
Variables Associated with Attitudes toward Biodebridement Using Lucilia sericata Larvae in a Group of Nurses
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Subjects
2.3. Research Tool
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Respondents
3.2. Perception of Wounds and Selected Variables
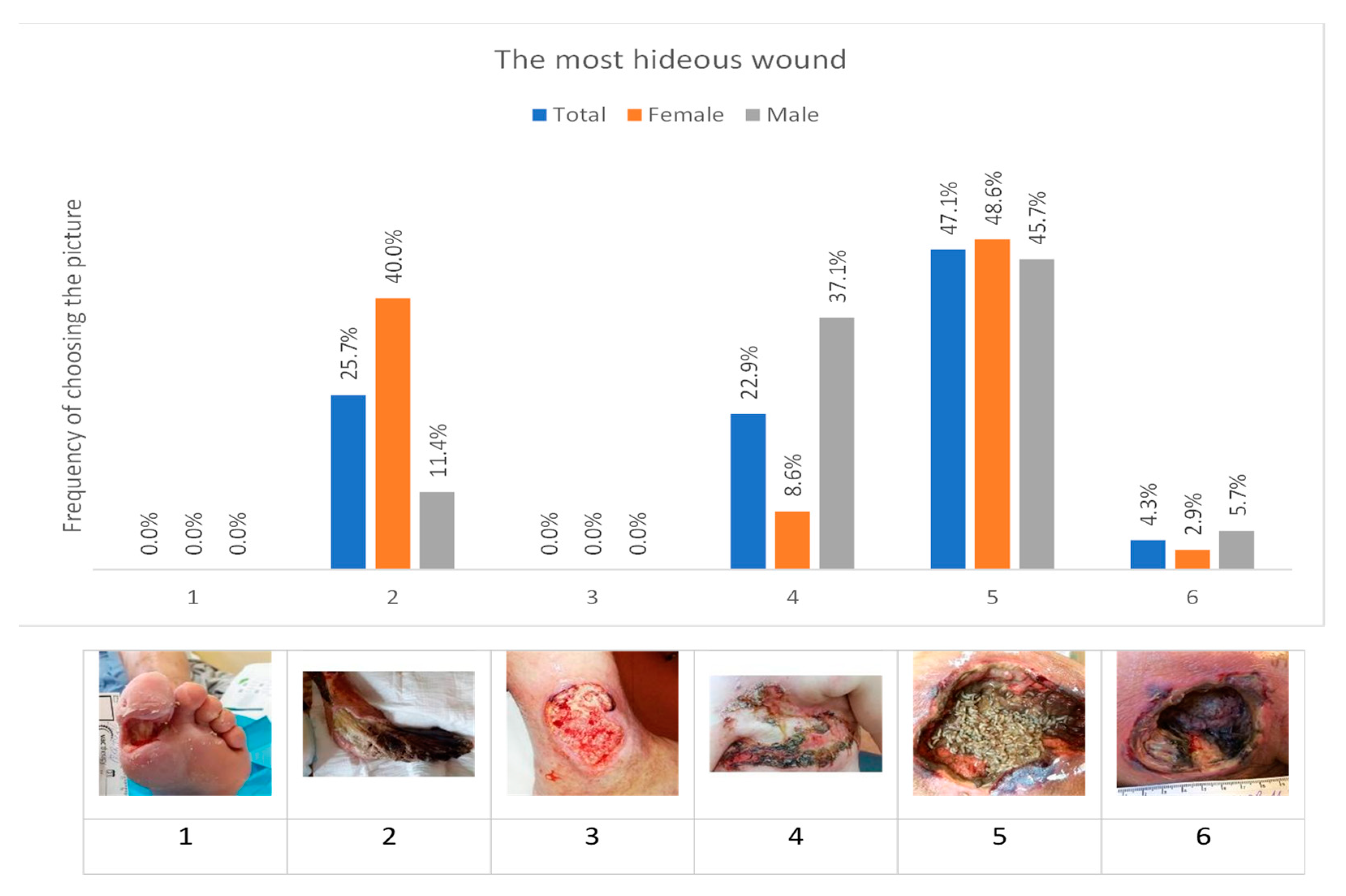
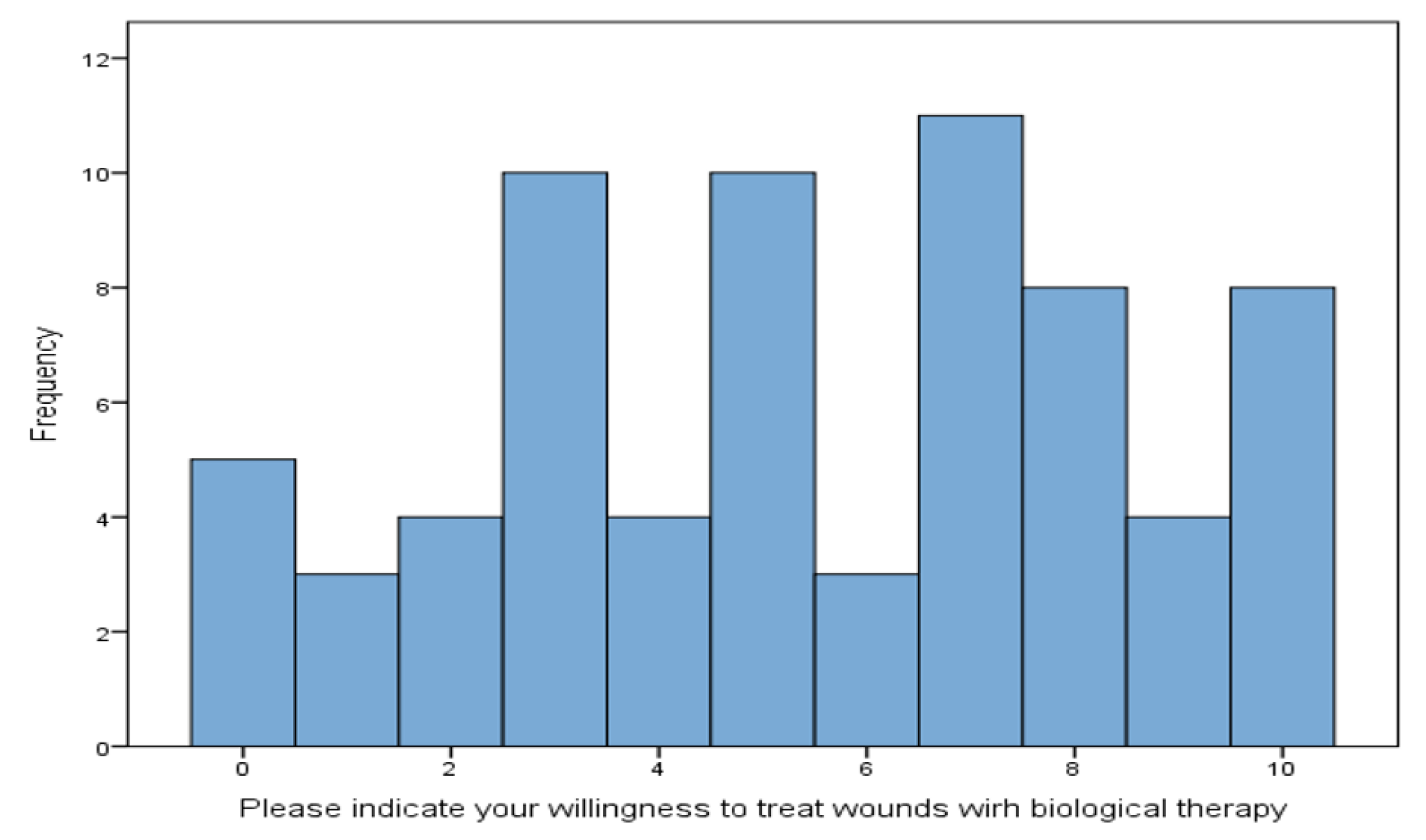
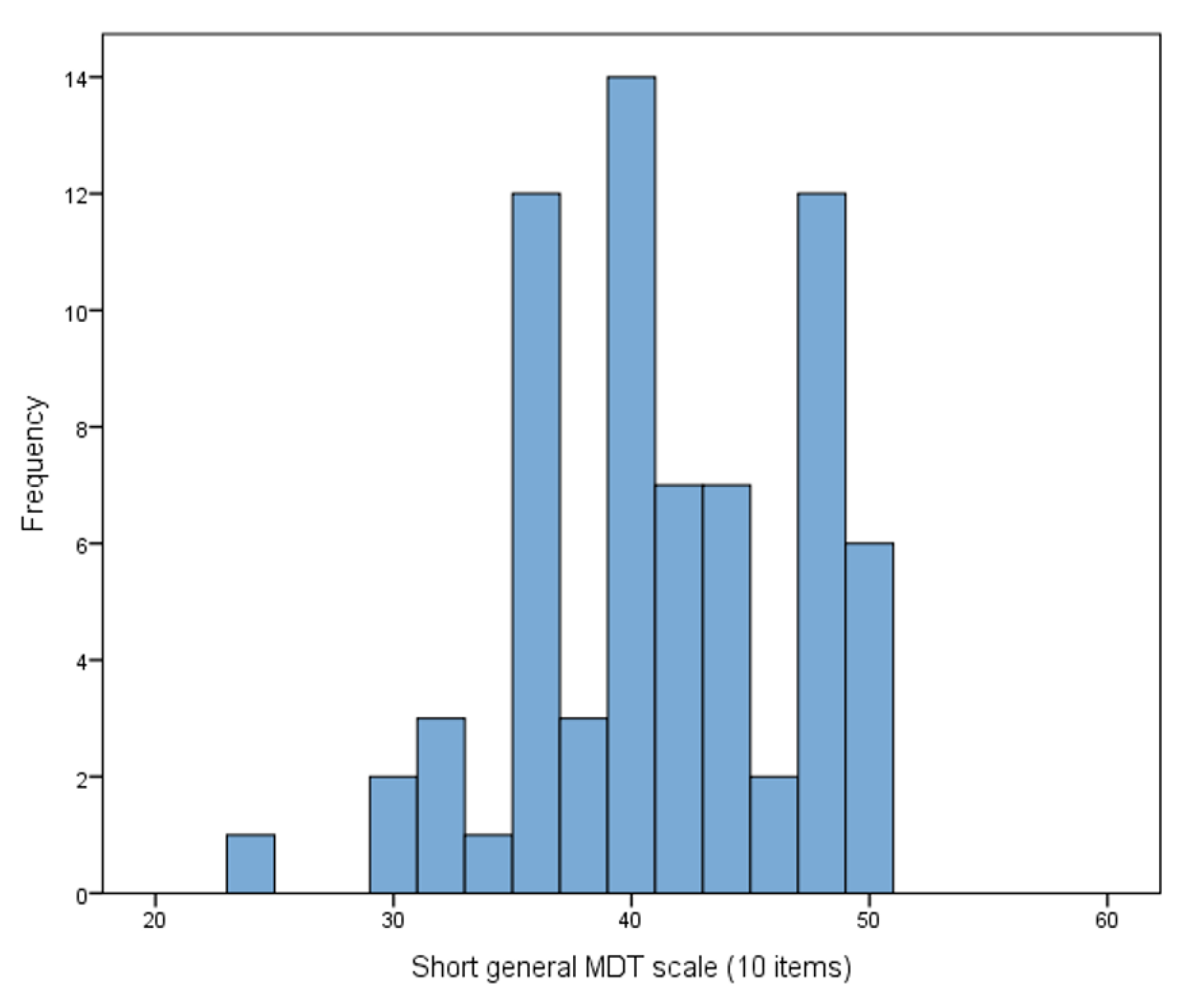
3.3. Perception of Wound Images and Readiness to Undertake MDT
3.4. Perceived Stress and the Perception of Wound Images
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sibbald, R.G.; Elliott, J.A.; Persaud-Jaimangal, R.; Goodman, L.; Armstrong, D.G.; Harley, C.; Coelho, S.; Xi, N.; Evans, R.; Mayer, D.O.; et al. Wound Bed Preparation 2021. Adv. Skin Wound Care 2021, 34, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Atkin, L.; Bućko, Z.; Conde-Montero, E.; Cutting, K.; Moffatt, C.; Probst, A.; Romanelli, M.; Schultz, G.S.; Tettelbach, W. Implementing TIMERS: The race against hard-to-heal wounds. J. Wound Care 2019, 28 (Suppl. S3), 1–49. [Google Scholar] [CrossRef] [PubMed]
- Cwajda-Białasik, J.; Mościcka, P.; Szewczyk, M. Antiseptics and antimicrobials for the treatment and management of chronic wounds: A systematic review of clinical trials. Adv. Dermatol. Allergol./Postępy Dermatol. Alergol. 2022, 39, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Malone, M.; Bjarnsholt, T.; McBain, A.J.; James, G.A.; Stoodley, P.; Leaper, D.; Tachi, M.; Schultz, G.; Swanson, T.; Wolcott, R.D. The prevalence of biofilms in chronic wounds: A systematic review and meta-analysis of published data. J. Wound Care 2017, 26, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Szewczyk, M.; Gospodarek, E.; Mościcka, P.; Jawień, A.; Cwajda-Białasik, J.; Cierzniakowska, K.; Hancke, E. Infections of chronic wounds—A serious medical problem. Pielęgniarstwo Chir. Angiol./Surg. Vasc. Nurs. 2015, 9, 1–6. [Google Scholar]
