
SGLT2 Inhibitors in Acute Heart Failure: A Meta-Analysis of Randomized Controlled Trials

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Statistical Analysis
2.5. Risk of Bias Assessment
3. Results
3.1. PRISMA
3.2. Risk of Bias
3.3. Baseline Characteristics
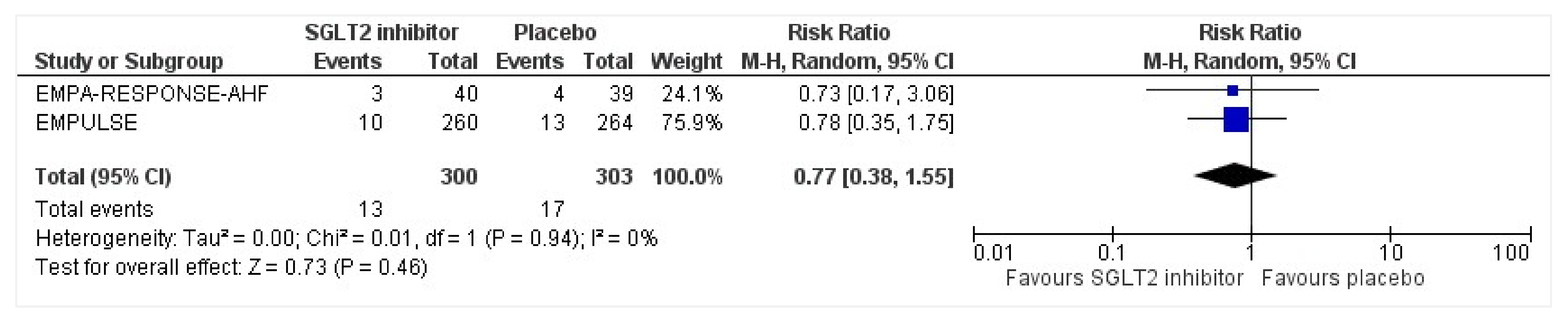
3.4. All-Cause Mortality
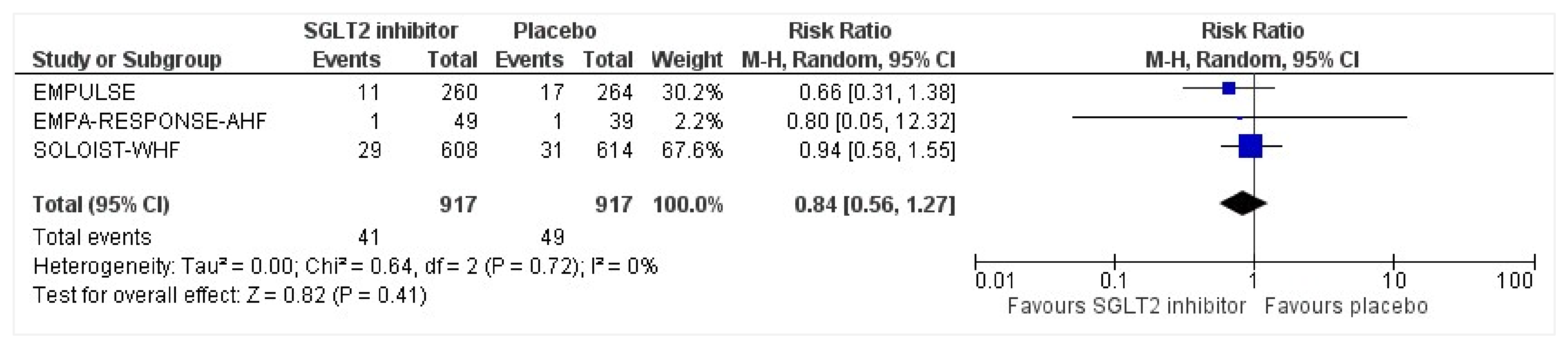
3.5. Heart Failure Events
3.6. Readmissions
3.7. Kansas City Cardiomyopathy Questionnaire Total Symptom Score (KCCQ TSS)
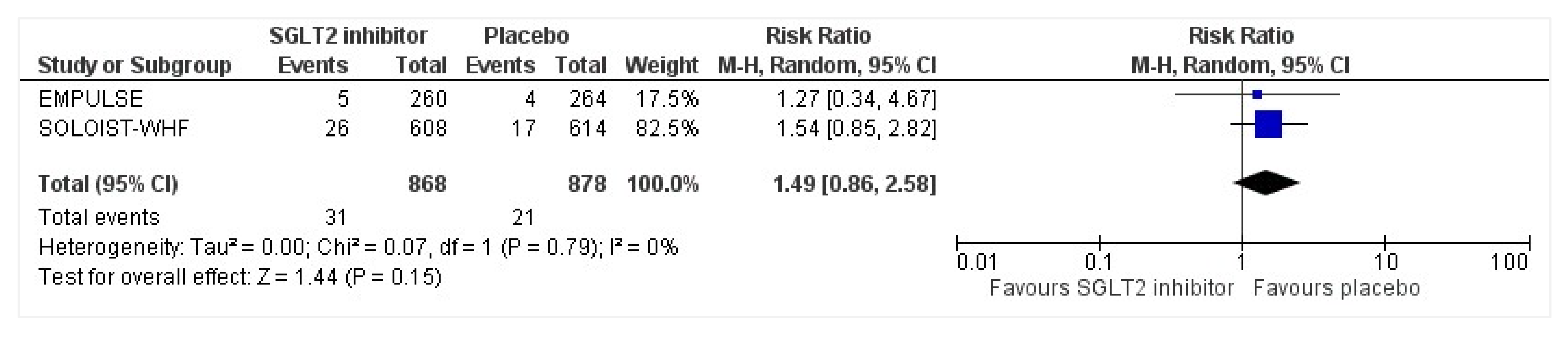
3.8. Serious Adverse Events
3.9. Ongoing Clinical Trials of SGLT2 inhibitors and Heart Failure
4. Discussion
4.1. Clinical Practice Recommendations
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fountoulaki, K.; Ventoulis, I.; Drokou, A.; Georgarakou, K.; Parissis, J.; Polyzogopoulou, E. Emergency Department Risk Assessment and Disposition of Acute Heart Failure Patients: Existing Evidence and Ongoing Challenges. Heart Fail. Rev. 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Arrigo, M.; Jessup, M.; Mullens, W.; Reza, N.; Shah, A.M.; Sliwa, K.; Mebazaa, A. Acute Heart Failure. Nat. Rev. Dis. Prim. 2020, 6, 16. [Google Scholar] [CrossRef]
- Farmakis, D.; Papingiotis, G.; Parissis, J. Acute Heart Failure: Epidemiology and Socioeconomic Burden. Contin. Cardiol. Educ. 2017, 3, 88–92. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.S.; Sreenivasan, J.; Lateef, N.; Abougergi, M.S.; Greene, S.J.; Ahmad, T.; Anker, S.D.; Fonarow, G.C.; Butler, J. Trends in 30-and 90-Day Readmission Rates for Heart Failure. Circ. Heart Fail. 2021, 14, e008335. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, Y.; Kohsaka, S.; Sato, N.; Takano, T.; Kitai, T.; Yoshikawa, T.; Matsue, Y. 9-year Trend in the Management of Acute Heart Failure in Japan: A Report from the National Consortium of Acute Heart Failure Registries. J. Am. Heart Assoc. 2018, 7, e008687. [Google Scholar] [CrossRef] [Green Version]
