
Association between Nutrition Literacy and Bangladeshi Adults’ Healthy Eating Behaviors: Evidence from the Nutrition Literacy Study 2021
 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
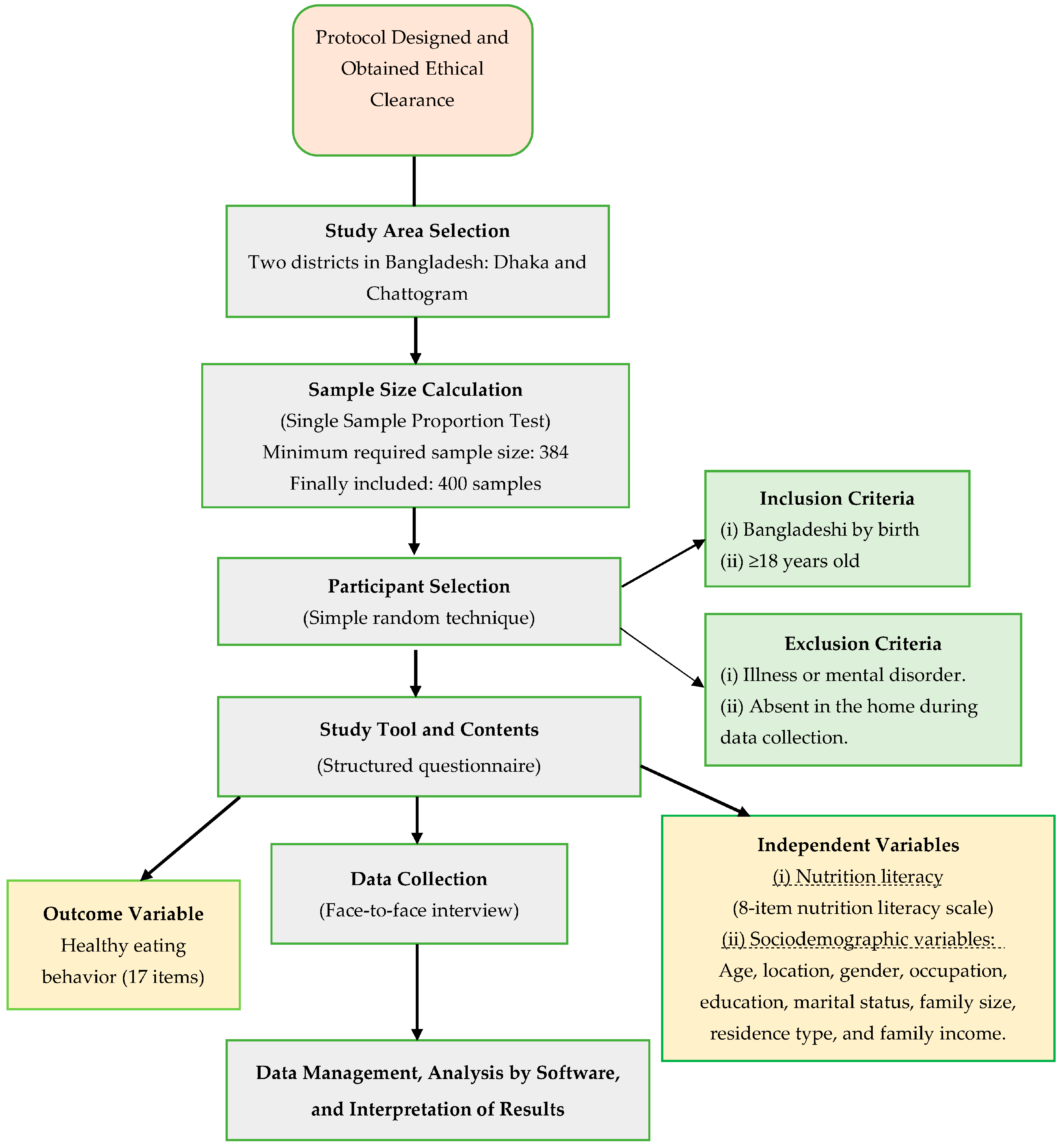
2.1. Research Design and Sample
2.2. Study Variables
2.3. Ethical Statement
2.4. Data Collection Procedure
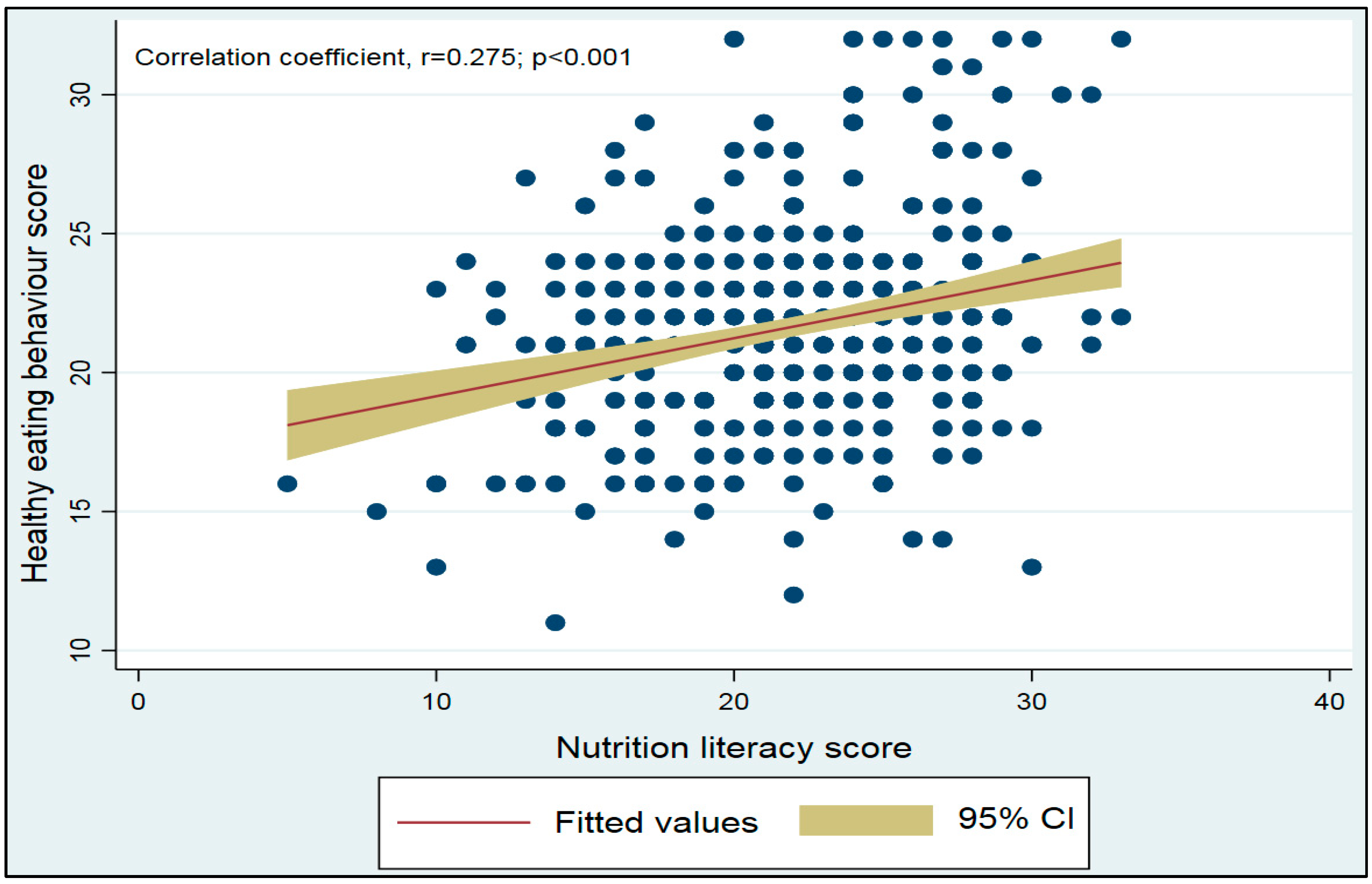
2.5. Statistical Analyses
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahman, M.M.; Farhana, Z.; Chowdhury, T.T.; Uddin, M.T.; Islam, M.Z.; Hamiduzzaman, M. High Nutritional Vulnerability and Associated Risk Factors of Bangladeshi Wetland Community People Aged 50 Years and Older. J. Ageing Longev. 2022, 2, 102–112. [Google Scholar] [CrossRef]
- Taylor, M.K.; Sullivan, D.K.; Ellerbeck, E.F.; Gajewski, B.J.; Gibbs, H.D. Nutrition Literacy Predicts Adherence to Healthy/Unhealthy Diet Patterns in Adults with a Nutrition-Related Chronic Condition. Public Health Nutr. 2019, 22, 2157–2169. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.-L.; Lai, I.-J.; Chang, L.-C. Nutrition Literacy Is Associated with Healthy-Eating Behaviour among College Students in Taiwan. Health Educ. J. 2019, 78, 756–769. [Google Scholar] [CrossRef]
- Silk, K.J.; Sherry, J.; Winn, B.; Keesecker, N.; Horodynski, M.A.; Sayir, A. Increasing Nutrition Literacy: Testing the Effectiveness of Print, Web Site, and Game Modalities. J. Nutr. Educ. Behav. 2008, 40, 3–10. [Google Scholar] [CrossRef]
- Rothman, R.L.; Housam, R.; Weiss, H.; Davis, D.; Gregory, R.; Gebretsadik, T.; Shintani, A.; Elasy, T.A. Patient Understanding of Food Labels: The Role of Literacy and Numeracy. Am. J. Prev. Med. 2006, 31, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Cha, E.; Kim, K.H.; Lerner, H.M.; Dawkins, C.R.; Bello, M.K.; Umpierrez, G.; Dunbar, S.B. Health Literacy, Self-Efficacy, Food Label Use, and Diet in Young Adults. Am. J. Health Behav. 2014, 38, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huizinga, M.M.; Carlisle, A.J.; Cavanaugh, K.L.; Davis, D.L.; Gregory, R.P.; Schlundt, D.G.; Rothman, R.L. Literacy, Numeracy, and Portion-Size Estimation Skills. Am. J. Prev. Med. 2009, 36, 324–328. [Google Scholar] [CrossRef] [Green Version]
