
What Are the Complications, Success and Survival Rates for Autotransplanted Teeth? An Overview of Systematic Reviews and Metanalyses

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Review Selection
2.3. Data Extraction
2.4. Analysis of Methodological Quality
3. Results
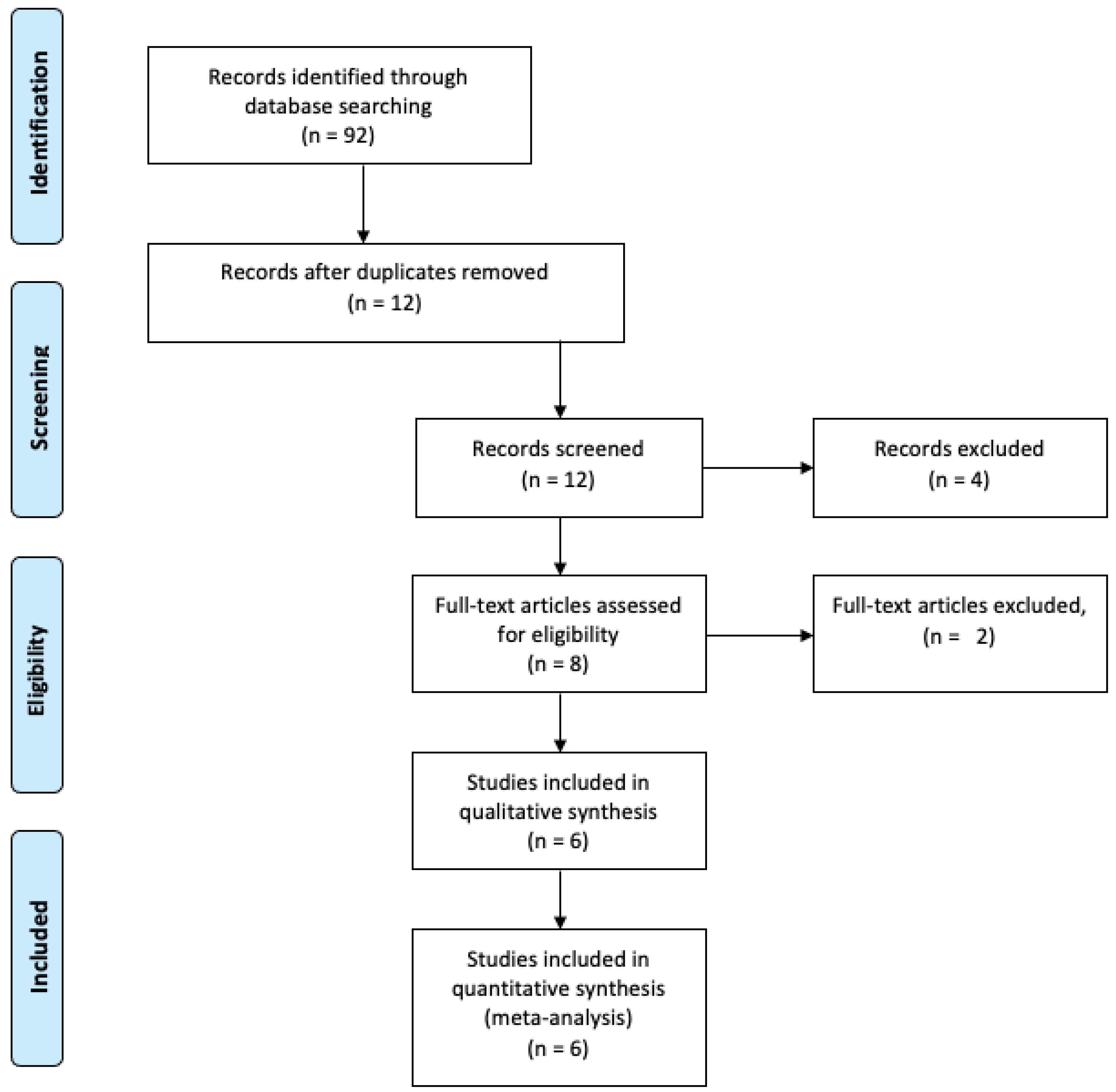
3.1. Search Results and Review Selection
3.2. Study Characteristics
3.3. Analysis of Methodological Quality
3.4. Success and Failure Rate
3.5. Ankylosis Rate
3.6. Infection-Related Root Resorption Rate
3.7. Other Reported Outcomes
3.8. Subgroup Analysis Based on Factors Could Potentially Mediate the Prognosis of ATT
3.9. Publication Bias
3.10. Analysis of Primary Studies Overlap in the Reviews
4. Discussion
4.1. Limitations and Strengths of This Overview
4.2. Implications for Practice and Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parvini, P.; Obreja, K.; Trimpou, G.; Mahmud, S.; Sader, R. Autotransplantation of teeth. Int. J. Esthet. Dent. 2018, 13, 274–282. [Google Scholar]
- Park, J.H.; Tai, K.; Hayashi, D. Tooth Autotransplantation as a Treatment Option: A Review. J. Clin. Pediatr. Dent. 2010, 35, 129–135. [Google Scholar] [CrossRef]
- Amos, M.J.; Day, P.F.; Littlewood, S.J. Autotransplantation of Teeth: An Overview. Dent. Update 2009, 36, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.K.; Cleverly, D.G. Tooth autotransplantation: An overview and case study. Northwest Dent. 2012, 91, 29–33. [Google Scholar]
- Thomas, S.; Turner, S.R.; Sandy, J.R. Autotransplantation of Teeth: Is There a Role? Br. J. Orthod. 1998, 25, 275–282. [Google Scholar] [CrossRef]
- Schwartz, O.; Bergmann, P.; Klausen, B. Autotransplantation of human teeth. A life-table analysis of prognostic factors. Int. J. Oral Surg. 1985, 14, 245–258. [Google Scholar] [CrossRef]
- Fernandes, S.; Habibullah, M.A.; Nalam, G.S.; Nair, P.P. Think before you extract—A case of tooth autotransplantation. BMJ Case Rep. 2011, 2011. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Gimbernat, D.; Recio-Lora, C.; Torres-Lagares, D.; Romero-Ruiz, M.; Pérez, J.L.G. Current state of dental autotransplantation. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e948–e952. [Google Scholar] [CrossRef] [Green Version]
- Cross, D.; El-Angbawi, A.; McLaughlin, P.; Keightley, A.; Brocklebank, L.; Whitters, J.; McKerlie, R.; Cross, L.; Welbury, R. Developments in autotransplantation of teeth. J. Surg. 2013, 11, 49–55. [Google Scholar] [CrossRef]
- Plotino, G.; Sans, F.A.; Duggal, M.S.; Grande, N.M.; Krastl, G.; Nagendrababu, V.; Gambarini, G. European Society of Endodontology position statement: Surgical extrusion, intentional replantation and tooth autotransplantation: European Society of Endo-dontology developed by. Int. Endod. J. 2021, 54, 655–659. [Google Scholar] [CrossRef]
- Tsukiboshi, M. Autotransplantation of teeth: Requirements for predictable success. Dent. Traumatol. 2002, 18, 157–180. [Google Scholar] [CrossRef]
- Tsukiboshi, M.; Yamauchi, N.; Tsukiboshi, Y. Long-term outcomes of autotransplantation of teeth: A case series. Dent. Traumatol. 2019, 35, 358–367. [Google Scholar] [CrossRef] [Green Version]
