
Aspects of Prevention of Urinary Tract Infections Associated with Urinary Bladder Catheterisation and Their Implementation in Nursing Practice


Abstract
:1. Introduction
2. Materials and Methods
2.1. Material
2.2. Methods
3. Results
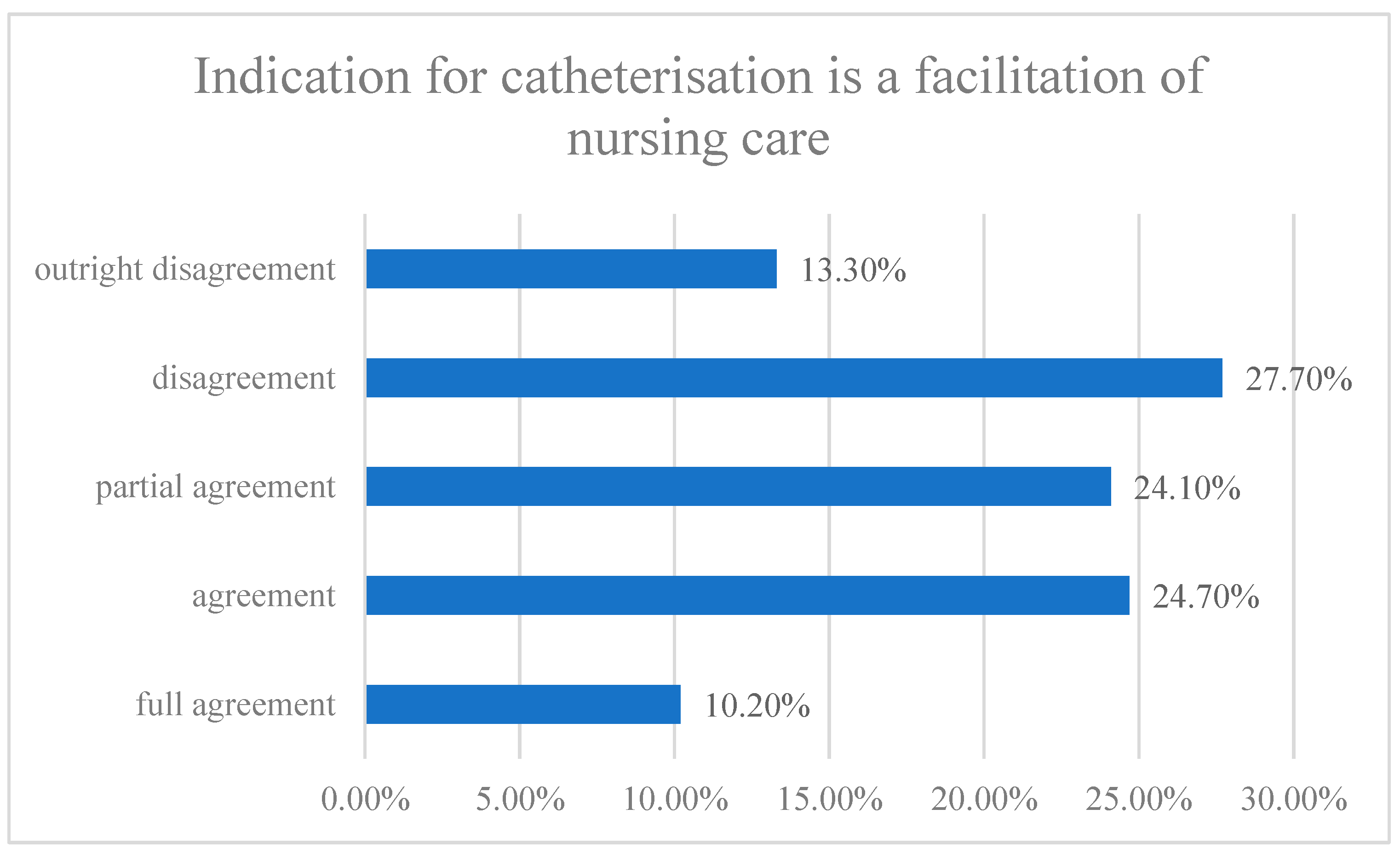
3.1. Indication for Catheterisation
3.2. Education
3.3. Increasing the Quality of Care and Care Quality Monitoring
3.4. Risk Management
3.5. Support of IT Technologies in the Process of Quality Improvement and Care Safety and Risk Management
3.6. Documentation of Urinary Bladder Atheterisation
3.7. Consumables and Aids
3.8. Teams of Experts
4. Discussion
5. Conclusions
Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Declaration
References
- Andreessen, L.; Wilde, M.H.; Herendeen, P. Preventing catheter-associated urinary tract infections in acute care: The bundle approach. J. Nurs. Care Qual. 2012, 27, 209–217. [Google Scholar] [CrossRef]
- Carter, N.M.; Reitmeier, L.; Godloe, L.R. An evidence-based approach to the prevention of catheter-associated urinary tract infections. Urol. Nurs. 2014, 34, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Jindrák, V.; HEDLOVÁ, D.; Urbášková, P. Antibiotická Politika a Prevence Infekcí v Nemocnici; Mladá Fronta: Praha, Czech Republic, 2014; ISBN 978-80-204-2815-8. [Google Scholar]
- Purvis, S.; Gion, T.; Kennedy, G.; Rees, S.; Safdar, N.; Van Den Bergh, S.; Weber, J. Catheter-associated urinary tract infection: A successful prevention effort employing a multipronged initiative at an academic medical center. J. Nurs. Care Qual. 2014, 29, 141–148. [Google Scholar] [CrossRef]
