Effects of Muscle Strengthening around the Hip on Pain, Physical Function, and Gait in Elderly Patients with Total Knee Arthroplasty: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
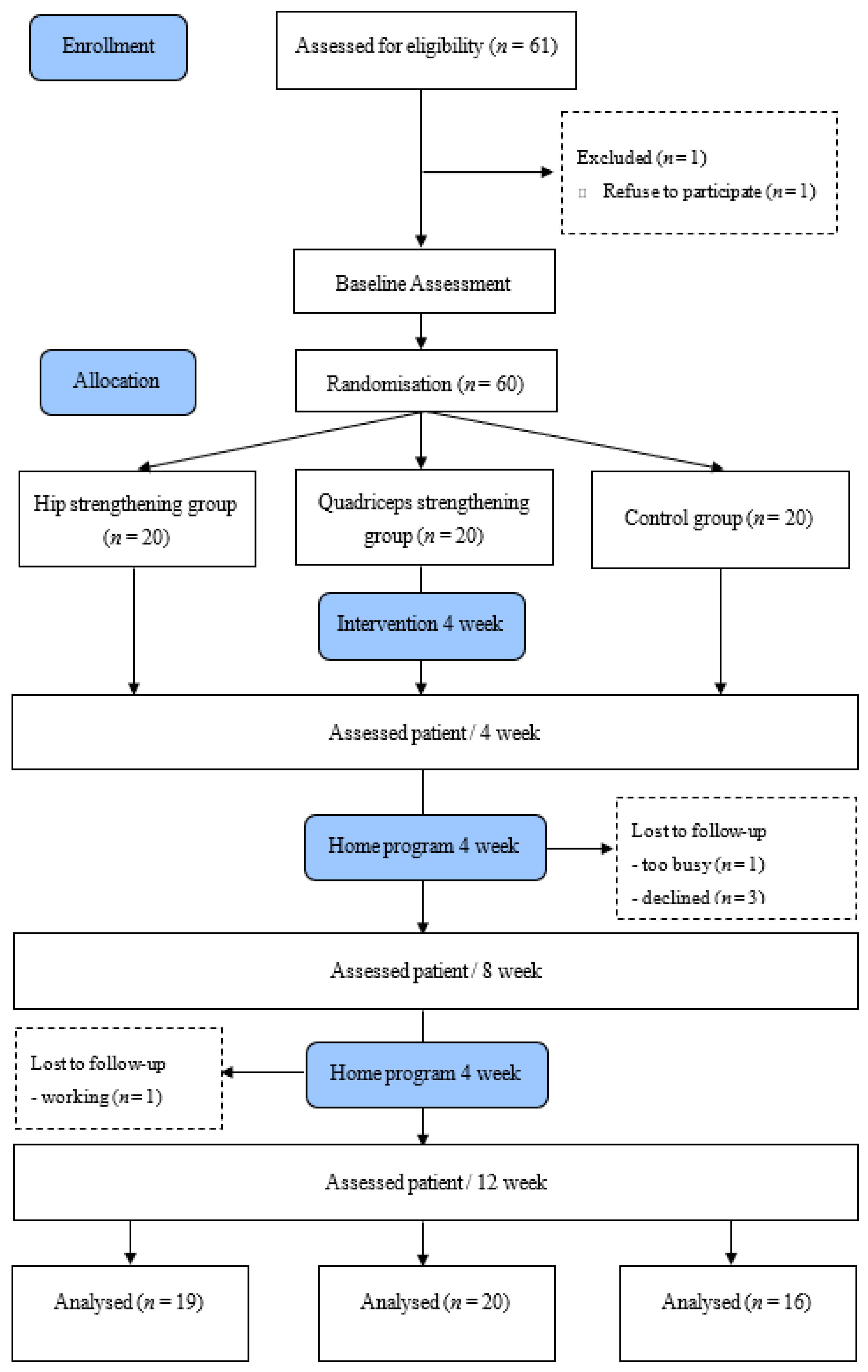
2.2. Randomization and Allocation Concealment
2.3. Procedure
2.4. Participants
2.5. Intervention
2.5.1. Hip Muscle Group (A)
2.5.2. Quadriceps Muscle Group (B)
2.5.3. Control Group (C)
2.6. Outcome Measure
2.6.1. Range of Motion (ROM)
2.6.2. Alternative Step Test (AST)
2.6.3. Five Times Sit to Stand Test (FTSST)
2.6.4. Times up and Go (TUG)
2.6.5. Six Meter Walking Test (6MWT)
2.6.6. Single Leg Stance (SLS)
2.6.7. Gait Analysis
2.6.8. Self-Reported Symptoms and Functional Status
2.7. Sample Size Calculations
2.8. Data and Statistical Analysis
3. Results
3.1. Pain and Range of Motion
3.2. Physical Function
3.3. Gait Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Felson, D.T.; Naimark, A.; Anderson, J.; Kazis, L.; Castelli, W.; Meenan, R.F. The prevalence of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study. Arthritis Rheum. 1987, 30, 914–918. [Google Scholar] [CrossRef]
- National Health Insurance Corporation. Health Insurance Major Surgery Statistics. Ranked 20th by Frequent Surgical Disease. Available online: https://kosis.kr/index/index.do.
