
The Prevalence of Vitamin and Mineral Deficiencies and High Levels of Non-Essential Heavy Metals in Saudi Arabian Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sampling and Sample Size
2.3. Participants and Recruitment Method
2.3.1. Phase I (Survey)
2.3.2. Phase II (Laboratory Measurements)
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Demographic and Health Characteristics
3.2. Prevalence of Micronutrient Deficiencies
3.2.1. Vitamin Deficiencies
Vitamin Deficiencies by Sex
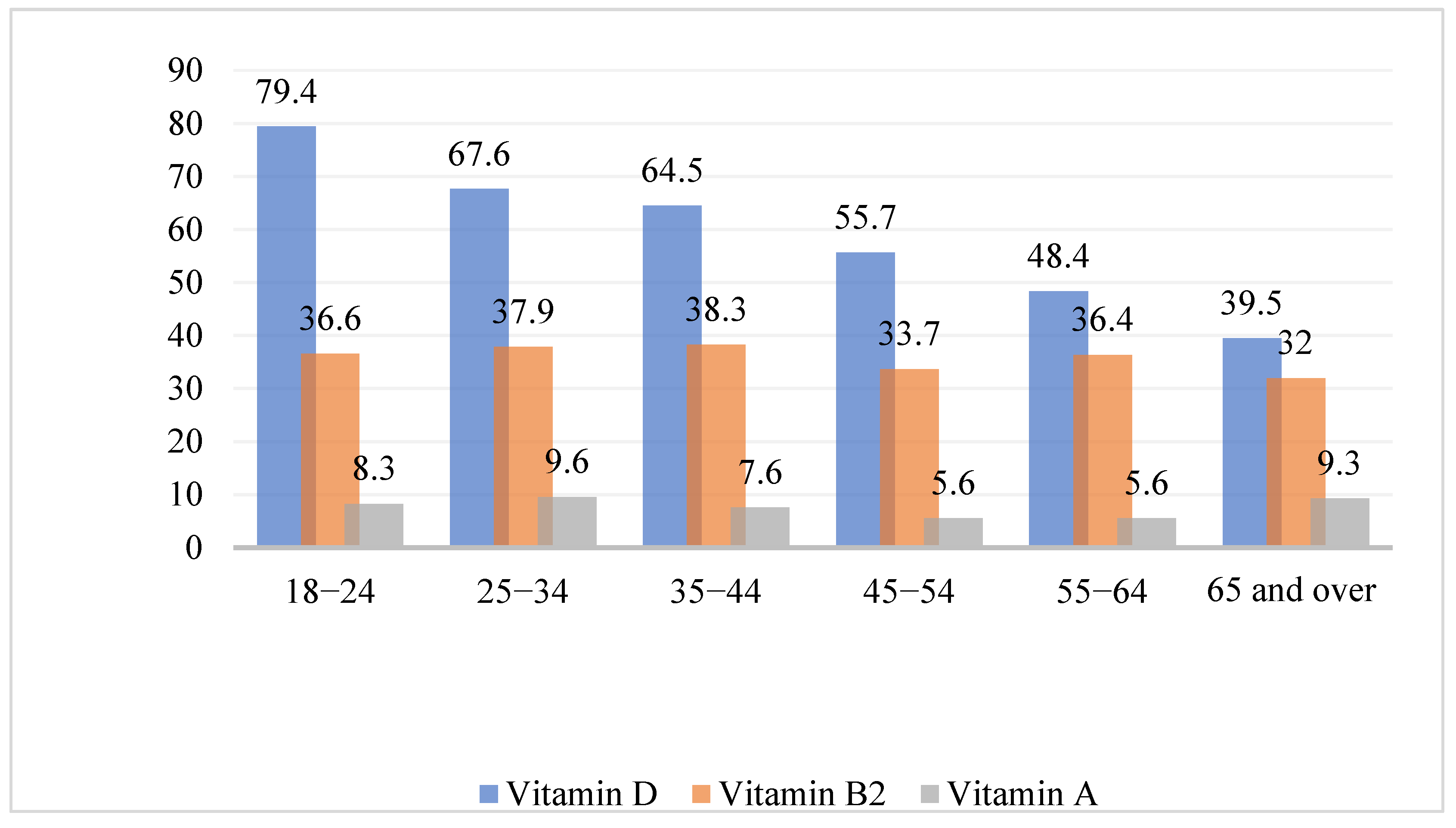
Vitamin Deficiencies by Age Group
3.2.2. Mineral Deficiencies
Mineral Deficiencies by Sex
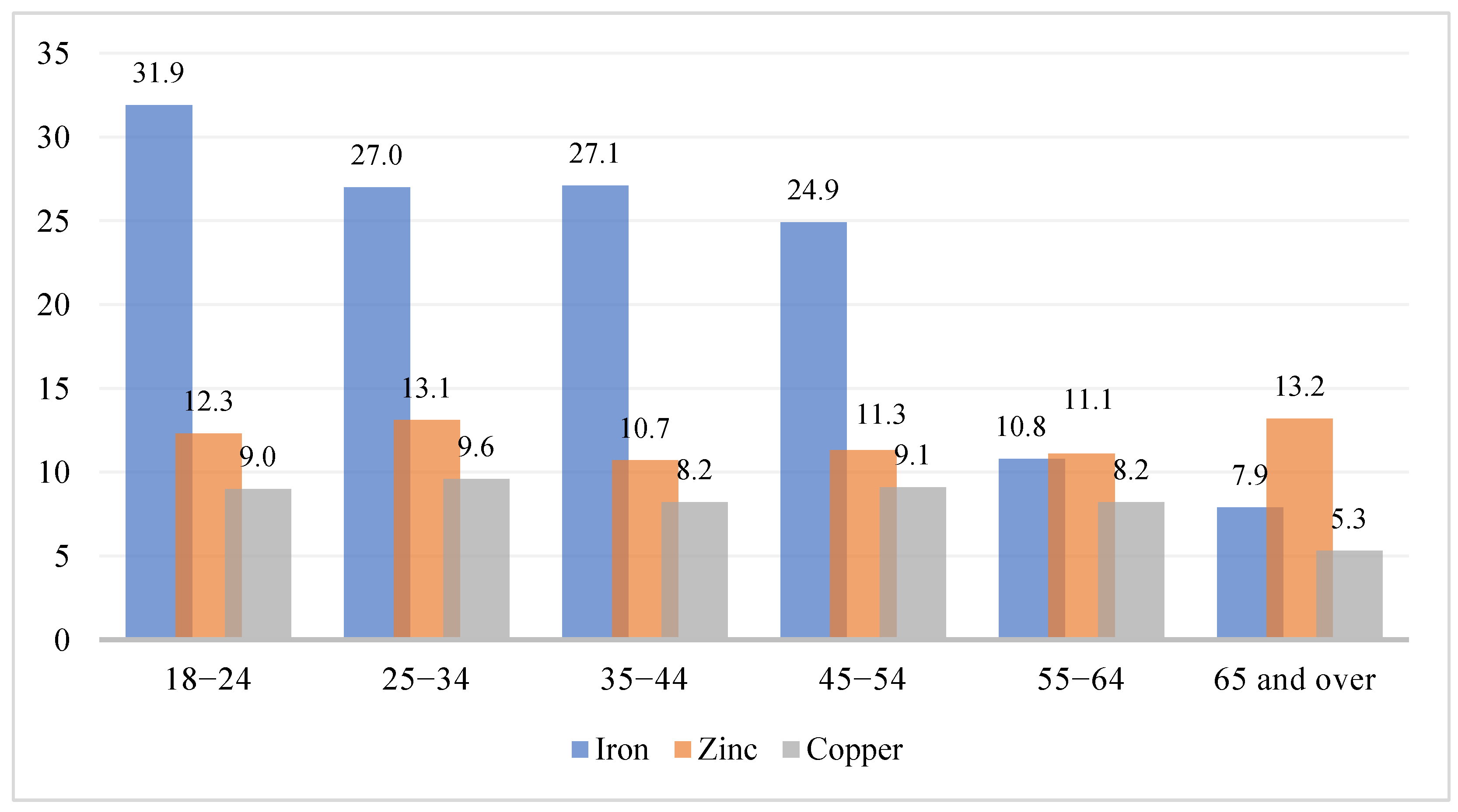
Mineral Deficiencies by Age Group
3.3. Heavy Metals
3.3.1. Heavy Metals by Sex
3.3.2. Heavy Metals by Age Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Type | Micronutrient | Methodology | Instrument | Measured Compound | Ref. Range |
|---|---|---|---|---|---|
| Vitamin | A | High-performance liquid chromatography (HPLC) | Waters HPLC Ultimate 3000 HPLC (Thermo Scientific) UV detector | Vitamin A (Retinol) | 30–70 μg/dL |
| B1 | High-performance liquid chromatography (HPLC) | Waters HPLC Ultimate 3000 HPLC (Thermo Scientific) Fluorescence detector | Vitamin B1 (Thiamine pyrophosphate) | 28–85 μg/L | |
| B2 | High-performance liquid chromatography (HPLC) | Waters HPLC Ultimate 3000 HPLC (Thermo Scientific) Fluorescence detector | Riboflavin | 2.3–14 μg/L | |
| B6 | High-performance liquid chromatography (HPLC) | Waters HPLC Ultimate 3000 HPLC (Thermo Scientific) Fluorescence detector | Vitamin B6 (pyridoxal-5′- phosphate) | 8.7–27.2 μg/L | |
| B9 (Folic acid) | Binding assay | Cobas e6000 | Serum folate | 4.6–18.7 ng/mL | |
