
Differences in Overweight and Obesity Prevalence among Young Men from Twelve Middle Eastern and Asian Countries Living in Saudi Arabia

 , , , , , and
, , , , , and
Abstract
:
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Sociodemographic Data
2.3. Anthropometry Data
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaacks, L.M.; Vandevijvere, S.; Pan, A.; McGowan, C.J.; Wallace, C.; Imamura, F.; Mozaffarian, D.; Swinburn, B.; Ezzati, M. The obesity transition: Stages of the global epidemic. Lancet Diabetes Endocrinol. 2019, 7, 231–240. [Google Scholar] [CrossRef]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregg, E.; Shaw, J.E. Global Health Effects of Overweight and Obesity. New Engl. J. Med. 2017, 377, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Alshwaiyat, N.M.; Ahmad, A.; Hassan, W.M.R.W.; Al-Jamal, H.A.N. Association between obesity and iron deficiency (Review). Exp. Ther. Med. 2021, 22, 1268. [Google Scholar] [CrossRef] [PubMed]
- Fruh, S.M. Obesity: Risk factors, complications, and strategies for sustainable long-term weight management. J. Am. Assoc. Nurse Pract. 2017, 29, S3–S14. [Google Scholar] [CrossRef]
- Wharton, S.; Lau, D.C.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in adults: A clinical practice guideline. Can. Med Assoc. J. 2020, 192, E875–E891. [Google Scholar] [CrossRef]
- Albuquerque, D.; Nóbrega, C.; Manco, L.; Padez, C. The contribution of genetics and environment to obesity. Br. Med Bull. 2017, 123, 159–173. [Google Scholar] [CrossRef]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic Of Obesity And Civilization Diseases. Diabetes, Metab. Syndr. Obes. Targets Ther. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [Green Version]
- Wadden, T.A.; Tronieri, J.S.; Butryn, M.L. Lifestyle modification approaches for the treatment of obesity in adults. Am. Psychol. 2020, 75, 235–251. [Google Scholar] [CrossRef]
- Dietz, W.H. Obesity and excessive weight gain in young adults: New targets for prevention. JAMA 2017, 318, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Larsen, P.; The, N.S.; Adair, L.S. Longitudinal Trends in Obesity in the United States From Adolescence to the Third Decade of Life. Obesity 2010, 18, 1801–1804. [Google Scholar] [CrossRef] [PubMed]
