
Effects of Patient-Generated Health Data: Comparison of Two Versions of Long-Term Mobile Personal Health Record Usage Logs

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of the “My Chart in My Hand” Application
2.2. Study Design and Procedure
2.3. Statistical Method
3. Results
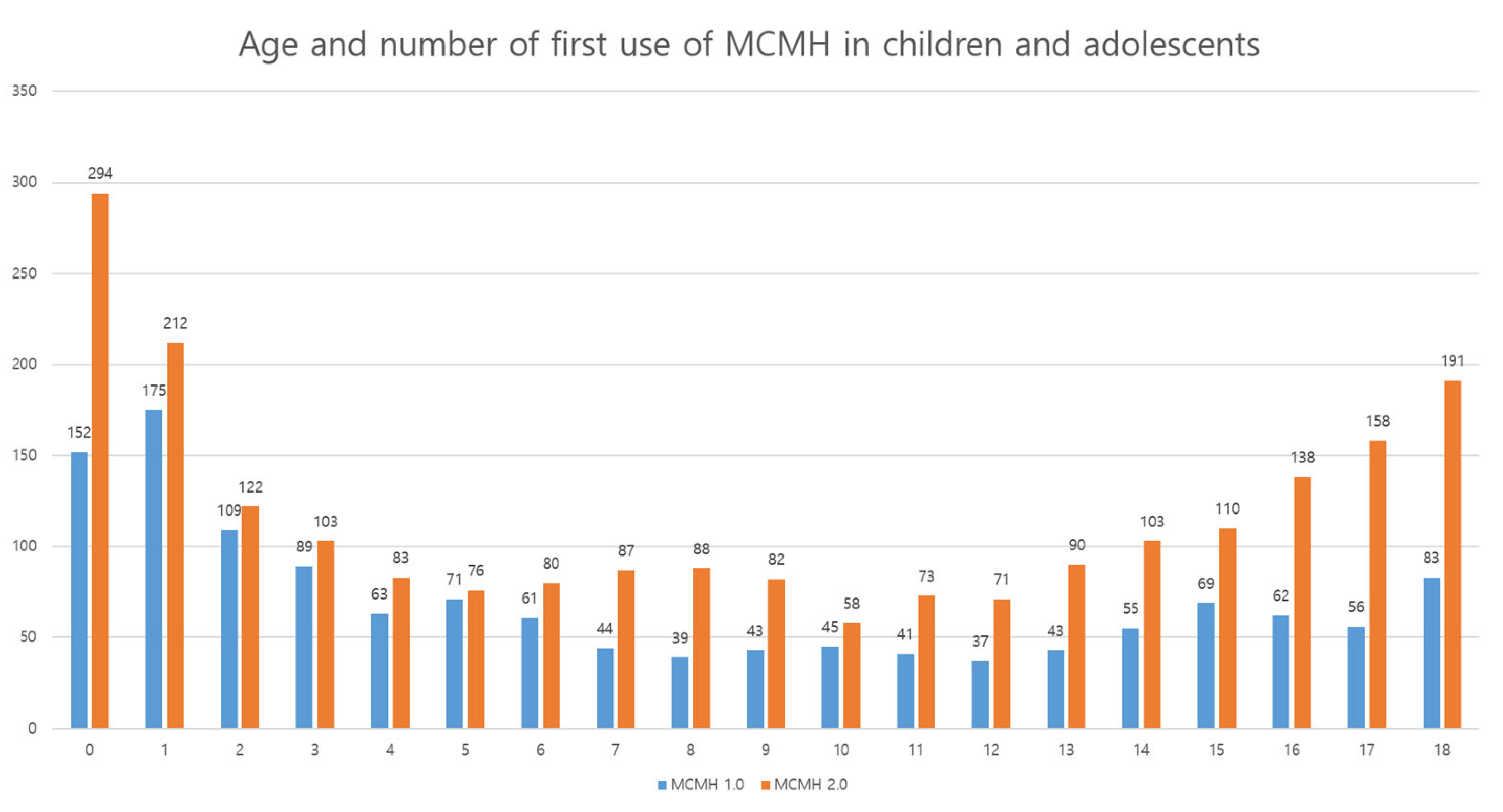
3.1. User Characteristics
3.2. Overall Usage Trend
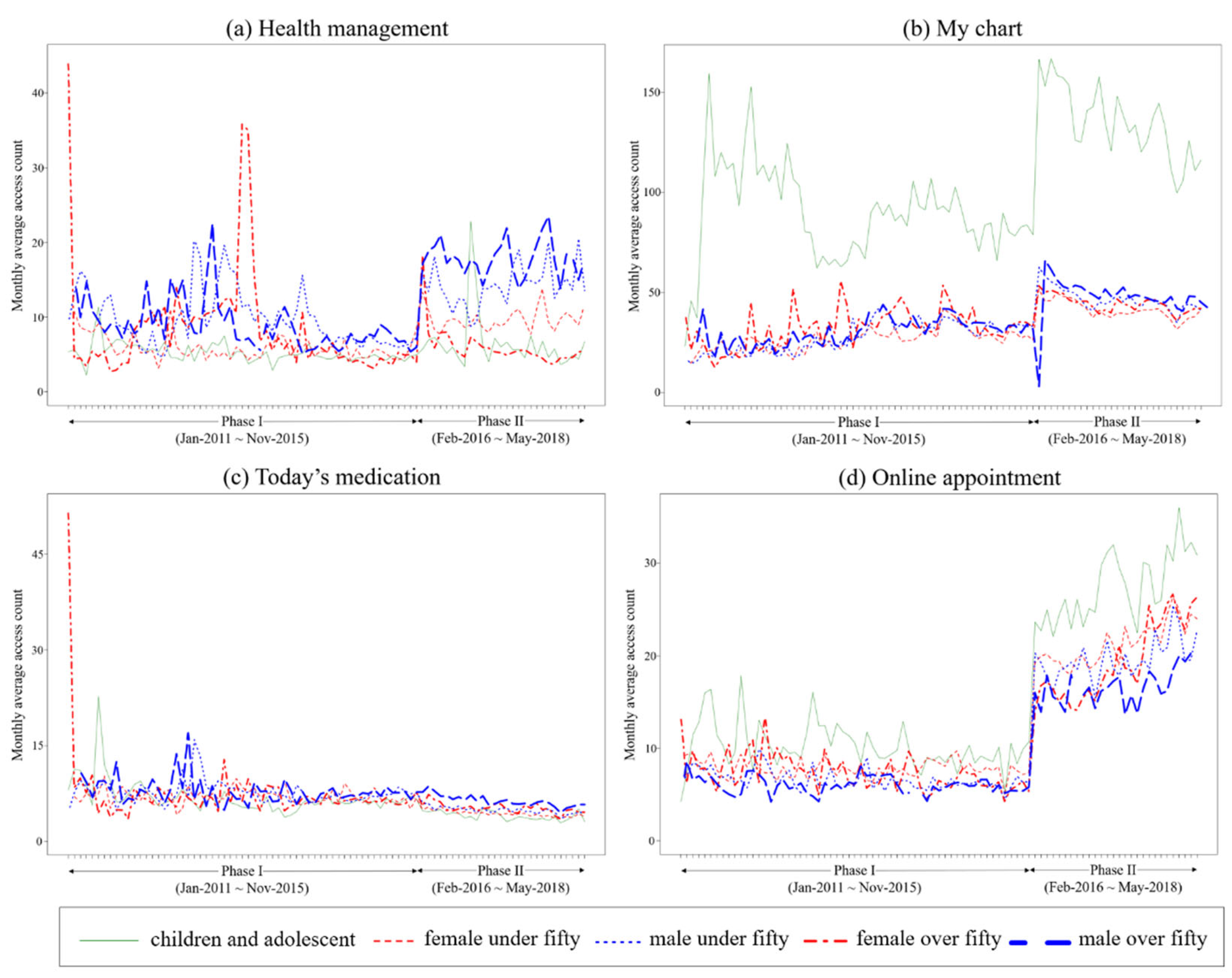
3.3. Monthly Average Access Count
3.4. Monthly Access Count per User
3.5. Changes in Functions’ Usage in MCMH According to Version-Up
4. Discussion
4.1. Principal Findings
4.2. Usage Trends of the MCMH According to Version-Up
4.3. Usage Pattern
4.4. Monthly Average Access Count and Monthly Access Count per User
4.5. Effect of PGHD in mPHR
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Tang, P.C.; Ash, J.S.; Bates, D.W.; Overhage, J.M.; Sands, D.Z. Personal health records: Definitions, benefits, and strategies for overcoming barriers to adoption. J. Am. Med. Inform. Assoc. 2006, 13, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Archer, N.; Fevrier-Thomas, U.; Lokker, C.; McKibbon, K.A.; Straus, S.E. Personal health records: A scoping review. J. Am. Med. Inform. Assoc. 2011, 18, 515–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spallek, H.; O’Donnell, J.; Clayton, M.; Anderson, P.; Krueger, A. Paradigm Shift or Annoying Distraction Emerging Implications of Web 2.0 for Clinical Practice. Appl. Clin. Inform. 2010, 1, 96–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.R.; Lee, Y.; Kim, J.Y.; Kim, J.; Kim, H.R.; Kim, Y.H.; Kim, W.S.; Lee, J.H. Managing Patient-Generated Health Data through Mobile Personal Health Records: Analysis of Usage Data. Jmir Mhealth Uhealth 2018, 6, e9620. [Google Scholar] [CrossRef] [PubMed]