- Ciofu, O.; Rojo-Molinero, E.; Macià, M.D.; Oliver, A. Antibiotic treatment of biofilm infections. APMIS 2017, 125, 304–319. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Andersen, C.; Black, J.; de Leon, J.; Fife, C.; Lantis Ii, J.C.; Niezgoda, J.; Snyder, R.; Sumpio, B.; Tettelbach, W.; et al. Management of chronic wounds: Diagnosis, preparation, treatment, and follow-up. Wounds 2017, 29, 19–36. [Google Scholar]
- Sherman, R.A.; Pechter, E.A. Maggot therapy: A review of the therapeutic applications of fly larvae in human medicine, especially for treating osteomyelitis. Med. Vet. Entomol. 1988, 2, 225–230. [Google Scholar] [CrossRef]
- Kramer, A.; Dissemond, J.; Kim Willy, C.; Mayer, D.; Papke, R.; Tuchmann, F.; Assadian, O. Consensus on Wound antisepsis: Update 2018. Skin Pharmacol. Physiol. 2018, 31, 28–58. [Google Scholar] [CrossRef]
- Bazaliński, D.; Kózka, M.; Karnas, M.; Więch, P. Effectiveness of Chronic Wound Debridement with the Use of Larvae of Lucilia Sericata. J. Clin. Med. 2019, 8, 1845. [Google Scholar] [CrossRef]
- Szewczyk, M.; Cwajda-Białasik, J.; Mościcka, P.; Cierzniakowska, K.; Bazaliński, D.; Jawień, A.; Spannbauer, A.; Polak, A.; Sopata, M.; Kozłowska, E.; et al. Treatment of pressure ulcers—Recommendations of the Polish Wound Management Association. Part II Leczenie Ran 2020, 17, 151–184. [Google Scholar] [CrossRef]
- Moya-López, J.; Costela-Ruiz, V.; García-Recio, E.; Sherman, R.; De Luna-Bertos, E. Advantages of Maggot Debridement Therapy for Chronic Wounds: A Bibliographic Review. Adv. Skin. Wound Care 2020, 33, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Mrozikiewicz-Rakowska, B.; Tusiński, M.; Lipiński, P.; Bazaliński, D.; Dynarska, J.; Czwakiel, L.; Zymon, A.; Mospan, B.; Malinowska, K.; Sopata, M.; et al. Statement of the Polish Wound Management Association on larval therapy in wound management. Leczenie Ran 2023, 20, 89–95. [Google Scholar] [CrossRef]