- Lanoye, A.; Brown, K.L.; LaRose, J.G. The Transition into Young Adulthood: A Critical Period for Weight Control. Curr. Diabetes Rep. 2017, 17, 114. [Google Scholar] [CrossRef] [PubMed]
- Melchior, M.; Chollet, A.; Fombonne, E.; Surkan, P.J.; Dray-Spira, R. Internet and Video Game Use in Relation to Overweight in Young Adults. Am. J. Health Promot. 2014, 28, 321–324. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K.; Chirwa, G.C.; Pemba, L.A.; Qattan, A.M.N. Does prolonged television viewing affect Body Mass Index? A case of the Kingdom of Saudi Arabia. PLoS ONE 2020, 15, e0228321. [Google Scholar] [CrossRef] [Green Version]
- Syed, N.K.; Syed, M.H.; Meraya, A.M.; Albarraq, A.A.; Al-kasim, M.A.; Alqahtani, S.; Makeen, H.A.; Yasmeen, A.; Banji, O.J.F.; Elnaem, M.H. The association of dietary behaviors and practices with overweight and obesity parameters among Saudi university students. PLoS ONE 2020, 15, e0238458. [Google Scholar] [CrossRef]
- Lazarevich, I.; Irigoyen-Camacho, M.E.; del Consuelo Velázquez-Alva, M.; Zepeda, M.Z. Relationship among obesity, depression, and emotional eating in young adults. Appetite 2016, 107, 639–644. [Google Scholar] [CrossRef]
- Cheng, H.L.; Medlow, S.; Steinbeck, K. The Health Consequences of Obesity in Young Adulthood. Curr. Obes. Rep. 2016, 5, 30–37. [Google Scholar] [CrossRef]
- Allman-Farinelli, M.A. Nutrition Promotion to Prevent Obesity in Young Adults. Healthcare 2015, 3, 809–821. [Google Scholar] [CrossRef] [Green Version]
- Poobalan, A.; Aucott, L. Obesity Among Young Adults in Developing Countries: A Systematic Overview. Curr. Obes. Rep. 2016, 5, 2–13. [Google Scholar] [CrossRef] [Green Version]
- DeNicola, E.; Aburizaiza, O.S.; Siddique, A.; Khwaja, H.; Carpenter, D.O. Obesity and public health in the Kingdom of Saudi Arabia. Rev. Environ. Health 2015, 30, 191–205. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; El Bcheraoui, C.; Tuffaha, M.; Robinson, M.; Daoud, F.; Jaber, S.; Mikhitarian, S.; Al Saeedi, M.; AlMazroa, M.A.; Mokdad, A.H.; et al. Obesity and Associated Factors—Kingdom of Saudi Arabia, 2013. Prev. Chronic Dis. 2014, 11, E174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Rethaiaa, A.S.; Fahmy AE, A.; Al-Shwaiyat, N.M. Obesity and eating habits among college students in Saudi Arabia: A cross sectional study. Nutr. J. 2010, 9, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ALFaris, N.A.; Al-Tamimi, J.Z.; Al-Jobair, M.O.; Al-Shwaiyat, N.M. Trends of fast food consumption among adolescent and young adult Saudi girls living in Riyadh. Food Nutr. Res. 2015, 59, 26488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlQuaiz, A.; Kazi, A.; Almigbal, T.; AlHazmi, A.; Qureshi, R.; AlHabeeb, K. Factors Associated with an Unhealthy Lifestyle among Adults in Riyadh City, Saudi Arabia. Healthcare 2021, 9, 221. [Google Scholar] [CrossRef]
- De Bel-Air, F. Demography, migration and labour market in Saudi Arabia. Gulf Labour Markets and Migration. European University Institute (EUI) and Gulf Research Center (GRC). GLMM-EN-No. 1/2014. 2014. Available online: https://cadmus.eui.eu/bitstream/handle/1814/32151/GLMM%20ExpNote_01-2014.pdf (accessed on 15 January 2022).
- General Authority of Statistics of Saudi Arabia. Population by Gender, Age Groups and Nationality (Saudi/Non-Saudi), The Fifth Saudi Census, 2010. Available online: https://www.stats.gov.sa/sites/default/files/ar-census2010-dtl-result_2_1.pdf (accessed on 15 January 2022).
- World Health Organization (WHO). Obesity and Overweight; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- AlTamimi, J.Z.; Alshwaiyat, N.M.; AlFaris, N.A.; AlKehayez, N.M.; Ahmad, A.; Alagal, R.I. Differences in Overweight and Obesity Prevalence in Middle-Aged Men from Twelve Middle Eastern and Asian Countries Living in Saudi Arabia. Int. J. Gen. Med. 2022, 15, 3333–3343. [Google Scholar] [CrossRef]
- Althumiri, N.A.; Basyouni, M.H.; AlMousa, N.; AlJuwaysim, M.F.; Almubark, R.A.; BinDhim, N.F.; Alkhamaali, Z.; Alqahtani, S.A. Obesity in Saudi Arabia in 2020: Prevalence, Distribution, and Its Current Association with Various Health Conditions. Healthcare 2021, 9, 311. [Google Scholar] [CrossRef]
- Wang, L.; Southerland, J.; Wang, K.; Bailey, B.A.; Alamian, A.; Stevens, M.A.; Wang, Y. Ethnic Differences in Risk Factors for Obesity among Adults in California, the United States. J. Obes. 2017, 2017, 2427483. [Google Scholar] [CrossRef] [Green Version]
- Higgins, V.; Nazroo, J.; Brown, M. Pathways to ethnic differences in obesity: The role of migration, culture and socio-economic position in the UK. SSM—Popul. Health 2019, 7, 10039. [Google Scholar]