- Bytyçi, I.; Bajraktari, G. Mortality in Heart Failure Patients. Anatol. J. Cardiol. 2015, 15, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buddeke, J.; Valstar, G.B.; Van Dis, I.; Visseren, F.L.J.; Rutten, F.H.; Den Ruijter, H.M.; Vaartjes, I.; Bots, M.L. Mortality after Hospital Admission for Heart Failure: Improvement over Time, Equally Strong in Women as in Men. BMC Public Health 2020, 20, 36. [Google Scholar] [CrossRef] [Green Version]
- Tsutsui, H. Recent Advances in the Pharmacological Therapy of Chronic Heart Failure: Evidence and Guidelines. Pharmacol. Ther. 2022, 238, 108185. [Google Scholar] [CrossRef]
- Mazza, A.; Townsend, D.M.; Torin, G.; Schiavon, L.; Camerotto, A.; Rigatelli, G.; Cuppini, S.; Minuz, P.; Rubello, D. The Role of Sacubitril/Valsartan in the Treatment of Chronic Heart Failure with Reduced Ejection Fraction in Hypertensive Patients with Comorbidities: From Clinical Trials to Real-World Settings. Biomed. Pharmacother. 2020, 130, 110596. [Google Scholar] [CrossRef]
- Mullens, W.; Damman, K.; Harjola, V.; Mebazaa, A.; Brunner-La Rocca, H.; Martens, P.; Testani, J.M.; Tang, W.H.W.; Orso, F.; Rossignol, P. The Use of Diuretics in Heart Failure with Congestion—A Position Statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 137–155. [Google Scholar] [CrossRef] [Green Version]
- Felker, G.M.; O’Connor, C.M.; Braunwald, E. Loop Diuretics in Acute Decompensated Heart Failure: Necessary? Evil? A Necessary Evil? Circ. Heart Fail. 2009, 2, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Chiong, J.R.; Cheung, R.J. Loop Diuretic Therapy in Heart Failure: The Need for Solid Evidence on a Fluid Issue. Clin. Cardiol. 2010, 33, 345–352. [Google Scholar] [CrossRef]
