency prevented a stable rate of 10 Tps. This limitation was imposed by the orderer’s memory and disk usage. However, this approach allowed the writing of 750 items per second, well above the 114 maximum achievable with writeOnchainData. The smart contract readOnchainBatch proved to be efficient and fast in all configurations at the expense of a slight increase in memory and CPU usage due to the larger transactions executed.
In the last part of our experiments, we analysed the impact of the off-chain storage, namely, the smart contracts writeOffchainData and readOffchainData, with increasing file-size (from 256 kb to 10 mb). During the writing phase, the file was transmitted to the IPFS service directly; then its hash was stored in a transaction using writeOnchainData. On the contrary, the reading phase included the invocation of readOnchainData in order to retrieve the hash used as a file anchor in the off-chain file download. In both cases, the latency was almost linear with the file size, with a maximum rate of 100 files per second in the smallest configuration. Access to the blockchain has proven to be much faster than the corresponding access to IPFS storage, whose performances were closely linked to the slowness of the disk subsystem.
7. Conclusions
Bullying among school children is not a new phenomenon. Recent statistics have proven that there is a growth rate year by year, impacting mainly the most vulnerable students, especially those with chronic physical illness or disabilities. Unfortunately, there is not an obvious bridge between well-being programs and academic outcomes. Hence, although there are several components and various programs available in schools that may positively influence children’s well-being, there is little evidence to suggest that an integrated program exists that can detect stress and incidents of victimisation among students in real time.
In this study, we proposed a private permission blockchain platform to enable real-time intervention triggered by IoMT data that could be collected by mobile wearable sensors already attached to students due to chronic conditions. Given the unavailability of physical devices, the performance and capabilities of the proposed platform were evaluated and demonstrated with the use of an emulator under different loads of sensor-generated data. With this testbed, we investigated the impact of IoMT sensors on the blockchain platform based on two main criteria: the transaction latency and the computational resources. The results proved that the interaction between the sensors and the blockchain can be limited by the access modes deployed. This could have a detrimental effect on the sizing of the various entities and components within an IoMT architecture. Additionally, the rate at which the information was generated and exchanged between nodes proved to be a crucial factor in the performance of a highly distributed platform governed by a consensus algorithm.
Future analysis will investigate additional attributes and parameters for sensors in Industrial Internet of Things (IIoT) deployments to enrich the emulator’s existing capabilities. Additionally, we are planning to develop a user-centric approach by designing a user interface-based use case usability study.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