- Zakerabasali, S.; Ayyoubzadeh, S.M.; Baniasadi, T.; Yazdani, A.; Abhari, S. Mobile Health Technology and Healthcare Providers: Systemic Barriers to Adoption. Healthc. Inform. Res. 2021, 27, 267–278. [Google Scholar] [CrossRef]
- Choi, B.K.; Park, Y.T.; Kwon, L.S.; Kim, Y.S. Analysis of Platforms and Functions of Mobile Based Personal Health Record Systems. Healthc. Inform. Res. 2020, 26, 311–320. [Google Scholar] [CrossRef]
- Kharrazi, H.; Chisholm, R.; VanNasdale, D.; Thompson, B. Mobile personal health records: An evaluation of features and functionality. Int. J. Med. Inform. 2012, 81, 579–593. [Google Scholar] [CrossRef]
- Kao, C.K.; Liebovitz, D.M. Consumer Mobile Health Apps: Current State, Barriers, and Future Directions. PmR 2017, 9, S106–S115. [Google Scholar] [CrossRef]
- Kim, J.; Lim, S.; Min, Y.H.; Shin, Y.W.; Lee, B.; Sohn, G.; Jung, K.H.; Lee, J.H.; Son, B.H.; Ahn, S.H.; et al. Depression Screening Using Daily Mental-Health Ratings from a Smartphone Application for Breast Cancer Patients. J. Med. Internet Res. 2016, 18, e5598. [Google Scholar] [CrossRef]
- Torkamani, A.; Andersen, K.G.; Steinhubl, S.R.; Topol, E.J. High-Definition Medicine. Cell 2017, 170, 828–843. [Google Scholar] [CrossRef]
- Singh, K.; Drouin, K.; Newmark, L.P.; Filkins, M.; Silvers, E.; Bain, P.A.; Zulman, D.M.; Lee, J.H.; Rozenblum, R.; Pabo, E.; et al. Patient-Facing Mobile Apps to Treat High-Need, High-Cost Populations: A Scoping Review. Jmir Mhealth Uhealth 2016, 4, e136. [Google Scholar] [CrossRef] [Green Version]
- Chunara, R.; Wisk, L.E.; Weitzman, E.R. Denominator Issues for Personally Generated Data in Population Health Monitoring. Am. J. Prev. Med. 2017, 52, 549–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.; Kwon, H.; Lee, B.; Lee, G.; Lee, J.H.; Park, Y.R.; Shin, S.Y. Effect of self-monitoring on long-term patient engagement with mobile health