- Yatim, J.; Wong, K.S.; Ling, M.L.; Tan, S.B.; Tan, K.Y.; Hockenberry, M. A nurse-driven process for timely removal of urinary catheters. Int. J. Urol. Nurs. 2016, 10, 167–172. [Google Scholar] [CrossRef]
- AACN Practice Alert. Prevention of catheer-associated urinary tract infections in adults. Crit. Care Nurse 2016, 36, e9–e11. [Google Scholar] [CrossRef]
- McNeill, L. Back to basics: How evidence-based nursing practice can prevent catheter-associated urinary tract infections. Urol. Nurs. 2017, 37, 204–206. [Google Scholar] [CrossRef]
- Parker, V.; Giles, M.; Graham, L.; Suthers, B.; Watts, W.; O’Brien, T.; Searles, A. Avoiding inappropriate urinary catheter use and catheter-associated urinary tract infection (CAUTI): A pre-post control intervention study. BMC Health Serv. Res. 2017, 17, 314. [Google Scholar] [CrossRef]
- Krocová, J.; Prokešová, R.; Horová, J. The prevention of healthcare associated urinary tract infections from the point of view of nursing care. Kontakt 2019, 21, 135–143. [Google Scholar] [CrossRef]
- The Centers for Disease Control and Prevention—CDC. Guideline for Prevention of Catheter-Associated Urinary Tract Infections (2009). HICPAC. Last Update: 6 June 2019. Available online: https://www.cdc.gov/infectioncontrol/pdf/guidelines/cauti-guidelines-H.pdf (accessed on 30 December 2021).
