
Patient-Oriented Research to Improve Internet-Delivered Cognitive Behavioural Therapy for People of Diverse Ethnocultural Groups in Routine Practice
 , and
, and
Abstract
:1. Introduction
1.1. Cultural Influence and the Need for Cultural Adaptation
1.2. Patient-Oriented Approach
1.3. Objectives
2. Materials and Methods
2.1. Setting
2.2. Wellbeing Course
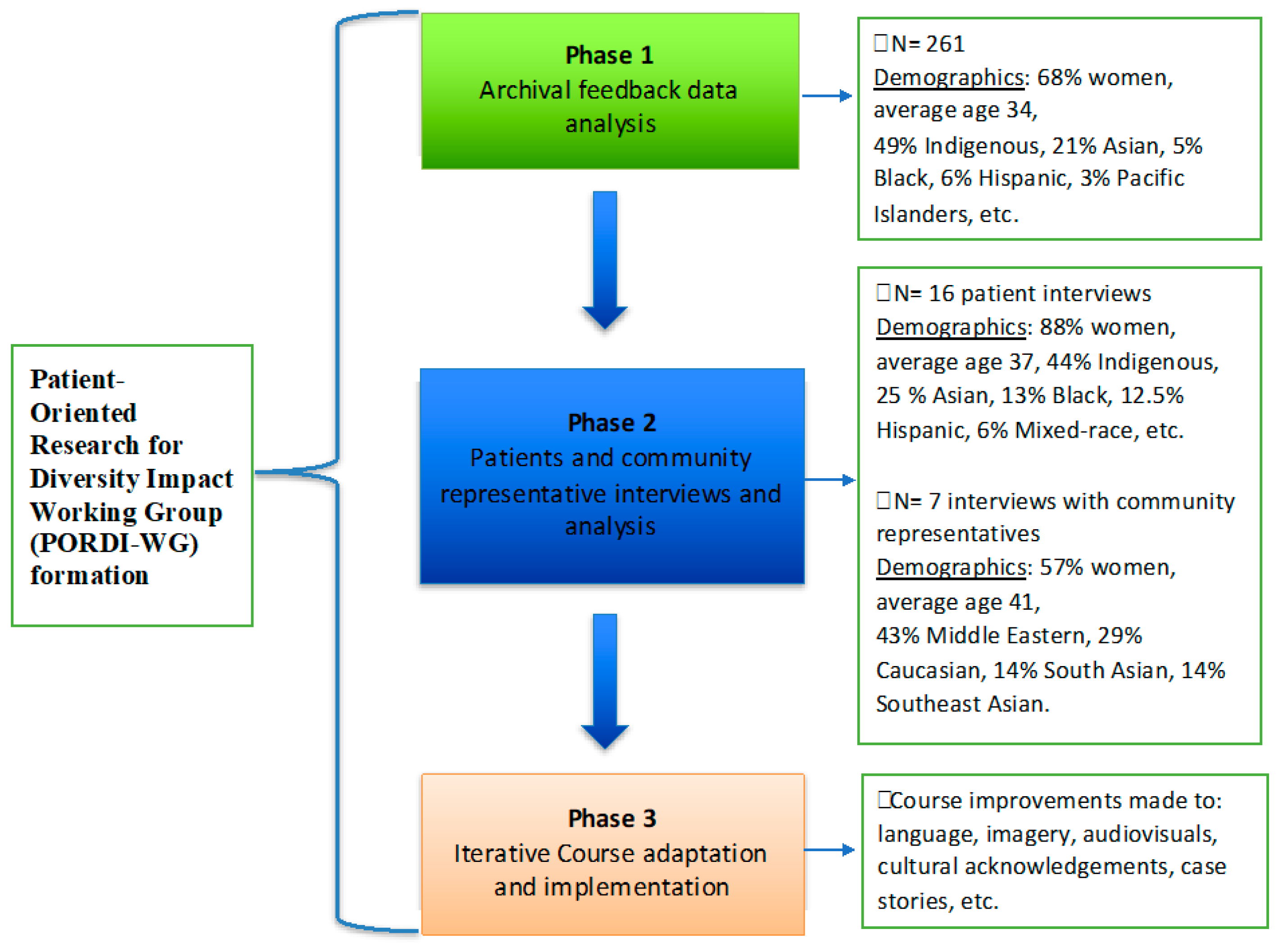
2.3. Working Group
2.4. Phase 1: Archival Data Analysis
2.5. Phase 2: Semi-Structured Interviews with Patients, Community Representatives, and Therapists
2.6. Phase 3: Iterative Course Adaptation Phase
3. Results
3.1. Archival Data Analysis
3.2. Interviews
“…She [therapist] was very dedicated and she was very capable. Even a little hint, she catches it and she starts guiding me. Also, she gave me a brief idea about the Course and how it applies to me in particular… she was very helpful”.[42, Male, Southeast Asian]
- i.
- “It was all good for me. I think it fit with me perfectly. I think that it doesn’t really matter if I’m like Asian…I think it was accessible for everyone”. [34, Female, Asian]
- ii.
