
The Immediate Effects of Muscle Energy Technique in Chronic Low Back Pain Patients with Functional Leg Length Discrepancy: A Randomized and Placebo-Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
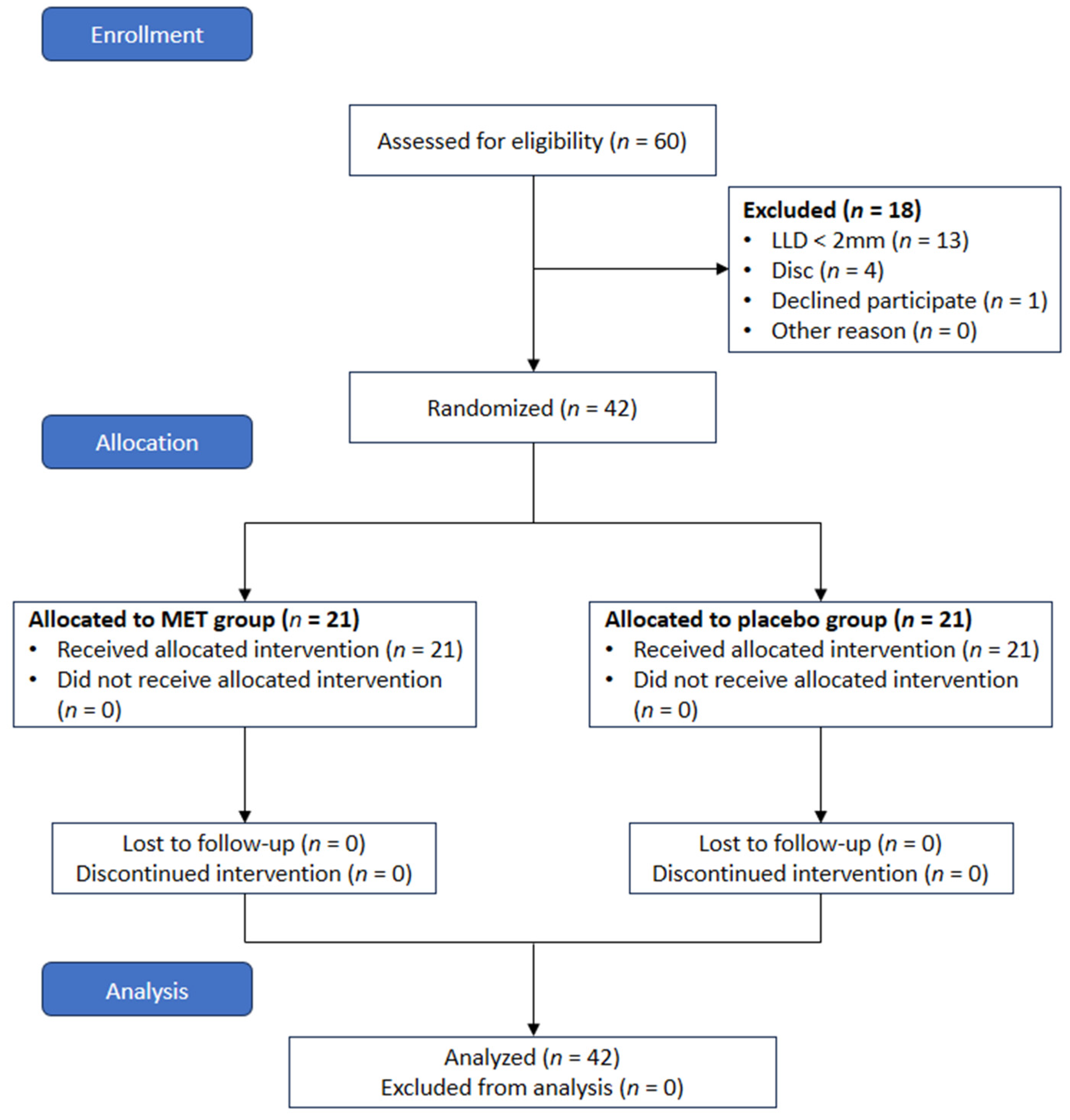
2.1. Participants
2.2. Experimental Procedure
2.3. Intervention
2.3.1. MET Group
2.3.2. Placebo Group
2.4. Outcome Measurements
2.4.1. Pelvic Alignment
2.4.2. Leg Length
2.4.3. Pain and Fatigue
2.5. Data Analysis
3. Results
3.1. Characteristics of Participants
3.2. Leg Length Discrepancy
3.3. Pelvic Alignment
3.4. Pain and Fatigue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vujcic, I.; Stojilovic, N.; Dubljanin, E.; Ladjevic, N.; Ladjevic, I.; Sipetic-Grujicic, S. Low back pain among medical students in belgrade (Serbia): A cross-sectional study. Pain Res. Manag. 2018, 6, 8317906. [Google Scholar] [CrossRef]
- Yang, J.H.; Suk, K.S.; Lee, B.H.; Jung, W.C.; Kang, Y.M.; Kim, J.H.; Kim, H.S.; Lee, H.M.; Moon, S.H. Efficacy and safety of different aceclofenac treatments for chronic lower back pain: Prospective, randomized, single center, open-label clinical trials. Yonsei Med. J. 2017, 58, 637–643. [Google Scholar] [CrossRef]
- Park, T.S.W.; Kuo, A.; Smith, M.T. Chronic low back pain: A mini-review on pharmacological management and pathophysiological insights from clinical and pre-clinical data. Inflammopharmacology 2018, 26, 881–898. [Google Scholar] [CrossRef]
- Kawada, T.; Suzuki, S. Physical symptoms and psychological health status by the type of job. Work 2008, 31, 397–403. [Google Scholar]
- Witt, C.M.; Pach, D.; Reinhold, T.; Wruck, K.; Brinkhaus, B.; Mank, S.; Willich, S.N. Treatment of the adverse effects from acupuncture and their economic impact: A prospective study in 73,406 patients with low back or neck pain. Eur. J. Pain 2011, 15, 193–197. [Google Scholar] [CrossRef]
- Andrade, N.S.; Flynn, J.P.; Bartanusz, V. Twenty-year perspective of randomized controlled trials for surgery of chronic nonspecific low back pain: Citation bias and tangential knowledge. Spine J. 2013, 13, 1698–1704. [Google Scholar] [CrossRef]
- Eckard, V.R.; Batinitzky, S.; Abrams, B.M.; Eckard, D.A. Radiology and the diagnosis and management of pain. In Practical Management of Pain, 3rd ed.; Raj, P.P., Ed.; Mosby: St Louis, MO, USA, 2000; pp. 338–407. [Google Scholar]
- Levangie, P.K. The association between static pelvic asymmetry and low back pain. Spine 1999, 24, 1234–1242. [Google Scholar] [CrossRef]
- Fann, A.V. The prevalence of postural asymmetry in people with and without chronic low back pain. Arch. Phys. Med. Rehabil. 2002, 83, 1736–1738. [Google Scholar] [CrossRef]