- Mohd Zubir, M.Z.; Holloway, S.; Mohd Noor, N. Maggot Therapy in Wound Healing: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6103. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.; Flores, M.; Harris, L.; Gammon, J.; Nigam, Y. Larval Therapy and Larval Excretions/Secretions: A Potential Treatment for Biofilm in Chronic Wounds? A Systematic Review. Microorganisms 2023, 11, 457. [Google Scholar] [CrossRef]
- Przybek Mita, J.; Bazaliński, D.; Sztembis, R.; Kuberka, I.; Więch, P. Perceived stress and readiness to undertake biodebridement in the group of nurses undertaking prevention and treatment of chronic wounds. Front. Public Health 2022, 10, 1090677. [Google Scholar] [CrossRef]
- Babapour, A.R.; Gahassab-Mozaffari, N.; Fathnezhad-Kazemi, A. Nurses’ job stress and its impact on quality of life and caring behaviors: A cross-sectional study. BMC Nurs. 2022, 21, 75. [Google Scholar] [CrossRef]
- Woo, B.F.Y.; Lee, J.X.Y.; Tam, W.W.S. The impact of the advanced practice nursing role on quality of care, clinical outcomes, patient satisfaction, and cost in the emergency and critical care settings: A systematic review. Hum. Resour. Health 2017, 15, 63. [Google Scholar] [CrossRef]
- Kalisch, B.J.; Aebersold, M. Interruptions and multitasking in nursing care. Jt. Comm. J. Qual. Patient Saf. 2010, 36, 126–132. [Google Scholar] [CrossRef]
- Layali, I.; Ghajar, M.; Abedini, E.; Emadian, S.O.; Joulaei, M. Role of Job Stressors on Quality of Life in Nurses. J. Maz. Univ. Med. Sci. 2019, 29, 129–133. [Google Scholar]
- Bazaliński, D.; Przybek Mita, J.; Ścisło, L.; Więch, P. Perception and Readiness to Undertake Maggot Debridement Therapy with the Use of Lucilia sericata Larvae in the Group of Nurses. Int. J. Environ. Res. Public Health 2022, 19, 2895. [Google Scholar] [CrossRef]
- BioTherapeutics, Education and Research Foundation. BioTherapy Live! w/Prof. Bazaliński, Aneta Zymon, Paulina Szymańska, Anna Wójcik: “Women & Larvae”—10/11/2022. Facebook. Available online: https://www.facebook.com/watch/?v=2696341927164419 (accessed on 20 March 2023).
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Ogińska-Bulik, N.; Juczyński, Z. Narzędzia Pomiaru Stresu i Radzenie Sobie ze Stresem; Pracownia Testów Psychologicznych: Warszawa, Poland, 2009. [Google Scholar]