- De Freitas Coutinho, N.B.; Nunes, F.C.; Intra, J.B.G.; Roldi, A.; de Jesus-Soares, A.; Coelho, M.S.; Frozoni, M. Success, Survival Rate, and Soft Tissue Esthetic of Tooth Autotransplantation. J. Endod. 2021, 47, 391–396. [Google Scholar] [CrossRef]
- Raabe, C.; Bornstein, M.M.; Ducommun, J.; Sendi, P.; von Arx, T.; Janner, S.F.M. A retrospective analysis of autotransplanted teeth including an evaluation of a novel surgical technique. Clin. Oral Investig. 2021, 25, 3513–3525. [Google Scholar] [CrossRef]
- Mertens, B.; Boukari, A.; Tenenbaum, H. Long-term follow up of post-surgical tooth autotransplantation: A retrospective study. J. Investig. Clin. Dent. 2014, 7, 207–214. [Google Scholar] [CrossRef]
- Ong, D.C.; Itskovich, Y.; Dance, G. Autotransplantation: A viable treatment option for adolescent patients with significantly compromised teeth. Aust. Dent. J. 2016, 61, 396–407. [Google Scholar] [CrossRef] [Green Version]
- Nagori, S.A.; Bhutia, O.; Roychoudhury, A.; Pandey, R.M. Immediate autotransplantation of third molars: An experience of 57 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 400–407. [Google Scholar] [CrossRef]
- Boschini, L.; Melillo, M.; Berton, F. Long term survival of mature autotransplanted teeth: A retrospective single center analysis. J. Dent. 2020, 98, 103371. [Google Scholar] [CrossRef]
- Juslin, J.; Jääsaari, P.; Teerijoki-Oksa, T.; Suominen, A.; Thorén, H. Survival of Autotransplanted Teeth with Open Apices: A Retrospective Cohort Study. J. Oral Maxillofac. Surg. 2020, 78, 902.e1–902.e9. [Google Scholar] [CrossRef]
- Ashurko, I.; Vlasova, I.; Yaremchuk, P.; Bystrova, O. Autotransplantation of teeth as an alternative to dental implantation. BMJ Case Rep. 2020, 13, e234889. [Google Scholar] [CrossRef]
- Yang, S.; Jung, B.-Y.; Pang, N.-S. Outcomes of autotransplanted teeth and prognostic factors: A 10-year retrospective study. Clin. Oral Investig. 2018, 23, 87–98. [Google Scholar] [CrossRef]
- Abela, S.; Murtadha, L.; Bister, D.; Andiappan, M.; Kwok, J. Survival probability of dental autotransplantation of 366 teeth over 34 years within a hospital setting in the United Kingdom. Eur. J. Orthod. 2019, 41, 551–556. [Google Scholar] [CrossRef]
- van Westerveld, K.; Verweij, J.; Toxopeus, E.; Fiocco, M.; Mensink, G.; van Merkesteyn, J. Long-term outcomes 1–20 years after autotransplantation of teeth: Clinical and radiographic evaluation of 66 premolars and 8 molars. Br. J. Oral Maxillofac. Surg. 2019, 57, 666–671. [Google Scholar] [CrossRef]
- Armstrong, L.; O’reilly, C.; Ahmed, B. Autotransplantation of third molars: A literature review and preliminary protocols. Br. Dent. J. 2020, 228, 247–251. [Google Scholar] [CrossRef]
- Czochrowska, E.M.; Plakwicz, P. Autotransplantation and healing. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 299–300. [Google Scholar] [CrossRef]
- Czochrowska, E.M. “Off the beaten track” solutions: Autotransplantation of teeth. Int. J. Esthet. Dent. 2018, 13, 234–239. [Google Scholar]
- Martin, K.; Nathwani, S.; Bunyan, R. Autotransplantation of teeth: An evidence-based approach. Br. Dent. J. 2018, 224, 861–864. [Google Scholar] [CrossRef]
