
Teaching and Learning of Clinical Competence in Ghana: Experiences of Students and Post-Registration Nurses



Abstract
:1. Introduction
Nursing Education in the Research Context
2. Methods
2.1. Design
2.2. Study Setting and Participants
2.3. Data Collection
2.4. Ethical Considerations
2.5. Data Analysis
2.6. Rigour
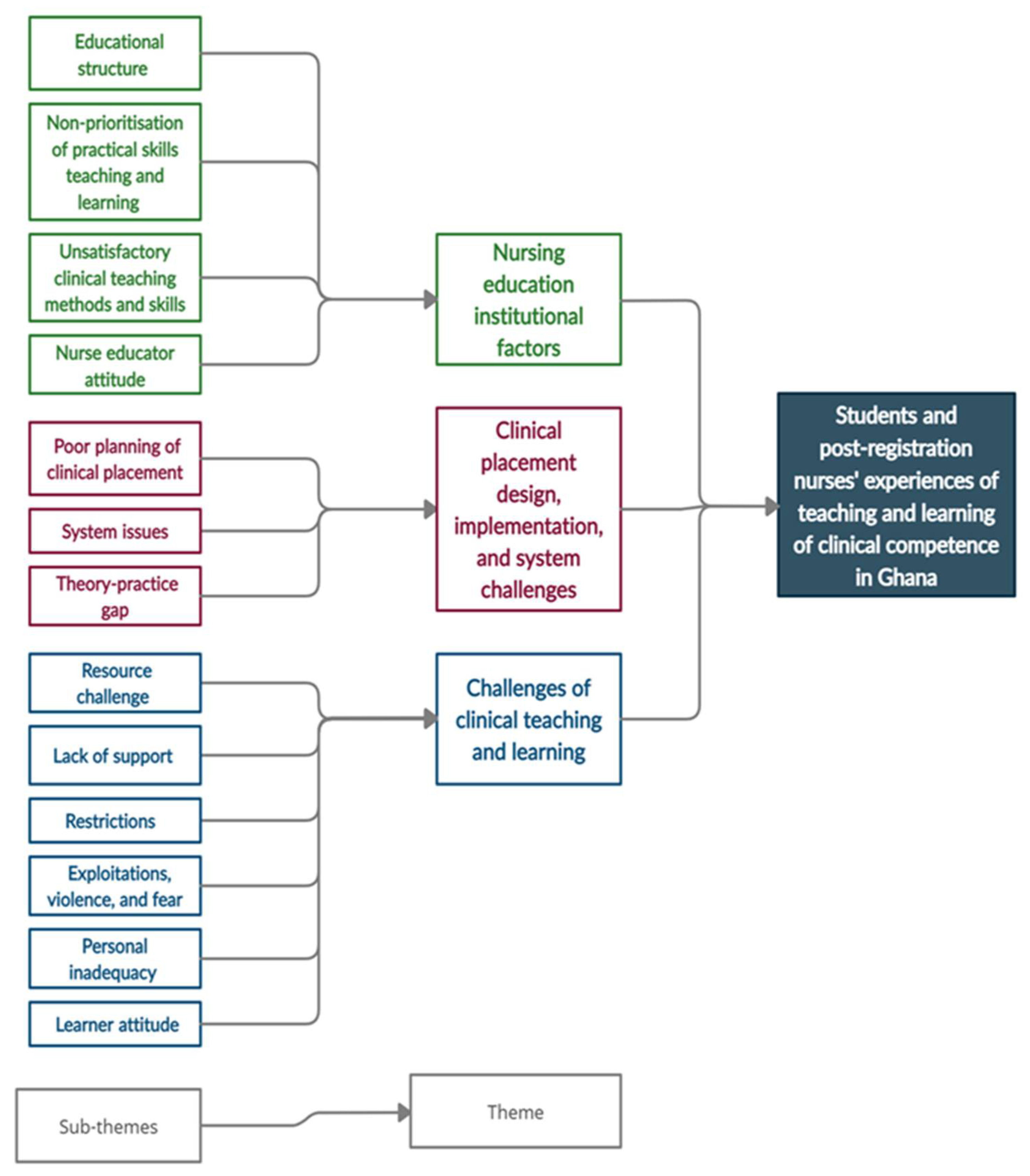
3. Results
3.1. Demographic Characteristics of Participants
3.2. Theme 1: Nursing Education Institutional Factors
3.2.1. Educational Structure
“Maybe the problem is coming from our education system, how our educational system is being structured is not helping us, the classroom is more of theory, theory, theory, since we reopened school, we’ve not done one practical at the skills laboratory, which is very bad, is theory, theory, theory, but the work is actually practical, so I prefer the practical should be more.”(Third-year student S3STN3).