- Chokshi, A.; Sifri, Z.; Cennimo, D.; Horng, H. Global Contributors to Antibiotic Resistance. J. Glob. Infect. Dis. 2019, 11, 36–42. [Google Scholar]
- Strohal, R.; Dissemond, J.; Jordan O’Brien, J.; Piaggesi, A.; Rimdeika, R.; Young, T.; Apelqvist, J. EWMA document: Debridement. An updated overview and clarification of the principle role of debridement. J. Wound Care 2013, 22, 5. [Google Scholar] [CrossRef]
- Morozov, A.M.; Sherman, R.A. Survey of patients of the Tver region of Russia regarding maggots and maggot therapy. Int. Wound J. 2019, 16, 401–405. [Google Scholar] [CrossRef]
- Pajarillo, C.; Sherman, R.A.; Sheridan, R.; Kazis, L.E. Health professionals’ perceptions of maggot debridement therapy. J. Wound Care 2021, 30, VIIi–VIIxi. [Google Scholar] [CrossRef]
- Cwajda-Białasik, J.; Mościcka, P.; Szewczyk, M. Selected methods of treatment of chronic wounds. Pielęgniarstwo Chir. Angiol./Surg. Vasc. Nurs. 2019, 13, 1–11. [Google Scholar]
- Naik, G.; Harding, K.G. Maggot debridement therapy: The current perspectives. Chronic Wound Care Manag. Res. 2017, 4, 121–128. [Google Scholar] [CrossRef]
- Matchett, G.; Davey, G.C. A test of a disease-avoidance model of animal phobias. Behav. Res. Ther. 1991, 29, 91–94. [Google Scholar] [CrossRef]
- Huang, Y.; Mao, B.; Hu, J.; Xu, B.; Ni, P.; Hou, L.; Xie, T. Consensus on the health education of home-based negative pressure wound therapy for patients with chronic wounds: A modified Delphi study. Burns Trauma 2021, 9, tkab046. [Google Scholar] [CrossRef]
- Melnyk, B.M. The future of evidence-based health care and worldviews: A worldwide vision and call for action to improve healthcare quality, reliability and population health. Worldviews Evid. Based Nurs. 2013, 10, 127–128. [Google Scholar] [CrossRef]
- Squires, J.E.; Estabrooks, C.A.; Gustavsson, P.; Wallin, L. Individual determinants of research utilization by nurses: A systematic review update. Implement. Sci. 2011, 6, 1. [Google Scholar] [CrossRef]