- Miller, L.M.S.; Cassady, D.L. The Effects of Nutrition Knowledge on Food Label Use. A Review of the Literature. Appetite 2015, 92, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Chari, R.; Warsh, J.; Ketterer, T.; Hossain, J.; Sharif, I. Association between Health Literacy and Child and Adolescent Obesity. Patient Educ. Couns. 2014, 94, 61–66. [Google Scholar] [CrossRef]
- Biswas, T.; Garnett, S.P.; Pervin, S.; Rawal, L.B. The Prevalence of Underweight, Overweight and Obesity in Bangladeshi Adults: Data from a National Survey. PLoS ONE 2017, 12, e0177395. [Google Scholar] [CrossRef]
- Das, S.; Fahim, S.M.; Islam, M.S.; Biswas, T.; Mahfuz, M.; Ahmed, T. Prevalence and Sociodemographic Determinants of Household-Level Double Burden of Malnutrition in Bangladesh. Public Health Nutr. 2019, 22, 1425–1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferdous, T.; Kabir, Z.N.; Wahlin, Å.; Streatfield, K.; Cederholm, T. The Multidimensional Background of Malnutrition among Rural Older Individuals in Bangladesh–a Challenge for the Millennium Development Goal. Public Health Nutr. 2009, 12, 2270–2278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pingki, F.H.; Hossain, M.B.; Amin, S.M.N.; Sultana, M.; Islam, M.M.; Rahman, A.F.M.A.; Nur, A.U.; Arshad, A. Prevalence of Malnutrition and Associated Factors of Pond Fish Farmers from Noakhali Coast, Bangladesh. J. Environ. Biol. 2020, 41, 1171–1178. [Google Scholar] [CrossRef]
- Rahman, M.A.; Halder, H.R.; Rahman, M.S.; Parvez, M. Poverty and Childhood Malnutrition: Evidence-Based on a Nationally Representative Survey of Bangladesh. PLoS ONE 2021, 16, e0256235. [Google Scholar]
- Shahid, M.; Cao, Y.; Ahmed, F.; Raza, S.; Guo, J.; Malik, N.I.; Rauf, U.; Qureshi, M.G.; Saheed, R.; Maryam, R. Does Mothers’ Awareness of Health and Nutrition Matter? A Case Study of Child Malnutrition in Marginalized Rural Community of Punjab, Pakistan. Front. Public Health 2022, 10, 792164. [Google Scholar] [CrossRef] [PubMed]