- “Yes. There wasn’t really anything cultural about it, right? I don’t think anyway”. [22, Female, Indigenous]
“There is nothing about being a newcomer… it was one of the factors that gave me a lot of anxiety, I think. Having this shock that I’m in a new country with no connections with other people. I think that’s one [reason for anxiety]. I think it [the Course] was not made with a newcomer in mind… it’s more of a general”.[40, Male, Black]
3.3. Improvements
- (i)
- First, the five lessons in the Course were thoroughly reviewed for opportunities to simplify language by the OTU researchers and clinicians. This step involved identifying English language and Euro-American culture-specific idioms, metaphors, examples of activities, and academic vocabulary. These phrases were replaced with more general and commonly used language to ensure the Course was accessible to everyone, regardless of education level or cultural understanding.
- (ii)
- Second, the Course content was reviewed by PWLE, trainees, and CBO members to identify any issues with case stories, DIY activities, language, cultural relevance, and techniques described in the materials. At this stage, the aesthetics and user-friendliness of the Course materials were also reviewed. The group provided suggestions for improvement.
- (iii)
- Third, the final adaptation of the Course was informed by the recommendations from the working group and the findings from phases 1 and 2.
3.3.1. Course Materials
3.3.2. Training
3.3.3. Outreach
4. Discussion
Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andersson, G.; Carlbring, P.; Titov, N.; Lindefors, N. Internet interventions for adults with anxiety and mood disorders: A narrative umbrella review of recent meta-analyses. Can. J. Psychiatry 2019, 64, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Carlbring, P.; Andersson, G.; Cuijpers, P.; Riper, H.; Hedman-Lagerlöf, E. Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: An updated systematic review and meta-analysis. Cogn. Behav. Ther. 2018, 47, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titov, N.; Dear, B.; Nielssen, O.; Staples, L.; Hadjistavropoulos, H.; Nugent, M.; Adlam, K.; Nordgreen, T.; Bruvik, K.H.; Hovland, A. ICBT in routine care: A descriptive analysis of successful clinics in five countries. Internet Interv. 2018, 13, 108–115. [Google Scholar] [CrossRef]
- Smetanin, P.; Briante, C.; Khan, M.; Stiff, D.; Ahmad, S.; The Life and Economic Impact of Major Mental illnesses in Canada: 2011 to 2041. Toronto: RiskAnalytica, on behalf of the Mental Health Commission of Canada 2011. Available online: https://www.mentalhealthcommission.ca/wp-content/uploads/drupal/MHCC_Report_Base_Case_FINAL_ENG_0_0.pdf (accessed on 10 August 2022).
- Dobson, K.G.; Vigod, S.N.; Mustard, C.; Smith, P.M. Trends in the prevalence of depression and anxiety disorders among working-age Canadian adults between 2000 and 2016. Health Rep. 2020, 31, 12–23. [Google Scholar]
- Jenkins, E.K.; McAuliffe, C.; Hirani, S.; Richardson, C.; Thomson, K.C.; McGuinness, L.; Morris, J.; Kousoulis, A.; Gadermann, A. A portrait of the early and differential mental health impacts of the COVID-19 pandemic in Canada: Findings from the first wave of a nationally representative cross-sectional survey. Prev. Med. 2021, 145, 106333. [Google Scholar] [CrossRef]
- Miconi, D.; Li, Z.Y.; Frounfelker, R.L.; Santavicca, T.; Cénat, J.M.; Venkatesh, V.; Rousseau, C. Ethno-cultural disparities in mental health during the COVID-19 pandemic: A cross-sectional study on the impact of exposure to the virus and COVID-19-related discrimination and stigma on mental health across ethno-cultural groups in Quebec (Canada). BJPsych Open 2021, 7, e14. [Google Scholar] [CrossRef] [PubMed]
- Arriagada, P.; Hahmann, T.; O’Donnell, V. Indigenous People and Mental Health during the COVID-19 Pandemic (Catalogue No. 4528000); Statistics Canada: Ottawa, ON, Canada, 2020; Available online: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00035-eng.htm. (accessed on 3 January 2023).
- Cohen, K.; Peachey, D. Access to Psychological Services for Canadians: Getting What Works to Work for Canada’s Mental and Behavioural Health. Can. Psychol. 2014, 55, 126–130. [Google Scholar] [CrossRef]
- Statistics Canada. Health Fact Sheets: Mental Health Care Needs, 2018; Catalogue No. 82-625-X; Statistics Canada: Ottawa, ON, Canada, 2019; Available online: https://www150.statcan.gc.ca/n1/en/pub/82-625-x/2019001/article/00011-eng.pdf (accessed on 10 August 2022).