- AlTamimi, J.Z.; Alshwaiyat, N.M.; Alkhalidy, H.; AlFaris, N.A.; AlKehayez, N.M.; Alagal, R.I. Breakfast Skipping among a Multi-Ethnic Population of Young Men and Relationship with Sociodemographic Determinants and Weight Status. Int. J. Environ. Res. Public Health 2022, 19, 2903. [Google Scholar] [CrossRef]
- AlFaris, N.A.; Alshwaiyat, N.M.; Alkhalidy, H.; Alagal, R.I.; AlTamimi, J.Z.; AlKehayez, N.M. Breakfast Skipping in a Multi-Ethnic Population of Middle-Aged Men and Relationship With Sociodemographic Variables and Weight Status. Front. Nutr. 2022, 8, 761383. [Google Scholar] [CrossRef] [PubMed]
- AlTamimi, J.Z.; Alagal, R.I.; AlKehayez, N.M.; Alshwaiyat, N.M.; Al-Jamal, H.A.; AlFaris, N.A. Physical Activity Levels of a Multi-Ethnic Population of Young Men Living in Saudi Arabia and Factors Associated With Physical Inactivity. Front. Public Health 2022, 9, 734968. [Google Scholar] [CrossRef] [PubMed]
- AlFaris, N.A.; Alshwaiyat, N.M.; AlTamimi, J.Z.; Alagal, R.I.; Al-Jamal, H.A.; AlKehayez, N.M. Physical Activity Levels of a Multi-Ethnic Population of Middle-Aged Men Living in Saudi Arabia and Factors Associated With Physical Inactivity. Int. J. Public Health 2022, 66, 1604328. [Google Scholar] [CrossRef] [PubMed]
- Moradi-Lakeh, M.; El Bcheraoui, C.; Afshin, A.; Daoud, F.; AlMazroa, M.A.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; Al Rabeeah, A.A.; Mokdad, A.H. Diet in Saudi Arabia: Findings from a nationally representative survey. Public Health Nutr. 2017, 20, 1075–1081. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Kishore, A.; Roy, D.; Joshi, K. A comparison of the Indian diet with the EAT-Lancet reference diet. BMC Public Health 2020, 20, 812. [Google Scholar] [CrossRef]
- Zaman, M.M.; Rahman, M.; Rahman, R.; Bhuiyan, M.R.; Karim, N.; Chowdhury, A.J. Prevalence of risk factors for non-communicable diseases in Bangladesh: Results from STEPS survey 2010. Indian J. Public Health 2016, 60, 17–25. [Google Scholar] [CrossRef]
- WHO. Global Strategy on Diet, Physical Activity and Health; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- WHO. Global Status Report on Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Caspersen, C.J.; Pereira, M.A.; Curran, K.M. Changes in physical activity patterns in the United States, by sex and cross-sectional age. Med. Sci. Sports Exerc. 2000, 32, 1601–1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzeidan, R.A.; Rabiee, F.; Mandil, A.A.; Hersi, A.S.; Ullah, A.A. Changes in dietary habits and physical activity and status of metabolic syndrome among expatriates in Saudi Arabia. East. Mediterr. Health J. 2017, 23, 836–844. [Google Scholar] [CrossRef]