- Boorsma, E.M.; Beusekamp, J.C.; Ter Maaten, J.M.; Figarska, S.M.; Danser, A.H.J.; van Veldhuisen, D.J.; van Der Meer, P.; Heerspink, H.J.L.; Damman, K.; Voors, A.A. Effects of Empagliflozin on Renal Sodium and Glucose Handling in Patients with Acute Heart Failure. Eur. J. Heart Fail. 2021, 23, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Ghani, M.A.; Norton, L.; DeFronzo, R.A. Renal Sodium-Glucose Cotransporter Inhibition in the Management of Type 2 Diabetes Mellitus. Am. J. Physiol. Physiol. 2015, 309, F889–F900. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Lee, T.; DeFronzo, R.A. Why Do SGLT2 Inhibitors Inhibit Only 30–50% of Renal Glucose Reabsorption in Humans? Diabetes 2012, 61, 2199–2204. [Google Scholar] [CrossRef] [Green Version]
- Gallo, L.A.; Wright, E.M.; Vallon, V. Probing SGLT2 as a Therapeutic Target for Diabetes: Basic Physiology and Consequences. Diabetes Vasc. Dis. Res. 2015, 12, 78–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez Lopez, G.; Gonzalez Albarran, O.; Cano Megias, M. Type 2 Sodium-Glucose Cotransporter (SGLT2) Inhibitors: From Familial Renal Glucosuria to the Treatment of Type 2 Diabetes Mellitus. Nefrologia 2010, 30, 618–625. [Google Scholar] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savarese, G.; Sattar, N.; Januzzi, J.; Verma, S.; Lund, L.H.; Fitchett, D.; Zeller, C.; George, J.T.; Brueckmann, M.; Ofstad, A.P. Empagliflozin Is Associated with a Lower Risk of Post-Acute Heart Failure Rehospitalization and Mortality: Insights from the EMPA-REG OUTCOME Trial. Circulation 2019, 139, 1458–1460. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- FDA. FDA Approves Treatment for Wider Range of Patients with Heart Failure. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-treatment-wider-range-patients-heart-failure (accessed on 7 October 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Cochrane RoB 2: A Revised Cochrane Risk-of-Bias Tool for Randomized Trials. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 7 August 2022).