- Thomson, M.S.; Chaze, F.; George, U.; Guruge, S. Improving Immigrant Populations’ Access to Mental Health Services in Canada: A Review of Barriers and Recommendations. J. Immigr. Minor. Health 2015, 17, 1895–1905. [Google Scholar] [CrossRef]
- Khattar, J.; Griffith, L.E.; Jones, A.; De Rubeis, V.; de Groh, M.; Jiang, Y.; Basta, N.E.; Kirkland, S.; Wolfson, C.; Raina, P. Symptoms of depression and anxiety, and unmet healthcare needs in adults during the COVID-19 pandemic: A cross-sectional study from the Canadian Longitudinal Study on Aging. BMC Public. Health 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Hahmann, T.; Kumar, M.B. Unmet Health Care Needs during the Pandemic and Resulting Impacts among First Nations People Living Off Reserve, Métis and Inuit; Statistics Canada: Ottawa, ON, Canada, 2022; Available online: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2022001/article/00008-eng.htm# (accessed on 3 January 2023).
- Chiu, M.; Amartey, A.; Wang, X.; Kurdyak, P. Ethnic differences in mental health status and service utilization: A population-based study in Ontario, Canada. Can. J. Psychiatry 2018, 63, 481–491. [Google Scholar] [CrossRef] [Green Version]
- Whitley, R.; Wang, J.; Fleury, M.-J.; Liu, A.; Caron, J. Mental health status, health care utilisation, and service satisfaction among immigrants in Montreal: An epidemiological comparison. Can. J. Psychiatry 2017, 62, 570–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goetz, C.J.; Mushquash, C.J.; Maranzan, K.A. An Integrative Review of Barriers and Facilitators Associated With Mental Health Help Seeking Among Indigenous Populations. Psychiatr. Serv. 2023, 74, 3. [Google Scholar] [CrossRef]
- Fante-Coleman, T.; Jackson-Best, F. Barriers and facilitators to accessing mental healthcare in Canada for Black youth: A scoping review. Adolesc. Res. Rev. 2020, 5, 115–136. [Google Scholar] [CrossRef] [Green Version]
- Kirmayer, L.J.; Jarvis, G.E. Culturally responsive services as a path to equity in mental healthcare. Healthc. Pap. 2019, 18, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Salam, Z.; Odenigbo, O.; Newbold, B.; Wahoush, O.; Schwartz, L. Systemic and individual factors that shape mental health service usage among visible minority immigrants and refugees in Canada: A scoping review. Adm. Policy Ment. Health 2022, 49, 552–574. [Google Scholar] [CrossRef]
- Pilarinos, A.; Field, S.; Vasarhelyi, K.; Hall, D.; Fox, E.D.; Price, E.R.; Bonshor, L.; Bingham, B. A Qualitative Exploration of Indigenous Patients’ Experiences Of Racism And Perspectives On Improving Cultural Safety Within Health Care. Can. Med. Assoc. J. Open Access 2023, 11, E404–E410. [Google Scholar] [CrossRef]
- Gone, J.P. Re-imagining mental health services for American Indian communities: Centering indigenous perspectives. Am. J. Community Psychol. 2022, 69, 257–268. [Google Scholar] [CrossRef]
- Stonefish, T.; Kwantes, C.T. Values and acculturation: A Native Canadian exploration. Int. J. Intercult. Relat. 2017, 61, 63–76. [Google Scholar] [CrossRef]
- Nelson, S.E.; Wilson, K. The mental health of Indigenous peoples in Canada: A critical review of research. Soc. Sci. Med. 2017, 176, 93–112. [Google Scholar] [CrossRef]
- Cohen, J.A.; Kassan, A.; Wada, K.; Arthur, N.; Goopy, S. Enhancing multicultural and social justice competencies in Canadian counselling psychology training. Can. Psychol. 2022, 63, 298–312. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.; Alberts, N.M.; Nugent, M.; Marchildon, G. Improving access to psychological services through therapist-assisted, Internet-delivered cognitive behaviour therapy. Can. Psychol. 2014, 55, 303–311. [Google Scholar] [CrossRef]
- Moskalenko, M.Y.; Hadjistavropoulos, H.D.; Katapally, T.R. Barriers to patient interest in internet-based cognitive behavioral therapy: Informing e-health policies through quantitative analysis. Health Policy Technol. 2020, 9, 139–145. [Google Scholar] [CrossRef]
- Kirmayer, L.J. Cultural variations in the clinical presentation of depression and anxiety: Implications for diagnosis and treatment. J. Clin. Psychiatry 2001, 62, 22–30. [Google Scholar] [PubMed]
- Lewis-Fernández, R.; Kirmayer, L.J. Cultural concepts of distress and psychiatric disorders: Understanding symptom experience and expression in context. Transcult. Psychiatry 2019, 56, 786–803. [Google Scholar] [CrossRef]
- Kirmayer, L.J.; Young, A. Culture and somatization: Clinical, epidemiological, and ethnographic perspectives. Psychosom. Med. 1998, 60, 420–430. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric association: Washington, DC, USA, 2013. [Google Scholar]
- Napier, A.D.; Ancarno, C.; Butler, B.; Calabrese, J.; Chater, A.; Chatterjee, H.; Guesnet, F.; Horne, R.; Jacyna, S.; Jadhav, S. Culture and health. Lancet 2014, 384, 1607–1639. [Google Scholar] [CrossRef] [PubMed]