- Yu, Q.; Huang, H.; Zhang, Z.; Hu, X.; Li, W.; Li, L.; Chen, M.; Liang, Z.; Lo, W.L.A.; Wang, C. The association between pelvic asymmetry and non-specific chronic low back pain as assessed by the global postural system. BMC Musculoskelet. Disord. 2020, 21, 596. [Google Scholar] [CrossRef]
- Knutson, G.A. Anatomic and functional leg-length inequality: A review and recommendation for clinical decision-making. Part I, anatomic leg-length inequality: Prevalence, magnitude, effects and clinical significance. Chiropr. Osteopat. 2005, 13, 11. [Google Scholar] [CrossRef]
- Ten Brinke, A.; van der Aa, H.E.; van der Palen, J.; Oosterveld, F. Is leg length discrepancy associated with the side of radiating pain in patients with a lumbar herniated disc? Spine 1999, 24, 684–686. [Google Scholar] [CrossRef] [PubMed]
- Cummings, G.; Scholz, J.P.; Barnes, K. The effect of imposed leg length difference on pelvic bone symmetry. Spine 1993, 18, 368–373. [Google Scholar] [CrossRef]
- Gofton, J.P. Persistent low back pain and leg length disparity. J. Rheumatol. 1985, 12, 747–750. [Google Scholar]
- Friberg, O. Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality. Spine 1983, 8, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Resende, R.A.; Kirkwood, R.N.; Deluzio, K.J.; Cabral, S.; Fonseca, S.T. Biomechanical strategies implemented to compensate for mild leg length discrepancy during gait. Gait Posture 2016, 46, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Oleksy, Ł.; Mika, A.; Kielnar, R.; Grzegorczyk, J.; Marchewka, A.; Stolarczyk, A. The influence of pelvis reposition exercises on pelvic floor muscles asymmetry: A randomized prospective study. Medicine 2019, 98, e13988. [Google Scholar] [CrossRef]
- Gnat, R.; Saulicz, E. Induced static asymmetry of the pelvis is associated with functional asymmetry of the lumbo-pelvo-hip complex. J. Manip. Physiol. Ther. 2008, 31, 204–211. [Google Scholar] [CrossRef]
- Lee, J.H.; Yoo, W.G. Application of posterior pelvic tilt taping for the treatment of chronic low back pain with sacroiliac joint dysfunction and increased sacral horizontal angle. Phys. Ther. Sport 2012, 13, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.; Payton, O.; Donegan-Shoaf, L.; Dec, K. Muscle energy technique in patients with acute low back pain: A pilot clinical trial. J. Orthop. Sports Phys. Ther. 2003, 33, 502–512. [Google Scholar] [CrossRef] [PubMed]
- Lisa, A. Greenman’s Principles of Manual Medicine, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; p. 401. [Google Scholar]
- Thomas, E.; Cavallaro, A.R.; Mani, D.; Bianco, A.; Palma, A. The efficacy of muscle energy techniques in symptomatic and asymptomatic subjects: A systematic review. Chiropr. Man. Ther. 2019, 27, 35. [Google Scholar] [CrossRef]