“Now when you also come to the school, there you will realize that most NCs they have moved from practical aspect, and they are now focusing on the theoretical aspect.”(Post-registration nurse NPRN6).
3.2.2. Non-Prioritization of Practical Skills Teaching and Learning
“The students are very plenty, we are too much, when you go for practical in the skills lab, to the extent that at times you don’t even see what they are doing when you are forced to stand at the back because of the huge numbers.”(Third-year student S3STN3).
“Concerning the challenges in our skills lab, first of all, let’s start with the overcrowding, because of our huge numbers, one class can have sixty plus students entering a small skills lab, no place to sit like my brother said always standing.”(Second-year student N2STN7).
“…the time we have for the skills laboratory within a week is too short, one hour for skills laboratory, that one hour is not really helping us. Because most of us don’t get the opportunity to practice.”(Third-year student S3STN2).
“Sometimes even if we go to the skills laboratory to learn those procedures, because the equipment is not available it will be very difficult for us to learn it.”(Third-year student N3STN6).
“You can’t even go there because you are even scared to go and spoil something, because here if you spoil anything you will buy.”(Second-year student S2STN1).
“Another challenge is that sometimes you will want to go to the skills lab…and then you realize that it is locked, then you can’t find the skills lab tutor to open it for you to learn.”(Third-year student N3STN1).
“…is the skills lab that is helping us to learn the practical properly … when we go there, we normally learn the right things as compared to when we go to the wards.”(Third-year nursing student N3STN2).
3.2.3. Unsatisfactory Clinical Teaching Methods and Skills
“We expect him to know each procedure he’s taking us through.”(Third-year student N3STN6).
“… the tutor will come, project what we are supposed to do and be reading the slides for you, but you know this is something you have to see, this is something that you have to handle but the person is reading it so that you will also follow.”(Post-registration nurse NPRN6).
“…what helps us in transferring the knowledge we received in the classroom into practical skills is that we do a lot of peer-tuition.”(Third-year student M3STN1).
“Regarding the videos, the video tutorials we watch, they are mostly in a different environment or usually setting the international world. So, there is always a vast difference. Sometimes the equipment they use to do it, we doubt that we have them in Ghana here but, we always just want to see how it is done so that we will just have an idea or a view of how that procedure is done.”(Third-year student N3STN1).
3.2.4. Nurse Educator Attitude
“Some of the tutors come to the class with their own issues from home, so they will come and bring their issues on you, like anger.”(Second-year student S2STN5).
3.3. Theme 2: Clinical Placement Design, Implementation, and System Challenges
3.3.1. Poor Planning of Clinical Placement
“…we go to the ward and then do like two weeks practical, when we come back learning becomes difficult for us, so for me, I think when we come to school, we should just focus on the theory and then do the practical when we go on vacation.”(Third-year student S3STN5).
“…the hospitals that they send students to go and learn, the schools should do much research on the hospitals to find out whether the hospitals have the equipment that can aid student learning. The school may send you to a district hospital and over there you go and maybe a day they wouldn’t even have patients in the hospital. You will just be sitting there until it is time for you to close then you close and go.”(Third-year student N3STN6).