- Gopalkrishnan, N. Cultural diversity and mental health: Considerations for policy and practice. Front. Public. Health 2018, 6, 179. [Google Scholar] [CrossRef] [Green Version]
- Sue, S.; Zane, N.; Nagayama Hall, G.C.; Berger, L.K. The case for cultural competency in psychotherapeutic interventions. Annu. Rev. Psychol. 2009, 60, 525–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirmayer, L.J. Cultural competence and evidence-based practice in mental health: Epistemic communities and the politics of pluralism. Soc. Sci. Med. 2012, 75, 249–256. [Google Scholar] [CrossRef]
- Kleinman, A.; Benson, P. Anthropology in the clinic: The problem of cultural competency and how to fix it. PLoS Med. 2006, 3, e294. [Google Scholar] [CrossRef] [Green Version]
- Wendt, D.C.; Huson, K.; Albatnuni, M.; Gone, J.P. What are the best practices for psychotherapy with indigenous peoples in the United States and Canada? A thorny question. J. Consult. Clin. Psychol. 2022, 90, 802. [Google Scholar] [CrossRef]
- Castro, F.G.; Barrera Jr, M.; Holleran Steiker, L.K. Issues and challenges in the design of culturally adapted evidence-based interventions. Annu. Rev. Clin. Psychol. 2010, 6, 213–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernal, G.; Sáez-Santiago, E. Culturally centered psychosocial interventions. J. Consult. Clin. Psychol. 2006, 34, 121–132. [Google Scholar] [CrossRef]
- Lewis-Fernández, R.; Aggarwal, N.K.; Bäärnhielm, S.; Rohlof, H.; Kirmayer, L.J.; Weiss, M.G.; Jadhav, S.; Hinton, L.; Alarcón, R.D.; Bhugra, D. Culture and psychiatric evaluation: Operationalizing cultural formulation for DSM-5. Psychiatry 2014, 77, 130–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, D.M.; Draheim, A.A.; Anderson, P.L. Culturally adapted digital mental health interventions for ethnic/racial minorities: A systematic review and meta-analysis. J. Consult. Clin. Psychol. 2022, 90, 717–733. [Google Scholar] [CrossRef]
- Hall, G.C.N.; Ibaraki, A.Y.; Huang, E.R.; Marti, C.N.; Stice, E. A meta-analysis of cultural adaptations of psychological interventions. Behav. Ther. 2016, 47, 993–1014. [Google Scholar] [CrossRef]
- Harper Shehadeh, M.H.; Heim, E.; Chowdhary, N.; Maercker, A.; Albanese, E. Cultural adaptation of minimally guided interventions for common mental disorders: A systematic review and meta-analysis. JMIR Ment. Health 2016, 3, e5776. [Google Scholar] [CrossRef] [Green Version]
- Benish, S.G.; Quintana, S.; Wampold, B.E. Culturally adapted psychotherapy and the legitimacy of myth: A direct-comparison meta-analysis. J. Couns. Psychol. 2011, 58, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Soto, A.; Smith, T.B.; Griner, D.; Domenech Rodríguez, M.; Bernal, G. Cultural adaptations and therapist multicultural competence: Two meta-analytic reviews. J. Clin. Psychol. 2018, 74, 1907–1923. [Google Scholar] [CrossRef] [Green Version]
- Leske, S.; Harris, M.G.; Charlson, F.J.; Ferrari, A.J.; Baxter, A.J.; Logan, J.M.; Toombs, M.; Whiteford, H. Systematic review of interventions for Indigenous adults with mental and substance use disorders in Australia, Canada, New Zealand and the United States. Aust. N. Z. J. Psychiatry 2016, 50, 1040–1054. [Google Scholar] [CrossRef]
- Spanhel, K.; Balci, S.; Feldhahn, F.; Bengel, J.; Baumeister, H.; Sander, L.B. Cultural adaptation of internet-and mobile-based interventions for mental disorders: A systematic review. NPJ Digit. Med. 2021, 4, 128. [Google Scholar] [CrossRef]
- Smith, T.B.; Domenech Rodríguez, M.; Bernal, G. Culture. J. Clin. Psychol. 2011, 67, 166–175. [Google Scholar] [CrossRef]
- Bernal, G.; Bonilla, J.; Bellido, C. Ecological validity and cultural sensitivity for outcome research: Issues for the cultural adaptation and development of psychosocial treatments with Hispanics. J. Abnorm. Child. Psychol. 1995, 23, 67–82. [Google Scholar] [CrossRef]
- Resnicow, K.; Baranowski, T.; Ahluwalia, J.S.; Braithwaite, R.L. Cultural sensitivity in public health: Defined and demystified. Ethn. Dis. 1999, 9, 10–21. [Google Scholar] [PubMed]
- Barrera, M.; Castro, F.G. A heuristic framework for the cultural adaptation of interventions. Clin. Psychol. 2006, 13, 311–316. [Google Scholar] [CrossRef]
- Leong, F.T.; Lee, S.-H. A cultural accommodation model for cross-cultural psychotherapy: Illustrated with the case of Asian Americans. Psychol. Psychother. 2006, 43, 410–423. [Google Scholar] [CrossRef]
- Hwang, W.-C. The Formative Method for Adapting Psychotherapy (FMAP): A community-based developmental approach to culturally adapting therapy. Prof. Psychol. Res. Pract. 2009, 40, 369–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidani, S.; Ibrahim, S.; Lok, J.; Fan, L.; Fox, M.; Guruge, S. An integrated strategy for the cultural adaptation of evidence-based interventions. Health 2017, 9, 738. [Google Scholar] [CrossRef] [Green Version]
