
Gender Differences in Psychosocial Outcomes and Coping Strategies of Patients with Colorectal Cancer: A Systematic Review


Abstract
:1. Introduction
Data Extraction and Synthesis
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Quality Assessment
3. Results
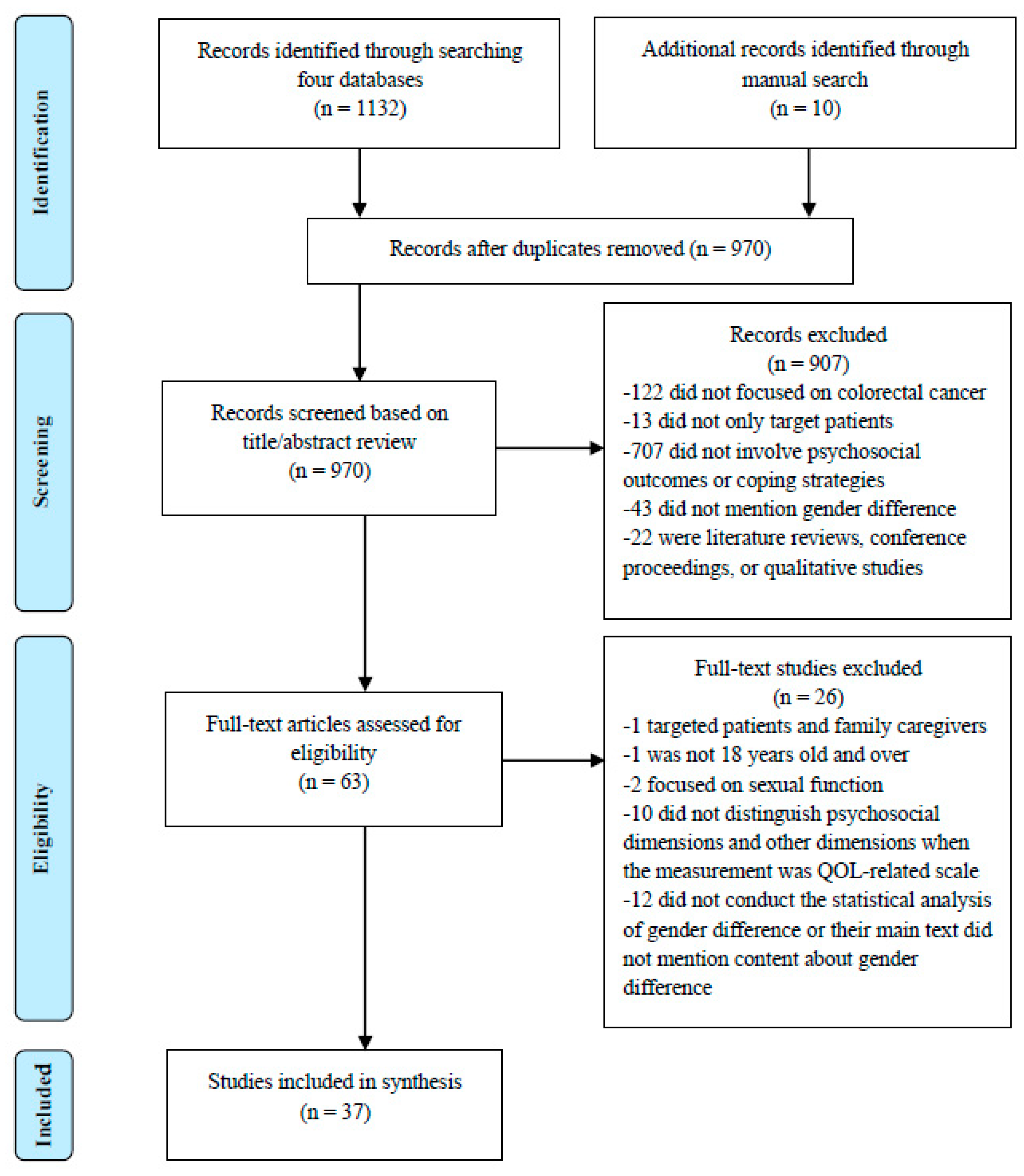
3.1. Study Selection Process
3.2. Quality of the Included Studies
3.3. Characteristics of the Included Studies
3.4. Gender Differences in Psychological Outcomes
3.5. Gender Differences in Social Outcomes
3.6. Gender Differences in Coping Strategies
4. Discussion
4.1. Potential Explanation of Gender Differences in Psychological Outcomes
4.2. Potential Explanation of Gender Differences in Social Outcomes
4.3. Potential Explanation of Gender Differences on Coping Strategies
4.4. Clinical Implications
4.5. Limitations of this Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef]
- Cheng, V.; Oveisi, N.; McTaggart-Cowan, H.; Loree, J.M.; Murphy, R.A.; De Vera, M.A. Colorectal Cancer and Onset of Anxiety and Depression: A Systematic Review and Meta-Analysis. Curr. Oncol. 2022, 29, 8751–8766. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.N.; Huang, M.L.; Kao, C.H. Prevalence of Depression and Anxiety in Colorectal Cancer Patients: A Literature Review. Int. J. Environ. Res. Public Health 2019, 16, 411. [Google Scholar] [CrossRef] [PubMed]
- Han, C.J.; Yang, G.S.; Syrjala, K. Symptom Experiences in Colorectal Cancer Survivors After Cancer Treatments: A Systematic Review and Meta-analysis. Cancer Nurs. 2020, 43, E132–E158. [Google Scholar] [CrossRef]
- Lim, C.Y.S.; Laidsaar-Powell, R.C.; Young, J.M.; Kao, S.C.; Zhang, Y.; Butow, P. Colorectal cancer survivorship: A systematic review and thematic synthesis of qualitative research. Eur. J. Cancer Care 2021, 30, e13421. [Google Scholar] [CrossRef]
- Buccafusca, G.; Proserpio, I.; Tralongo, A.C.; Rametta Giuliano, S.; Tralongo, P. Early colorectal cancer: Diagnosis, treatment and survivorship care. Crit. Rev. Oncol. Hematol. 2019, 136, 20–30. [Google Scholar] [CrossRef]
- Phung, V.D.; Fang, S.Y. Body Image Issues in Patients With Colorectal Cancer: A Scoping Review. Cancer Nurs. 2023, 46, 233–247. [Google Scholar] [CrossRef]
- Traa, M.J.; De Vries, J.; Roukema, J.A.; Den Oudsten, B.L. Sexual (dys)function and the quality of sexual life in patients with colorectal cancer: A systematic review. Ann. Oncol. 2012, 23, 19–27. [Google Scholar] [CrossRef]
- Mols, F.; Schoormans, D.; de Hingh, I.; Oerlemans, S.; Husson, O. Symptoms of anxiety and depression among colorectal cancer survivors from the population-based, longitudinal PROFILES Registry: Prevalence, predictors, and impact on quality of life. Cancer 2018, 124, 2621–2628. [Google Scholar] [CrossRef] [PubMed]
- Reese, J.B.; Handorf, E.; Haythornthwaite, J.A. Sexual quality of life, body image distress, and psychosocial outcomes in colorectal cancer: A longitudinal study. Support. Care Cancer 2018, 26, 3431–3440. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Román, K.; Tovar-Gálvez, M.I.; Liñán-González, A.; Cañadas de la Fuente, G.A.; de la Fuente-Solana, E.I.; Díaz-Rodríguez, L. Coping Strategies in Elderly Colorectal Cancer Patients. Cancers 2022, 14, 608. [Google Scholar] [CrossRef] [PubMed]
- Abelson, J.S.; Chait, A.; Shen, M.J.; Charlson, M.; Dickerman, A.; Yeo, H.L. Sources of distress among patients undergoing surgery for colorectal cancer: A qualitative study. J. Surg. Res. 2018, 226, 140–149. [Google Scholar] [CrossRef]
- Sterba, K.R.; Zapka, J.; Gore, E.I.; Ford, M.E.; Ford, D.W.; Thomas, M.; Wallace, K. Exploring dimensions of coping in advanced colorectal cancer: Implications for patient-centered care. J. Psychosoc. Oncol. 2013, 31, 517–539. [Google Scholar] [CrossRef]
