
The Use of Modern Technologies by Dentists in Poland: Questionnaire among Polish Dentists

 , ,
, ,  ,
, 
Abstract
:1. Introduction
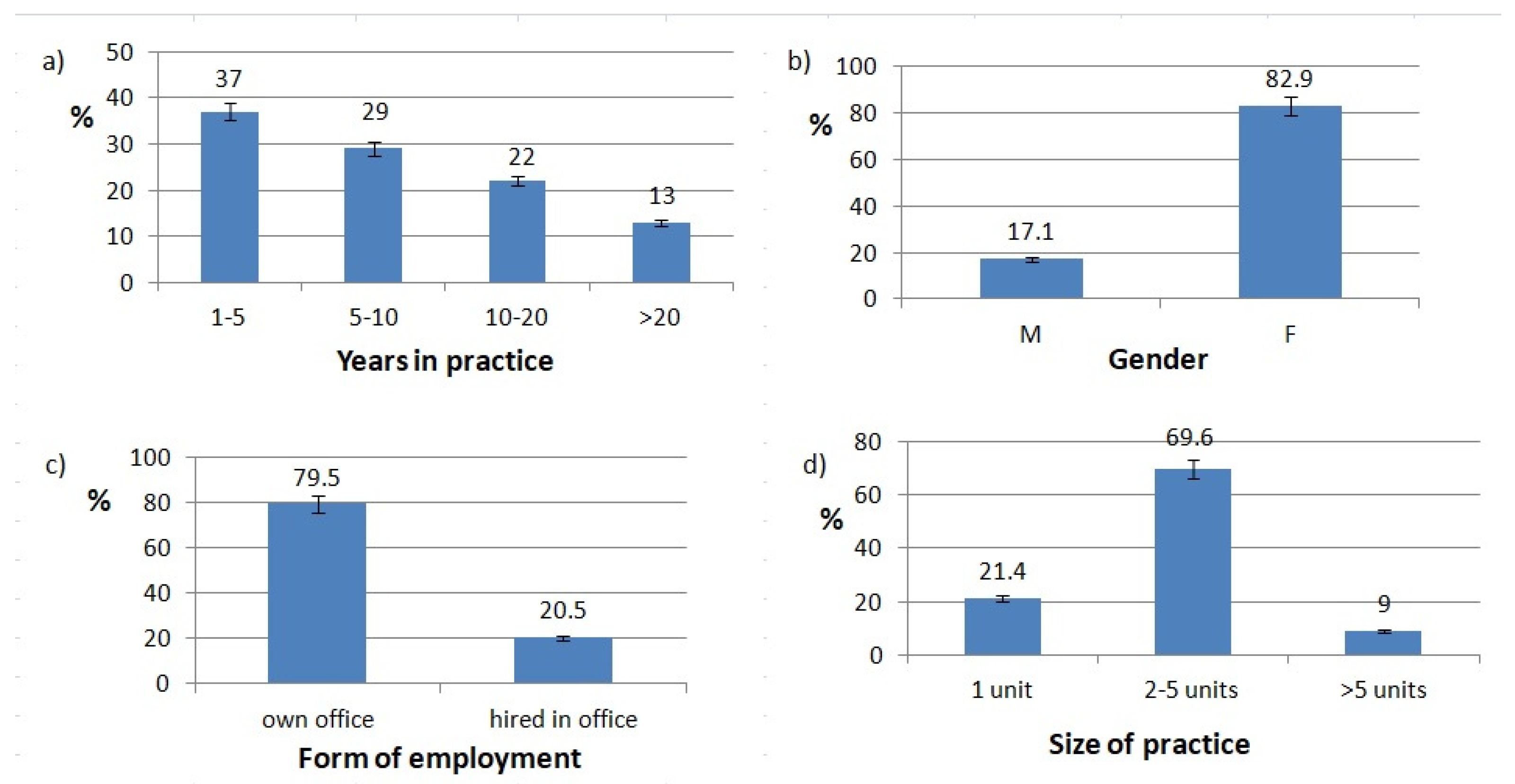
2. Materials and Methods
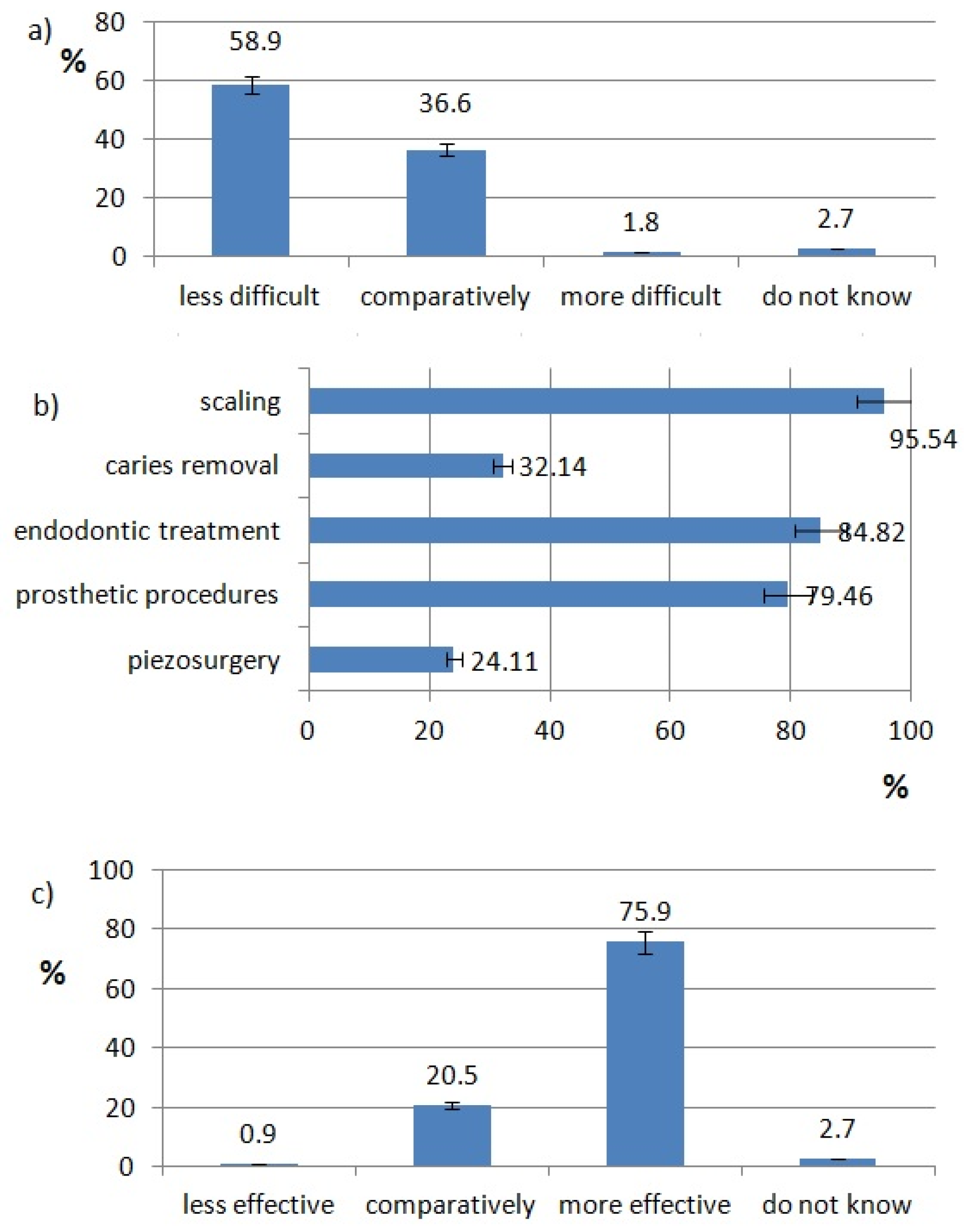
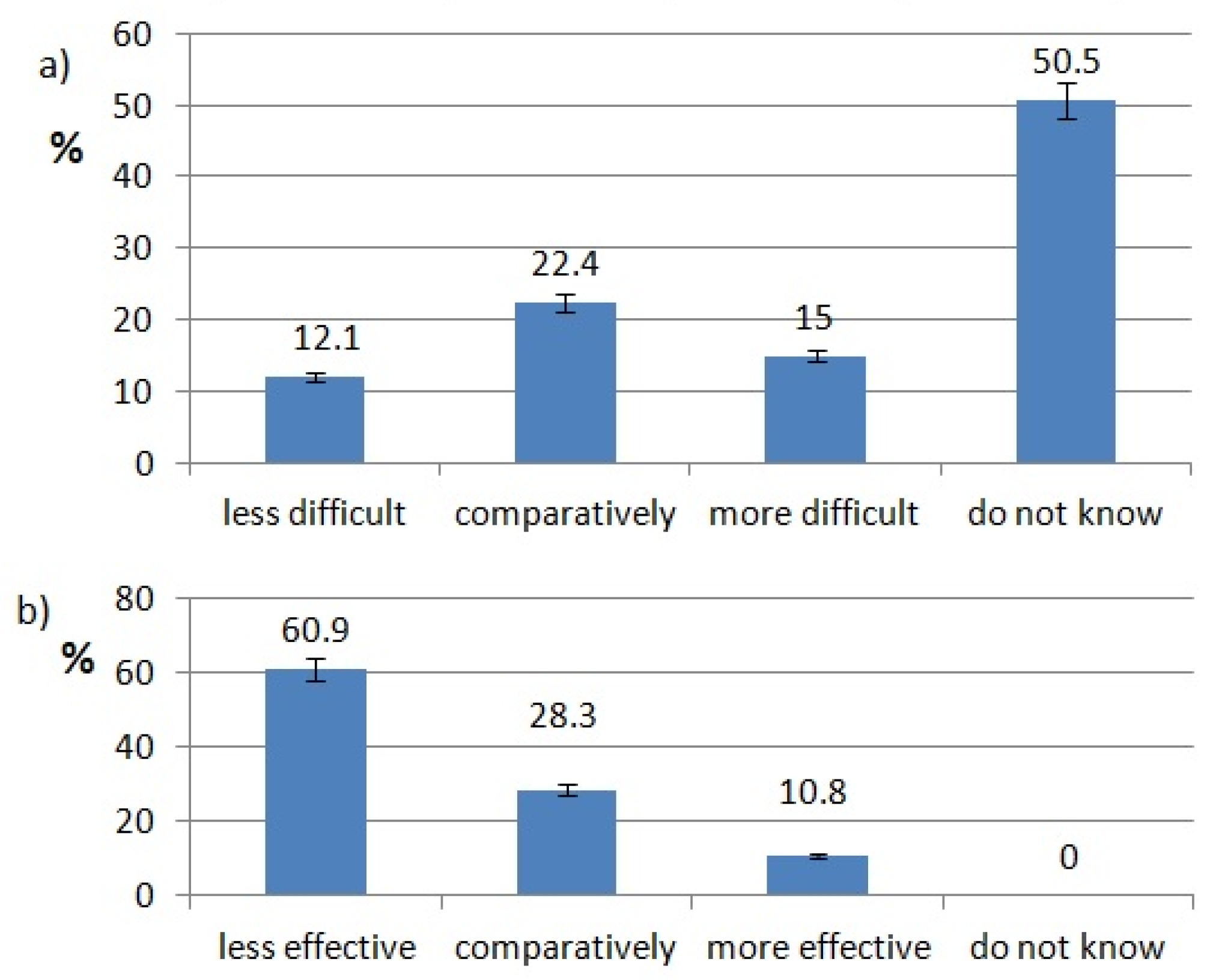
3. Results
4. Discussion
Publications Which Compare Use of Other Modern Technologies by Dentists in Europe
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Azarpazhooh, A.; Limeback, H. The application of ozone in dentistry: A systematic review of literature. J. Dent. 2008, 36, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Maiman, T.H. Stimulated Optical Radiation in Ruby. Nature 1960, 187, 493–494. [Google Scholar] [CrossRef]
- Lussi, A.; Imwinkelried, S.; Pitts, N.B.; Longbottom, C.; Reich, E. Performance and Reproducibility of a Laser Fluorescence System for Detection of Occlusal Caries in vitro. Caries Res. 1999, 33, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Gopikrishna, V.; Tinagupta, K.; Kandaswamy, D. Evaluation of Efficacy of a New Custom-Made Pulse Oximeter Dental Probe in Comparison With the Electrical and Thermal Tests for Assessing Pulp Vitality. J. Endod. 2007, 33, 411–414. [Google Scholar] [CrossRef]
- Friedman, M.J.; Hochman, M.N. A 21st century computerized injection system for local pain control. Compend. Contin. Educ. Dent. 1997, 18, 995–1003. [Google Scholar]
- Available online: https://forms.gle/SKwkp97q1j54N3wF7 (accessed on 22 February 2019).