applications. PLoS ONE 2018, 13, e0201166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, M.; Rhee, S.Y. Effect of Adherence to Smartphone App Use on the Long-term Effectiveness of Weight Loss in Developing and OECD Countries: Retrospective Cohort Study. Jmir Mhealth Uhealth 2021, 9, e13496. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Kang, D.; Kim, S.; Lim, J.; Yoon, J.; Kim, Y.; Shim, S.; Kang, E.; Ahn, J.S.; Cho, J.; et al. Who is more likely to adopt and comply with the electronic patient-reported outcome measure (ePROM) mobile application? A real-world study with cancer patients undergoing active treatment. Supportive Care Cancer 2022, 30, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Deng, N.; Cui, T.R.; Qian, S.Y.; Liu, F.; Guan, Y.P.; Yu, P. Measuring Success of Patients’ Continuous Use of Mobile Health Services for Self-management of Chronic Conditions: Model Development and Validation. J. Med. Internet Res. 2021, 23, e26670. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Shin, S.Y.; Kim, J.Y.; Kim, J.H.; Seo, D.W.; Joo, S.; Park, J.Y.; Kim, W.S.; Lee, J.H.; Bates, D.W. Evaluation of Mobile Health Applications Developed by a Tertiary Hospital as a Tool for Quality Improvement Breakthrough. Healthc. Inform. Res. 2015, 21, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.; Park, J.Y.; Shin, S.Y.; Hwang, J.S.; Ryu, H.J.; Lee, J.H.; Bates, D.W. Which Users Should Be the Focus of Mobile Personal Health Records? Analysis of User Characteristics Influencing Usage of a Tethered Mobile Personal Health Record. Telemed. E-Health 2016, 22, 419–428. [Google Scholar] [CrossRef] [Green Version]
- Bouri, N.; Ravi, S. Going Mobile: How Mobile Personal Health Records Can Improve Health Care during Emergencies. Jmir Mhealth Uhealth 2014, 2, e3017. [Google Scholar] [CrossRef]