- Brennan, J. Adjustment to cancer—Coping or personal transition? Psychooncology 2001, 10, 1–18. [Google Scholar] [CrossRef]
- McCaughan, E.; Prue, G.; Parahoo, K. A systematic review of quantitative studies reporting selected patient experienced outcomes, with a specific focus on gender differences in people with colorectal cancer. Eur. J. Oncol. Nurs. 2009, 13, 376–385. [Google Scholar] [CrossRef]
- Grant, M.; McMullen, C.K.; Altschuler, A.; Mohler, M.J.; Hornbrook, M.C.; Herrinton, L.J.; Wendel, C.S.; Baldwin, C.M.; Krouse, R.S. Gender differences in quality of life among long-term colorectal cancer survivors with ostomies. Oncol. Nurs. Forum 2011, 38, 587–596. [Google Scholar] [CrossRef]
- Heidari, S.; Babor, T.F.; De Castro, P.; Tort, S.; Curno, M. Sex and Gender Equity in Research: Rationale for the SAGER guidelines and recommended use. Res. Integr. Peer Rev. 2016, 1, 2. [Google Scholar] [CrossRef]
- Acevedo-Ibarra, J.N.; Juarez-Garcia, D.M.; Espinoza-Velazco, A.; Buenaventura-Cisneros, S. Quality of life in Mexican colorectal cancer patients: Analysis with sociodemographic, medical, and psychological variables. Psychol. Health Med. 2021, 26, 853–866. [Google Scholar] [CrossRef]
- Akyol, M.; Ulger, E.; Alacacioglu, A.; Kucukzeybek, Y.; Yildiz, Y.; Bayoglu, V.; Gumus, Z.; Yildiz, I.; Salman, T.; Varol, U.; et al. Sexual satisfaction, anxiety, depression and quality of life among Turkish colorectal cancer patients Izmir Oncology Group (IZOG) study. Jpn. J. Clin. Oncol. 2015, 45, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Akyol, M.; Ulger, E.; Alacacioglu, A.; Kucukzeybek, Y.; Bayoglu, V.; Yildiz, Y.; Yildiz, I.; Salman, T.; Varol, U.; Demir, L.; et al. Quality of life in colorectal cancer patients: An Izmir Oncology Group (IZOG) study. J. Buon 2015, 20, 1015–1022. [Google Scholar] [PubMed]
- Al-Shandudi, M.; Al-Mandhari, M.; Chan, M.F.; Al-Hajri, T.; Al-Balushi, M.; Al-Azri, M. Health-Related Quality of Life of Omani Colorectal Cancer Survivors. Cancer Control J. Moffitt Cancer Cent. 2022, 29, 10732748221084198. [Google Scholar] [CrossRef]
- Alabbas, F.F.; Al-Otaibi, S.M.; Pasha, M.H.; Alghamdi, A.M.; Al-Hindi, H.M.; Al-Ahwal, M.S.; El-Deek, B.S. Impact of Physiological Symptoms and Complications of Colorectal Cancer on the Quality of Life of Patients at King Abdulaziz University Hospital. J. Cancer Educ. 2016, 31, 221–227. [Google Scholar] [CrossRef]
- Aminisani, N.; Nikbakht, H.A.; Shojaie, L.; Jafari, E.; Shamshirgaran, M. Gender Differences in Psychological Distress in Patients with Colorectal Cancer and Its Correlates in the Northeast of Iran. J. Gastrointest. Cancer 2021, 53, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Au, T.Y.; Zauszniewski, J.A.; King, T.M. Health-seeking behaviors and sexuality in rectal cancer survivors in Taiwan: Associations with spirituality and resourcefulness. Oncol. Nurs. Forum 2012, 39, E390–E397. [Google Scholar] [CrossRef]
- Baldwin, C.M.; Grant, M.; Wendel, C.; Hornbrook, M.C.; Herrinton, L.J.; McMullen, C.; Krouse, R.S. Gender differences in sleep disruption and fatigue on quality of life among persons with ostomies. J. Clin. Sleep Med. 2009, 5, 335–343. [Google Scholar] [CrossRef]
- Belachew, A.A.; Reyes, M.E.; Ye, Y.; Raju, G.S.; Rodriguez, M.A.; Wu, X.; Hildebrandt, M.A.T. Patterns of racial/ethnic disparities in baseline health-related quality of life and relationship with overall survival in patients with colorectal cancer. Qual. Life Res. 2020, 29, 2977–2986. [Google Scholar] [CrossRef]