- Verweij, J.; Anssari Moin, D.; Mensink, G.; Wismeijer, D.; van Merkesteyn, J.P.R. Autotransplantation 2.0. Considerations, results and the latest techniques. Ned. Tijdschr. Voor Tandheelkd. 2016, 123, 348–353. [Google Scholar] [CrossRef]
- Almpani, K.; Papageorgiou, S.N.; Papadopoulos, M.A. Autotransplantation of teeth in humans: A systematic review and meta-analysis. Clin. Oral Investig. 2015, 19, 1157–1179. [Google Scholar] [CrossRef]
- Machado, L.; Nascimento, R.D.; Ferreira, D.; Mattos, C.; Vilella, O. Long-term prognosis of tooth autotransplantation: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 610–617. [Google Scholar] [CrossRef]
- Atala-Acevedo, C.; Abarca, J.; Martínez-Zapata, M.J.; Díaz, J.; Olate, S.; Zaror, C. Success Rate of Autotransplantation of Teeth with an Open Apex: Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2017, 75, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Rohof, E.C.M.; Kerdijk, W.; Jansma, J.; Livas, C.; Ren, Y. Autotransplantation of teeth with incomplete root formation: A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 1613–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, W.-C.; Tu, Y.-K.; Lin, Y.-H.; Lu, H.-K. Outcomes of autotransplanted teeth with complete root formation: A systematic review and meta-analysis. J. Clin. Periodontol. 2014, 41, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Akhlef, Y.; Schwartz, O.; Andreasen, J.O.; Jensen, S.S. Autotransplantation of teeth to the anterior maxilla: A systematic review of survival and success, aesthetic presentation and patient-reported outcome. Dent. Traumatol. 2017, 34, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.; Savović, J.; Higgins, J.P.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Lunny, C.; Pieper, D.; Thabet, P.; Kanji, S. Managing overlap of primary study results across systematic reviews: Practical considerations for authors of overviews of reviews. BMC Med. Res. Methodol. 2021, 21, 140. [Google Scholar] [CrossRef]
- Hennessy, E.A.; Blair, T.J. Examining overlap of included studies in meta-reviews: Guidance for using the corrected covered area index. Res. Synth. Methods 2020, 11, 134–145. [Google Scholar] [CrossRef]
- Kallu, R.; Vinckier, F.; Politis, C.; Mwalili, S.; Willems, G. Tooth transplantations: A descriptive retrospective study. Int. J. Oral Maxillofac. Surg. 2005, 34, 745–755. [Google Scholar] [CrossRef]
- Mendes, R.A.; Rocha, G. Mandibular third molar autotransplantation—literature review with clinical cases. J. Can. Dent. Assoc. 2004, 70, 761–766. [Google Scholar]
- Abu Tair, J.A.; Rahhal, A. Tooth autotransplantation in orthodontic patients. J. Contemp. Dent. Pract. 2010, 11, 63–70. [Google Scholar] [CrossRef]