- Graetz, I.; Huang, J.; Brand, R.; Hsu, J.; Reed, M.E. Mobile-accessible personal health records increase the frequency and timeliness of PHR use for patients with diabetes. J. Am. Med. Inform. Assoc. 2019, 26, 50–54. [Google Scholar] [CrossRef]
- Office of the National Coordinator for Health Information Technology. Conceptualizing a Data Infrastructure for the Capture, Use, and Sharing of Patient-Generated Health Data in Care Delivery and Research through 2024. Available online: https://www.healthit.gov/sites/default/files/pghd_white_paper_final_formatted_by_onc_508_11-29-17.pdf (accessed on 16 December 2021).
- Onodera, R.; Sengoku, S. Innovation process of mHealth: An overview of FDA-approved mobile medical applications. Int. J. Med. Inform. 2018, 118, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Redelmeier, D.A.; Kraus, N.C. Patterns in Patient Access and Utilization of Online Medical Records: Analysis of MyChart. J. Med. Internet Res. 2018, 20, e43. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R. Kaiser Permanente Northern California: Current Experiences With Internet, Mobile, and Video Technologies. Health Aff. 2014, 33, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Silvestre, A.L.; Sue, V.M.; Allen, J.Y. If You Build It, Will They Come? The Kaiser Permanente Model of Online Health Care. Health Aff. 2009, 28, 334–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ketterer, T.; West, D.W.; Sanders, V.P.; Hossain, J.; Kondo, M.A.; Sharif, I. Correlates of Patient Portal Enrollment and Activation in Primary Care Pediatrics. Acad. Pediatrics 2013, 13, 264–271. [Google Scholar] [CrossRef]
- Hawkins, M. Survey of Physician Appointment Wait Times. Available online: https://www.merritthawkins.com/uploadedFiles/MerrittHawkins/Content/Pdf/mha2017waittimesurveyPDF.pdf (accessed on 16 December 2021).