- Braamse, A.M.; van Turenhout, S.T.; Terhaar Sive Droste, J.S.; de Groot, G.H.; van der Hulst, R.W.; Klemt-Kropp, M.; Kuiken, S.D.; Loffeld, R.J.; Uiterwaal, M.T.; Mulder, C.J.; et al. Factors associated with anxiety and depressive symptoms in colorectal cancer survivors. Eur. J. Gastroenterol. Hepatol. 2016, 28, 831–835. [Google Scholar] [CrossRef]
- Du, X.; Wang, D.; Du, H.; Zou, Q.; Jin, Y. The correlation between intimate relationship, self-disclosure, and adaptability among colorectal cancer enterostomy patients. Medicine 2021, 100, e25904. [Google Scholar] [CrossRef]
- Dunn, J.; Ng, S.K.; Holland, J.; Aitken, J.; Youl, P.; Baade, P.D.; Chambers, S.K. Trajectories of psychological distress after colorectal cancer. Psycho-Oncology 2013, 22, 1759–1765. [Google Scholar] [CrossRef] [PubMed]
- Eddington, H.S.; McLeod, M.; Trickey, A.W.; Barreto, N.; Maturen, K.; Morris, A.M. Patient-reported distress and age-related stress biomarkers among colorectal cancer patients. Cancer Med. 2021, 10, 3604–3612. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, K.S.; Lode, K.; Husebø, S.I.E.; Kørner, H. Exploring variables affecting sense of coherence and social support in recovery after colorectal cancer surgery among the oldest old. Geriatr. Nurs. 2022, 47, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Gautam, S.; Poudel, A. Effect of gender on psychosocial adjustment of colorectal cancer survivors with ostomy. J. Gastrointest. Oncol. 2016, 7, 938–945. [Google Scholar] [CrossRef]
- Giesinger, J.; Kemmler, G.; Mueller, V.; Zabernigg, A.; Mayrbaeurl, B.; Thaler, J.; Ofner, D.; Pegger, C.; Rumpold, G.; Weber, B.; et al. Are gender-associated differences in quality of life in colorectal cancer patients disease-specific? Qual. Life Res. 2009, 18, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Goldzweig, G.; Andritsch, E.; Hubert, A.; Walach, N.; Perry, S.; Brenner, B.; Baider, L. How relevant is marital status and gender variables in coping with colorectal cancer? A sample of middle-aged and older cancer survivors. Psycho-Oncology 2009, 18, 866–874. [Google Scholar] [CrossRef]
- Han, C.J.; Gigic, B.; Schneider, M.; Kulu, Y.; Peoples, A.R.; Ose, J.; Kölsch, T.; Jacobsen, P.B.; Colditz, G.A.; Figueiredo, J.C.; et al. Risk factors for cancer-related distress in colorectal cancer survivors: One year post surgery. J. Cancer Surviv. 2020, 14, 305–315. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Chishaki, A.; Kawamoto, R.; Manabe, T.; Ueki, T.; Hirata, K.; Miyazono, M.; Kanaoka, M.; Tomioka, A.; Nakano, M.; et al. A longitudinal study of gender differences in quality of life among Japanese patients with lower rectal cancer treated with sphincter-saving surgery: A 1-year follow-up. World J. Surg. Oncol. 2015, 13, 91. [Google Scholar] [CrossRef]
- Laghousi, D.; Jafari, E.; Nikbakht, H.; Nasiri, B.; Shamshirgaran, M.; Aminisani, N. Gender differences in health-related quality of life among patients with colorectal cancer. J. Gastrointest. Oncol. 2019, 10, 453–461. [Google Scholar] [CrossRef]
- Mahjoubi, B.; Mirzaei, R.; Azizi, R.; Jafarinia, M.; Zahedi-Shoolami, L. A cross-sectional survey of quality of life in colostomates: A report from Iran. Health Qual. Life Outcomes 2012, 10, 136. [Google Scholar] [CrossRef]
- Milbury, K.; Cohen, L.; Jenkins, R.; Skibber, J.M.; Schover, L.R. The association between psychosocial and medical factors with long-term sexual dysfunction after treatment for colorectal cancer. Support. Care Cancer 2013, 21, 793–802. [Google Scholar] [CrossRef]