- Chu, J.; Leino, A. Advancement in the maturing science of cultural adaptations of evidence-based interventions. J. Consult. Psychol. 2017, 85, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Heim, E.; Kohrt, B.A. Cultural adaptation of scalable psychological interventions. Clin. Psychol. Eur. 2019, 1, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Naeem, F.; Sajid, S.; Naz, S.; Phiri, P. Culturally adapted CBT–the evolution of psychotherapy adaptation frameworks and evidence. Cogn. Behav. Ther. 2023, 16, e10. [Google Scholar] [CrossRef]
- Rathod, S.; Gega, L.; Degnan, A.; Pikard, J.; Khan, T.; Husain, N.; Munshi, T.; Naeem, F. The current status of culturally adapted mental health interventions: A practice-focused review of meta-analyses. Neuropsychiatr. Dis. Treat. 2018, 14, 165–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernal, G.; Jiménez-Chafey, M.I.; Domenech Rodríguez, M.M. Cultural adaptation of treatments: A resource for considering culture in evidence-based practice. Prof. Psychol. Res. Pract. 2009, 40, 361–368. [Google Scholar] [CrossRef]
- Statistics Canada. The Canadian Census: A Rich Portrait of the Country’s Religious and Ethnocultural Diversity; Statistics Canada: Ottawa, ON, Canada, 2022; Available online: https://www150.statcan.gc.ca/n1/en/daily-quotidien/221026/dq221026b-eng.pdf?st=v070_cQJ (accessed on 3 January 2023).
- Bernal, G.; Adames, C. Cultural adaptations: Conceptual, ethical, contextual, and methodological issues for working with ethnocultural and majority-world populations. Prev. Sci. 2017, 18, 681–688. [Google Scholar] [CrossRef]
- Cuijpers, P.; Cristea, I.A.; Karyotaki, E.; Reijnders, M.; Hollon, S.D. Component studies of psychological treatments of adult depression: A systematic review and meta-analysis. Psychother. Res. 2019, 29, 15–29. [Google Scholar] [CrossRef]
- Kirmayer, L.J.; Narasiah, L.; Munoz, M.; Rashid, M.; Ryder, A.G.; Guzder, J.; Hassan, G.; Rousseau, C.; Pottie, K. Common mental health problems in immigrants and refugees: General approach in primary care. CMAJ 2011, 183, E959–E967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumpfer, K.L.; Pinyuchon, M.; de Melo, A.T.; Whiteside, H.O. Cultural adaptation process for international dissemination of the strengthening families program. Eval. Health Prof. 2008, 31, 226–239. [Google Scholar] [CrossRef]
- Canadian Institutes of Health Research. Canada’s Strategy for Patient-Oriented Research: Improving Health Outcomes through Evidence-Informed Care. 2011. Available online: https://cihr-irsc.gc.ca/e/44000.html (accessed on 10 August 2022).
- Canadian Institutes of Health Research. Strategy For Patient-Oriented Research: Patient Engagement Framework. 2014. Available online: https://cihr-irsc.gc.ca/e/48413.html (accessed on 10 August 2022).
- Patrick, K.; Kebbe, M.; Aubin, D. A home for patient-oriented research. CMAJ 2018, 190, E607. [Google Scholar] [CrossRef] [Green Version]
- Aubin, D.; Hebert, M.; Eurich, D. The importance of measuring the impact of patient-oriented research. CMAJ 2019, 191, E860–E864. [Google Scholar] [CrossRef] [Green Version]
- Black, A.; Strain, K.; Wallsworth, C.; Charlton, S.-G.; Chang, W.; McNamee, K.; Hamilton, C. What constitutes meaningful engagement for patients and families as partners on research teams? J. Health Serv. Res. Policy 2018, 23, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Baker, G.R.; Fancott, C.; Judd, M.; O’Connor, P. Expanding patient engagement in quality improvement and health system redesign: Three Canadian case studies. Healthc. Manage. Forum 2016, 29, 176–182. [Google Scholar] [CrossRef]
- Li, L.C.; Hoens, A.M.; Wilhelm, L.; Bubber, V.; PausJenssen, E.; McKinnon, A.; Leese, J.; Otamendi, T.; Hamilton, C.B.; Zarin, W. Patient engagement in the SPOR Evidence Alliance: Reflection and learnings. Facets 2022, 7, 126–138. [Google Scholar] [CrossRef]
- Esmail, L.; Moore, E.; Rein, A. Evaluating patient and stakeholder engagement in research: Moving from theory to practice. J. Comp. Eff. Res. 2015, 4, 133–145. [Google Scholar] [CrossRef] [Green Version]
- Hadjistavropoulos, H.; Peynenburg, V.; Thiessen, D.L.; Nugent, M.; Karin, E.; Staples, L.; Dear, B.F.; Titov, N. Utilization, patient characteristics, and longitudinal improvements among patients from a provincially funded transdiagnostic internet-delivered cognitive behavioural therapy program: Observational study of trends over 6 years. Can. J. Psychiatry 2022, 67, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Titov, N.; Dear, B.F.; Staples, L.G.; Bennett-Levy, J.; Klein, B.; Rapee, R.M.; Shann, C.; Richards, D.; Andersson, G.; Ritterband, L. MindSpot clinic: An accessible, efficient, and effective online treatment service for anxiety and depression. Psychiatr. Serv. 2015, 66, 1043–1050. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.; Nugent, M.M.; Alberts, N.M.; Staples, L.; Dear, B.F.; Titov, N. Transdiagnostic Internet-delivered cognitive behaviour therapy in Canada: An open trial comparing results of a specialized online clinic and nonspecialized community clinics. J. Anxiety Disord. 2016, 42, 19–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjistavropoulos, H.; Peynenburg, V.; Thiessen, D.; Nugent, M.; Adlam, K.; Owens, K.; Karin, E.; Dear, B.; Titov, N. A pragmatic factorial randomized controlled trial of transdiagnostic internet-delivered cognitive behavioural therapy: Exploring benefits of homework reflection questionnaires and twice-weekly therapist support. Internet. Interv. 2020, 22, 100357. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.; Schneider, L.; Mehta, S.; Karin, E.; Dear, B.; Titov, N. Preference trial of internet-delivered cognitive behaviour therapy comparing standard weekly versus optional weekly therapist support. J. Anxiety Disord. 2019, 63, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Hadjistavropoulos, H.; Peynenburg, V.; Thiessen, D.; Nugent, M.; Karin, E.; Dear, B.; Titov, N. A randomized factorial trial of internet-delivered cognitive behavioural therapy: An 8-week program with or without extended support and booster lesson. Internet Interv. 2022, 27, 100499. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.; Schneider, L.; Edmonds, M.; Karin, E.; Nugent, M.; Dirkse, D.; Dear, B.; Titov, N. Randomized controlled trial of internet-delivered cognitive behaviour therapy comparing standard weekly versus optional weekly therapist support. J. Anxiety Disord. 2017, 52, 15–24. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.; Peynenburg, V.; Nugent, M.; Karin, E.; Titov, N.; Dear, B. Transdiagnostic internet-delivered cognitive behaviour therapy with therapist support offered once-weekly or once-weekly supplemented with therapist support within one-business-day: Pragmatic randomized controlled trial. Internet. Interv. 2020, 22, 100347. [Google Scholar] [CrossRef] [PubMed]
- McCall, H.C.; Beahm, J.D.; Fournier, A.K.; Burnett, J.L.; Carleton, R.N.; Hadjistavropoulos, H.D. Stakeholder perspectives on internet-delivered cognitive behavioural therapy for public safety personnel: A qualitative analysis. Can. J. Behav. Sci. 2021, 53, 232–242. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.; Faller, Y.; Klatt, A.; Nugent, M.; Dear, B.; Titov, N. Patient perspectives on strengths and challenges of therapist-assisted internet-delivered cognitive behaviour therapy: Using the patient voice to improve care. Community Ment. Health J. 2018, 54, 944–950. [Google Scholar] [CrossRef] [Green Version]
- Hedman-Lagerlöf, E.; Carlbring, P.; Svärdman, F.; Riper, H.; Cuijpers, P.; Andersson, G. Therapist-supported Internet-based cognitive behaviour therapy yields similar effects as face-to-face therapy for psychiatric and somatic disorders: An updated systematic review and meta-analysis. World Psychiatry. 2023, 22, 305–314. [Google Scholar] [CrossRef]
- Bradley, E.H.; Curry, L.A.; Devers, K.J. Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Serv. Res. 2007, 42, 1758–1772. [Google Scholar] [CrossRef] [Green Version]
- Bucholtz, M. The politics of transcription. J. Pragmat. 2000, 32, 1439–1465. [Google Scholar] [CrossRef]
- McMullin, C. Transcription and qualitative methods: Implications for third sector research. Voluntas 2021, 34, 140–153. [Google Scholar] [CrossRef] [PubMed]
- Goudreau, G.; Weber-Pillwax, C.; Cote-Meek, S.; Madill, H.; Wilson, S. Hand drumming: Health-promoting experiences of Aboriginal women from a Northern Ontario urban community. Int. J. Indig. Health 2008, 4, 72–83. [Google Scholar] [CrossRef]
- Weiss, M. Explanatory Model Interview Catalogue (EMIC): Framework for comparative study of illness. Transcult. Psychiatry 1997, 34, 235–263. [Google Scholar] [CrossRef]
- Groleau, D.; Young, A.; Kirmayer, L.J. The McGill Illness Narrative Interview (MINI): An interview schedule to elicit meanings and modes of reasoning related to illness experience. Transcult. Psychiatry 2006, 43, 671–691. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.; Gullickson, K.M.; Adrian-Taylor, S.; Wilhelms, A.; Sundström, C.; Nugent, M. Stakeholder perceptions of internet-delivered cognitive behavior therapy as a treatment option for alcohol misuse: Qualitative analysis. JMIR Ment. Health 2020, 7, e14698. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.; Naz, S. The need for service change and community outreach work to support trans-cultural cognitive behaviour therapy with Black and Minority Ethnic communities. Cogn. Behav. Ther. 2019, 12, e1. [Google Scholar] [CrossRef] [Green Version]
- Statistics Canada. Primary Health Care Providers, 2019. 2020. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2020001/article/00004-eng.htm (accessed on 10 August 2022).