- Lassetter, J.H.; Callister, L.C. The impact of migration on the health of voluntary migrants in western societies: A review of the literature. J. Transcult. Nurs. 2009, 20, 93–104. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Frequencies/Means | %/SD |
|---|---|---|
| Participants’ Nationality | ||
| Saudi | 289 | 8.0% |
| Egyptian | 289 | 8.0% |
| Yemeni | 335 | 9.3% |
| Syrian | 293 | 8.1% |
| Jordanian | 280 | 7.8% |
| Sudanese | 276 | 7.7% |
| Turkish | 203 | 5.6% |
| Pakistani | 306 | 8.5% |
| Afghan | 303 | 8.4% |
| Indian | 297 | 8.3% |
| Bangladeshi | 350 | 9.7% |
| Filipino | 379 | 10.5% |
| Age (years) | 29.6 | 3.2 |
| Residency Duration (years) | 7.2 | 7.0 |
| Household Type | ||
| Non-family household | 2920 | 81.1% |
| Family household | 680 | 18.9% |
| Marital Status | ||
| Single | 1919 | 53.3% |
| Married | 1681 | 46.7% |
| Educational Level | ||
| Low (secondary school or less) | 2284 | 63.4% |
| High (college degree or more) | 1316 | 36.6% |
| Monthly Income | ||
| Low (˂USD 1000) | 2630 | 73.1% |
| High (≥USD 1000) | 970 | 26.9% |
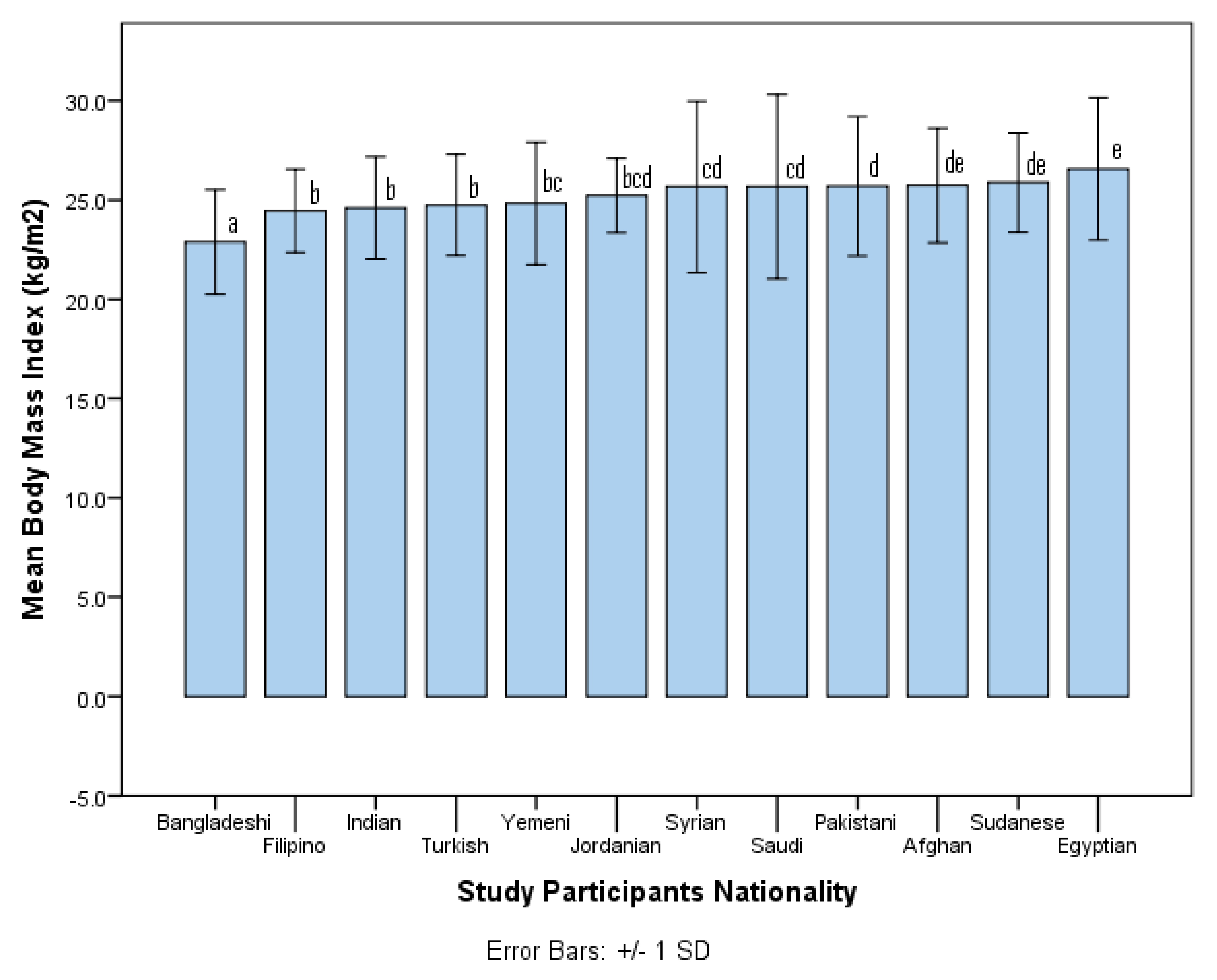
| Body Mass Index (kg/m2) | 25.1 | 3.2 |
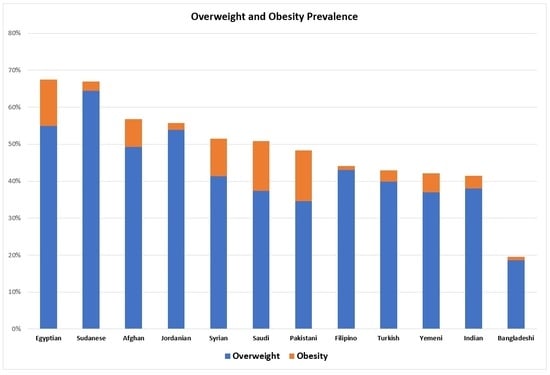
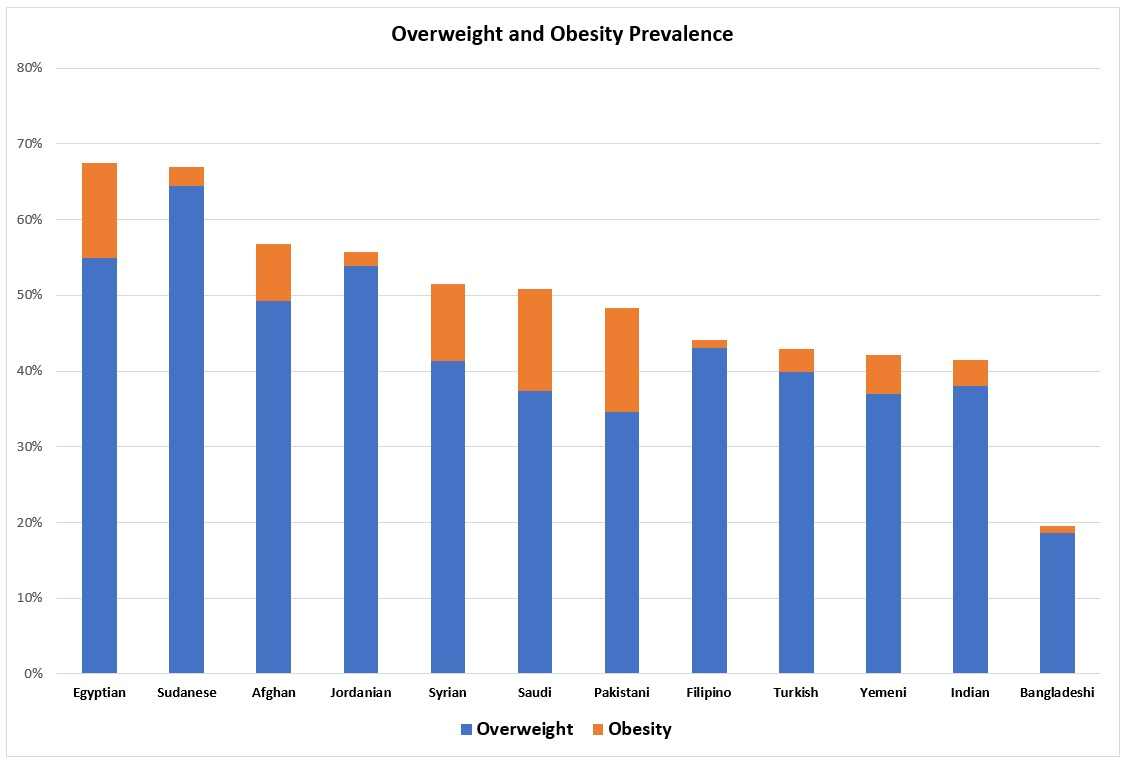
| Study Participants | n (%) | Body Weight Status * | |||
|---|---|---|---|---|---|
| Underweight | Normal | Overweight | Obesity | ||
| All | 3600 (100%) | 31 (0.9%) | 1829 (50.8%) | 1518 (42.2%) | 222 (6.2%) |
| Saudi | 289 (8.0%) | 7 (2.4%) | 135 (46.7%) | 108 (37.4%) | 39 (13.5%) |
| Egyptian | 289 (8.0%) | 0 (0.0%) | 94 (32.5%) | 159 (55.0%) | 36 (12.5%) |
| Yemeni | 335 (9.3%) | 0 (0.0%) | 194 (57.9%) | 124 (37.0%) | 17 (5.1%) |
| Syrian | 293 (8.1%) | 4 (1.4%) | 138 (47.1%) | 121 (41.3%) | 30 (10.2%) |
| Jordanian | 280 (7.8%) | 0 (0.0%) | 124 (44.3%) | 151 (53.9%) | 5 (1.8%) |
| Sudanese | 276 (7.7%) | 1 (0.4%) | 90 (32.6%) | 178 (64.5%) | 7 (2.5%) |
| Turkish | 203 (5.6%) | 0 (0.0%) | 116 (57.1%) | 81 (39.9%) | 6 (3.0%) |