- Mrabti, H.; Amziren, M.; ElGhissassi, I.; Bensouda, Y.; Berrada, N.; Abahssain, H.; Boutayeb, S.; El Fakir, S.; Nejjari, C.; Benider, A.; et al. Quality of life of early stage colorectal cancer patients in Morocco. BMC Gastroenterol. 2016, 16, 131. [Google Scholar] [CrossRef] [PubMed]
- Palas, J.C.M.; Hyland, K.A.; Nelson, A.M.; Small, B.J.; Jim, H.S.L.; Jacobsen, P.B. An examination of the relationship of patient modifiable and non-modifiable characteristics with fear of cancer recurrence among colorectal cancer survivors. Support. Care Cancer 2021, 29, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.P.D.; Cesarino, C.B.; Martins, M.R.I.; Pinto, M.H.; Netinho, J.G. Associations among socio-demographic and clinical factors and the quality of life of ostomized patients. Rev. Lat. Am. Enferm. 2012, 20, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Ran, L.Y.; Jiang, X.D.; Qian, E.Z.; Kong, H.Q.; Wang, X.L.; Liu, Q. Quality of life, self-care knowledge access, and self-care needs in patients with colon stomas one month post-surgery in a Chinese Tumor Hospital. Int. J. Nurs. Sci. 2016, 3, 252–258. [Google Scholar] [CrossRef]
- Repić, G.; Ivanović, S.; Stanojević, Č.; Trgovčević, S. Psychological and spiritual well-being aspects of the quality of life in colostomy patients. Vojnosanit. Pregl. 2016, 75, 357. [Google Scholar] [CrossRef]
- Reyes, M.E.; Ye, Y.; Zhou, Y.; Liang, A.; Kopetz, S.; Rodriquez, M.A.; Wu, X.; Hildebrandt, M.A.T. Predictors of health-related quality of life and association with survival may identify colorectal cancer patients at high risk of poor prognosis. Qual. Life Res. 2017, 26, 319–330. [Google Scholar] [CrossRef]
- Ristvedt, S.L.; Trinkaus, K.M.; Ristvedt, S.L.; Trinkaus, K.M. Trait anxiety as an independent predictor of poor health-related quality of life and post-traumatic stress symptoms in rectal cancer. Br. J. Health Psychol. 2009, 14, 701–715. [Google Scholar] [CrossRef]
- Tejada, M.G.-S.d.; Bilbao, A.; Baré, M.; Briones, E.; Sarasqueta, C.; Quintana, J.M.; Escobar, A. Association between social support, functional status, and change in health-related quality of life and changes in anxiety and depression in colorectal cancer patients. Psychooncology 2017, 26, 1263–1269. [Google Scholar] [CrossRef]
- Thong, M.S.Y.; Doege, D.; Koch-Gallenkamp, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Waldeyer-Sauerland, M.; Waldmann, A.; Zeissig, S.R.; Brenner, H.; et al. Age at Diagnosis and Sex Are Associated with Long-term Deficits in Disease-Specific Health-Related Quality of Life of Survivors of Colon and Rectal Cancer: A Population-Based Study. Dis. Colon Rectum 2019, 62, 1294–1304. [Google Scholar] [CrossRef]
- Trinquinato, I.; Marques da Silva, R.; Ticona Benavente, S.B.; Antonietti, C.C.; Siqueira Costa Calache, A.L. Gender differences in the perception of quality of life of patients with colorectal cancer. Investig. Educ. Enferm. 2017, 35, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Yost, K.J.; Hahn, E.A.; Zaslavsky, A.M.; Ayanian, J.Z.; West, D.W. Predictors of health-related quality of life in patients with colorectal cancer. Health Qual. Life Outcomes 2008, 6, 66. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Sun, H. The longitudinal changes of anxiety and depression, their related risk factors and prognostic value in colorectal cancer survivors: A 36-month follow-up study. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101511. [Google Scholar] [CrossRef]
- Zimmaro, L.A.; Deng, M.Y.; Handorf, E.; Fang, C.Y.; Denlinger, C.S.; Reese, J.B. Understanding benefit finding among patients with colorectal cancer: A longitudinal study. Support. Care Cancer 2021, 29, 2355–2362. [Google Scholar] [CrossRef] [PubMed]