| B12 | Two-step immunoassay using chemiluminescent microparticle immuno assay (CMIA) technology with flexible assay protocols, referred to as Chemiflex | Architect 2000 | Vitamin B 12 (Cyanocobalamin) | 187–883 pg/mL | |
| D | Direct competitive chemiluminescence immunoassay (CLIA) | Liaison XL | 25-OH vitamin D (Total) | 20–100 ng/mL | |
| E | High-performance liquid chromatography (HPLC) | Waters HPLC Ultimate 3000 HPLC (Thermo Scientific) UV detector | α-Tocopherol | 5.7–19.9 mg/L | |
| Mineral | Copper | Atomic absorption spectrometry | Thermo Scientific E3000 series | Copper (Cu) | 70–175 μg/dL |
| Zinc | Atomic absorption spectrometry | Thermo Scientific E3000 series | Zinc (Zn) | 60–130 μg/dL | |
| Magnesium | Colorimetric method with chlorophosphonazo III | Cobas c501 | Magnesium | 1.6–2.6 mg/dL | |
| Ferritin | Colorimetric assay | Cobas c501 | Iron | Women: 13–150 ng/mL Men: 30–400 ng/mL | |
| Heavy metal | Arsenic | Inductively coupled plasma/mass spectrometry (ICP/MS) | Outsourced to Quest Diagnostics | Arsenic | <12 μg/L |
| Mercury | Inductively coupled plasma/mass spectrometry (ICP/MS) | Outsourced to Quest Diagnostics | Mercury | ≤8 μg/L |
| Age Group | Vitamin A | Vitamin B1 | Vitamin B2 | Vitamin B6 | Vitamin B9 | Vitamin B12 | Vitamin D | Vitamin E |
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| 18–24 | 29 (8.3) | 6 (1.7) | 229 (36.6) | 2 (0.6) | 10 (2.8) | 36 (10.7) | 281 (79.4) | 5 (1.4) |
| 25–34 | 108 (9.6) | 34 (3.0) | 426 (37.9) | 16 (1.4) | 45 (4.0) | 72 (7.0) | 760 (67.6) | 35 (3.1) |
| 35–44 | 78 (7.6) | 48 (4.6) | 396 (38.3) | 26 (2.5) | 41 (4.0) | 90 (8.7) | 664 (64.5) | 39 (3.6) |