- Tenke, P.; Kovacs, B.; Bjerklund Johansen, T.E.; Matsumoto, T.; Tambyah, P.A.; Naber, K.G. European and Asian guidelines on management and prevention of catheter-associated urinary tract infections. Int. J. Antimicrob. Agents 2008, 31, 68–78. [Google Scholar] [CrossRef]
- Conway, L.J.; Larson, E.L. Guidelines to prevent catheter-associated urinary tract infection: 1980 to 2010. Heart Lung 2012, 41, 271–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trautner, B.W. Management of catheter-associated urinary tract infection. Curr. Opin. Infect. Dis. 2010, 23, 76–82. [Google Scholar] [CrossRef]
- Quinn, P. Chasing Zero: A Nurse-Driven Process for Catheter-Associated Urinary Tract Infection Reduction in a Community Hospital. Nurs. Econ. 2015, 33, 320–325. [Google Scholar]
- Durant, D.J. Nurse-driven protocols and the prevention of catheter-associated urinary tract infections: A systematic review. Am. J. Infect. Control 2017, 45, 1331–1341. [Google Scholar] [CrossRef] [PubMed]
- Zurmehly, J. Implementing a Nurse-Driven Protocol to Reduce Catheter-Associated Urinary Tract Infections in a Long-Term Acute Care Hospital. J. Contin. Educ. Nurs. 2018, 49, 372–377. [Google Scholar] [CrossRef]
- Bernard, M.S.; Hunter, K.F.; Moore, K.N. A review of strategies to decrease the duration of indwelling urethral catheters and potentially reduce the incidence of catheter-associated urinary tract infections. Urol. Nurs. 2012, 32, 29–37. [Google Scholar] [CrossRef]
- Underwood, L. The effect of implementing a comprehensive unit-based safety program on urinary catheter use. Urol. Nurs. 2015, 35, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Alexantis, I.; Broome, B. Implementation of a Nurse-Driven Protocol to Prevent Catheter-Associated Urinary Tract Infections. J. Nurs. Care Qual. 2014, 29, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Powers, J. Impact of an aseptic procedure for breaking the integrity of the urinary drainage system on the development of catheter-associated urinary tract infections in the intensive care unit. Intensive Crit. Care Nurs. 2016, 37, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Carter, E.J.; Pallin, D.J.; Mandel, L.; Sinnette, C.; Schuur, J.D. A qualitative study of factors facilitating clinical nurse engagement in emergency department catheter-associated urinary tract infection prevention. J. Nurs. Adm. 2016, 46, 495–500. [Google Scholar] [CrossRef]
- Peter, S.; Devi, E.S.; Nayak, S.G. Effectiveness of clinical practice guidelines on prevention of catheter-associated urinary tract infections in selected hospitals. J. Krishna Inst. Med. Sci. Univ. 2018, 7, 55–66. [Google Scholar]
- Viner, S. Urinary Tract Infection Knowledge of Long-Term Care Nursing Staff: The Effect of an Educational Intervention. Urol. Nurs. 2020, 40, 7–11. [Google Scholar] [CrossRef]
- Freeman-Jobson, J.H.; Rogers, J.L.; Ward-Smith, P. Effect of an Education Presentation on the Knowledge and Awareness of Urinary Tract Infection among Non-Licensed and Licensed Health Care Workers in Long-Term Care Facilities. Urol. Nurs. 2016, 36, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Sublett, C.M. Application to the evidence base: Effect of an education intervention on urinary tract infection knowledge. Urol. Nurs. 2016, 6, 72–73. [Google Scholar] [CrossRef]
- Burston, S.; Chaboyer, W.; Gillespie, B. Nurse-sensitive indicators suitable to reflect nursing care quality: A review and discussion of issues. J. Clin. Nurs. 2014, 23, 1785–1795. [Google Scholar] [CrossRef]
- Pokojová, R. Bezpečnost Pacienta při Poskytování Ošetřovatelské péče. Č. Budějovice. Ph.D. Thesis, Faculty of Health and Social Sciences, University of South Bohemia in České Budějovice, České Budějovice, Czech Republic, 2018. [Google Scholar]
- Fuchs, M.A.; Sexton, D.J.; Thornlow, D.K.; Champagne, M.T. Evaluation of an evidence-based, nurse-driven checklist to prevent hospital-acquired catheter-associated urinary tract infections in intensive care units. J. Nurs. Care Qual. 2011, 26, 101–109. [Google Scholar] [CrossRef]