- JBI Manual for Evidence Synthesis. Available online: https://jbi-global-wiki.refined.site/space/MANUAL (accessed on 28 April 2021).
- Liberali, R.; Kupek, E.; Assis, M.A.A. Dietary Patterns and Childhood Obesity Risk: A Systematic Review. Child. Obes. 2020, 16, 70–85. [Google Scholar] [CrossRef]
- McCaughan, E.; Prue, G.; Parahoo, K.; McIlfatrick, S.; McKenna, H. Exploring and comparing the experience and coping behaviour of men and women with colorectal cancer at diagnosis and during surgery. J. Adv. Nurs. 2011, 67, 1591–1600. [Google Scholar] [CrossRef]
- McCaughan, E.; Prue, G.; Parahoo, K.; McIlfatrick, S.; McKenna, H. Exploring and comparing the experience and coping behaviour of men and women with colorectal cancer after chemotherapy treatment: A qualitative longitudinal study. Psychooncology 2012, 21, 64–71. [Google Scholar] [CrossRef]
- Eagly, A.H.; Wood, W. Social Role Theory. In Handbook of Theories of Social Psychology; Lange, P.A.M.V., Kruglanski, A.W., Higgins, E.T., Eds.; Sage Publications Ltd.: Thousand Oaks, CA, USA, 2012; Volume 2, pp. 458–476. [Google Scholar]
- Wall, D.; Kristjanson, L. Men, culture and hegemonic masculinity: Understanding the experience of prostate cancer. Nurs. Inq. 2005, 12, 87–97. [Google Scholar] [CrossRef]
- Nikita; Rani, R.; Kumar, R. Body image distress among cancer patients: Needs for psychosocial intervention development. Support. Care Cancer 2022, 30, 6035–6043. [Google Scholar] [CrossRef]
- Clarke, S.A.; Booth, L.; Velikova, G.; Hewison, J. Social support: Gender differences in cancer patients in the United Kingdom. Cancer Nurs. 2006, 29, 66–72. [Google Scholar] [CrossRef]
- Shi, P.; Yang, A.; Zhao, Q.; Chen, Z.; Ren, X.; Dai, Q. A Hypothesis of Gender Differences in Self-Reporting Symptom of Depression: Implications to Solve Under-Diagnosis and Under-Treatment of Depression in Males. Front. Psychiatry 2021, 12, 589687. [Google Scholar] [CrossRef] [PubMed]
- Zakowski, S.G.; Harris, C.; Krueger, N.; Laubmeier, K.K.; Garrett, S.; Flanigan, R.; Johnson, P. Social barriers to emotional expression and their relations to distress in male and female cancer patients. Br. J. Health Psychol. 2003, 8, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.E.; Bestmann, B.; Küchler, T.; Kremer, B. Factors influencing sexual function in patients with rectal cancer. Int. J. Impot. Res 2005, 17, 231–238. [Google Scholar] [CrossRef]
- Lange, M.M.; Marijnen, C.A.; Maas, C.P.; Putter, H.; Rutten, H.J.; Stiggelbout, A.M.; Meershoek-Klein Kranenbarg, E.; van de Velde, C.J. Risk factors for sexual dysfunction after rectal cancer treatment. Eur. J. Cancer 2009, 45, 1578–1588. [Google Scholar] [CrossRef]
- Tamres, L.K.; Janicki, D.; Helgeson, V.S. Sex differences in coping behavior: A meta-analytic review and an examination of relative coping. Personal. Soc. Psychol. Rev. 2002, 6, 2–30. [Google Scholar] [CrossRef]
- Emslie, C.; Browne, S.; Macleod, U.; Rozmovits, L.; Mitchell, E.; Ziebland, S. ‘Getting through’ not ‘going under’: A qualitative study of gender and spousal support after diagnosis with colorectal cancer. Soc. Sci. Med. 2009, 68, 1169–1175. [Google Scholar] [CrossRef]
- Manne, S.; Badr, H. Intimacy processes and psychological distress among couples coping with head and neck or lung cancers. Psychooncology 2010, 19, 941–954. [Google Scholar] [CrossRef]
- Manne, S.; Badr, H.; Kashy, D.A. A longitudinal analysis of intimacy processes and psychological distress among couples coping with head and neck or lung cancers. J. Behav. Med. 2012, 35, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Chen, X.; Wang, Z.; Li, Q. Couple-Based Communication Interventions for Cancer Patient-Spousal Caregiver Dyads’ Psychosocial Adaptation to Cancer: A Systematic Review. Healthcare 2023, 11, 236. [Google Scholar] [CrossRef]