- Verma, S.K.; Chaudhari, P.K.; Maheshwari, S.; Singh, R.K. Laser in dentistry: An innovative tool in modern dental practice. Natl. J. Maxillofac. Surg. 2012, 3, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Cozean, C.; Arcoria, C.J.; Pelagalli, J.; Powell, G.L. Dentistry for the 21st century? Erbium:Yag laser for teeth. J. Am. Dent. Assoc. 1997, 128, 1080–1087. [Google Scholar] [CrossRef]
- Valenti, C.; Pagano, S.; Bozza, S.; Ciurnella, E.; Lomurno, G.; Capobianco, B.; Coniglio, M.; Cianetti, S.; Marinucci, L. Use of the Er:YAG Laser in Conservative Dentistry: Evaluation of the Microbial Population in Carious Lesions. Materials 2021, 14, 2387. [Google Scholar] [CrossRef]
- Schwarz, F.; Arweiler, N.; Georg, T.; Reich, E. Desensitizing effects of an Er:YAG laser on hypersensitive dentine. J. Clin. Periodontol. 2002, 29, 211–215. [Google Scholar] [CrossRef]
- Walmsley, D.; Laird, W.; Lumley, P. Ultrasound in dentistry. Part 2—periodontology and endodontics. J. Dent. 1992, 20, 11–17. [Google Scholar] [CrossRef]
- Plotino, G.; Pameijer, C.H.; Grande, N.M.; Somma, F. Ultrasonics in Endodontics: A Review of the Literature. J. Endod. 2007, 33, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Abu Hasna, A.; Da Silva, L.P.; Pelegrini, F.C.; Ferreira, C.L.R.; De Oliveira, L.D.; Carvalho, C.A.T. Effect of sodium hypochlorite solution and gel with/without passive ultrasonic irrigation on Enterococcus faecalis, Escherichia coli and their endotoxins. F1000Research 2020, 9, 642. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.; Yadav, R.-K.; Tikku, A.-P.; Chandra, A.; Verma, P.; Bharti, R.; Shakya, V.-K. A randomized controlled trial of endodontic treatment using ultrasonic irrigation and laser activated irrigation to evaluate healing in chronic apical periodontitis. J. Clin. Exp. Dent. 2020, 12, e821–e829. [Google Scholar] [CrossRef] [PubMed]
- Ealla, K.K.R.; Thomas, M.; Akula, U.; Gajjada, N. Piezosurgery: A boon for modern periodontics. J. Int. Soc. Prev. Community Dent. 2017, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, E. Escalating Role of Piezosurgery in Dental Therapeutics. J. Clin. Diagn. Res. 2014, 8, ZE08–11. [Google Scholar] [CrossRef] [PubMed]
- Otake, Y.; Nakamura, M.; Henmi, A.; Takahashi, T.; Sasano, Y. Experimental Comparison of the Performance of Cutting Bone and Soft Tissue between Piezosurgery and Conventional Rotary Instruments. Sci. Rep. 2018, 8, 17154. [Google Scholar] [CrossRef] [PubMed]
- Hegde, V.S.; Khatavkar, A.R. A new dimension to conservative dentistry: Air abrasion. J. Conserv. Dent. 2010, 13, 4–8. [Google Scholar] [CrossRef] [Green Version]
- Bhushan, U.; Goswami, M. Evaluation of retention of pit and fissure sealants placed with and without air abrasion pretreatment in 6-8 year old children—An in vivo study. J. Clin. Exp. Dent. 2017, 9, e211–e217. [Google Scholar] [CrossRef]
- Domb, W.C. Ozone Therapy in Dentistry. Interv. Neuroradiol. 2014, 20, 632–636. [Google Scholar] [CrossRef] [Green Version]
- Gupta, G.; Mansi, B. Ozone therapy in periodontics. J. Med. Life 2012, 5, 59–67. [Google Scholar]
- Gomez, J.L. Detection and diagnosis of the early caries lesion. BMC Oral Health 2015, 15, S3. [Google Scholar] [CrossRef] [Green Version]
- Cho, K.H.; Kang, C.-M.; Jung, H.-I.; Lee, H.-S.; Lee, K.; Lee, T.Y.; Song, J.S. The diagnostic efficacy of quantitative light-induced fluorescence in detection of dental caries of primary teeth. J. Dent. 2021, 115, 103845. [Google Scholar] [CrossRef]