- Banasiewicz, T.; Kobiela, J.; Cwaliński, J.; Spychalski, P.; Przybylska, P.; Kornacka, K.; Bogdanowska-Charkiewicz, D.; Leyk-Kolańczak, M.; Borejsza-Wysocki, M.; Batycka-Stachnik, D.; et al. Recommendations for the use of prehabilitation, or comprehensive preparation of the patient for surgery. Pol. Przegl Chir. 2023, 95, 62–91. [Google Scholar] [CrossRef]
- Romeyke, T. Maggot Therapy as a Part of a Holistic Approach in the Treatment of Multimorbid Patients with Chronic Ulcer. Clin. Pract. 2021, 11, 347–357. [Google Scholar] [CrossRef]
- Barker, E.; Kelly, P.W. Mentoring: A vital link in nurse practitioner development. J. Am. Assoc. Nurse Pract. 2020, 32, 621–625. [Google Scholar] [CrossRef]
- Brook, J.; Aitken, L.; Webb, R.; MacLaren, J.; Salmon, D. Characteristics of successful interventions to reduce turnover and increase retention of early career nurses: A systematic review. Int. J. Nurs. Stud. 2019, 91, 47–59. [Google Scholar] [CrossRef]
- Sherman, R.A. Mechanisms of Maggot-Induced Wound Healing: What Do We Know, and Where Do We Go from Here? Evid.-Based Complement. Altern. Med. 2014, 2014, 592419. [Google Scholar] [CrossRef]
- Contreras-Ruiz, J.; Fuentes-Suárez, A.; Arroyo-Escalante, S.; Moncada-Barron, D.; Sosa-de-Martínez, M.C.; Maravilla-Franco, E.; Domínguez-Cherit, J.G. Estudio comparativo de la eficacia de la larvaterapia (LT) para desbridar y controlar la carga bacteriana en úlceras venosas comparado con desbridamiento quirúrgico y aplicación de un antimicrobiano tópico [Comparative study of the efficacy of larva therapy for debridement and control of bacterial burden compared to surgical debridement and topical application of an antimicrobial]. Gac. Med. Mex. 2016, 152 (Suppl. S2), 78–87. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Males (N) | Females (N) | Total (N) | % of This Demographic | ||
|---|---|---|---|---|---|
| Total Subjects | 35 | 35 | 70 | 100.0% | |
| Age | 24–34 | 15 | 15 | 30 | 42.9% |
| 35–44 | 14 | 14 | 28 | 40.0% | |