- MacLean, A.; Hunt, K.; Smith, S.; Wyke, S. Does gender matter? An analysis of men’s and women’s accounts of responding to symptoms of lung cancer. Soc. Sci. Med. 2017, 191, 134–142. [Google Scholar] [CrossRef]
- Bowie, J.; Brunckhorst, O.; Stewart, R.; Dasgupta, P.; Ahmed, K. Body image, self-esteem, and sense of masculinity in patients with prostate cancer: A qualitative meta-synthesis. J. Cancer Surviv. 2022, 16, 95–110. [Google Scholar] [CrossRef] [PubMed]
- Aylaz, G.; Akyol, C.; Kocaay, A.F.; Gökmen, D.; Yavuzarslan, A.B.; Erkek, A.B.; Kuzu, M.A. Quality of life after colorectal surgery: A prospective study of patients compared with their spouses. World J. Gastrointest. Surg. 2021, 13, 1050–1062. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.W.; Paek, M.S.; Shon, E.J. Gender and Role Differences in Couples’ Communication during Cancer Survivorship. Cancer Nurs. 2015, 38, E51–E60. [Google Scholar] [CrossRef]
- Tuinstra, J.; Hagedoorn, M.; Van Sonderen, E.; Ranchor, A.V.; Van den Bos, G.A.; Nijboer, C.; Sanderman, R. Psychological distress in couples dealing with colorectal cancer: Gender and role differences and intracouple correspondence. Br. J. Health Psychol. 2004, 9, 465–478. [Google Scholar] [CrossRef] [PubMed]
- Nijboer, C.; Tempelaar, R.; Triemstra, M.; Sanderman, R.; van den Bos, G.A. Dynamics in cancer caregiver’s health over time: Gender-specific patterns and determinants. Psychol. Health 2001, 16, 471–488. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I.; Goldzweig, G.; Sela-Oren, T.; Pizem, N.; Bar-Sela, G.; Wolf, I. Attachment style, social support and finding meaning among spouses of colorectal cancer patients: Gender differences. Palliat. Support. Care 2015, 13, 527–535. [Google Scholar] [CrossRef]
- Badr, H. Couple Relationships and Cancer. In Psychological Aspects of Cancer: A Guide to Emotional and Psychological Consequences of Cancer, Their Causes, and Their Management; Steel, J.L., Carr, B.I., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 41–51. [Google Scholar]
- Donovan, E.E.; Kristen LeBlanc, F. Interpersonal Communication and Coping with Cancer: A Multidisciplinary Theoretical Review of the Literature. Commun. Theory 2019, 29, 236–256. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year) Country [Reference] | SD | No. of Participants (Distribution of Gender); Time Points/Intervals | Measurement Tools | Main Conclusions |
|---|---|---|---|---|
| Acevedo-Ibarra et al. (2021) Mexico [20] | C; Single-center | 192 CRC patients (90 women, 102 men); T: after diagnosis | -European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ)-C30 -EORTC QLQ-CR29 -Impact of Event Scale (IES) | -Psychological outcomes
|
| Akyol et al. (2015) Turkey [21] | C; Single-center | 105 colon cancer patients (33 women, 72 men); T: unclear | -Hospital Anxiety and Depression Scale (HADS) -EORTC QLQ-C30 -Golombok–Rust Inventory of Sexual Satisfaction (GRISS) | -Psychological outcomes
|
| Akyol et al. (2015) Turkey [22] | C; Single-center | 222 CRC patients (80 women, 142 men); T: unclear | -EORTC QLQ-C30 | -Psychological outcomes
|
| Al-Shandudi et al. (2022) Oman [23] | C; Multicenter | 118 CRC patients (59 women, 59 men); T: at least 6 months of survival left | -EORTC QLQ-CR 29 | -Psychological outcomes
|
| Alabbas et al. (2016) Saudi Arabia [24] | C; Single-center | 40 CRC patients (15 women, 25 men); T: unclear | -FACT-C | -Psychological outcomes
|