| Pakistani | 306 (8.5%) | 1 (0.3%) | 157 (51.3%) | 106 (34.6%) | 42 (13.7%) |
| Afghan | 303 (8.4%) | 0 (0.0%) | 131 (43.2%) | 149 (49.2%) | 23 (7.6%) |
| Indian | 297 (8.3%) | 1 (0.3%) | 173 (58.2%) | 113 (38.0%) | 10 (3.4%) |
| Bangladeshi | 350 (9.7%) | 16 (4.6%) | 266 (76.0%) | 65 (18.6%) | 3 (0.9%) |
| Filipino | 379 (10.5%) | 1 (0.3%) | 211 (55.7%) | 163 (43.0%) | 4 (1.1%) |
| Study Participants by Nationality | Saudi | Egyptian | Yemeni | Syrian | Jordanian | Sudanese | Turkish | Pakistani | Afghan | Indian | Bangladeshi |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Saudi | 1.000 * 1.000 ** | ||||||||||
| Egyptian | 0.001 0.001 | 1.000 1.000 | |||||||||
| Yemeni | 0.001 0.028 | 0.001 0.001 | 1.000 1.000 | ||||||||
| Syrian | 0.434 0.871 | 0.001 0.001 | 0.002 0.018 | 1.000 1.000 | |||||||
| Jordanian | 0.001 0.246 | 0.001 0.004 | 0.001 0.001 | 0.001 0.316 | 1.000 1.000 | ||||||
| Sudanese | 0.001 0.001 | 0.001 0.910 | 0.001 0.001 | 0.001 0.001 | 0.030 0.006 | 1.000 1.000 | |||||
| Turkish | 0.001 0.080 | 0.001 0.001 | 0.446 0.861 | 0.003 0.057 | 0.009 0.005 | 0.001 0.001 | 1.000 1.000 | ||||
| Pakistani | 0.121 0.542 | 0.001 0.001 | 0.001 0.111 | 0.125 0.438 | 0.001 0.075 | 0.001 0.001 | 0.001 0.222 | 1.000 1.000 | |||
| Afghan | 0.001 0.150 | 0.011 0.007 | 0.001 0.001 | 0.049 0.200 | 0.004 0.798 | 0.001 0.011 | 0.003 0.002 | 0.001 0.038 | 1.000 1.000 | ||
| Indian | 0.001 0.022 | 0.001 0.001 | 0.522 0.864 | 0.001 0.014 | 0.001 0.001 | 0.001 0.001 | 0.830 0.748 | 0.001 0.086 | 0.001 0.001 | 1.000 1.000 | |
| Bangladeshi | 0.001 0.001 | 0.001 0.001 | 0.001 0.001 | 0.001 0.001 | 0.001 0.001 | 0.001 0.001 | 0.001 0.001 | 0.001 0.001 | 0.001 0.001 | 0.001 0.001 | 1.000 1.000 |
| Filipino | 0.001 0.081 | 0.001 0.001 | 0.006 0.595 | 0.001 0.054 | 0.023 0.003 | 0.001 0.001 | 0.300 0.780 | 0.001 0.261 | 0.001 0.001 | 0.137 0.490 | 0.001 0.001 |
| Variables | Unadjusted Odds Ratio * | 95% CI | p Value | Adjusted Odds Ratio ** | 95% CI | p Value |
|---|---|---|---|---|---|---|
| Participants’ Nationality | ||||||
| Bangladeshi | 1.00 | 1.00 | ||||
| Saudi | 4.29 | 3.02–6.10 | ˂0.001 | 3.90 | 2.54–5.98 | ˂0.001 |
| Egyptian | 8.60 | 5.99–12.35 | ˂0.001 | 7.37 | 4.98–10.90 | ˂0.001 |
| Yemeni | 3.01 | 2.14–4.24 | ˂0.001 | 2.76 | 1.92–3.96 | ˂0.001 |
| Syrian | 4.41 | 3.11–6.26 | ˂0.001 | 3.72 | 2.50–5.53 | ˂0.001 |