“Most often too, what you learnt that you need to put to practice is not where you get to be posted to, a typical example is, you learnt pediatric nursing and you go and you have been sent to the labor ward.”(Third-year student M3STN3).
“It is quite unfortunate sometimes we get there and because all of us cannot be contained in a particular ward, we have to be distributed to other wards.”(Third-year student M3STN2).
“We go with our competencies and at the end of the day sometimes, after your clinical you haven’t even done one procedure from the competencies, its other things you are doing.”(Post-registration nurse NPRN3).
3.3.2. System Issues
“…because our school do not care, the only thing they do is they will give you the competencies you will go on clinical and at the end of the day they will be expecting you to bring back your book signed but, if the school is there they are monitoring, they have sat down with the hospital, my students are coming because of this procedure in Obstetric and Gynecological ward, so please make sure you send them to O and G block so that they can learn what is on the competencies, that one is going to help them.”(Post-registration nurse NPRN3).
“Let me take the cardiac bed for instance, some books will say you should use four pillows, and some will say five. We don’t even know which one to stick to. This person will be reading different thing and I will also be reading a different thing. We will end up confusing ourselves. So, it makes it difficult for us to actually practice what is right.”(Third-year student N3STN8).
“…after completion, our postings delay, we like this, we sat home for almost a year before we were posted for our national service, and you know, nursing is a practice profession, when you sit home for that long without practicing and you are posted later, you turn to forget most of the things, it is hurtful.”(Post-registration nurse NPRN 7).
3.3.3. Theory-Practice Gap
“So, looking at what is happening in our hospitals or wards right now, sending students for clinical is waste of their time because how things are done in the ward is different from what is being taught in the classroom.”(Post-registration nurse NPRN 7).
“So, I feel like now we actually learnt and now we are unlearning because some skills that you have or some knowledge that you have you can’t put them in practice because they will tell you that you just can’t practice it because that is what is available for them to practice so you also just have to go through the trend.”(Post-registration nurse NPRN7).
“I have passed through this problem before during practical, what I did was what the man taught me, but the other person said it was not like that, it is different. So, I got angry, very, very angry and the tutor walked me out.”(Second-year student N2STN2).
3.4. Theme 3: Challenges of Clinical Teaching and Learning
3.4.1. Resource Challenge
“The more you practice the better you become, unfortunately, most at times we don’t even get, the material to do the right thing, so we always end up doing the wrong thing at the clinical site.”(Second-year student M2STN2).
“I think it’s as a result of insufficient equipment that is why maybe the staff use “shortcuts” in performing nursing procedures in the ward.”(Second-year student M2STN3).
“We have to improvise or we have to imagine that the item is there and we are using it and nursing is not about imagining or improvising.”(Second-year student M2STN1).
3.4.2. Lack of Support
“… the unwillingness of the staff nurses to teach us, you see the thing, they are not willing to teach at all.”(Second-year student N2STN7).
“I have specific wards where I have made friends, so whenever we go to that hospital, I usually make sure that when they are to draw the timetable, I will lobby with them to partner me with those people on shifts. When I am running shift with them, I learn a lot.”(Second-year student N2STN5).
“…when you come to the ward, we are all doing trial and error, so if it works it works, because we have to get it and that is what we are doing.”(Post-registration nurse NPRN6).
3.4.3. Restrictions
“…if you are a student all the time vitals, that’s all. Medication is done by the staff and the vitals students, documentation and stuff students. But when it comes to the actual procedures like medication administration and wound dressing, they won’t even allow you the student to come near.”(Third-year student N3STN8).
“I remember I was at one ward and I got there and the patient was like why? Is it because there are no staff in the ward that is why they are assigning a student to her? She even sacked me from the room that I shouldn’t come near her, it was very bad.”(Third-year student S3STN4).
3.4.4. Exploitations, Violence, and Fear
“They leave the work in our hands then they will be sitting at the nurses’ station, is very bad.”(Second-year student S2STN3).