- Gulati, A.; Roy, R. Linkage Between Agriculture, Poverty and Malnutrition in India. In Revitalizing Indian Agriculture and Boosting Farmer Incomes; Springer: Singapore, 2021; pp. 39–74. [Google Scholar]
- Sharon Friel, L.H.; Hattersley, L.; Ford, L.; O’Rourke, K. Evidence Review: Addressing the Social Determinants of Inequities in Healthy Eating; Victorian Health Promotion Foundation: Carlton, VIC, Australia, 2015. [Google Scholar]
- Kalkan, I. The Impact of Nutrition Literacy on the Food Habits among Young Adults in Turkey. Nutr. Res. Pract. 2019, 13, 352–357. [Google Scholar] [CrossRef]
- Al Banna, M.H.; Hamiduzzaman, M.; Kundu, S.; Ara, T.; Abid, M.T.; Brazendale, K.; Seidu, A.-A.; Disu, T.R.; Mozumder, N.H.M.R.; Frimpong, J.B. The Association Between Bangladeshi Adults’ Demographics, Personal Beliefs, and Nutrition Literacy: Evidence From a Cross-Sectional Survey. Front. Nutr. 2022, 9, 867926. [Google Scholar] [CrossRef]
- Ministry of Health and Family Welfare. Second National Plan of Action for Nutrition 2016–2025; Ministry of Health and Family Welfare: Dhaka, Bangladesh, 2017.
- Ministry of Health and Family Welfare. Advocacy Plan for Nutrition, Bangladesh 2019–2025; Ministry of Health and Family Welfare: Dhaka, Bangladesh, 2019.
- Nahar, Q.; Choudhury, S.; Faruque, M.M.; Saliheen Sultana, S.S.; Siddiquee, M.A. Dietary Guidelines for Bangladesh; Bangladesh Institute of Research and Rehabilitation in Diabetes, Endocrine and Metabolic Disorders (BIRDEM): Dhaka, Bangladesh, 2013. [Google Scholar]
- Aihara, Y.; Minai, J. Barriers and Catalysts of Nutrition Literacy among Elderly Japanese People. Health Promot. Int. 2011, 26, 421–431. [Google Scholar] [CrossRef] [Green Version]
- Chung, L.M.Y. Food Literacy of Adolescents as a Predictor of Their Healthy Eating and Dietary Quality. J. Child. Adolesc. Behav. 2017, 5, e117. [Google Scholar]