| Aminisani et al. (2021) Iran [25] | C; Single-center | 303 CRC patients (136 women, 167 men); T: regardless of stage or treatment | -HADS | -Psychological outcomes No gender difference existed in anxiety and depression. |
| Au et al. (2012) China [26] | C; Single-center | 120 rectal cancer patients (32 women, 88 men); T: after surgery | -Resourcefulness Scale (RS); -Body-Mind-Spirit Well-Being Inventory-Spirituality (BMSWBI-Spirituality) Scale | -Coping strategies
|
| Baldwin et al. (2009) USA [27] | C; Multicenter | 286 CRC patients (118 women, 168 men); T: at least 5 years of survival left | -The Short Form-36 (SF-36) | -Psychological outcomes
|
| Belachew et al. (2020) USA [28] | C; Single-center | 1132 CRC patients (492 women, 640 men); T: unclear | -SF-12 | -Psychological outcomes
|
| Braamse et al. (2016) The Netherlands [29] | C; Multicenter | 91 CRC patients (37 women, 54 men); T: 3.5 to 5 years after diagnosis | -Beck Anxiety Inventory (BAI); -Inventory of Depressive Symptomatology (IDS) | -Psychological outcomes
|
| Du et al. (2021) China [30] | C; Single-center | 390 CRC patients (159 women, 231 men); T: after colostomy | -Marital Adjustment Test (MAT); -Distress Disclosure Index Scale (DDI) -Ostomy adjustment inventory-20 scale (OAI-20) | -Social outcomes
|
| Dunn et al. (2013) Australia [31] | L; Single-center | 1703 CRC patients (680 women, 1023 men); T: at 5, 12, 24, 36, 48, 60 months after diagnosis | -The Brief Symptom Inventory (BSI) | -Psychological outcomes
|
| Eddington et al. (2021) USA [32] | C; Single-center | 238 CRC patients (98 women, 140 men) T: 3 months after treatment | -National Comprehensive Cancer Network (NCCN) Distress Thermometer -Impact Thermometer | -Psychological outcomes
|
| Eriksen et al. (2022) Norway [33] | C; Single-center | 54 CRC patients over 80 years old (37 women, 17 men) T: at least 1 year after surgery | -Sense of Coherence Scale (SOC); -Medical Outcomes Study–Social Support Survey (MOS-SSS) | -Coping strategies
|
| Gautam et al. (2016) Nepal [34] | C; Single-center | 122 CRC patients (60 women, 62 men); T: at least 6 months after colostomy | -Ostomy Adjustment Inventory-23 (OAI-23) | -Coping strategies
|
| Giesinger et al. (2009) Austria [35] | C; Multicenter | 206 CRC patients (97 women, 109 men); T: at least 3 months of survival left | -EORTC QLQ-C30 | -Psychological outcomes
|
| Goldzweig et al. (2009) Israel [36] | C; Multicenter | 339 CRC patients over 60 years old (153 women, 186 men); T: within 2 to 6 years after diagnosis | -BSI -IES -Cancer Perceived Agents of Social Support (CPASS) -Mental Adjustment to Cancer (MAC) | -Psychological outcomes
|
| Han et al. (2020) Germany [37] | L; Multicenter | 212 CRC patients (75 women, 137 men); T: at 6 and 12 months after surgery | -Cancer and Treatment Distress (CTXD) | -Psychological outcomes
|
| Kinoshita et al. (2015) Japan [38] | L; Multicenter | 75 rectal cancer patients (33 women, 42 men); T: before surgery and 1, 6, 12 months after surgery | -EORTC QLQ-C30 -EORTC QLQ-CR38 | -Psychological outcomes
|
| Laghousi et al. (2019) Iran [39] | C; Single-center | 303 CRC patients (136 women, 167 men); T: regardless of stage or treatment | -EORTC QLQ-C30 | -Psychological outcomes
|
| Mahjoubi et al. (2012) Iran [40] | C; Single-center | 96 CRC patients (54 women, 42 men); T: after surgery | -EORTC QLQ-C30 -EORTC QLQ-CR38 | -Psychological outcomes
|
| Milbury et al. (2013) USA [41] | C; Single-center | 261 CRC patients (117 women, 144 men); T: at least 6 months after surgery or at least 1 month after treatment | -Center for Epidemiological Studies Depression Scale (CES-D) -EORTC QLQ-CR38 -MOS-SSS -Abbreviated Dyadic Adjustment Scale (A-DAS) | -Psychological outcomes