| 45–54 | 33 (5.6) | 15 (2.5) | 199 (33.7) | 8 (1.4) | 18 (3.1) | 35 (5.9) | 327 (55.7) | 19 (3.2) |
| 55–64 | 14 (5.6) | 7 (2.8) | 90 (36.4) | 4 (1.6) | 7 (2.8) | 17 (6.8) | 120 (48.4) | 6 (2.4) |
| ≥65 | 7 (9.3) | 1 (1.3) | 24 (32.0) | 1 (1.3) | 3 (4.0) | 2 (2.6) | 30 (39.5) | 3 (3.9) |
| p-value | 0.51 | 0.048 | 0.453 | 0.158 | 0.771 | 0.53 | 0.001 | 0.362 |
| Age Group | Copper | Iron | Magnesium | Zinc | Arsenic | Mercury |
|---|---|---|---|---|---|---|
| Deficient | Deficient | Deficient | Deficient | Normal | Normal | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| 18–24 | 31 (9.0) | 113 (31.9) | 1 (0.3) | 43 (12.3) | 354 (100) | 352 (99.4) |
| 25–34 | 107 (9.6) | 304 (27.0) | 6 (0.5) | 147 (13.1) | 1124 (99.8) | 1121 (99.7) |
| 35–44 | 83 (8.2) | 279 (27.1) | 7 (0.7) | 110 (10.7) | 1126 (99.7) | 1028 (99.5) |
| 45–54 | 52 (9.1) | 146 (24.9) | 1 (0.2) | 66 (11.3) | 591 (100) | 591 (100) |
| 55–64 | 20 (8.2) | 27 (10.8) | 6 (2.4) | 27 (11.1) | 248 (99.6) | 249 (100) |
| ≥65 | 4 (5.3) | 6 (7.9) | 1 (1.3) | 10 (13.2) | 76 (100) | 76 (100) |
| p-value | 0.731 | 0.001 | 0.008 | 0.642 | 0.653 | 0.426 |
References
- Whitney, E.; Rolfes, S.R. Understanding Nutrition, 2nd ed.; Cengage Learning: Melbourne, VIC, Australia, 2018. [Google Scholar]
- Shenkin, A. The key role of micronutrients. Clin. Nutr. 2006, 25, 1–13. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Malnutrition. 2021. Available online: https://www.who.int/health-topics/malnutrition#tab=tab_1 (accessed on 15 September 2022).
- Bailey, R.L.; West, K.P.; Black, R.E. The epidemiology of global micronutrient deficiencies. Ann. Nutr. Metab. 2015, 66, 22–33. [Google Scholar] [CrossRef]