- Voors, A.A.; Angermann, C.E.; Teerlink, J.R.; Collins, S.P.; Kosiborod, M.; Biegus, J.; Ferreira, J.P.; Nassif, M.E.; Psotka, M.A.; Tromp, J. The SGLT2 Inhibitor Empagliflozin in Patients Hospitalized for Acute Heart Failure: A Multinational Randomized Trial. Nat. Med. 2022, 28, 568–574. [Google Scholar] [CrossRef]
- Damman, K.; Beusekamp, J.C.; Boorsma, E.M.; Swart, H.P.; Smilde, T.D.J.; Elvan, A.; van Eck, J.W.M.; Heerspink, H.J.L.; Voors, A.A. Randomized, Double-blind, Placebo-controlled, Multicentre Pilot Study on the Effects of Empagliflozin on Clinical Outcomes in Patients with Acute Decompensated Heart Failure (EMPA-RESPONSE-AHF). Eur. J. Heart Fail. 2020, 22, 713–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef]
- Kosiborod, M.N.; Angermann, C.E.; Collins, S.P.; Teerlink, J.R.; Ponikowski, P.; Biegus, J.; Comin-Colet, J.; Ferreira, J.P.; Mentz, R.J.; Nassif, M.E. Effects of Empagliflozin on Symptoms, Physical Limitations and Quality of Life in Patients Hospitalized for Acute Heart Failure-Results from the EMPULSE Trial. Circulation 2022, 146, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Tromp, J.; Ponikowski, P.; Salsali, A.; Angermann, C.E.; Biegus, J.; Blatchford, J.; Collins, S.P.; Ferreira, J.P.; Grauer, C.; Kosiborod, M. Sodium–Glucose Co-transporter 2 Inhibition in Patients Hospitalized for Acute Decompensated Heart Failure: Rationale for and Design of the EMPULSE Trial. Eur. J. Heart Fail. 2021, 23, 826–834. [Google Scholar] [CrossRef]
- Cox, Z.L.; Collins, S.P.; Aaron, M.; Hernandez, G.A.; McRae, A.T., III; Davidson, B.T.; Fowler, M.; Lindsell, C.J.; Harrell, F.E., Jr.; Jenkins, C.A. Efficacy and Safety of Dapagliflozin in Acute Heart Failure: Rationale and Design of the DICTATE-AHF Trial. Am. Heart J. 2021, 232, 116–124. [Google Scholar] [CrossRef]
- Spertus, J.A.; Birmingham, M.C.; Nassif, M.; Damaraju, C.V.; Abbate, A.; Butler, J.; Lanfear, D.E.; Lingvay, I.; Kosiborod, M.N.; Januzzi, J.L. The SGLT2 Inhibitor Canagliflozin in Heart Failure: The CHIEF-HF Remote, Patient-Centered Randomized Trial. Nat. Med. 2022, 28, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, S.; Yamada, T.; Watanabe, T.; Morita, T.; Furukawa, Y.; Kawasaki, M.; Kikuchi, A.; Kawai, T.; Seo, M.; Abe, M. Effect of Empagliflozin as an Add-on Therapy on Decongestion and Renal Function in Patients with Diabetes Hospitalized for Acute Decompensated Heart Failure: A Prospective Randomized Controlled Study. Circ. Heart Fail. 2021, 14, e007048. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.S.; Singh, T.; Newby, D.E.; Singh, J. Sodium-Glucose Co-Transporter 2 Inhibitor Therapy: Mechanisms of Action in Heart Failure. Heart 2021, 107, 1032–1038. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EMPULSE | EMPA-RESPONSE-AHF | SOLOIST-WHF | |
|---|---|---|---|
| Clinical trial identifier | NCT04157751 | NCT03200860 | NCT03521934 |
| Author-year | Voors-2022 [25] | Damman-2020 [26] | Bhatt-2021 [27] |
| Country | The Netherlands | The Netherlands | United States of America |
| Dose of SGLT2 | 10 mg Empagliflozin | 10 mg Empagliflozin | 200–400 mg Sotagliflozin |
| Frequency of intervention | Every day for 90 days | Every day for 30 days | Every day for 8 months with uptritation depending on side effects |
| Total sample size | 530 | 79 | 1222 |
| Intervention arm sample size | 265 | 40 | 608 |
| Control arm sample size | 265 | 39 | 614 |
| Follow-up duration | 90 days | 60 days | 9 months |
| Primary outcome(s) | Clinical benefit is defined as a hierarchical composite of all-cause mortality, number of heart failure events, and time to a first heart failure event, or a 5-point or more difference in baseline score of KCCQ-TSS | Change in visual analog scale (VAS) dyspnea score, diuretic response, the percentage change in N-terminal pro-brain natriuretic peptide (NT-proBNP), and length of hospital stay | Total number of deaths from cardiovascular causes and hospitalizations and urgent visits for heart failure |