- Korzinski, D. Doc Deficits: Half of Canadians Either Can’t Find a Doctor or Can’t Get a Timely Appointment with the One They Have; Angus Reid Institute 2022. Available online: https://angusreid.org/canada-health-care-family-doctors-shortage/ (accessed on 3 January 2023).


{kind=link}
| Most Helpful Skills | Examples | n | % |
|---|---|---|---|
| Thought challenging | “Thought challenging because examining your negative thoughts helps to put them in perspective and to create a healthier view of them”. “Thought challenging was the most helpful skill in this course because without it I would not have been able to overcome my negative mindset. Through it I was able to change my ways of thinking into a more positive one. It was a steppingstone for me to be confident in learning new skills for the other lessons. I was able to be hopeful that I can overcome my symptoms”. | 165 | 63.22 |
| Controlled breathing | “Controlled breathing was my most helpful skill specifically from this course, given how simple the technique is, I think I found it extremely beneficial to complement other strategies I was starting to work on as well”. “controlled breathing has greatly improved my functioning throughout daily tasks” | 71 | 27.20 |
| Graded exposure | “Graded exposure will probably be the most helpful skill in short and long term. It is very helpful for me and will benefit me for years; I am sure of it”. “I feel graded exposure is the most helpful skill in this course, because I used to play games and watch videos to escape from the real world, but now I can plan to do something every day”. “…graded exposure was helpful in getting out and about. I also noticed that I started playing chess again and reading more often. In other words, I am enjoying past activities rather than doing nothing”. | 46 | 17.62 |
| Activity planning | “Becoming more active struck me as the most important skill—I actually noticed a direct impact in my life once I started to apply activity scheduling in my life (as much as I could)”. “Becoming more active has been what gets me to the point of happiness, when I sit too much the symptoms increase drastically and I become so overwhelmed to the point of being numb and I can’t feel anything even love for my loved ones”. | 44 | 16.86 |
| Cycle of symptoms | “I really liked learning about the cycle of symptoms and realizing what healthy versus un-healthy anxiety/stress is. I really thought I was more educated on this topic but had a real eye opening experience when I started to learn about it”. “Increased awareness of symptoms and what can be done before it escalates”. | 22 | 8.43 |
| Overall positive reflection | “All of the lessons were very helpful”. “I can’t choose just one this course was challenging but beneficial in learning that I can help myself” | 13 | 4.98 |
| No new skills learned | “There wasn’t a most helpful skill. I found that I was already doing the things that had been suggested” | 8 | 3.06 |
| No response provided | N/A; | 3 | 1.15 |
| Relapse prevention | “The relapse plan. Even reading the three reasons we relapse are all items I certainly relate to and know that by recognizing any of those I will set myself up for make changes that will be positive going forward”. | 3 | 1.15 |
| Most Liked Elements | Examples | n | % |
|---|---|---|---|
| DIY Guides | “…even though I knew about most lessons beforehand, the DIY guides helped me remember the lessons and pushed/motivated me to act on what I learned”. “I really liked the DIY guides as they provided great activities as well as they summarized many of the main points of a given weeks lesson. These lesson summaries in the DIY guides where helpful to me as I didn’t always have consistent access to my computer throughout the course, so being able to print off and have the DIY guides available to take places with me provided a good alternative for when I wanted to review some of the most important points of a given weeks lesson”. | 112 | 42.91 |
| Stories | “The stories, I felt a connection to the stories and I could relate to them. Reading how the different skills helped them feel better gave me hope that this actually does work”. “Including examples from other people who are dealing with anxiety and depression helps me realize that I am not the only one who deals with these feelings. It really puts it into perspective that I’m not perfect, but I am a good person and its about time I realized that”. “The stories were nice to read as they made me feel like I wasn’t alone in my symptoms and feelings” | 88 | 33.72 |
| Additional Resources | “I think the resources are helpful that I learn a lot from them”. “…I liked being able to access the supplements at my own pace, I think that allowed me to read the resources for the problems I was facing earlier on which allowed me to start on some strategies sooner rather than later as well, although I eventually went through all the supplements (apart from motherhood I suppose, since being a parent is not part of my life at this time)”. | 55 | 21.07 |
| Accessibility | “Easier access and flexible to accommodate with busy life style”. “How it explains in a simple and logical way the material”. “I liked that I was able to do/complete the course at my own pace and with what worked for me—online”. | 44 | 16.86 |