“Immediately staff see students in the ward they begin to make you run errands. You can run errands for the whole shift. So, you wouldn’t even have time to learn what you are supposed to learn. Sometimes you go to the ward then a staff gives you a motor bike to go to town and buy food, which is very far, by the time you are back another one is sending you to go and buy fuel, by the time you are back your shift is over.”(Third-year student N3STN1).
“…some hospitals demand gloves, you have to buy gloves before you are accepted into the hospital on clinical placement. We are students, we are not people who have salary, so why that policy? In this corona era, one box of gloves cost over GH₵50, so you are asking a student each to produce one box of gloves why.”(Second-year student N2STN3).
“…they will be shouting on you and they will let every patient know that you are a student, that’s the bad aspect of nursing, so, at times when you go to the patient’s bedside, they will be like are you a student, some will even tell us that they won’t allow us to work on them.”(Third-year student S3STN1).
“Sometimes you are eager to do something for the patient but they will tell you if you do something and it goes wrong, they will hand you over to the appropriate quarters so that they would deal with you. So, in these instances, it put a lot of fears in us the students to come out of our shells and do something.”(Third-year student M3STN1).
3.4.5. Personal Inadequacy
“When you are being asked to say it verbally, you will do it or if you are being asked to write it, you will do it. But here is the case, do it let me see so that I can score you, then you find yourself wanton because you don’t know the equipment.”(Second-year student M2STN3).
3.4.6. Learner Attitude
“Some of the student too because of their attitude they tend to run away and not practice or learn anything from the ward.”(Third-year student S3STN5).
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jeffries, P.R. The NLN Jeffries Simulation Theory, 1st ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2016; pp. 39–44. [Google Scholar]
- Dunn, S.; Ehrich, L.; Mylonas, A.; Hansford, B. Students’ perceptions of filed experience in professional development: A comparative study. J. Nurs. Educ. 2000, 39, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.I.; Kim, J.A.; Ko, J.-K.; Chung, M.S.; Bang, K.-S.; Choe, M.-A.; Yoo, M.S.; Jang, H.Y. An identification study on core nursing competency. J. Korean Acad. Soc. Nurs. Educ. 2013, 19, 663–674. [Google Scholar] [CrossRef] [Green Version]
- Fukada, M. Nursing Competency: Definition, Structure and Development. Yonago Acta Med. 2018, 61, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Notarnicola, I.; Petrucci, C.; De Jesus Barbosa, M.; Giorgi, F.; Stievano, A.; Lancia, L. Clinical competence in nursing: A concept analysis. Prof. Inferm. 2016, 69, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Dahlke, S.; O’Connor, M.; Hannesson, T.; Cheetham, K. Understanding clinical nursing education: An exploratory study. Nurse Educ. Pract. 2016, 17, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Heidari, M.R.; Norouzadeh, R. Nursing students’ perspectives on clinical education. J. Adv. Med. Educ. Prof. 2015, 3, 39–43. [Google Scholar]
- Farzi, S.; Shahriari, M.; Farzi, S. Exploring the challenges of clinical education in nursing and strategies to improve it: A qualitative study. J. Educ. Health Promot. 2019, 7, 1–8. [Google Scholar] [CrossRef]
- Voldbjerg, S.L.; Gronkjaer, M.; Sorensen, E.E.; Hail, E.O.C. Newly graduated nurses’ use of knowledge sources: A meta-ethnography. J. Adv. Nurs. 2016, 72, 1751–1765. [Google Scholar] [CrossRef] [PubMed]
- Rodger, S.; Webb, G.; Devitt, L.; Gilbert, J.; Wrightson, P.; McMeeken, J. Clinical education and practice placements in the allied health professions: An international perspective. J. Allied Health 2008, 37, 53–62. [Google Scholar] [PubMed]
- Fawaz, M.A.; Hamdan-Mansour, A.M.; Tassi, A. Challenges facing nursing education in the advanced healthcare environment. Int. J. Afr. Nurs. Sci. 2018, 9, 105–110. [Google Scholar] [CrossRef]