| Secondary outcome(s) | Cardiovascular death or HFE, KCCQ-TSS improvement of 10 or more points, reduction in NT-proBNP concentration, hospitalization for HF, and diuretic response | Worsening HF, all-cause mortality, and HF readmission | Number of hospitalizations and urgent visits for HF, cardiovascular death, all-cause mortality, and change in KCCQ-TSS score |
| Sr. No. | NCT Number | Title | Acronym | Status | Conditions | Interventions |
|---|---|---|---|---|---|---|
| 1 | NCT04298229 | Efficacy and Safety of Dapagliflozin in Acute Heart Failure | DICTATE-AHF | Recruiting | Heart Failure, Diabetes Mellitus Type 2 | Dapagliflozin 10 mg; protocolized diuretic therapy |
| 2 | NCT05392764 | Early Treatment with a Sodium-glucose Co-transporter 2 Inhibitor in High-risk Patients With Acute Heart Failure | EMPA-AHF | Recruiting | Acute Heart Failure | Empagliflozin 10 mg; placebo |
| 3 | NCT05556044 | Empagliflozin for New On-set Heart Failure Study Regardless of Ejection Fraction | EMPA | Recruiting | Acute Heart Failure | Empagliflozin 10 mg |
| 4 | NCT05406505 | Effect of Dapagliflozin in Patients With Acute Heart Failure (DAPA-RESPONSE-AHF) | Recruiting | Acute Decompensated Heart Failure | Dapagliflozin 10 mg; placebo | |
| 5 | NCT04899479 | Peri-treatment of SGLT-2 Inhibitor on Myocardial Infarct Size and Remodeling Index in Patients With Acute Myocardial Infarction and High Risk of Heart Failure Undergoing Percutaneous Coronary Intervention | PRESTIGE-AMI | Recruiting | Acute Myocardial Infarction, Heart Failure | SGLT2 inhibitor; control |
| 6 | NCT05346653 | The Hemodynamic Effects of SGLT2i in Acute Decompensated Heart Failure | Not yet recruiting | Acute Decompensated Heart Failure | SGLT2 inhibitor; control | |
| 7 | NCT05305495 | Empagliflozin in Acute Heart Failure | DRIP-AHF-1 | Not yet recruiting | Acute Heart Failure, Chronic Kidney Diseases | Empagliflozin 25 mg |
| 8 | NCT04363697 | Dapagliflozin and Effect on Cardiovascular Events in Acute Heart Failure -Thrombolysis in Myocardial Infarction 68 (DAPA ACT HF-TIMI 68) | Recruiting | Acute Heart Failure, Heart Failure | Dapagliflozi; placebo | |
| 9 | NCT04782245 | Acute Reno-Cardiac Action of Dapagliflozin In Advanced Heart Failure Patients on Heart Transplant Waiting List | ARCADIA-HF | Not yet recruiting | End-stage Heart Failure | Dapagliflozin 10mg; placebo |
| 10 | NCT04869124 | Dapagliflozin on Volume Vascular Outcomes. | DAPA-VOLVO | Recruiting | Heart Failure, Congestive | Dapagliflozin; placebo |
| 11 | NCT04778787 | Sodium-glucose Cotransporter Type 2 Inhibitors for Acute Cardiorenal Syndrome Prevention | Recruiting | Congestive Heart Failure | Standard list of drugs used for acute decompensation of CHF (loop diuretics, vasodilators, digoxin, inotropic agents, vasopressors), plus dapagliflozin (Forxiga; MP-002596) | |
| 12 | NCT04717986 | Dapagliflozin Effects on Mayor Adverse Cardiovascular Events in Patients with Acute Myocardial Infarction (DAPA-AMI) | DAPA-AMI | Enrolling by invitation | Acute Myocardial Infarction, Cardiovascular Morbidity, Heart Failure, Angina, Unstable | Dapagliflozin 10 mg; placebo |
| 13 | NCT04564742 | Dapagliflozin Effects on Cardiovascular Events in Patients with an Acute Heart Attack | DAPA-MI | Recruiting | Acute Myocardial Infarction, Heart Failure | Dapagliflozin; placebo |
| 14 | NCT04509674 | EMPACT-MI: A Study to Test Whether Empagliflozin Can Lower the Risk of Heart Failure and Death in People Who Had a Heart Attack (Myocardial Infarction) | Recruiting | Myocardial Infarction | Empagliflozin; placebo | |
| 15 | NCT05364190 | Canagliflozin in Patients with Acute Decompensated Heart Failure | Recruiting | Chronic Heart Failure, Acute Decompensated Heart Failure, Diabetes Mellitus | Canagliflozin and Empagliflozin | |