- Bade, M.J.; Kohrt, W.M.; Stevens-Lapsley, J.E. Outcomes before and after total knee arthroplasty compared to healthy adults. J. Orthop. Sports Phys. Ther. 2010, 40, 559–567. [Google Scholar] [CrossRef] [Green Version]
- Walsh, M.; Woodhouse, L.J.; Thomas, S.G.; Finch, E. Physical impairments and functional limitations: A comparison of individuals 1 year after total knee arthroplasty with control subjects. Phys. Ther. 1998, 78, 248–258. [Google Scholar] [CrossRef]
- Blue, C.; Coomes, S.; Yoshida, Y. A Novel Downhill Gait-Training Program Following a Total Knee Arthroplasty: A Case Report Highlighting the Impacts of Self-selected Speed on Gait Symmetry. J. Orthop. Sports Phys. Ther. 2018, 48, 104–110. [Google Scholar] [CrossRef]
- Levinger, P.; Menz, H.B.; Morrow, A.D.; Wee, E.; Feller, J.A.; Bartlett, J.R.; Bergman, N. Lower limb proprioception deficits persist following knee replacement surgery despite improvements in knee extension strength. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1097–1103. [Google Scholar] [CrossRef]
- Hinman, R.S.; Hunt, M.A.; Creaby, M.W.; Wrigley, T.V.; McManus, F.J.; Bennell, K.L. Hip muscle weakness in individuals with medial knee osteoarthritis. Arthritis Care Res. 2010, 62, 1190–1193. [Google Scholar] [CrossRef] [PubMed]
- Childs, J.D.; Sparto, P.J.; Fitzgerald, G.K.; Bizzini, M.; Irrgang, J.J. Alterations in lower extremity movement and muscle activation patterns in individuals with knee osteoarthritis. Clin. Biomech. 2004, 19, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Al-Zahrani, K.; Bakheit, A. A study of the gait characteristics of patients with chronic osteoarthritis of the knee. Disabil. Rehabil. 2002, 24, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Farr, J.N.; Going, S.B.; Lohman, T.G.; Rankin, L.; Kasle, S.; Cornett, M.; Cussler, E. Physical activity levels in patients with early knee osteoarthritis measured by accelerometry. Arthritis Care Res. 2008, 59, 1229–1236. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.; Hayes, K.; Dunlop, D.; Song, J.; Hurwitz, D.; Cahue, S.; Sharma, L. Hip abduction moment and protection against medial tibiofemoral osteoarthritis progression. Arthritis Rheum. 2005, 52, 3515–3519. [Google Scholar] [CrossRef]
- Mündermann, A.; Asay, J.L.; Mündermann, L.; Andriacchi, T.P. Implications of increased medio-lateral trunk sway for ambulatory mechanics. J. Biomech. 2008, 41, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Mündermann, A.; Dyrby, C.O.; Andriacchi, T.P. Secondary gait changes in patients with medial compartment knee osteoarthritis: Increased load at the ankle, knee, and hip during walking. Arthritis Rheum. 2005, 52, 2835–2844. [Google Scholar] [CrossRef] [PubMed]
- Yamada, H.; Koshino, T.; Sakai, N.; Saito, T. Hip adductor muscle strength in patients with varus deformed knee. Clin. Orthop. Relat. Res. 2001, 386, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Oliver, G.D.; Dwelly, P.M.; Sarantis, N.D.; Helmer, R.A.; Bonacci, J.A. Muscle activation of different core exercises. J. Strength Cond. Res. 2010, 24, 3069–3074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sled, E.A.; Khoja, L.; Deluzio, K.J.; Olney, S.J.; Culham, E.G. Effect of a home program of hip abductor exercises on knee joint loading, strength, function, and pain in people with knee osteoarthritis: A clinical trial. Phys. Ther. 2010, 90, 895–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennell, K.; Hunt, M.; Wrigley, T.; Hunter, D.; McManus, F.; Hodges, P.; Li, L.; Hinman, R. Hip strengthening reduces symptoms but not knee load in people with medial knee osteoarthritis and varus malalignment: A randomised controlled trial. Osteoarthr. Cartil. 2010, 18, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Alnahdi, A.H.; Zeni, J.A.; Snyder-Mackler, L. Hip abductor strength reliability and association with physical function after unilateral total knee arthroplasty: A cross-sectional study. Phys. Ther. 2014, 94, 1154–1162. [Google Scholar] [CrossRef] [Green Version]