- Jung, C.M.; Padman, R. Virtualized healthcare delivery: Understanding users and their usage patterns of online medical consultations. Int. J. Med. Inform. 2014, 83, 901–914. [Google Scholar] [CrossRef]
- Wildenbos, G.A.; Peute, L.; Jaspers, M. Aging barriers influencing mobile health usability for older adults: A literature based framework (MOLD-US). Int. J. Med. Inform. 2018, 114, 66–75. [Google Scholar] [CrossRef]
- Rogers, W.A.; Fisk, A.D. Toward a Psychological Science of Advanced Technology Design for Older Adults. J. Gerontol. Ser. B-Psychol. Sci. Soc. Sci. 2010, 65, 645–653. [Google Scholar] [CrossRef] [Green Version]
- Grindrod, K.A.; Li, M.; Gates, A. Evaluating User Perceptions of Mobile Medication Management Applications with Older Adults: A Usability Study. Jmir Mhealth Uhealth 2014, 2, e3048. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MCMH 1 1.0 | MCMH 1 2.0 | |
|---|---|---|
| Operating system | Android | Android + iOS |
| User | Available to the general public | Only patients registered in the hospital |
| Chronic disease management | Primitive | Cancer, diabetes, pediatric asthma/atopic dermatitis, health promotion |
| Key values | Patient empowerment (access to medical information) | Patient engagement (diary, survey) |
| OPD 2 support | OPD 2 waiting list | Information and guide, my schedule, payment |
| Changes during the version-up |
| |
| MCMH 1.0 (59 Months) | MCMH 2.0 (28 Months) | Total (87 Months) | p-Value | |
|---|---|---|---|---|
| Users, n | 15,357 | 51,553 | 66,910 | - |
| Age, years (mean ± standard deviation) | 41.7 ± 16.7 | 45.6 ± 15.6 | 45.0 ± 16.0 | <0.001 |
| Sex, n (%) | - | - | - | <0.001 |
| Male | 8364 (54.5) | 25,961 (50.4) | 34,325 (51.3) | - |
| Female | 6993 (45.5) | 25,592 (49.6) | 32,585 (48.7) | - |
| Group, n (%) | - | - | - | <0.001 |
| Children and adolescents (<19 years) | 1337 (8.7) | 2219 (4.3) | 3556 (5.3) | - |
| Females under 50 (19–50 years) | 4494 (29.3) | 15,604 (30.3) | 20,098 (30.0) | - |
| Males under 50 (19–50 years) | 4148 (27.0) | 11,780 (22.9) | 15,928 (23.8) | - |
| Females over 50 (50 years or older) | 1895 (12.3) | 8972 (17.4) | 10,867 (16.2) | - |
| Males over 50 (50 years or older) | 3483 (22.7) | 12,978 (25.2) | 16,461 (24.6) | - |
| MCMH 1.0 | MCMH 2.0 | Fold Increase | |||
|---|---|---|---|---|---|
| Total Access Count | Access Count /Month | Total Access Count | Access Count /Month | ||
| Login | 849,134 | 14,640 | 3,672,568 | 131,163 | 8.96 |
| Functions | 4,240,403 | 73,110 | 18,518,700 | 661,382 | 9.05 |