| Sr. No. | NCT Number | Outcome Measures | Phases | Enrollment | Completion Date | Locations |
|---|---|---|---|---|---|---|
| 1 | NCT04298229 | Cumulative change in weight (kilograms); Incidence of worsening heart failure; Hospital readmission | Phase 3 | 240 | 31 January-2023 | United States |
| 2 | NCT05392764 | Within 90 days: Composite endpoint consisting of death, heart failure rehospitalization; WHF during hospitalization, urine output up to 48 h after treatment initiation; worsening NYHA class; Improvement in KCCQ-TSS points from randomization to 30 and 90 days after treatment initiation; Time to hemodynamic stabilization during index hospitalization; Death; Composite of renal replacement therapy, renal transplantation, eGFR <15 mL/min/1.73m2; Trend in eGFR after randomization to 24 h, 48 h, 30 days, and 90 days | Phase 3 | 500 | 1 April 2023 | Japan |
| 3 | NCT05556044 | Heart failure (HF) events; All-cause mortality; KCCQ-TSS total symptom score; NT-proBNP level; New York Heart Association (NYHA) class; Major Adverse Cardiovascular Event (MACE); Occurrence of kidney damage; Weight loss; Quality-adjusted life years (QALY) gained; Change in 6 min hall walk (6MHW) | Phase 3 | 200 | 31 May 2024 | Hong Kong |
| 4 | NCT05406505 | Change in dyspnea- Visual analog scale; Incidence of worsening heart failure (HF); All-cause death; Hospital readmission; Urinary sodium 2 h post randomization; Difference in serum levels of congestion biomarkers | Phase 2/3 | 100 | 5 January 2023 | Egypt |
| 5 | NCT04899479 | Myocardial infarct size; Left ventricular end-systolic volume; Acute kidney injury; Myocardial salvage index (MSI); Microvascular obstruction (MVO); Hemorraghic infarction (HI); Thrombolysis in myocardial infarction (TIMI) flow grade; ST resolution after PCI; left ventricular end-diastolic volume; left ventricular ejection fraction; LV adverse remodeling; LV reverse remodeling; MSI; MVO; Changes of NT-proBNP level; Estimated glomerular filtration rate; Cardiac death or re-hospitalization due to heart failure; All-cause death or re-hospitalization due to heart failure; Target lesion failure; Target vessel failure; All-cause death; Cardiac death; Target vessel; Re-hospitalization due to heart failure; Any re-hospitalization | Phase 4 | 200 | 30 June 2024 | Republic of Korea |
| 6 | NCT05346653 | Change in Indirect Fick cardiac index; Change in pulmonary capillary wedge pressure (PCWP) | Phase 4 | 40 | October 2023 | United States |
| 7 | NCT05305495 | The diuretic effect of empagliflozin in association with furosemide; Fractional excretion of sodium in the urine; Total urine sodium output; Changes in volume status; Incidence of AKI; Electrolyte abnormalities—Sodium; Electrolyte abnormalities- Potassium; Electrolyte abnormalities—Magnesium | Phase 4 | 25 | July 2025 | Canada |
| 8 | NCT04363697 | Cardiovascular (CV) death or worsening heart failure; Composite CV death, rehospitalization for heart failure, urgent heart failure visit; Composite CV death, rehospitalization for heart failure; Rehospitalization for heart failure, urgent heart failure visit; Readmission; CV death; Death | Phase 4 | 2400 | 31 May 2023 | United States |
| 9 | NCT04782245 | Levels of suPAR (ng/mL); VO2 max assessment; assessed by right heart catheterization: cardiac output, pulmonary capillary wedge pressure, pulmonary artery systolic and mean pressure, mean pressure, right atrial pressure; assessed by echocardiograpgy: left ventricular ejection function, left ventricular end-diastolic diameter, left ventricular end-systolic volume, mitral regurgitation grade, left atrial volume; Nt-proBNP level; Creatinine level; Quality of life assessed by KCCQ | Phase 2 | 80 | April 2024 | France |