- Godswill, C.; Somtochukwu, V. Nutritional Diseases and Nutrient Toxicities: A Systematic Review of the Diets and Nutrition for Prevention and Treatment. Int. J. Adv. Acad. Res. Sci. 2020, 6, 1–46. [Google Scholar]
- Muthayya, S.; Rah, J.H.; Sugimoto, J.D.; Roos, F.F.; Kraemer, K.; Black, R.E. The Global Hidden Hunger Indices and Maps: An Advocacy Tool for Action. PLoS ONE 2013, 8, e67860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peraza, M.A.; Ayala-Fierro, F.; Barber, D.S.; Casarez, E.; Rael, L.T. Effects of Micronutrients on Metal Toxicity. Environ. Health Perspect. 1998, 106 (Suppl. S1), 203–216. [Google Scholar]
- Balali-Mood, M.; Naseri, K.; Tahergorabi, Z.; Khazdair, M.R.; Sadeghi, M. Toxic Mechanisms of Five Heavy Metals: Mercury, Lead, Chromium, Cadmium, and Arsenic. Front. Pharmacol. 2021, 12, 643972. [Google Scholar] [CrossRef]
- Shaji, E.; Santosh, M.; Sarath, K.V.; Prakash, P.; Deepchand, V.; Divya, B.V. Arsenic contamination of groundwater: A global synopsis with focus on the Indian Peninsula. Geosci. Front. 2021, 12, 101079. [Google Scholar] [CrossRef]
- World Health Organization. Arsenic. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/arsenic (accessed on 15 September 2022).
- Almutairi, M.; Alsaleem, T.; Jeperel, H.; Alsamti, M.; Alowaifeer, A.M. Determination of inorganic arsenic, heavy metals, pesticides and mycotoxins in Indian rice (Oryza sativa) and a probabilistic dietary risk assessment for the population of Saudi Arabia. Regul. Toxicol. Pharmacol. 2021, 125, 104986. [Google Scholar] [CrossRef]
- World Health Organization. Mercury and Health. 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/mercury-and-health (accessed on 16 September 2022).