| Health management | 233,953 | 4034 | 529,139 | 18,898 | 4.68 |
| Blood sugar test | 68,532 | 1182 | 203,499 | 7268 | 6.15 |
| Blood pressure | 39,738 | 685 | 194,464 | 6945 | 10.14 |
| Body mass index | 78,003 | 1345 | 74,369 | 2656 | 1.97 |
| 10 CVD 1 risk | 26,019 | 449 | 32,554 | 1163 | 2.59 |
| Metabolic syndrome | 21,661 | 373 | 24,253 | 866 | 2.32 |
| My chart | 3,352,838 | 57,808 | 16,248,385 | 580,300 | 10.04 |
| Laboratory results | 3,158,288 | 54,453 | 15,653,989 | 559,071 | 10.27 |
| Condition | 148,618 | 2562 | 352,642 | 12,594 | 4.92 |
| Allergies | 45,932 | 792 | 241,754 | 8634 | 10.92 |
| Today’s medication | 235,483 | 4060 | 292,180 | 10,435 | 2.57 |
| Online appointment | 418,129 | 7209 | 1,448,996 | 51,750 | 7.18 |
| Groups | Health Management | My Chart | Today’s Medication | Online Appointment | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MCMH 1.0 | MCMH 2.0 | p-Value | MCMH 1.0 | MCMH 2.0 | p-Value | MCMH 1.0 | MCMH 2.0 | p-Value | MCMH 1.0 | MCMH 2.0 | p-Value | |
| Children and adolescents | 5.0 (4.5–5.8) | 5.7 (4.6–6.7) | 0.087 | 89.7 (78.6–104.4) | 134.6 (124.0–149.3) | <0.001 | 6.3 (5.7–7.2) | 3.9 (3.4–4.6) | <0.001 | 9.8 (8.7–11.4) | 26.1 (24.6–30.4) | <0.001 |
| Females under 50 | 5.6 (4.8–6.5) | 9.4 (8.7–10.5) | <0.001 | 26.3 (22.3–28.7) | 41.1 (38.4–44.3) | <0.001 | 6.8 (6.1–7.7) | 4.3 (4.0–4.5) | <0.001 | 7.8 (7.2–8.4) | 21.1 (19.4–22.8) | <0.001 |
| Males under 50 | 8.6 (7.1–11.0) | 13.9 (12.6–15.2) | <0.001 | 28.3 (10.7–33.7) | 45.2 (43.3–49.3) | <0.001 | 7.5 (6.6–8.4) | 4.8 (4.6–5.2) | <0.001 | 6.4 (5.9–7.0) | 19.3 (18.5–20.5) | <0.001 |
| Females over 50 | 5.8 (4.4–9.9) | 5.3 (4.8–6.0) | 0.381 | 32.5 (26.6–37.1) | 44.4 (41.2–46.4) | <0.001 | 6.5 (5.9–7.5) | 5.1 (4.8–5.5) | 0.006 | 7.1 (6.0–8.4) | 18.1 (16.1–23.0) | <0.001 |
| Males over 50 | 7.9 (6.8–10.0) | 17.7 (16.6–19.0) | <0.001 | 30.3 (24.6–34.5) | 48.0 (46.5–51.9) | <0.001 | 7.7 (6.6–8.4) | 6.2 (5.8–7.0) | <0.001 | 6.0 (5.4–6.6) | 16.3 (15.6–17.9) | <0.001 |
| Total | 6.4 (5.0–9.1) | 9.5 (5.9–14.9) | <0.001 | 31.6 (24.8–41.3) | 46.5 (42.0–53.5) | <0.001 | 6.9 (6.1–8.0) | 4.8 (4.2–5.5) | <0.001 | 7.2 (6.1–8.6) | 19.9 (17.7–23.7) | <0.001 |
| Groups | Health Management | My Chart | Today’s Medication | Online Appointment | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MCMH 1.0 | MCMH 2.0 | p-Value | MCMH 1.0 | MCMH 1.0 | MCMH 2.0 | p-Value | MCMH 1.0 | MCMH 1.0 | MCMH 2.0 | |||