- Santos, G.K.; Gonçalves de Oliveira, R.; Campos de Oliveira, L.; Ferreira C de Oliveira, C.; Andraus, R.A.; Ngomo, S.; Fusco, A.; Cortis, C.; DA Silva, R.A. Effectiveness of muscle energy technique in patients with nonspecific low back pain: A systematic review with meta-analysis. Eur. J. Phys. Rehabil. Med. 2022, 58, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Malarvizhi, D.; Harshavardhan, S.; Sivakumar, V.P.R. Effectiveness of muscle energy technique to quadratus lumborum for treating innominate up-slip sacroiliac joint dysfunction: A single case study. Int. J. Clin. Ski. 2017, 11, 65–67. [Google Scholar]
- Patel, V.D.; Eapen, C.; Ceepee, Z.; Kamath, R. Effect of muscle energy technique with and without strain-counterstrain technique in acute low back pain—A randomized clinical trial. Hong Kong Physiother. J. 2018, 38, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Szulc, P.; Wendt, M.; Waszak, M.; Tomczak, M.; Cieślik, K.; Trzaska, T. Impact of McKenzie method therapy enriched by muscular energy techniques on subjective and objective parameters related to spine function in patients with chronic low back pain. Med. Sci. Monit. 2015, 21, 2918–2932. [Google Scholar] [CrossRef] [PubMed]
- Saghaei, M. Random allocation software for parallel group randomized trials. BMC Med. Res. Methodol. 2004, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Betsch, M.; Rapp, W.; Przibylla, A.; Jungbluth, P.; Hakimi, M.; Schneppendahl, J.; Thelen, S.; Wild, M. Determination of the amount of leg length inequality that alters spinal posture in healthy subjects using rasterstereography. Eur. Spine J. 2013, 22, 1354–1361. [Google Scholar] [CrossRef]
- Kjellberg, M.; Al-Amiry, B.; Englund, E.; Sjödén, G.O.; Sayed-Noor, A.S. Measurement of leg length discrepancy after total hip arthroplasty. The reliability of a plain radiographic method compared to CT-scanogram. Skelet. Radiol. 2012, 41, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Friberg, O.; Koivisto, E.; Wegelius, C. A radiographic method for measurement of leg length inequality. Diagn. Imaging Clin. Med. 1985, 54, 78–81. [Google Scholar]
- Terry, M.A.; Winell, J.J.; Green, D.W.; Schneider, R.; Peterson, M.; Marx, R.G.; Widmann, R.F. Measurement variance in limb length discrepancy: Clinical and radiographic assessment of interobserver and intraobserver variability. J. Pediatr. Orthop. 2005, 25, 197–201. [Google Scholar] [CrossRef]
- Neelly, K.; Wallmann, H.W.; Backus, C.J. Validity of measuring leg length with a tape measure compared to a computed tomography scan. Physiother. Theory Pract. 2013, 29, 487–492. [Google Scholar] [CrossRef]
- Wagner, D.R.; Tatsugawa, K.; Parker, D.; Young, T.A. Reliability and utility of a visual analog scale for the assessment of acute mountain sickness. High Alt. Med. Biol. 2007, 8, 27–31. [Google Scholar] [CrossRef]