- Lai, I.-J.; Chang, L.-C.; Lee, C.-K.; Liao, L.-L. Nutrition Literacy Mediates the Relationships between Multi-Level Factors and College Students’ Healthy Eating Behavior: Evidence from a Cross-Sectional Study. Nutrients 2021, 13, 3451. [Google Scholar] [CrossRef]
- Natour, N.; Al-Tell, M.; Ikhdour, O. Nutrition Literacy Is Associated with Income and Place of Residence but Not with Diet Behavior and Food Security in the Palestinian Society. BMC Nutr. 2021, 7, 78. [Google Scholar] [CrossRef] [PubMed]
- Banna, M.H.; Brazendale, K.; Hasan, M.; Khan, M.S.I.; Sayeed, A.; Kundu, S. Factors Associated with Overweight and Obesity among Bangladeshi University Students: A Case-Control Study. J. Am. Coll. Health 2020, 70, 2327–2333. [Google Scholar] [CrossRef] [PubMed]
- Al Muktadir, M.H.; Islam, M.A.; Amin, M.N.; Ghosh, S.; Siddiqui, S.A.; Debnath, D.; Islam, M.M.; Ahmed, T.; Sultana, F. Nutrition Transition–Pattern IV: Leads Bangladeshi Youth to the Increasing Prevalence of Overweight and Obesity. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1943–1947. [Google Scholar] [CrossRef]
- Axelson, M.L.; Federline, T.L.; Brinberg, D. A Meta-Analysis of Food-and Nutrition-Related Research. J. Nutr. Educ. 1985, 17, 51–54. [Google Scholar] [CrossRef]
- Spronk, I.; Kullen, C.; Burdon, C.; O’Connor, H. Relationship between Nutrition Knowledge and Dietary Intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef] [PubMed]
- Marías, Y.F.; Glasauer, P. Guidelines for Assessing Nutrition-Related Knowledge, Attitudes and Practices; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2014; ISBN 9251080976. [Google Scholar]
- Contento, I.; Balch, G.I.; Bronner, Y.L.; Lytle, L.A.; Maloney, S.K.; Olson, C.M.; Swadener, S.S. Theoretical Frameworks or Models for Nutrition Education. J. Nutr. Educ. 1995, 27, 287–290. [Google Scholar]
- Smith, S.; Bhattacharyya, K. Men’s Perceptions of Their Roles and Involvement in Household Decisions around Food in Rural Bangladesh. Feed the Future Project. 2016. Available online: https://www.g-fras.org/en/nwg-case-studies/item/890-men-s-perceptions-of-their-roles-and-involvement-in-household-decisions-around-food-in-rural-bangladesh.html (accessed on 4 December 2022).