- Tchounwou, P.B.; Yedjou, C.G.; Patlolla, A.K.; Sutton, D.J. Heavy Metals Toxicity and the Environment. Mol. Clin. Environ. Toxicol. 2012, 101, 133–164. [Google Scholar] [CrossRef] [Green Version]
- Hakami, O. Risk Assessment of Heavy Metals in Fish in Saudi Arabia. Am. J. Environ. Sci. 2016, 2, 341–357. [Google Scholar] [CrossRef] [Green Version]
- Hwalla, N.; Al Dhaheri, A.S.; Radwan, H.; Alfawaz, H.A.; Fouda, M.A.; Al-Daghri, N.M. The prevalence of micronutrient deficiencies and inadequacies in the middle east and approaches to interventions. Nutrients 2017, 9, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuffaha, M.; El Bcheraoui, C.; Daoud, F.; Al Hussaini, H.A.; Alamri, F.; Al Saeedi, M. Deficiencies under plenty of sun: Vitamin D status among adults in the Kingdom of Saudi Arabia, 2013. N. Am. J. Med. Sci. 2015, 7, 467–475. [Google Scholar] [CrossRef]
- General Authority for Statistics. Statistical Yearbook of 2017; General Authority for Statistics: Riyadh, Saudi Arabia, 2017. [Google Scholar]
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 17 September 2022).
- Algabbani, A.; Alqahtani, A.; BinDhim, N. Prevalence and determinants of non-communicable diseases in Saudi Arabia. Food Drug Regul. Sci. J. 2019, 2, 1. [Google Scholar] [CrossRef]
- WHO Regional Office for the Eastern Mediterranean. Regional Strategy on Nutrition 2010–2019. 2009. Available online: https://apps.who.int/iris/handle/10665/116694 (accessed on 18 September 2022).
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Al-Alyani, H.; Al-Turki, H.A.; Al-Essa, O.N.; Alani, F.M.; Sadat-Ali, M. Vitamin D deficiency in Saudi Arabians: A reality or simply hype: A meta-analysis (2008–2015). J. Fam. Community Med. 2018, 25, 1–4. [Google Scholar] [CrossRef]
- Zainel, A.J.A.L.; Qotba, H.; Al Nuaimi, A.; Syed, M. Vitamin D status among adults (18–65 years old) attending primary healthcare centres in Qatar: A cross-sectional analysis of the Electronic Medical Records for the year 2017. BMJ Open 2019, 9, e029334. [Google Scholar] [CrossRef] [Green Version]
- Abiaka, C.; Delghandi, M.; Kaur, M.; Al-Saleh, M. Vitamin D Status and Anthropometric Indices of an Omani Study Population. Sultan Qaboos Univ. Med. J. 2013, 13, 224–231. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.F.; Al Hooti, S.; Al Zenki, S.; Alomirah, H.; Jamil, K.M.; Rao, A. Vitamin D deficiency is associated with high prevalence of diabetes in Kuwaiti adults: Results from a national survey Chronic Disease epidemiology. BMC Public Health 2016, 16, 100. [Google Scholar] [CrossRef] [Green Version]
- Forrest, K.Y.Z.; Wendy, S.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlQuaiz, A.J.M.; Kazi, A.; Fouda, M.; Alyousefi, N. Age and gender differences in the prevalence and correlates of vitamin D deficiency. Arch. Osteoporos. 2018, 13, 49. [Google Scholar] [CrossRef]
- Nair, R.; Maseeh, A. Vitamin D: The sunshine vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar] [CrossRef]
- Alshahrani, F.M.; Almalki, M.H.; Aljohani, N.; Alzahrani, A.; Alsaleh, Y.; Holick, M.F. Vitamin D: Light side and best time of sunshine in Riyadh, Saudi Arabia. Dermatoendocrinology 2013, 5, 177–180. [Google Scholar] [CrossRef] [Green Version]
- Zareef, T.A.; Jackson, R.T. Knowledge and attitudes about vitamin D and sunlight exposure in premenopausal women living in Jeddah, and their relationship with serum vitamin D levels. J. Health Popul. Nutr. 2021, 40, 38. [Google Scholar] [CrossRef] [PubMed]
- The National Institutes of Health. Riboflavin: Fact Sheet for Health Professionals. 2021. Available online: https://ods.od.nih.gov/factsheets/Riboflavin-HealthProfessional/ (accessed on 4 October 2022).