- Oman, K.S.; Makic, M.B.; Fink, R.; Schraeder, N.; Hulett, T.; Keecht, T.; Wald, H. Nurse-directed interventions to reduce catheter-associated urinary tract infections. Am. J. Infect. Control 2012, 40, 548–553. [Google Scholar] [CrossRef] [PubMed]
- McCoy, C.; Paredes, M.; Allen, S.; Blackey, J.; Nielsen, C.; Paluzzi, A.; Jonas, B. Catheter-Associated Urinary Tract Infections: Implementing a protocol to decrease incidence in oncology populations. Clin. J. Oncol. Nurs. 2017, 21, 460–465. [Google Scholar] [CrossRef]
- Johnson, P.; Gilman, A.; Lintner, A.; Buckner, E. Nurse-Driven Catheter-Associated Urinary Tract Infection Reduction Process and Protocol: Development Through an Academic-Practice Partnership. Crit. Care Nurs. Q. 2016, 39, 352–362. [Google Scholar] [CrossRef]
- Kim, B.; Pai, H.; Choi, W.S.; Kim, Y.; Kweon, K.T.; Kim, H.A.; Ryu, S.Y.; Wie, S.H.; Kim, J. Current status of indwelling urinary catheter utilization and catheter-associated urinary tract infection throughout hospital wards in Korea: A multicenter prospective observational study. PLoS ONE 2017, 12, e0185369. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.; Dogra, V.; Mishra, B.; Thakur, A.; Loomba, P.S. Knowledge and attitude of doctors and nurses regarding indication for catheterization and prevention of catheter-associated urinary tract infection in a tertiary care hospital. Indian J. Crit. Care Med. 2015, 19, 76–81. [Google Scholar] [CrossRef]
- Parry, M.F.; Grant, B.; Sestovic, M. Successful reduction in catheter-associated urinary tract infections: Focus on nurse-directed catheter removal. Am. J. Infect. Control 2013, 41, 1178–1181. [Google Scholar] [CrossRef] [PubMed]
- Markovic-Denic, L.; Mijovic, B.; Jankovic, S. Risk factors for hospital-acquired urinary tract infection: A case–control study. Int. Urol. Nephrol. 2010, 43, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Holroyd, S. Indwelling catheterisation: Evidence-based practice. J. Community Nurs. 2019, 33, 40–46. [Google Scholar]
- Wanat, M.; Borek, A.J.; Atkins, L.; Sallis, A.; Ashiru-Oredope, D.; Beech, E.; Butler, C.C.; Chadborn, T.; Hopkins, S.; Jones, L.; et al. Optimising Interventions for Catheter-Associated Urinary Tract Infections (CAUTI) in Primary, Secondary and Care Home Settings. Antibiotics 2020, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Pintar, P.A. An intrepreneurial innovative role: Integration of the clinical nurse specialist and infection prevention professional. Clin. Nurse Spec. 2013, 27, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Savitz, L.A.; Jones, C.B.; Bernard, S. Quality Indicators Sensitive to Nurse Staffing in Acute Care Settings. In Advances in Patient Safety: From Research to Implementation, Volume 4: Programs, Tools, and Products; Henriksen, K., Ed.; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2005. [Google Scholar]
- Kilíková, M.; Jakušová, V. Teoria a Prax v Manažmentu v Ošetrovatelstve; Osveta: Martin, Slovakia, 2008; ISBN 978-80-8063-290-8. [Google Scholar]
- Czech Republic; Ministry of Health of the Czech Republic. National Nursing Procedure “Urinary Bladder Catheterisation”. Available online: https://www.mzcr.cz/wp-content/uploads/wepub/18576/40359/NOP%20Katetrizace%20mo%C4%8Dov%C3%A9ho%20m%C4%9Bch%C3%BD%C5%99e.pdf (accessed on 31 December 2021).


{kind=link}
| Hospital Type | Absolute Frequency | Relative Frequency |
|---|---|---|
| University | 50 | 26.9% |
| Regional I | 36 | 19.4% |
| Regional II | 27 | 14.5% |
| Municipal | 28 | 15.1% |
| Private | 35 | 18.8% |
| Other | 10 | 5.4% |
| Overall | 186 | 100.0% |
| Competence to Assess Indications for Catheterisation and Acceptance of the Nurses Opinion-Assessment of Indications for Cathetrisation | Outright Disagreemen | Disagreement | Partial Agreement | Agreement | Full Agreement |
|---|---|---|---|---|---|
| Competency of A general nurse to voice HIS OR her opinion ON the indication of catheterisation and… | 4.2% | 3.6% | 25.3% | 37.3% | 29.5% |
| the opinion of the general nurse regarding the indication of catheterisation IS RESPECTED by THE physician | 5.4% | 3.0% | 41.0% | 30.7% | 19.9% |
| Improving Quality of Care and Monitoring Quality of Care | Yes | No | ||
|---|---|---|---|---|