| 10 | NCT04869124 | Change in relative plasma volume status, blood volume, red blood cell volume, total hemoglobin mass, extracellular to total body water ratio, intracellular to total body water ratio, flicker-light induced retinal arteriolar dilatation, flicker-light induced retinal venular dilatation, retinal arterial to venous ratio, pulse wave velocity, flow-mediated dilatation of the brachial artery, glyceryl-trinitrate- induced dilatation of the brachial artery | Phase 4 | 80 | 31 December 23 | Switzerland |
| 11 | NCT04778787 | Death due to heart failure; deterioration of renal function (increase in blood creatinine by 0.3 mg/dl within 48 h); development of resistance to diuretics; re-hospitalization about decompensation of chronic heart failure within 30 days after discharge from the hospital | Phase 4 | 370 | 1 August 2022 | Russian Federation |
| 12 | NCT04717986 | Mayor adverse cardiovascular effects; Left ventricular ejection fraction; Chronic heart failure; Post infarction angina; Mortality due to cardiovascular cause | NA | 188 | 1 September 2022 | Mexico |
| 13 | NCT04564742 | Time to the first occurrence of any of the components of this composite: hospitalization for heart failure or cardiovascular death; Time to the first occurrence of any of the components of this composite: myocardial infarction or stroke (incl. ischaemic, hemorrhagic, and undetermined stroke) or cardiovascular death; Time to the first occurrence of a fatal or a non-fatal MI/CV Death/death of any cause/new onset of type 2 diabetes mellitus post-randomization | Phase 3 | 6400 | 22 September 2023 | Sweden, United Kingdom |
| 14 | NCT04509674 | Composite of time to first heart failure hospitalization or all-cause mortality; Total number of HHF or all-cause mortality; Total number of non-elective Cardiovascular (CV) hospitalizations or all-cause mortality; Total number of non-elective all-cause hospitalizations or all-cause mortality; Total number of hospitalizations for MI or all-cause mortality; Time to CV mortality | Phase 3 | 6500 | 31 March 2023 | United States, Argentina, Australia, Brazil, Bulgaria, Canada, China, Denmark, France, Germany, Hungary, India, Israel, Japan, Korea, Netherlands, Poland, Romania, Russian Federation, Serbia, Spain, Ukraine |
| 15 | NCT05364190 | The cumulative mean of daily diuresis, diuretic; change in the level of NT-pro BNP; Presence of symptoms of congestion and dyspnea at discharge; ICU length of stay; incidence of worsening of heart failure case; fractional excretion of sodium-based diuretic efficiency; Serum potassium; Incidence of ketoacidosis; Serum glucose covariate-adjusted for baseline with attention to both elevations; Incidence of symptomatic, sustained hypovolemic hypotension; In-hospital mortality; Hospital readmission within 90 days of discharge for heart failure; Incidence of mortality within 90 days from discharge due cardiovascular cause; The incidence of worsening of renal function; Any reported adverse events during follow up period; The progression of heart failure severity | Phase 3 | 180 | 9 November 2023 | Egypt |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ul Amin, N.; Sabir, F.; Amin, T.; Sarfraz, Z.; Sarfraz, A.; Robles-Velasco, K.; Cherrez-Ojeda, I. SGLT2 Inhibitors in Acute Heart Failure: A Meta-Analysis of Randomized Controlled Trials. Healthcare 2022, 10, 2356. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122356
Ul Amin N, Sabir F, Amin T, Sarfraz Z, Sarfraz A, Robles-Velasco K, Cherrez-Ojeda I. SGLT2 Inhibitors in Acute Heart Failure: A Meta-Analysis of Randomized Controlled Trials. Healthcare. 2022; 10(12):2356. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122356
Chicago/Turabian StyleUl Amin, Noor, Faiza Sabir, Talal Amin, Zouina Sarfraz, Azza Sarfraz, Karla Robles-Velasco, and Ivan Cherrez-Ojeda. 2022. "SGLT2 Inhibitors in Acute Heart Failure: A Meta-Analysis of Randomized Controlled Trials" Healthcare 10, no. 12: 2356. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122356