- Neumann, D.A. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation, 2nd ed.; Mosby: Maryland Heights, MO, USA, 2009. [Google Scholar]
- Franke, H.; Fryer, G.; Ostelo, R.W.; Kamper, S.J. Muscle energy technique for non-specific low-back pain. Cochrane Database Syst. Rev. 2015, 2, CD009852. [Google Scholar] [CrossRef] [PubMed]
- Houk, J.; Henneman, E. Responses of Golgi tendon organs to active contractions of the soleus muscle of the cat. J. Neurophysiol. 1967, 30, 466–481. [Google Scholar] [CrossRef] [PubMed]
- Knutson, G.A. Incidence of foot rotation, pelvic crest unleveling, and supine leg length alignment asymmetry and their relationship to self-reported back pain. J. Manip. Physiol. Ther. 2002, 25, 110E. [Google Scholar] [CrossRef] [PubMed]
- Hägg, O.; Fritzell, P.; Nordwall, A. The clinical importance of changes in outcome scores after treatment for chronic low back pain. Eur. Spine J. 2003, 12, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P. Sacroiliac joint pain: A comprehensive review of anatomy, diagnosis, and treatment. Anesth. Analg. 2005, 101, 1440–1453. [Google Scholar] [CrossRef]
- Cibulka, M.T.; Delitto, A.; Koldehoff, R.M. Changes in innominate tilt after manipulation of the sacroiliac joint in patients with low back pain. An experimental study. Phys. Ther. 1988, 68, 1359–1363. [Google Scholar] [CrossRef]
- Childs, J.D.; Piva, S.R.; Erhard, R.E. Immediate improvements in side-to-side weight bearing and iliac crest symmetry after manipulation in patients with low back pain. J. Manip. Physiol. Ther. 2004, 27, 306–313. [Google Scholar] [CrossRef]
- Levangie, P.K.; Norkin, C.C. Joint Structure and Function: A Comprehensive Analysis; FA Davis: Philadelphia, PA, USA, 2011. [Google Scholar]
- Selkow, N.M.; Grindstaff, T.L.; Cross, K.M.; Pugh, K.; Hertel, J.; Saliba, S. Short-term effect of muscle energy technique on pain in individuals with non-specific lumbopelvic pain: A pilot study. J. Man. Manip. Ther. 2009, 17, E14–E18. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | MET Group | Placebo MET Group | p-Value |
|---|---|---|---|
| * Male/Female (n) | 13/8 | 12/9 | 0.753 a |
| Age (year) | 31.14 ± 5.46 | 33.67 ± 5.66 | 0.149 b |
| Height (cm) | 168.33 ± 7.52 | 170.30 ± 7.69 | 0.408 b |
| Weight (kg) | 66.83 ± 12.35 | 65.52 ± 10.16 | 0.822 b |
| BMI (kg/m2) | 23.78 ± 5.08 | 22.79 ± 4.50 | 0.538 b |
| TMM | |||
| SLLD (mm) | 0.24 ± 0.16 | 0.28 ± 0.18 | 0.434 b |
| FLLD (mm) | 2.29 ± 0.22 | 2.33 ± 0.28 | 0.552 b |
| Radiography | |||
| HL-HI (mm) | 5.61 ± 4.59 | 5.74 ± 2.83 | 0.911 b |
| HL-HH (mm) | 3.96 ± 2.21 | 4.55 ± 2.10 | 0.588 b |
| HL-BI (mm) | 4.07 ± 2.17 | 3.84 ± 2.00 | 0.544 b |
| Obliquity (°) | 3.14 ± 1.19 | 2.70 ± 1.10 | 0.227 b |
| VAS | |||
| Pain (mm) | 43.15 ± 15.99 | 45.62 ± 13.16 | 0.588 b |
| Fatigue (mm) | 47.81 ± 19.49 | 47.95 ± 22.26 | 0.982 b |