| Absolute Frequency | Relative Frequency % | Absolute Frequency | Relative Frequency % | |
| There is a special internal calculation for quality improvement | 88 | 47.3 | 98 | 52.7 |
| One or more control groups or committees are established | 159 | 85.5 | 27 | 14.5 |
| One or more quality/safety managers/coordinators are appointed | 170 | 91.4 | 16 | 8.6 |
| Acknowlegments/incentives for quality improvement exist | 74 | 39.8 | 112 | 60.2 |
| Increasing the Quality of Care and Care Quality Monitoring | I Disagree | I Mostly Disagree | I Mostly Agree | I Agree |
|---|---|---|---|---|
| …Provision of feedback to patient care | 2.2% | 17.7% | 30.9% | 49.2% |
| …Is supported to report accidents and undesirable events | 0.0% | 9.9% | 28.7% | 61.4% |
| …Authorisations for activities are checked by the administrative body | 1.7% | 16.0% | 26.5% | 55.8% |
| Healthcare workers are trained in procedures ensuring patient safety | 0.0% | 11.6% | 38.1% | 50.3% |
| Existence of a Standard of Care and Regular Audits | Outright Disagreemen | Disagreement | Partial Agreement | Agreement | Full Agreement |
|---|---|---|---|---|---|
| Existence of standard of care for the procedure of urinary bladder catheterisation | 1.8% | 9.0% | 2.4% | 15.7% | 71.7% |
| Regular audits of the procedure of urinary bladder catheterisation | 14.5% | 25.9% | 23.5% | 12.7% | 23.5% |
| Introduction of It Technologies in the Process of Increasing the Quality and Safety of Care and Risk Management | Introduced | Not Introduced | ||
|---|---|---|---|---|
| Absolute Frequency | Relative Frequency % | Absolute Frequency | Relative Frequency % | |
| Reminder … in electronic form | 18 | 10.8 | 168 | 89.2 |
| Reminder … not in electronic form | 58 | 36.8 | 128 | 63.2 |
| Electronic patient medical records | 89 | 49.2 | 97 | 50.8 |
| Test results … in electronic form | 62 | 34.3 | 124 | 65.7 |
| Electronic drug prescription | 79 | 43.6 | 107 | 56.4 |
| Supportive systems (reminders, notes) | 19 | 10.5 | 167 | 89.5 |
| Regular Re-Evaluations of the Indication for Urinary Bladder Catheterisation Once in 24 h | X2 Value | p |
|---|---|---|
| “Reminder” of the evaluation of the indication of catheterisation as part of electronic documentation | 21.096 | <0.001 |
| “Reminder” of the evaluation of the indication of catheterisation in other ways than electronically | 37.507 | <0.001 |
| Teams of Experts for the Prevention of HAI and Form of HAI Reporting | I Disagree | I Mostly Disagree | I Mostly Agree | I Agree | I Fully Agree |
|---|---|---|---|---|---|
| Functioning of team of experts for the prevention of hospital infections | 4.9% | 10.2% | 10.8% | 22.8% | 51.3% |
| Authorised employee for prevention of infections at of the workplace | 10.8% | 27.7% | 12.1% | 17.5% | 31.9% |
| Reporting of the occurrence of HAI in the form of a printed document | 5.4% | 24.7% | 15.1% | 24.7% | 30.1% |
| Reporting of the occurrence of HAI in the form of an electronic form | 16.8% | 9.6% | 12.7% | 19.9% | 41.0% |
| Employee of the ward/section entrusted with reporting the occurrence of HAI | 8.4% | 12.7% | 8.4% | 32.5% | 38.0% |
| Occurrence of HAI is reported by the attending physician | 3.6% | 10.2% | 18.1% | 28.3% | 39.8% |
| Regular audits are performed by an expert for HAI prevention | 5.3% | 14.5% | 13.9% | 22.3% | 44.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krocová, J.; Prokešová, R. Aspects of Prevention of Urinary Tract Infections Associated with Urinary Bladder Catheterisation and Their Implementation in Nursing Practice. Healthcare 2022, 10, 152. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010152
Krocová J, Prokešová R. Aspects of Prevention of Urinary Tract Infections Associated with Urinary Bladder Catheterisation and Their Implementation in Nursing Practice. Healthcare. 2022; 10(1):152. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010152
Chicago/Turabian StyleKrocová, Jitka, and Radka Prokešová. 2022. "Aspects of Prevention of Urinary Tract Infections Associated with Urinary Bladder Catheterisation and Their Implementation in Nursing Practice" Healthcare 10, no. 1: 152. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010152