- Venkataraghavan, K.; Kush, A.; Lakshminarayana, C.; Diwakar, L.; Ravikumar, P.; Patil, S.; Karthik, S. Chemomechanical Caries Removal: A Review & Study of an Indigen-ously Developed Agent (Carie Care (TM) Gel) In Children. J. Int. Oral Health 2013, 5, 84–90. [Google Scholar]
- Sontakke, P.; Jain, P.; Patil, A.D.; Biswas, G.; Yadav, P.; Makkar, D.K.; Jeph, V.; Sakina, B.P. A comparative study of the clinical efficiency of chemo-mechanical caries removal using Carie-Care gel for permanent teeth of children of age group of 12-15 years with that of conventional drilling method: A randomized controlled trial. Dent. Res. J. 2019, 16, 42–46. [Google Scholar] [CrossRef]
- Yavagal, C.; Prabhakar, A.; Lokeshwari, M.; Naik, S.V. Efficacy of Caries Removal by Carie-Care and Erbiumdoped Yttrium Aluminum Garnet Laser in Primary Molars: A Scanning Electron Microscope Study. Int. J. Clin. Pediatr. Dent. 2018, 11, 323–329. [Google Scholar] [CrossRef]
- Cardoso, M.; Coelho, A.; Lima, R.; Amaro, I.; Paula, A.; Marto, C.M.; Sousa, J.; Spagnuolo, G.; Ferreira, M.M.; Carrilho, E. Efficacy and Patient’s Acceptance of Alternative Methods for Caries Removal—a Systematic Review. J. Clin. Med. 2020, 9, 3407. [Google Scholar] [CrossRef]
- Salgar, A.R.; Singh, S.H.; Podar, R.S.; Kulkarni, G.P.; Babel, S.N. Determining predictability and accuracy of thermal and electrical dental pulp tests: An in vivo study. J. Conserv. Dent. 2017, 20, 46–49. [Google Scholar] [CrossRef]
- Mainkar, A.; Kim, S.G. Diagnostic Accuracy of 5 Dental Pulp Tests: A Systematic Review and Meta-analysis. J. Endod. 2018, 44, 694–702. [Google Scholar] [CrossRef]
- Aggarwal, K.; Lamba, A.K.; Faraz, F.; Tandon, S.; Makker, K. Comparison of anxiety and pain perceived with conventional and computerized local anesthesia delivery systems for different stages of anesthesia delivery in maxillary and mandibular nerve blocks. J. Dent. Anesthesia Pain Med. 2018, 18, 367–373. [Google Scholar] [CrossRef]
- Mittal, M.; Chopra, R.; Kumar, A.; Srivastava, D. Comparison of Pain Perception Using Conventional Versus Computer-Controlled Intraligamentary Local Anesthetic Injection for Extraction of Primary Molars. Anesth. Prog. 2019, 66, 69–76. [Google Scholar] [CrossRef]
- Flisfisch, S.; Woelber, J.P.; Walther, W. Patient evaluations after local anesthesia with a computer-assisted method and a conventional syringe before and after reflection time: A prospective randomized controlled trial. Heliyon 2021, 7, e06012. [Google Scholar] [CrossRef] [PubMed]
- Pozos-Guillén, A.; Loredo-Cruz, E.; Esparza-Villalpando, V.; Martínez-Rider, R.; Noyola-Frías, M.; Garrocho-Rangel, A. Pain and Anxiety Levels Using Conventional versus Computer-Controlled Local Anesthetic Systems in Pediatric Patients: A Meta-Analysis. J. Clin. Pediatr. Dent. 2020, 44, 371–399. [Google Scholar] [CrossRef] [PubMed]
- Nassar, H.M.; Yeslam, H.E. Current Novel Caries Diagnostic Technologies: Restorative Dentists’ Attitude and Use Preferences. Healthcare 2021, 9, 1387. [Google Scholar] [CrossRef] [PubMed]
- Tran, D.; Nesbit, M.; Petridis, H. Survey of UK dentists regarding the use of CAD/CAM technology. Br. Dent. J. 2016, 221, 639–644. [Google Scholar] [CrossRef]
- Van Der Zande, M.M.; Gorter, R.C.; Aartman, I.H.A.; Wismeijer, D. Adoption and Use of Digital Technologies among General Dental Practitioners in the Netherlands. PLoS ONE 2015, 10, e0120725. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions in Survey | Responds |