- Whitfield, K.; McCann, A.; Karakochuk, C.; Talukder, A.; Ward, M.; McNulty, H.; Green, T. High rates of riboflavin deficiency in women of childbearing age in Cambodia and Canada (1041.12). FASEB J. 2014, 4 (Suppl. S1), 2469–2475. [Google Scholar] [CrossRef]
- Choi, J.Y.; Kim, Y.N.; Cho, Y.O. Evaluation of riboflavin intakes and status of 20–64-year-old adults in South Korea. Nutrients 2015, 7, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Beverley, B.; Alison, L.; Ann, P.; Chris, B.; Polly, P.; Sonja, N. National Diet and Nutrition Survey: Results from Years 1, 2, 3 and 4 (Combined) of the Rolling Programme (2008/2009–2011/2012); Public Health England and Food Standards Agency: London, UK, 2014. [Google Scholar]
- Leblanc, J.G.; Laiñ, J.E.; Juarez Del Valle, M.; Vannini, V.; Van Sinderen, D.; Taranto, M.P. B-Group vitamin production by lactic acid bacteria-current knowledge and potential applications. J. Appl. Microbiol. 2011, 111, 1297–1309. [Google Scholar] [CrossRef] [PubMed]
- Thakur, K.; Tomar, S.; Singh, A.K.; Mandal, S.; Arora, S. Riboflavin and health: A review of recent human research. Crit. Rev. Food Sci. Nutr. 2017, 57, 3650–3660. [Google Scholar] [CrossRef]
- Owaidah, T.; Al-Numair, N.; Al-Suliman, A.; Zolaly, M.; Hasanato, R.; Al Zahrani, F. Iron Deficiency and Iron Deficiency Anemia Are Common Epidemiological Conditions in Saudi Arabia: Report of the National Epidemiological Survey. Anemia 2020, 2020, 6642568. [Google Scholar] [CrossRef]
- Chueh, H.W.; Jung, H.L.; Shim, Y.J.; Choi, H.S.; Han, J.Y. High anemia prevalence in Korean older adults, an advent healthcare problem: 2007–2016 KNHANES. BMC Geriatr. 2020, 20, 509. [Google Scholar] [CrossRef]
- Patel, K.V. Epidemiology of Anemia in Older Adults. Semin. Hematol. 2008, 45, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirmiran, P.; Golzarand, M.; Serra-Majem, L.; Azizi, F. Iron, iodine and vitamin a in the Middle East: A systematic review of deficiency and food fortification. Iran J. Public Health 2012, 41, 8–19. [Google Scholar] [PubMed]
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on iron and its importance for human health. J. Res. Med. Sci. 2014, 19, 164. [Google Scholar] [PubMed]
- Wessells, K.R.; Brown, K.H. Estimating the Global Prevalence of Zinc Deficiency: Results Based on Zinc Availability in National Food Supplies and the Prevalence of Stunting. PLoS ONE 2012, 7, e50568. [Google Scholar] [CrossRef] [Green Version]
- Abiaka, C.; Olusi, S.; Al-Awadhi, A. Reference Ranges of Copper and Zinc and the Prevalence of Their Deficiencies in an Arab Population Aged 15–80 Years. Biol. Trace Elem. Res. 2003, 91, 33–43. [Google Scholar] [CrossRef]
- Ghasemi, A.; Zahediasl, S.; Hosseini-Esfahani, F.; Azizi, F. Reference Values for Serum Zinc Concentration and Prevalence of Zinc Deficiency in Adult Iranian Subjects. Biol. Trace Elem. Res. 2012, 149, 307–314. [Google Scholar] [CrossRef]
- Prasad, A.S. Reviews from ASN EB 2012 Symposia Discovery of Human Zinc Deficiency: Its Impact on Human Health and Disease 1–3. J. Trace Elem. Med. Biol. 2014, 28, 357–363. [Google Scholar] [CrossRef]
- National Institutes of Health (NIH). Zinc: Fact Sheet for Health Professionals. 2021. Available online: https://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/ (accessed on 5 October 2022).