| 45–54 | 4 | 4 | 8 | 11.4% | |
| 55–64 | 2 | 2 | 4 | 5.7% | |
| Age | Mean (SD) | 38.43 (8.441) | 38.34 (7.784) | 38.39 (8.060) | |
| Median (Range) | 38.00 (24–57) | 37.00 (26–57) | 38.00 (24–57) | ||
| Education | Registered nurse | 4 | 4 | 8 | 11.4% |
| Bachelor of nursing | 7 | 7 | 14 | 20.0% | |
| Master of nursing | 24 | 24 | 48 | 68.6% | |
| Work experience in the profession of a nurse | 1–5 years | 6 | 6 | 12 | 17.1% |
| 6–10 years | 6 | 6 | 12 | 17.1% | |
| 11–15 years | 9 | 9 | 18 | 25.7% | |
| 16–20 years | 6 | 6 | 12 | 17.1% | |
| 21–30 years | 6 | 6 | 12 | 17.1% | |
| More than 30 years | 2 | 2 | 4 | 5.7% | |
| Work experience (years) | Mean (SD) | 15.37 (8.630) | 13.63 (8.461) | 14.50 (8.529) | |
| Median (Range) | 14.00 (1–35) | 15.00 (2–36) | 14.50 (1–36) | ||
| Work Experience in the Profession of a Nurse | |||||||
|---|---|---|---|---|---|---|---|
| Total | 1–5 yrs | 6–10 yrs | 11–15 yrs | 16–20 yrs | ≥21 yrs | ||
| Photo 5 chosen as the most disgusting | N | 33 | 10 | 8 | 5 | 6 | 4 |
| % | 47.1% | 83.3% | 66.7% | 27.8% | 50.0% | 25.0% | |
| Other photo chosen as the most disgusting | N | 37 | 2 | 4 | 13 | 6 | 12 |
| % | 52.9% | 16.7% | 33.3% | 72.2% | 50.0% | 75.0% | |
| Total | N | 70 | 12 | 12 | 18 | 12 | 16 |
| % | 100.0% | 17.1% | 17.1% | 25.7% | 17.1% | 22.9% | |
| Total | Bachelor in Nursing | Master in Nursing | ||
|---|---|---|---|---|
| Photo 5 chosen as the most disgusting | N | 29 | 11 | 18 |
| % | 50.0% | 78.6% | 40.9% | |
| Other photo chosen as the most disgusting | N | 29 | 3 | 26 |
| % | 50.0% | 21.4% | 59.1% | |
| Total | N | 58 | 14 | 44 |
| % | 100.0% | 24.1% | 75.9% |
| Total | Self-Assessment of Readiness to Use Biological Therapy | |||
|---|---|---|---|---|
| Low (0–3) | Medium (4–7) | High (8–10) | ||
| Photo 5 selected as the most disgusting | 33 | 16 | 10 | 7 |
| 47.1% | 72.7% | 35.7% | 35.0% | |
| Other photo chosen as the most disgusting | 37 | 6 | 18 | 13 |
| 52.9% | 27.3% | 64.3% | 65.0% | |
| Total | 70 | 22 | 28 | 20 |