- Whitehead, B.; Owen, P.; Holmes, D.; Beddingham, E.; Simmons, M.; Henshaw, L.; Barton, M.; Walker, C. Supporting newly qualified nurses in the UK: A systematic literature review. Nurse Educ. Today 2013, 33, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Salifu, D.A.; Gross, J.; Salifu, M.A.; Ninnoni, J.P. Experiences and perceptions of the theory—Practice gap in nursing in a resource—Constrained setting: A qualitative description study. Nurs. Open 2019, 6, 72–83. [Google Scholar] [CrossRef]
- Jamshidi, N.; Molazem, Z.; Sharif, F.; Torabizadeh, C.; Kalyani, M.N. The Challenges of nursing students in the clinical learning environment: A qualitative study. Sci. World J. 2016, 2016, 1846178. [Google Scholar] [CrossRef] [Green Version]
- Begley, T. Who am I now? The experience of being a post-registration children’s student nurse in the first clinical placement. Nurse Educ. Today 2007, 27, 375–381. [Google Scholar] [CrossRef]
- Asirifi, M.; Ogilvie, L.; Barton, S.; Aniteye, P.; Stobart, K.; Bilash, O.; Eliason, C.; Achempim-Ansong, G.; Kwashie, A.; Aziato, L. Reconceptualizing preceptorship in clinical nursing education in Ghana. Int. J. Afr. Nurs. Sci. 2019, 10, 159–166. [Google Scholar] [CrossRef]
- Botma, Y.; Rensburg, G.H.; Van Coetzee, I.M.; Heyns, T. A conceptual framework for educational design at modular level to promote transfer of learning. Innov. Educ. Teach. Int. 2016, 52, 499–509. [Google Scholar] [CrossRef] [Green Version]
- Talley, B. Nurses and nursing education in Ghana: Creating collaborative opportunities. Int. Nurs. Rev. 2006, 53, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Khatiban, M.; Sangestani, G. The effects of using problem-based learning in the clinical nursing education on the students’ outcomes in Iran: A quasi-experimental study. Nurse Educ. Pract. 2014, 14, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.; Echeazarra, L.; Sanz-Santamaría, S.; Gutiérrez, J. Student generated online videos to develop cross-curricular and curricular competencies in Nursing Studies. Comput. Hum. Behav. 2014, 31, 580–590. [Google Scholar] [CrossRef]
- Asamani, J.A.; Christmals CDela Reitsma, G.M. Health service activity standards and standard workloads for primary healthcare in Ghana: A cross-sectional survey of health professionals. Healthcare 2021, 9, 332. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.; Williams, E.P. Contemporary Models for Clinical Nursing Education; Sigma Repository: Hattiesburg, MS, USA, 2017. [Google Scholar]
- Niederhauser, V.; Schoessler, M.; Gubrud-Howe, P.M.; Magnussen, L.; Codier, E. Creating innovative models of clinical nursing education. J. Nurs. Educ. 2012, 51, 603–608. [Google Scholar] [CrossRef] [Green Version]
- Mar, I.; Fern, C.; Hern, M. Role-Play versus Standardised Patient Simulation for Teaching Interprofessional Communication in Care of the Elderly for Nursing Students. Healthcare 2022, 10, 46. [Google Scholar] [CrossRef]
- Cant, R.P.; Cooper, S.J. Use of simulation-based learning in undergraduate nurse education: An umbrella systematic review. Nurse Educ. Today 2017, 49, 63–71. [Google Scholar] [CrossRef]
- Opare, M.; Mill, J.E. The evolution of nursing education in a postindependence context-Ghana from 1957 to 1970. West. J. Nurs. Res. 2000, 22, 936. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.A.; Rominski, S.; Bam, V.; Donkor, E.; Lori, J. Analysis of nursing education in Ghana: Priorities for scaling-up the nursing workforce. Nurs. Health Sci. 2013, 15, 244–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asamani, J.A.; Amertil, N.P.; Ismaila, H.; Orem, J.N. The imperative of evidence-based health workforce planning and implementation: Lessons from nurses and midwives’ unemployment crisis in Ghana. Hum. Resour. Health 2020, 18, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Standards for the Initial Education of Professional Nurses and Midwives; World Health Organization: Geneva, Switzerland, 2009. Available online: http://www.who.int/hrh/nursing_midwifery/en/ (accessed on 25 December 2021).