{kind=link}
{kind=link}
| Variables | Number | Percentage |
|---|---|---|
| Location | ||
| Dhaka | 200 | 50.0 |
| Chattogram | 200 | 50.0 |
| Gender | ||
| Male | 246 | 61.5 |
| Female | 154 | 38.5 |
| Age age (in years) | ||
| 18–29 | 233 | 58.3 |
| 30–39 | 105 | 26.3 |
| 40–49 | 41 | 10.3 |
| 50 or above | 21 | 5.3 |
| Occupation | ||
| Student | 132 | 33.0 |
| Business | 61 | 15.3 |
| Unemployed | 37 | 9.3 |
| Private job | 82 | 20.5 |
| Housewife | 36 | 9.0 |
| Others # | 52 | 13.0 |
| Education level | ||
| Primary education | 41 | 10.3 |
| Secondary and higher secondary | 105 | 26.3 |
| Under graduation | 89 | 22.3 |
| Graduation | 78 | 19.5 |
| Masters or above | 87 | 21.8 |
| Marital status | ||
| Single | 227 | 56.8 |
| Married | 164 | 41.0 |
| Divorced, separated or widowed | 9 | 2.3 |
| Family size | ||
| ≤5 members | 291 | 72.8 |
| >5 members | 109 | 27.3 |
| Permanent residence | ||
| City area | 299 | 74.8 |
| Sub-urban | 47 | 11.8 |
| Rural area | 54 | 13.5 |
| Monthly family income (BDT) | ||
| ≤20,000 | 115 | 28.7 |
| 21,000–40,000 | 137 | 34.3 |
| >40,000 | 148 | 37.0 |
| Eating Behavior and Related Issues | Frequency of Eating | ||
|---|---|---|---|
| Regular | Occasionally | Never | |
| Eat a variety of food from 6–8 food groups of food pyramid | 45 (11.3%) | 195 (48.8%) | 160 (40.0%) |
| Eat unpolished rice, wheat | 191 (47.8%) | 80 (20.0%) | 129 (32.3%) |
| Eat citrus and Vit-A rich fruits | 62 (15.5%) | 153 (38.3%) | 185 (46.3%) |
| Eat vegetables (leafy and non-leafy) | 25 (6.3%) | 144 (36.0%) | 231 (57.8%) |
| Eat fish/meat | 15 (3.8%) | 124 (31.0%) | 261 (65.3%) |
| Eat pulses and legumes | 49 (12.3%) | 124 (31.0%) | 227 (56.8%) |
| Eat foods containing excessive fats and oils/ eating fast foods | 67 (16.8%) | 167 (41.8%) | 166 (41.5%) |
| Eat sweetened foods | 191 (47.8%) | 151 (37.8%) | 58 (14.5%) |
| Drink milk and milk-based products | 157 (39.3%) | 113 (28.2%) | 130 (32.5%) |
| Eat fresh, well-prepared foods | 35 (8.8%) | 110 (27.5%) | 255 (63.7%) |