- Kvint, S.; Lindsten, R.; Magnusson, A.; Nilsson, P.; Bjerklin, K. Autotransplantation of Teeth in 215 Patients. A follow-up study. Angle Orthod. 2010, 80, 446–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshino, K.; Kariya, N.; Namura, D.; Noji, I.; Mitsuhashi, K.; Kimura, H.; Fukuda, A.; Kikukawa, I.; Hayashi, T.; Yamazaki, N.; et al. Influence of age on tooth autotransplantation with complete root formation. J. Oral Rehabil. 2013, 40, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Gilijamse, M.; Baart, J.A.; Wolff, J.; Sándor, G.K.; Forouzanfar, T. Tooth autotransplantation in the anterior maxilla and mandible: Retrospective results in young patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, e187–e192. [Google Scholar] [CrossRef] [PubMed]
- Ong, D.C.; Dance, G. Posterior tooth autotransplantation: A case series. Aust. Dent. J. 2021, 66, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Moin, D.A.; Derksen, W.; Verweij, J.; van Merkesteyn, R.; Wismeijer, D. A Novel Approach for Computer-Assisted Template-Guided Autotransplantation of Teeth with Custom 3D Designed/Printed Surgical Tooling. An Ex Vivo Proof of Concept. J. Oral Maxillofac. Surg. 2016, 74, 895–902. [Google Scholar] [CrossRef]
- Verweij, J.; Anssari Moin, D.; Mensink, G.; Wismeijer, D.; van Merkesteyn, J.P.R. Replacing heavily damaged molars with the use of 3D-techniques. Ned. Tijdschr. Voor Tandheelkd. 2018, 125, 21–26. [Google Scholar] [CrossRef]
- Dreizin, D.; Nam, A.J.; Hirsch, J.; Bernstein, M. New and emerging patient-centered CT imaging and image-guided treatment paradigms for maxillofacial trauma. Emerg. Radiol. 2018, 25, 533–545. [Google Scholar] [CrossRef]
- Al-Rimawi, A.; Ezeldeen, M.; Schneider, D.; Politis, C.; Jacobs, R. 3D Printed Temporary Veneer Restoring Autotransplanted Teeth in Children: Design and Concept Validation Ex Vivo. Int. J. Environ. Res. Public Health 2019, 16, 496. [Google Scholar] [CrossRef] [Green Version]
- Kamio, T.; Kato, H. Autotransplantation of Impacted Third Molar Using 3D Printing Technology: A Case Report. Bull. Tokyo Dent. Coll. 2019, 60, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Curtis, J.M.T.; Foster, E.C.; Ananth, S.; Eckhardt, C.; Knox, J.; Alvarez, A.G.; Newton, R. Autotransplantation of a surgically removed canine using a customised 3D-printed surgical template. J. Orthod. 2020, 47, 82–90. [Google Scholar] [CrossRef]
- Cousley, R.R.J.; Gibbons, A.; Nayler, J. A 3D printed surgical analogue to reduce donor tooth trauma during autotransplantation. J. Orthod. 2017, 44, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Sokolowski, A.A.; Sokolowski, A.A.; Kammerhofer, J.; Madreiter-Sokolowski, C.T.; Payer, M.; Koller, M.; Jakse, N.; Wegscheider, A. Accuracy assess-ment of 3D-printed tooth replicas. Int. J. Comput. Dent. 2019, 22, 321–329. [Google Scholar] [PubMed]
- Kim, K.; Choi, H.; Pang, N. Clinical application of 3D technology for tooth autotransplantation: A case report. Aust. Endod. J. 2019, 45, 122–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahbazian, M.; Jacobs, R.; Wyatt, J.; Willems, G.; Pattijn, V.; Dhoore, E.; van Lierde, C.; Vinckier, F. Accuracy and surgical feasibility of a CBCT-based stereolithographic surgical guide aiding autotransplantation of teeth: In vitro validation. J. Oral Rehabil. 2010, 37, 854–859. [Google Scholar] [CrossRef]
- Ezeldeen, M.; Wyatt, J.; Al-Rimawi, A.; Coucke, W.; Shaheen, E.; Lambrichts, I.; Willems, G.; Politis, C.; Jacobs, R. Use of CBCT Guidance for Tooth Autotransplantation in Children. J. Dent. Res. 2019, 98, 406–413. [Google Scholar] [CrossRef]