|---|---|
| Biometric questions | |
| 1. Gender (choice question) | Male/Female |
| 2. Years in practice (graded question) | <5/5–10/10–20/>20 |
| 3. specialization (multiple choice question) |
|
| 4. Form of employment (choice question) |
|
| 5. Size of office (graded question) | one unit/two to five units/>five units |
| Questions in each technology section | |
| 1. Have you access to this technology in your practice? (graded question) | Yes/No |
| 2. How often do you use this technology? (graded question) |
|
| 3. How do you rate efficiency of this technology? (graded question) |
|
| 4. How do you rate difficulty of this technology? (graded question) |
|
| 5. Will you use this technology in the future? (choice question) | Yes/No/Maybe |
| General questions | |
| 1. About how many methods you didn’t know? (graded question) | 1–5/6–10/>10 |
| 2. Why don’t you use mentioned technologies? (multiple choice question) |
|
| 3. What is the attitude of patients to innovative technologies? (choice question) |
|
| 4. Which sources of knowledge do you use to acquire competency about mentioned technologies? (multiple choice question) |
|
| Technology | Percentage of Use |
|---|---|
| Laser | 25 |
| Ultrasounds | 97 |
| Air abrasion | 28 |
| Ozone | 6 |
| CDM | 33 |
| CMCR | 21 |
| PVT | 18 |
| CCLAD | 43 |
| CCLAD | PVT | CMCR | CDM | Ozone | Air Abrasion | Ultrasounds | Laser | Technology | |
|---|---|---|---|---|---|---|---|---|---|
| 33 (43) | 11 (16) | 20 (29) | 18 (26) | 2 (3) | 20 (29) | 65 (94) | 13 (19) | <5 (n = 69) | Years in practice |
| 23 (43) | 7 (13) | 8 (15) | 18 (33) | 6 (11) | 15 (28) | 54 (100) | 17 (31) | 5–10 (n = 54) | |
| 11 (27) | 8 (20) | 12 (29) | 15 (37) | 2 (5) | 13 (32) | 41 (100) | 12 (29) | 10–20 (n = 41) | |
| 13 (57) | 7 (30) | 0 (0) | 11 (48) | 2 (9) | 5 (22) | 22 (96) | 12 (29) | >20 (n = 23) | |
| 0.08 | 0.03 | 0.009 * | 0.261 | 0.288 | 0.862 | 0.142 | 0.373 | P | |
| 8 (20) | 7 (18) | 7 (18) | 15 (38) | 2 (5) | 8 (20) | 37 (93) | 2 (5) | 1 unit (n = 40) | Size of office |
| 64 (49) | 23 (18) | 28 (22) | 42 (32) | 8 (6) | 41 (32) | 128 (98) | 41 (32) | 2–5 u. (n = 130) | |
| 8 (47) | 3 (18) | 5 (29) | 5 (29) | 2 (12) | 3 (18) | 17 (100) | 4 (24) | >5 u. (n = 17) | |
| 0.004 * | 0.999 | 0.603 | 0.782 | 0.619 | 0.224 | 0.096 | 0.003 * | P | |
| 67 (43) | 28 (18) | 33 (21) | 55 (35) | 12 (8) | 50 (32) | 152 (97) | 37 (24) | F (n = 157) | Gender |
| 13 (43) | 5 (17) | 7 (23) | 7 (23) | 0 (0) | 3 (10) | 30 (100) | 10 (33) | M (n = 30) | |
| 0.947 | 0.878 | 0.777 | 0.212 | 0.118 | 0.015 * | 0.322 | 0.259 | P |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Świtała, M.; Zakrzewski, W.; Rybak, Z.; Szymonowicz, M.; Dobrzyński, M. The Use of Modern Technologies by Dentists in Poland: Questionnaire among Polish Dentists. Healthcare 2022, 10, 225. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10020225
Świtała M, Zakrzewski W, Rybak Z, Szymonowicz M, Dobrzyński M. The Use of Modern Technologies by Dentists in Poland: Questionnaire among Polish Dentists. Healthcare. 2022; 10(2):225. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10020225
Chicago/Turabian StyleŚwitała, Mateusz, Wojciech Zakrzewski, Zbigniew Rybak, Maria Szymonowicz, and Maciej Dobrzyński. 2022. "The Use of Modern Technologies by Dentists in Poland: Questionnaire among Polish Dentists" Healthcare 10, no. 2: 225. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10020225