| Variables | Pre | Post | Source | F (df) | p | Partial η2 |
|---|---|---|---|---|---|---|
| FLLD (mm) | ||||||
| MET group | 2.29 ± 0.22 | 0.45 ± 0.21 a,* | Time | 269.168 (1) | <0.001 | 0.87 |
| Placebo group | 2.33 ± 0.28 | 2.26 ± 0.58 | Group | 86.998 (1) | <0.001 | 0.69 |
| T*G | 229.608 (1) | <0.001 | 0.85 | |||
| HL-HI (mm) | ||||||
| MET group | 5.61 ± 4.59 | 3.83 ± 3.37 a | Time | 26.525 (1) | <0.001 | 0.40 |
| Placebo group | 5.74 ± 2.83 | 5.64 ± 2.59 | Group | 0.862 (1) | 0.359 | 0.02 |
| T*G | 20.969 (1) | <0.001 | 0.34 | |||
| HL-HH (mm) | ||||||
| MET group | 3.96 ± 2.21 | 2.96 ± 1.85 a,* | Time | 8.243 (1) | 0.007 | 0.17 |
| Placebo group | 4.55 ± 2.1 | 4.42 ± 2.04 | Group | 2.905 (1) | 0.096 | 0.07 |
| T*G | 4.783 (1) | 0.035 | 0.11 | |||
| HL-BI (mm) | ||||||
| MET group | 4.07 ± 2.17 | 2.79 ± 1.86 a | Time | 5.561 (1) | 0.023 | 0.12 |
| Placebo group | 3.84 ± 2 | 3.79 ± 2.52 | Group | 0.409 (1) | 0.526 | 0.01 |
| T*G | 4.735 (1) | 0.036 | 0.11 | |||
| Obliquity (°) | ||||||
| MET group | 3.14 ± 1.19 | 1.61 ± 1.09 a,* | Time | 65.024 (1) | <0.001 | 0.62 |
| Placebo group | 2.70 ± 1.10 | 2.49 ± 1.11 | Group | 0.475 (1) | 0.495 | 0.01 |
| T*G | 37.660 (1) | <0.001 | 0.49 |
| Variables | Pre | Post | Source | F (df) | p | Partial η2 |
|---|---|---|---|---|---|---|
| Pain (mm) | ||||||
| MET group | 43.15 ± 15.99 | 21.94 ± 14.34 a,* | Time | 159.099 (1) | <0.001 | 0.80 |
| Placebo group | 45.62 ± 13.16 | 44.38 ± 14.33 | Group | 8.078 (1) | 0.007 | 0.17 |
| T*G | 125.943 (1) | <0.001 | 0.76 | |||
| Fatigue (mm) | ||||||
| MET group | 47.81 ± 19.49 | 22.76 ± 13.51 a,* | Time | 56.153 (1) | <0.001 | 0.58 |
| Placebo group | 47.95 ± 22.26 | 45.48 ± 23.25 | Group | 3.766 (1) | 0.059 | 0.09 |
| T*G | 37.764 (1) | <0.001 | 0.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, J.-D.; Jung, J.-H.; Cho, H.-Y.; Shin, H.-J. The Immediate Effects of Muscle Energy Technique in Chronic Low Back Pain Patients with Functional Leg Length Discrepancy: A Randomized and Placebo-Controlled Trial. Healthcare 2024, 12, 53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12010053
Yoon J-D, Jung J-H, Cho H-Y, Shin H-J. The Immediate Effects of Muscle Energy Technique in Chronic Low Back Pain Patients with Functional Leg Length Discrepancy: A Randomized and Placebo-Controlled Trial. Healthcare. 2024; 12(1):53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12010053
Chicago/Turabian StyleYoon, Jung-Dae, Jin-Hwa Jung, Hwi-Young Cho, and Ho-Jin Shin. 2024. "The Immediate Effects of Muscle Energy Technique in Chronic Low Back Pain Patients with Functional Leg Length Discrepancy: A Randomized and Placebo-Controlled Trial" Healthcare 12, no. 1: 53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12010053