- Sandelowski, M. Whatever happened to qualitative description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streubert, H.J.; Carpenter, D.R. Qualitative Research in Nursing: Advancing the Humanistic Perspective; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011. [Google Scholar]
- Gerrish, K.; Lacey, A. The Research Process in Nursing, 6th ed.; Wiley-Blackwell: Oxford, UK, 2010. [Google Scholar]
- Pope, C.; Ziebland, S.; Mays, N. Analyzing qualitative data. Qual. Res. Health Care Br. Med. J. 2000, 320, 114–116. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Coleman, P. “Yes, the type of student supervision matters, but what about the placement structure?”—A critical realist review of block and integrated practice learning models within pre-registration nursing programmes. J. Nurs. Educ. Pract. 2020, 11, 39. [Google Scholar] [CrossRef]
- Rohatinsky, N.; Chachula, K.; Compton, R.; Sedgwick, M.; Press, M.; Lane, B. Nursing student preference for block versus nonblock clinical dodels. J. Nurs. Educ. 2017, 56, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Killam, L.A.; Heerschap, C. Challenges to student learning in the clinical setting: A qualitative descriptive study. Nurse Educ. Today 2013, 33, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Spector, N.; Blegen, M.A.; Silvestre, J.; Barnsteiner, J.; Lynn, M.; Ulrich, B.; Fogg, L.; Alexander, M. Transition to practice study in hospital settings. J. Nurs. Regul. 2015, 5, 24–38. [Google Scholar] [CrossRef]
- Elliot, K.M.; Dooyoung, S. Student satisfaction: An alternative approach to assessing this important concept. J. High Educ. Policy Manag. 2002, 24, 197–209. [Google Scholar] [CrossRef]
- Bvumbwe, T.; Mtshali, N.G. Transforming nursing education to strengthen health system in Malawi: An exploratory study. Open Nurs. J. 2018, 12, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Levett-Jones, T.; Fitzgerald, M. A review of graduate nurse transition programs in Australia. Aust. J. Adv. Nurs. 2005, 23, 40–45. [Google Scholar]


{kind=link}
|
| Variables | Students | Post-Registration Nurses |
|---|---|---|
| Gender | ||
| Male | 25 | 7 |
| Female | 15 | 8 |
| Age (in years) | ||
| 21–25 | 33 | 7 |
| 26–30 | 7 | 8 |
| 31–35 | - | - |
| 36–40 | - | - |
| 41–45 | - | - |
| Program level | ||
| Second year | 20 | - |
| Third year | 20 | - |
| Zone | ||
| Northern zone | 15 | 7 |
| Middle zone | 12 | 5 |
| Southern zone | 13 | 4 |
| Work experience (in months) | ||
| 1–5 | - | 6 |
| 6–10 | - | 2 |
| 11–15 | - | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salifu, D.A.; Heymans, Y.; Christmals, C.D. Teaching and Learning of Clinical Competence in Ghana: Experiences of Students and Post-Registration Nurses. Healthcare 2022, 10, 538. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10030538
Salifu DA, Heymans Y, Christmals CD. Teaching and Learning of Clinical Competence in Ghana: Experiences of Students and Post-Registration Nurses. Healthcare. 2022; 10(3):538. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10030538
Chicago/Turabian StyleSalifu, David Abdulai, Yolande Heymans, and Christmal Dela Christmals. 2022. "Teaching and Learning of Clinical Competence in Ghana: Experiences of Students and Post-Registration Nurses" Healthcare 10, no. 3: 538. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10030538