| Jordanian | 5.22 | 3.66–7.44 | ˂0.001 | 4.15 | 2.78–6.20 | ˂0.001 |
| Sudanese | 8.43 | 5.85–12.14 | ˂0.001 | 7.59 | 5.24–10.98 | ˂0.001 |
| Turkish | 3.11 | 2.12–4.57 | ˂0.001 | 2.43 | 1.63–3.61 | ˂0.001 |
| Pakistani | 3.89 | 2.75–5.50 | ˂0.001 | 3.82 | 2.68–5.44 | ˂0.001 |
| Afghan | 5.45 | 3.84–7.72 | ˂0.001 | 5.42 | 3.80–7.73 | ˂0.001 |
| Indian | 2.93 | 2.06–4.17 | ˂0.001 | 2.85 | 1.99–4.07 | ˂0.001 |
| Filipino | 3.27 | 2.34–4.56 | ˂0.001 | 3.22 | 2.21–4.68 | ˂0.001 |
| Age (years) | 1.10 | 1.08–1.12 | ˂0.001 | 1.07 | 1.04–1.10 | ˂0.001 |
| Residency Duration (years) | 1.02 | 1.01–1.03 | ˂0.001 | 1.05 | 1.03–1.08 | ˂0.001 |
| Household Type | ||||||
| Non-family household | 1.00 | 1.00 | ||||
| Family household | 1.40 | 1.18–1.66 | ˂0.001 | 0.87 | 0.69–1.11 | 0.262 |
| Marital Status | ||||||
| Single | 1.00 | 1.00 | ||||
| Married | 1.32 | 1.16–1.50 | ˂0.001 | 1.04 | 0.87–1.23 | 0.689 |
| Educational Level | ||||||
| Low (secondary school or less) | 1.00 | 1.00 | ||||
| High (college degree or more) | 1.53 | 1.34–1.76 | ˂0.001 | 1.22 | 0.99–1.51 | 0.061 |
| Monthly Income | ||||||
| Low (˂USD 1000) | 1.00 | 1.00 | ||||
| High (≥USD 1000) | 1.57 | 1.35–1.82 | ˂0.001 | 1.21 | 0.99–1.48 | 0.067 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alagal, R.I.; AlFaris, N.A.; AlTamimi, J.Z.; Alshwaiyat, N.M.; Ahmad, A.; Alzaheb, R.A.; AlKehayez, N.M. Differences in Overweight and Obesity Prevalence among Young Men from Twelve Middle Eastern and Asian Countries Living in Saudi Arabia. Healthcare 2022, 10, 690. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10040690
Alagal RI, AlFaris NA, AlTamimi JZ, Alshwaiyat NM, Ahmad A, Alzaheb RA, AlKehayez NM. Differences in Overweight and Obesity Prevalence among Young Men from Twelve Middle Eastern and Asian Countries Living in Saudi Arabia. Healthcare. 2022; 10(4):690. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10040690
Chicago/Turabian StyleAlagal, Reham I., Nora A. AlFaris, Jozaa Z. AlTamimi, Naseem M. Alshwaiyat, Aryati Ahmad, Riyadh A. Alzaheb, and Nora M. AlKehayez. 2022. "Differences in Overweight and Obesity Prevalence among Young Men from Twelve Middle Eastern and Asian Countries Living in Saudi Arabia" Healthcare 10, no. 4: 690. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10040690