- Chen, J.-M.; Wu, Y.; He, P.-T.; Xie, F.-P.; Liu, H.-H.; Lin, L.-S. Application of computer virtual design to assist the accuracy of sock-et preparation during tooth autotransplantation. Shanghai Kou Qiang Yi Xue 2020, 29, 65–68. [Google Scholar]
- Yu, H.; Jia, P.; Lv, Z.; Qiu, L. Autotransplantation of third molars with completely formed roots into surgically created sockets and fresh extraction sockets: A 10-year comparative study. Int. J. Oral Maxillofac. Surg. 2017, 46, 531–538. [Google Scholar] [CrossRef]
- Ahlberg, K.; Bystedt, H.; Eliasson, S.; Odenrick, L. Long-Term Evaluation of Autotransplanted Maxillary Canines with Completed Root Formation. Acta Odontol. Scand. 1983, 41, 23–31. [Google Scholar] [CrossRef]
- Herrera, H.; Herrera, H.; Leonardo, M.R.; Paula-Silva, F.W.; da Silva, L.A.B. Treatment of external inflammatory root resorption after autogenous tooth transplantation: Case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, e51–e54. [Google Scholar] [CrossRef]
- Andreasen, J. Periodontal healing after replantation and autotransplantation of incisors in monkeys. Int. J. Oral Surg. 1981, 10, 54–61. [Google Scholar] [CrossRef]


{kind=link}
| Query | Filters | Search Details | Results |
|---|---|---|---|
| (teeth OR tooth) AND (((autotransplant) OR (autotransplant *)) OR (autotransplantation)) | Systematic Review | ((“teeth s”[All Fields] OR “teeths”[All Fields] OR “tooth”[MeSH Terms] OR “tooth”[All Fields] OR “teeth”[All Fields] OR “tooth s”[All Fields] OR “tooths”[All Fields] OR (“teeth s”[All Fields] OR “teeths”[All Fields] OR “tooth”[MeSH Terms] OR “tooth”[All Fields] OR “teeth”[All Fields] OR “tooth s”[All Fields] OR “tooths”[All Fields])) AND (“autografts”[MeSH Terms] OR “autografts”[All Fields] OR “autotransplant”[All Fields] OR “autotransplants”[All Fields] OR “autotransplanted”[All Fields] OR “autotransplanting”[All Fields] OR “autotransplant *”[All Fields] OR (“autotransplantion”[All Fields] OR “transplantation, autologous”[MeSH Terms] OR (“transplantation”[All Fields] AND “autologous”[All Fields]) OR “autologous transplantation”[All Fields] OR “autotransplantation”[All Fields] OR “autotransplantations”[All Fields]))) AND (systematicreview[Filter]) | 28 |
| Author and Year Published | Country of Study | Study Design | Database Search | Language and Time Period Restriction | Included Study Character |
|---|---|---|---|---|---|
| Chung et al., 2014 [33] | Taiwan | SR and MA | PubMed, Google Scholar, Scopus | Language: English Date; between 1771 and 28 February 2013 | a sample size of at least 10 permanent transplanted teeth. complete root formation and a closed apical foramen. at least a 1-year follow-up period |
| Almpani et al., 2015 [29] | Germany | SR and MA | MEDLINE, LILACS, Scopus, Ovid database, BioMed Central, ProQuest, Cochrane Library, African Journals Online, Lippincott Williams and Wilkins (LWW), Bibliografia Brasileira de Odontologia, Google Scholar Beta, Wiley Online Library, Elsevier Book Series and Health Sciences | Language: No restriction Date: up to November 2012 | studies providing information regarding the success/survival rate of autologous transplantation of teeth in the short- or/and long-term |