| Therapist support | “I really liked having someone contact me every Tuesday to let me know they care about my progress. It has helped me make it through this course and not give up”. “I think the setup is excellent, I also believe having someone to check in every week helps to keep the client accountable. I’m pretty sure I would have withdrawn weeks ago if it weren’t for the accountability I felt towards Kerry as she was working so hard to keep me engaged and supporting me in every way she could through email”. “I also really liked emailing with my therapist. It added accountability in addition to giving me feedback, suggestions, etc. It was a bit tricky that she would check in on Fridays because that was the end of the week for most lessons, but it ended up reinforcing the inter-connectedness between the different lessons and I think it helped me integrate everything better”. | 39 | 14.94 |
| Lessons | “Each lesson provided valuable insight. I enjoyed making appointments with friends so I would keep doing it”. “The lessons are pretty easy to understand and read”. | 25 | 9.58 |
| Overall positive response | “I liked all aspects of the course and think it is well laid out”. | 18 | 6.90 |
| Educational approach | “I liked how everything was explained, the symptoms and terminologies”. “I liked the way that the course was approached. It wasn’t a looking down upon approach but a down to earth, ‘this is how things are, how can we fix them?’” | 9 | 3.45 |
| No response provided | “N/A” | 3 | 1.15 |
| Most Disliked | Example | n | % |
|---|---|---|---|
| Issue with content | 103 | 39.46 | |
| Stories | “The stories I didn’t find to be super engaging, mainly just glossed over them” “The stories were a bit hard to relate to since I felt like Glenn and Jo were so much more successful than I was and were so normal/well adjusted”. “It would be helpful if you could include some scenarios where people are trying to deal with difficult relationships, or people around them who are very negative and toxic. This was the cause of much of my depression and it would be very helpful to read some examples or stories of people dealing with this type of problem” | 34 | 13.03 |
| Website interface or utilities | “I don’t enjoy reading the font selected to write out the information and surveys. It’s difficult for me to read, the words are squished together and it takes extra effort just to make sure I’m seeing the words properly”. “One thing I would suggest is for the questionary layout, every time when I finish the questions I have to remember to click the “Press to submit” button (which by the way it’s not easy to spot and easily to miss it on the left hand side) before going to the next section, if I forgot then I have to restart all over again. This is not user friendly layout and it can be done in a much better way for end-users”. “I guess improve upon the interface for the surveys; you have any idea how infuriating it is to fill out the survey and hit “next” instead of “submit” and all your answers get reset because you didn’t hit “submit” first?” | 33 | 12.64 |
| Content not personal relevant | “Lack of personalization” | 10 | 3.83 |
| Additional resources | “the resources while informative about the issue didn’t always offer many Tips for dealing with it | 9 | 3.45 |
| DIY guide | “DIY I thought it was full of activities and not just a summary of the lesson. I thought it was going to be like a booklet of stuff that will help me feel better and not a bunch of the same information that I read”. “I would suggest creating a daily activity that we can follow in the DIY for example. Journaling daily to keep us more on track in the course. I find that I only read the materials once a week and forget to review until the next week”. | 7 | 2.68 |
| Generic information | “Somewhat generic” | 6 | 2.30 |
| Repetitive material | “Lots of repetitiveness. I understand why though. At times, it was a little much”. | 4 | 1.53 |
| Issues with process | 53 | 20.31 | |
| Limited time | “I would like to have more time to do the lessons. Maybe shorter lessons and a longest period (e.g., 3 months)”. | 27 | 10.34 |
| Therapist support | “I would like to have more contact with my therapist. Possibly even twice a week instead of just once a week”. | 19 | 7.28 |
| Lack of structure | “Being on my own pace with no forced communication. Allowed me to not keep up with the work and I wouldn’t reach out to the therapist on my own”. | 7 | 2.68 |
| Overall positive reflection | “There wasn’t anything I didn’t like about the course”. | 84 | 32.18 |
| No response provided | “N/A” | 30 | 11.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sapkota, R.P.; Valli, E.; Wilhelms, A.; Adlam, K.; Bourgeault, L.; Heron, V.; Dickerson, K.; Nugent, M.; Hadjistavropoulos, H.D. Patient-Oriented Research to Improve Internet-Delivered Cognitive Behavioural Therapy for People of Diverse Ethnocultural Groups in Routine Practice. Healthcare 2023, 11, 2135. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11152135
Sapkota RP, Valli E, Wilhelms A, Adlam K, Bourgeault L, Heron V, Dickerson K, Nugent M, Hadjistavropoulos HD. Patient-Oriented Research to Improve Internet-Delivered Cognitive Behavioural Therapy for People of Diverse Ethnocultural Groups in Routine Practice. Healthcare. 2023; 11(15):2135. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11152135
Chicago/Turabian StyleSapkota, Ram P., Emma Valli, Andrew Wilhelms, Kelly Adlam, Lee Bourgeault, Vanessa Heron, Kathryn Dickerson, Marcie Nugent, and Heather D. Hadjistavropoulos. 2023. "Patient-Oriented Research to Improve Internet-Delivered Cognitive Behavioural Therapy for People of Diverse Ethnocultural Groups in Routine Practice" Healthcare 11, no. 15: 2135. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11152135