| Avoid overeating | 46 (11.5%) | 136 (34.0%) | 218 (54.5%) |
| Eat food with proper chewing | 49 (12.3%) | 91 (22.8%) | 260 (65.0%) |
| Always wash hands before meals | 12 (3.0%) | 42 (10.5%) | 346 (86.5%) |
| Has your body weight been measured monthly? | 145 (36.3%) | 106 (26.5%) | 149 (37.3%) |
| Perform exercise | 184 (46.0%) | 99 (24.8%) | 117 (29.3%) |
| Undertake clinical check-up at least once a year | 78 (19.5%) | 142 (35.5%) | 180 (45.0%) |
| Take enough rest and sleep (8 h) | 30 (7.5%) | 109 (27.3%) | 261 (65.3%) |
| Variable | Unadjusted Model | Adjusted Model † | ||||
|---|---|---|---|---|---|---|
| β | 95% CI | p Value | β | 95% CI | p Value | |
| Nutrition literacy | 0.275 | 0.24, 0.49 | <0.001 | 0.223 | 0.18, 0.41 | <0.001 |
| Model fitness | R2 | AIC | Mean VIF | Adjusted R2 | AIC | |
| 0.076 | 2367.03 | 1.47 | 0.354 | 2231.91 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Banna, M.H.; Hamiduzzaman, M.; Kundu, S.; Sultana, M.S.; Seidu, A.-A.; Brazendale, K.; Abid, M.T.; Ara, T.; Rifat, M.A.; Mozumder, N.H.M.R.; et al. Association between Nutrition Literacy and Bangladeshi Adults’ Healthy Eating Behaviors: Evidence from the Nutrition Literacy Study 2021. Healthcare 2022, 10, 2508. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122508
Al Banna MH, Hamiduzzaman M, Kundu S, Sultana MS, Seidu A-A, Brazendale K, Abid MT, Ara T, Rifat MA, Mozumder NHMR, et al. Association between Nutrition Literacy and Bangladeshi Adults’ Healthy Eating Behaviors: Evidence from the Nutrition Literacy Study 2021. Healthcare. 2022; 10(12):2508. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122508
Chicago/Turabian StyleAl Banna, Md. Hasan, Mohammad Hamiduzzaman, Satyajit Kundu, Mst. Sadia Sultana, Abdul-Aziz Seidu, Keith Brazendale, Mohammad Tazrian Abid, Tasnu Ara, M. A. Rifat, N. H. M. Rubel Mozumder, and et al. 2022. "Association between Nutrition Literacy and Bangladeshi Adults’ Healthy Eating Behaviors: Evidence from the Nutrition Literacy Study 2021" Healthcare 10, no. 12: 2508. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10122508