| Machado et al., 2015 [30] | Brazil | SR and MA | PubMed, Scopus, Web of Science, Lilacs, and The Cochrane Library | Language: No restriction Date: (1 January 1990 to 7 July 2014). | studies reporting at least one of the following: survival rate, pulp condition, mobility, presence of ankylosis, and root resorption of autotransplanted teeth with complete or incomplete root formation. Follwup >6 years. |
| Akhlef et al., 2016 [34] | Denmark | SR and MA | PubMed | Language: English Date: NR | Autotransplantation to the anterior maxilla. Studies including ≥10 teeth. |
| Atala et al., 2017 [31] | Chile, Spain | SR and MA | MEDLINE, EMBASE, LILACS, SciELO | Language-English, Spanish, Portuguese Date: January 1997 to August 2015 | open apex with or without preparation of the socket. a minimum follow-up period of 12 months. |
| C.M. Rohof et al., 2018 [32] | Netherland | SR and MA | PubMed, EMBASE, Web of Science, Cochrane Library | Language-English Date: all data published until July 2016 | involving 5 or more participants and at least 10 permanent transplanted teeth. incomplete root formation Open apex reported or deducible success rates at least 1-year mean follow-up period |
| Review | Phase 2 | Phase 3 | |||
|---|---|---|---|---|---|
| 1. Study Eligibility Criteria | 2. Identification and Selection of Studies | 3. Data Collection and Study Appraisal | 4. Synthesis and Findings | Risk of Bias in the Review | |
| Machado et al. [30] |  | | | | |
| Evelyn Rohof et al. [32] |  | | | | |
| Chung et al. [33] | | | | ? | |
| Atala-Avecado et al. [31] | | | | ? | |
| Almpani et al. [29] | | ? | | | ? |
| Akhlef et al. [34] | | ? | | | |
= low risk; = high risk; ? = unclear risk.| Author and Year Published Number of Included Studies | Subgroup Analysis | Results and Conclusion |
|---|---|---|
| Chung et al., 2014 [33] 26 studies | systemic antibiotics (SAs), endodontic and splinting modalities and donor tooth morphology | Systemic Antibiotics: FR (IRR = 2.5, 95% CI: 0.9–7.2) and Root resorption (IRR = 1.4, 95% CI: 0.2–8.9) Endodontic treatment: FR (IRR = 1.0, 95% CI: 0.2–5.2) and Root resorption (IRR = 2.0, 95% CI: 0.2–9.3) Splinting: FR (IRR = 0.8, 95% CI: 0.1–5.5) Splinting ≥14 days vs. Splinting <14 days FR (IRR = 0.4, 95% CI: 0.1–2.0) Wire splinting vs. Suture splinting AR (IRR = 3.0, 95% CI: 0.0–607.9) Donor tooth: Annual Failure rate anterior (0.6% (95% CI: 0.2–2.3%), premolar 1.6% (95% CI 0.3–9.1%), and molar donors was 3.3% (95% CI: 2.4–4.7%) 1-Year Survival rate anterior, 99.4% (95% CI: 97.7–99.8%), premolar 98.4% (95% CI: 90.9–99.7%) and molar donors was 96.7% (95% CI: 95.3–97.6%) 5-Year Survival rate anterior, 96.9% (95% CI: 89.1–99.2%), premolar 92.3% (95% CI: 62.1–98.6%) and molar donors was 84.3% (95% CI: 78.7–88.6%) |
| Almpani et al., 2015 [29] 38 studies | Open apex vs. Closed apex Splinting Donor tooth | Open apex vs. closed apex: FR (RR: 0.3; 95% CI: 0.2–0.6) Wire splint vs. suture splint FR (RR: 3.7; 95% CI: 1.1–12.6) NSD for donor tooth, patient age (>20 vs. <20), gender, recipient site and surgical technique. |