- Saudi Food And Drug Authority. Overview. 2022. Available online: https://www.sfda.gov.sa/en/overview (accessed on 5 October 2022).
- Saudi Food and Drug Authority. SFDA Warns about Cosmetics Containing High Percentage of Lead. 2011. Available online: https://www.sfda.gov.sa/en/news/48727 (accessed on 6 October 2022).
- Yahia, E.M.; García-Solís, P.; MaldonadoCelis, M.E. Contribution of fruits and vegetables to human nutrition and health. In Postharvest Physiology and Biochemistry of Fruits and Vegetables; Woodhead Publishing: Sawston, UK, 2019; pp. 19–45. [Google Scholar] [CrossRef]
- Steenhuis, I.H.; Waterlander, W.E.; De Mul, A. Consumer food choices: The role of price and pricing strategies. Public Health Nutr. 2011, 14, 2220–2226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyles, H.; Mhurchu, C.N.; Nghiem, N.; Blakely, T. Food Pricing Strategies, Population Diets, and Non-Communicable Disease: A Systematic Review of Simulation Studies. PLoS Med. 2012, 9, e1001353. [Google Scholar] [CrossRef] [Green Version]
- Just, D.R.; Byrne, A.T. Evidence-based policy and food consumer behaviour: How empirical challenges shape the evidence. Eur. Rev. Agric. Econ. 2020, 47, 348–370. [Google Scholar] [CrossRef]
- Choi, S.E.; Seligman, H.; Basu, S. Cost Effectiveness of Subsidizing Fruit and Vegetable Purchases Through the Supplemental Nutrition Assistance Program. Am. J. Prev. Med. 2017, 52, e147–e155. [Google Scholar] [CrossRef] [PubMed]
- Moradi-Lakeh, M.; El Bcheraoui, C.; Afshin, A.; Daoud, F.; AlMazroa, M.A.; Al Saeedi, M. Diet in Saudi Arabia: Findings from a nationally representative survey. Public Health Nutr. 2022, 20, 1075–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokdad, A.; El Bcheraoui, C.; Basulaiman, M.; AlMazroa, M.; Tuffaha, M.; Daoud, F. Fruit and vegetable consumption among adults in Saudi Arabia, 2013. Nutr. Diet. Suppl. 2015, 7, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L. Current Vitamin D status in European and Middle East countries and strategies to prevent Vitamin D deficiency: A position statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, P23–P54. [Google Scholar] [CrossRef] [Green Version]
- Mannar, M.G.V.; Hurrell, R.F. Food fortification: Past experience, current status, and potential for globalization. In Food Fortification in a Globalized World; Academic Press: Cambridge, MA, USA, 2018; pp. 3–11. [Google Scholar] [CrossRef]
- Sadat-Ali, M.; Al Elq, A.; Al-Farhan, M.; Sadat, N. Fortification with vitamin D: Comparative study in the Saudi Arabian and US markets. J. Fam. Community Med. 2013, 20, 49–52. [Google Scholar] [CrossRef]


| Characteristic | Men | Women | Total | Total (Weighted%) |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Sample size | 1674 (48.8) | 1758 (51.2) | 3432 (100) | 100 |
| Age group | ||||
| 18–24 | 130 (7.8) | 224 (12.7) | 354 (10.3) | 13.9 |
| 25–34 | 579 (34.6) | 547 (31.1) | 1126 (21.8) | 30.1 |
| 35-44 | 555 (33.2) | 481 (27.4) | 1036 (30.2) | 29.0 |
| 45–54 | 259 (15.5) | 332 (18.9) | 591 (17.2) | 17.0 |
| 55–64 | 118 (7.0) | 131 (7.5) | 249 (7.3) | 7.9 |
| ≥65 | 33 (2.0) | 43 (2.4) | 76 (2.2) | 2.1 |
| Smoking and tobacco use status | ||||