| 100.0% | 31.4% | 40.0% | 28.6% | |
| Scale MDT (10 Items) | Total | Woman | Man |
|---|---|---|---|
| Low result | 19 | 12 | 7 |
| 27.1% | 34.3% | 20.0% | |
| Medium result | 29 | 14 | 15 |
| 41.4% | 40.0% | 42.9% | |
| High result | 22 | 9 | 13 |
| 31.4% | 25.7% | 37.1% | |
| Total | 70 | 35 | 35 |
| 100.0% | 50.0% | 50.0% |
| Frequency of a “Most Disgusting” Rank | Total | Stress Intensity Level | ||
|---|---|---|---|---|
| Low Stress Level | Average Stress Level | High Stress Level | ||
| Photo 1 | 0 | 0 | 0 | 0 |
| 0.0% | 0.0% | 0.0% | 0.0% | |
| Photo 2 | 18 | 2 | 9 | 7 |
| 25.7% | 33.3% | 23.7% | 26.9% | |
| Photo 3 | 0 | 0 | 0 | 0 |
| 0.0% | 0.0% | 0.0% | 0.0% | |
| Photo 4 | 16 | 3 | 5 | 8 |
| 22.9% | 50.0% | 13.2% | 30.8% | |
| Photo 5 | 33 | 1 | 22 | 10 |
| 47.1% | 16.7% | 57.9% | 38.5% | |
| Photo 6 | 3 | 0 | 2 | 1 |
| 4.3% | 0.0% | 5.3% | 3.8% | |
| Total | 70 | 6 | 38 | 26 |
| 100.0% | 8.6% | 54.3% | 37.1% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bazaliński, D.; Pytlak, K.; Przybek-Mita, J.; Szymańska, P.; Wójcik, A.; Zymon, A.; Sherman, R.; Nguyen, A.; Sałacińska, I.; Więch, P. Variables Associated with Attitudes toward Biodebridement Using Lucilia sericata Larvae in a Group of Nurses. Healthcare 2023, 11, 3081. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11233081
Bazaliński D, Pytlak K, Przybek-Mita J, Szymańska P, Wójcik A, Zymon A, Sherman R, Nguyen A, Sałacińska I, Więch P. Variables Associated with Attitudes toward Biodebridement Using Lucilia sericata Larvae in a Group of Nurses. Healthcare. 2023; 11(23):3081. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11233081
Chicago/Turabian StyleBazaliński, Dariusz, Kamila Pytlak, Joanna Przybek-Mita, Paulina Szymańska, Anna Wójcik, Aneta Zymon, Ronald Sherman, Albert Nguyen, Izabela Sałacińska, and Paweł Więch. 2023. "Variables Associated with Attitudes toward Biodebridement Using Lucilia sericata Larvae in a Group of Nurses" Healthcare 11, no. 23: 3081. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11233081