| Atala-Acevedo et al., 2016 [31] 17 studies | Donor tooth, Recipient site, stage of root formation. | Donor tooth (Premolar vs. Molar) FR (OR, 0.46; 95% CI, 0.25 to 0.84) Recipient (Maxilla vs. Mandible) FR (OR, 0.38; 95% CI, 0.09 to 1.60) |
| C.M. Rohof et al., 2018 [32] 32 studies | donor tooth type recipient site, root development, splinting procedure, splinting duration, orthodontic procedure, and antibiotic regimen. | Survival rate: Premolar as recipient site (98.6%), Molar (97.3%) Premolar donor (98.4%), Molar (97.2%) Success rate: As recipient site; Incisor (98.5%), Canine (97.7%), Premolar (97.8%), Molar (95.1%) Maxillary recipient site (98.5%) vs. Mandibular recipient site (97.3%) Ankylosis rate: Premolar donor (1.9%), Molar donor(2.2%) Root Resorption Premolar donor (1.5%), Molar donor (5%) Pulp Necrosis: Premolar donor (4.4%), Molar donor (2.5%) |
| Primary Studies | Akhlef 2017 | Almpani 2015 | Atala 2016 | Chung 2014 | Evelyn Rohof 2018 | Machado 2016 | Size of Overlap |
|---|---|---|---|---|---|---|---|
| 1. Andreasen et al., 1990 | X | 1 | |||||
| 2. Bowden et al., 1990 | X | 1 | |||||
| 3. Czochrowska et al., 2000 | X | X | X | X | 4 | ||
| 4. Gilijamse et al., 2016 | X | 1 | |||||
| 5. Kristerson and Lagerström, 1991 | X | X | X | 3 | |||
| 6. Kugelberg et al., 1994 | X | X | X | 3 | |||
| 7. Kvint et al., 2010 | X | 1 | |||||
| 8. Mendoza-Mendoza et al., 2012 | X | X | X | X | 4 | ||
| 9. Slagsvold et al., 1978 | X | X | 2 | ||||
| 10. Stange et al., 2016 | X | 1 | |||||
| 11. Tanaka et al., 2008 | X | X | X | 3 | |||
| 12. Ahlberg et al., 1983 | X | X | 2 | ||||
| 13. Akiyama et al., 1998 | X | 1 | |||||
| 14. Akkocaoglu and Kasaboglu | X | 1 | |||||
| 15. Altonen et al., 1978 | X | 1 | |||||
| 16. Andreasen et al., 1990 | X | X | X | 3 | |||
| 17. Andreasen et al., 1990 | X | X | 2 | ||||
| 18. Andreasen et al., 1990 | X | X | 2 | ||||
| 19. Andreasen et al., 1990 | X | X | X | 3 | |||
| 20. Arikan et al. 32 2008 | X | X | 2 | ||||
| 21. Azaz et al., 1978 | X | X | 2 | ||||
| 22. Bauss et al., 2002 | X | X | 2 | ||||
| 23. Bauss et al., 2008 | X | 1 | |||||
| 24. Bauss et al., 2004 | X | 1 | |||||
| 25. Bauss et al., 2004 | X | 1 | |||||
| 26. Bauss et al., 2005 | X | 1 | |||||
| 27. Bauss et al., 2008 | X | 1 | |||||
| 28. Bauss et al., 2008 | X | 1 | |||||
| 29. Bauss and Kiliaridis 2009 | X | 1 | |||||
| 30. Eliasson et al., 1988 | X | X | 2 | ||||
| 31. Kahnberg 1987 | X | 1 | |||||
| 32. Kristerson 1985 | X | X | X | 3 | |||
| 33. Kristerson et al., 1991 | X | X | 2 | ||||
| 34. Lagerstron and Kristerson 1986 | X | 1 | |||||
| 35. Lundberg and Isaksson 1996 | X | X | X | 3 | |||
| 36. Marques- Ferreira et al., 2011 | X | 1 | |||||
| 37. Mejare et al., 2004 | X | X | 2 | ||||
| 38. Myrlund et al., 2004 | X | X | 2 | ||||
| 39. Nethander et al., 1988 | X | 1 | |||||
| 40. Nethander 1994 | X | 1 | |||||
| 41. Nethander 1998 | X | X | 2 | ||||
| 42. Ploder et al., 2001 | X | 1 | |||||