| Children and adolescents | 3 (1–7) | 3 (1–6) | <0.001 | 27 (8–88) | Children and adolescents | 3 (1–7) | 3 (1–6) | <0.001 | 27 (8–88) | Children and adolescents | 3 (1–7) | 3 (1–6) |
| Females under 50 | 3 (1–6) | 2 (1–5) | <0.001 | 13 (5–31) | Females under 50 | 3 (1–6) | 2 (1–5) | <0.001 | 13 (5–31) | Females under 50 | 3 (1–6) | 2 (1–5) |
| Males under 50 | 3 (1–7) | 3 (1–6) | <0.001 | 13 (5–32) | Males under 50 | 3 (1–7) | 3 (1–6) | <0.001 | 13 (5–32) | Males under 50 | 3 (1–7) | 3 (1–6) |
| Females over 50 | 2 (1–5) | 2 (1–4) | <0.001 | 15 (5–35) | Females over 50 | 2 (1–5) | 2 (1–4) | <0.001 | 15 (5–35) | Females over 50 | 2 (1–5) | 2 (1–4) |
| Males over 50 | 3 (1–6) | 3 (1–6) | 0.115 | 15 (6–35) | Males over 50 | 3 (1–6) | 3 (1–6) | 0.115 | 15 (6–35) | Males over 50 | 3 (1–6) | 3 (1–6) |
| Total | 3 (1–6) | 2 (1–5) | <0.001 | 15 (6–37) | Total | 3 (1–6) | 2 (1–5) | <0.001 | 15 (6–37) | Total | 3 (1–6) | 2 (1–5) |
| My Chart in My Hand | |||||
|---|---|---|---|---|---|
| Odds Ratio | 95 % CI 1 | p Value | |||
| Lower | Upper | ||||
| Version | 0.726 | 0.713 | 0.740 | <0.001 | |
| Age | 0.998 | 0.998 | 0.999 | <0.001 | |
| Gender | Male | 1.011 | 0.994 | 1.029 | 0.203 |
| Female | 1.000 | - | - | - | |
| HM 2 | 1.134 | 1.092 | 1.178 | <0.001 | |
| Version HM 2 | 1.245 | 1.188 | 1.306 | <0.001 | |
| MC 3 | 1.288 | 1.252 | 1.325 | <0.001 | |
| Version * MC 3 | 1.040 | 1.010 | 1.072 | 0.0093 | |
| TM 4 | 1.186 | 1.152 | 1.222 | <0.001 | |
| Version * TM 4 | 1.050 | 1.014 | 1.087 | 0.0058 | |
| OA 5 | 1.328 | 1.296 | 1.361 | <0.001 | |
| Version * OA 5 | 0.925 | 0.898 | 0.953 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-H.; Lee, Y.; Oh, J.S.; Seo, D.-W.; Lee, K.H.; Kim, Y.-H.; Kim, W.S.; Lee, J.-H. Effects of Patient-Generated Health Data: Comparison of Two Versions of Long-Term Mobile Personal Health Record Usage Logs. Healthcare 2022, 10, 53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010053
Kim D-H, Lee Y, Oh JS, Seo D-W, Lee KH, Kim Y-H, Kim WS, Lee J-H. Effects of Patient-Generated Health Data: Comparison of Two Versions of Long-Term Mobile Personal Health Record Usage Logs. Healthcare. 2022; 10(1):53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010053
Chicago/Turabian StyleKim, Do-Hoon, Yura Lee, Ji Seon Oh, Dong-Woo Seo, Kye Hwa Lee, Young-Hak Kim, Woo Sung Kim, and Jae-Ho Lee. 2022. "Effects of Patient-Generated Health Data: Comparison of Two Versions of Long-Term Mobile Personal Health Record Usage Logs" Healthcare 10, no. 1: 53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010053