|
| Mols et al. (2018) The Netherlands [11] | L; Multicenter | 2625 CRC patients (1178 women, 1447 men) T: in 2010, 2011, 2012, 2013 | -HADS | -Psychological outcomes
|
| Mrabti et al. (2016) Morocco [42] | L; Multicenter | 294 CRC patients (135 women, 159 men); T: within 3 months after diagnosis | -EORTC QLQ-C30 | -Psychological outcomes
|
| Palas et al. (2021) USA [43] | C; Single-center | 120 CRC patients (61 women, 59 men); T: within 6 to 36 months after treatment | -Fear of Cancer Recurrence Inventory (FCRI) | -Psychological outcomes
|
| Pereira et al. (2012) Brazil [44] | C; Single-center | 60 CRC patients (26 women, 34 men); T: unclear | -World Health Organization QOL Instrument (WHOQOL) | -Psychological outcomes
|
| Ran et al. (2016) China [45] | C; Single-center | 142 CRC patients (39 women, 103 men); T: 1 month after colostomy | -WHOQOL | -Psychological outcomes
|
| Reese et al. (2018) USA [12] | L; Single-center | 141 CRC patients (59 women, 82 men); T: within 5 years after diagnosis and 6-month follow-up | -CES-D -Body Image Scale (BIS) -The Index of Sexual Satisfaction (ISS) -DAS | -Psychological outcomes
|
| Repić et al. (2016) Serbia [46] | C; Single-center | 67 CRC patients (33 women, 34 men) T: after colostomy | -Quality of Life Questionnaire for a Patient with an Ostomy (QOL-O) | -Psychological outcomes
|
| Reyes et al. (2017) USA [47] | C; Single-center | 3734 CRC patients (1566 women, 2168 men); T: within 1 year after diagnosis | -SF-12 | -Psychological outcomes
|
| Ristvedt et al. (2009) USA [48] | L; Single-center | 80 rectal cancer patients (35 women, 45 men) T: soon after initial treatment and 2–5-year follow-up | -FACT-C | -Social outcomes
|
| Tejada et al. (2017) Spain [49] | L; Multicenter | 947 CRC patients (344 women, 603 men) T: before surgery and 12-month follow-up | -HADS | -Psychological outcomes
|
| Thong et al. (2019) Germany [50] | C; Multicenter | 1176 CRC patients (477 female, 699 male); T: within 5 to 16 years after diagnosis | -EORTC QLQ-CR29 | -Psychological outcomes
|
| Trinquinato et al. (2017) Brazil [51] | C; Single-center | 144 CRC patients (72 women, 72 men); T: undergoing chemotherapy treatment | -EORTC QLQ-C30; -EORTC QLQ-CR29 | -Psychological outcomes
|
| Yost et al. (2008) USA [52] | L; Multicenter | 568 CRC patients (unclear); T: at 9 and 19 months after diagnosis | -FACT-C | -Psychological outcomes
|
| Zhou et al. (2021) China [53] | L; Single-center | 302 CRC patients (132 women, 170 men); T: baseline (discharged from hospital), 1-, 2-, 3-year follow-up | -HADS | -Psychological outcomes
|
| Zimmaro et al. (2021) USA [54] | L; Single-center | 133 CRC patients (54 women, 79 men); T: baseline and 6-month follow-up | -Benefit Finding Scale | -Psychological outcomes
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, J.; Wang, Z.; Chen, X.; Li, Q. Gender Differences in Psychosocial Outcomes and Coping Strategies of Patients with Colorectal Cancer: A Systematic Review. Healthcare 2023, 11, 2591. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11182591
Zhou J, Wang Z, Chen X, Li Q. Gender Differences in Psychosocial Outcomes and Coping Strategies of Patients with Colorectal Cancer: A Systematic Review. Healthcare. 2023; 11(18):2591. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11182591
Chicago/Turabian StyleZhou, Junrui, Zhiming Wang, Xuan Chen, and Qiuping Li. 2023. "Gender Differences in Psychosocial Outcomes and Coping Strategies of Patients with Colorectal Cancer: A Systematic Review" Healthcare 11, no. 18: 2591. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11182591