| Never smoked | 897 (56.8) | 1646 (95.4) | 2543 (76.9) | 75.3 |
| Previous smoker | 151 (9.6) | 11 (0.6) | 162 (4.9) | 4.4 |
| Current smoker | 532 (318) | 68 (3.9) | 600 (18.2) | 20.3 |
| Dietary supplements | ||||
| Had taken supplements within the past 7 days | 341 (20.4) | 495 (28.7) | 836 (25.3) | 25.2 |
| History of chronic condition diagnoses | ||||
| Diabetes | 155 (9.3) | 143 (8.1) | 298 (9.0) | 8.5 |
| Heart disease | 24 (1.4) | 15 (0.9) | 39 (1.1) | 1.2 |
| Respiratory disease | 48 (2.9) | 60 (3.4) | 108 (3.1) | 3.6 |
| Depression | 20 (1.4) | 32 (18) | 52 (1.6) | 2.9 |
| History of morbidity | ||||
| Morbidity (≥1 chronic condition) | 327 (20.7) | 341 (19.8) | 668 (20.2) | 22.1 |
| Multimorbidity (≥2 chronic conditions) | 127 (7.6) | 197 (11.2) | 324 (9.8) | 11.7 |
| Vitamin Deficiency Variables | Men | Women | p-Value | Total | Total (Weighted%) |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Sample size | 1674 (48.8) | 1758 (51.2) | 3432 (100) | 100 | |
| A | 81 (4.8) | 188 (10.7) | <0.001 | 269 (7.9) | 9.6 |
| B1 | 54 (3.2) | 57 (3.2) | 0.974 | 111 (3.2) | 2.3 |
| B2 | 662 (39.5) | 602 (34.2) | <0.001 | 1264 (36.9) | 44.8 |
| B6 | 20 (1.2) | 37 (2.1) | 0.57 | 57 (1.7) | 2.4 |
| B9 | 87 (5.2) | 37 (2.1) | <0.001 | 124 (3.6) | 3.5 |
| B12 | 99 (5.9) | 160 (9.1) | <0.001 | 259 (7.5) | 8.1 |
| D | 1141 (68.2) | 1041 (59.2) | <0.001 | 2182 (63.8) | 64.3 |
| E | 50 (3.0) | 57(3.3) | 0.666 | 107 (3.1) | 4.9 |
| Mineral Deficiency Variables | Men | Women | p-Value | Total | Total (Weighted%) |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Sample size | 1674 (48.8) | 1758 (51.2) | 3432 (100) | 100 | |
| Copper | 211 (12.6) | 86 (4.9) | <0.001 | 297 (8.8) | 8.7 |
| Iron | 188 (11.3) | 687 (39.2) | <0.001 | 875 (25.6) | 23.2 |
| Magnesium | 10 (0.6) | 12 (0.7) | 0.753 | 22 (0.6) | 0.4 |
| Zinc | 149 (8.9) | 254 (14.4) | <0.001 | 403 (11.9) | 15.3 |
| Heavy Metals | Classification | Men | Women | p-Value | Total | Total (Weighted%) |
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||||
| Arsenic | Normal | 1670 (99.8) | 1756 (99.8) | 0.380 | 3426 (99.8) | 99.7 |
| High | 4 (0.3) | 2 (0.1) | 6 (0.2) | 0.3 | ||
| Mercury | Normal | 1664 (99.6) | 1752 (97.8) | 0.476 | 3416 (99.7) | 99.9 |
| High | 6.0 (0.4) | 4 (0.2) | 10 (0.3) | 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albalawi, O.; Almubark, R.; Almarshad, A.; Alqahtani, A.S. The Prevalence of Vitamin and Mineral Deficiencies and High Levels of Non-Essential Heavy Metals in Saudi Arabian Adults. Healthcare 2022, 10, 2415. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122415
Albalawi O, Almubark R, Almarshad A, Alqahtani AS. The Prevalence of Vitamin and Mineral Deficiencies and High Levels of Non-Essential Heavy Metals in Saudi Arabian Adults. Healthcare. 2022; 10(12):2415. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122415
Chicago/Turabian StyleAlbalawi, Omar, Rasha Almubark, Abdulrahman Almarshad, and Amani S. Alqahtani. 2022. "The Prevalence of Vitamin and Mineral Deficiencies and High Levels of Non-Essential Heavy Metals in Saudi Arabian Adults" Healthcare 10, no. 12: 2415. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122415