| 43. Pogrel et al., 1987 | X | 1 | |||||
| 44. Reich 2008 | X | 1 | |||||
| 45. Sagne et al., 1986 | X | 1 | |||||
| 46. Sobhi et al., 2003 | X | 1 | |||||
| 47. Sugai et al., 2010 | X | X | 2 | ||||
| 48. Thomson et al., 1984 | X | X | 2 | ||||
| 49. Yan et al., 2010 | X | X | X | X | 4 | ||
| 50. Bauss et al., 2002 | X | 1 | |||||
| 51. Bauss et al., 2004 | X | 1 | |||||
| 52. Bauss et al., 2003 | X | 1 | |||||
| 53. Czochrowska et al.,2000 | X | X | 2 | ||||
| 54. Denys et al., 2013 | X | 1 | |||||
| 55. Dıaz et al., 2014 (17) | X | 1 | |||||
| 56. Isa-Kara et al., 2011 | X | X | X | 3 | |||
| 57. Josefsson et al., 1999 | X | X | 2 | ||||
| 58. Kallu et al., 2005 | X | 1 | |||||
| 59. Mertens et al., 2014 | X | 1 | |||||
| 60. Nagori et al., 2014 | X | X | 2 | ||||
| 61. Naranjo et al., 2002 | X | 1 | |||||
| 62. Plakwicz et al., 2013 | X | X | 2 | ||||
| 63. Schutz et al., 2013 | X | X | 2 | ||||
| 64. Vilhjalmsson et al., 2011 | X | X | 2 | ||||
| 65. Forssell and Oksala (1986) | X | 1 | |||||
| 66. Gault and Warocquier-Clerout (2002) | X | 1 | |||||
| 67. Hovinga (1969) | X | 1 | |||||
| 68. Masif and Youseff (1977) | X | 1 | |||||
| 69. Moss (1968) | X | 1 | |||||
| 70. Niimi et al. (2011) | X | 1 | |||||
| 71. Patel et al. (2011) | X | 1 | |||||
| 72. Reade et al. (1973) | X | 1 | |||||
| 73. Schatz and Joho (1993) | X | 1 | |||||
| 74. Sange and Thilander (1990) | X | 1 | |||||
| 75. Schwartz et al. (1985) | X | 1 | |||||
| 76. Wang et al. (2007) | X | 1 | |||||
| 77. Watanabe et al. (2010) | X | X | 2 | ||||
| 78. Borring-Møller et al.1979 | X | 1 | |||||
| 79. de Carvalho et al. (2014) | X | 1 | |||||
| 80. Díaz et al., 2008 | X | 1 | |||||
| 81. Gonnissen et al., 2010 | X | X | 2 | ||||
| 82. Hernandez and Cuestascarner 1988 | X | 1 | |||||
| 83. Jonsson and Sigurdsson 2004 | X | 1 | |||||
| 84. Marcusson and Lilja-Karlander 1996 | X | 1 | |||||
| 85. Mertens et al., 2016 | X | 1 | |||||
| 86. Mensink and van Merkesteyn 2010 | X | 1 | |||||
| 87. Nagori et al. (2014) | X | 1 | |||||
| 88. Schatz and Joho 1992 | X | 1 | |||||
| 89. Shahbazian et al., 2013 | X | 1 | |||||
| 90. Paulsen and Andreasen (1998) | X | 1 | |||||
| 91. Paulsen et al. (1995) | X | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, A.K.; Khanal, N.; Acharya, N.; Hasan, M.R.; Saito, T. What Are the Complications, Success and Survival Rates for Autotransplanted Teeth? An Overview of Systematic Reviews and Metanalyses. Healthcare 2022, 10, 835. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050835
Singh AK, Khanal N, Acharya N, Hasan MR, Saito T. What Are the Complications, Success and Survival Rates for Autotransplanted Teeth? An Overview of Systematic Reviews and Metanalyses. Healthcare. 2022; 10(5):835. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050835
Chicago/Turabian StyleSingh, Ashutosh Kumar, Nikita Khanal, Nisha Acharya, Md Riasat Hasan, and Takashi Saito. 2022. "What Are the Complications, Success and Survival Rates for Autotransplanted Teeth? An Overview of Systematic Reviews and Metanalyses" Healthcare 10, no. 5: 835. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050835