- Loyd, B.J.; Jennings, J.M.; Judd, D.L.; Kim, R.H.; Wolfe, P.; Dennis, D.A.; Stevens-Lapsley, J.E. Influence of hip abductor strength on functional outcomes before and after total knee arthroplasty: Post hoc analysis of a randomized controlled trial. Phys. Ther. 2017, 97, 896–903. [Google Scholar] [CrossRef]
- Piva, S.R.; Teixeira, P.E.; Almeida, G.J.; Gil, A.B.; DiGioia III, A.M.; Levison, T.J.; Fitzgerald, G.K. Contribution of hip abductor strength to physical function in patients with total knee arthroplasty. Phys. Ther. 2011, 91, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Berryman Reese, N.; Bandy, W. Joint Range of Motion and Muscle Length Testing; Saunders: Philadelphia, PA, USA, 2002. [Google Scholar]
- Cibere, J.; Bellamy, N.; Thorne, A.; Esdaile, J.M.; McGorm, K.J.; Chalmers, A.; Huang, S.; Peloso, P.; Shojania, K.; Singer, J. Reliability of the knee examination in osteoarthritis: Effect of standardization. Arthritis Rheum. 2004, 50, 458–468. [Google Scholar] [CrossRef]
- Tiedemann, A.; Lord, S.R.; Sherrington, C. The development and validation of a brief performance-based fall risk assessment tool for use in primary care. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Whitney, S.L.; Wrisley, D.M.; Marchetti, G.F.; Gee, M.A.; Redfern, M.S.; Furman, J.M. Clinical measurement of sit-to-stand performance in people with balance disorders: Validity of data for the Five-Times-Sit-to-Stand Test. Phys. Ther. 2005, 85, 1034–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Choi, S.; Trang, A.; McCartney, C.J. Reporting functional outcome after knee arthroplasty and regional anesthesia: A methodological primer. Reg. Anesth. Pain Med. 2013, 38, 340–349. [Google Scholar] [CrossRef]
- Jakobsen, T.L.; Kehlet, H.; Husted, H.; Petersen, J.; Bandholm, T. Early progressive strength training to enhance recovery after fast-track total knee arthroplasty: A randomized controlled trial. Arthritis Care Res. 2014, 66, 1856–1866. [Google Scholar] [CrossRef]
- Kennedy, D.M.; Stratford, P.W.; Riddle, D.L.; Hanna, S.E.; Gollish, J.D. Assessing recovery and establishing prognosis following total knee arthroplasty. Phys. Ther. 2008, 88, 22–32. [Google Scholar] [CrossRef]
- Naylor, J.M.; Crosbie, J.; Ko, V. Is there a role for rehabilitation streaming following total knee arthroplasty? Preliminary insights from a randomized controlled trial. J. Rehabil. Med. 2015, 47, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Su, E.; Perna, M.; Boettner, F.; Mayman, D.; Gerlinger, T.; Barsoum, W.; Randolph, J.; Lee, G. A prospective, multi-center, randomised trial to evaluate the efficacy of a cryopneumatic device on total knee arthroplasty recovery. J. Bone Jt. Surg. 2012, 94-A, 153–156. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Larkin, P.A.; Cook, A.C.; Gear, J.; Singer, J. Decrease in timed balance test scores with aging. Phys. Ther. 1984, 64, 1067–1070. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Stucki, G.; Sangha, O.; Stucki, S.; Michel, B.A.; Tyndall, A.; Dick, W.; Theiler, R. Comparison of the WOMAC (Western Ontario and McMaster Universities) osteoarthritis index and a self-report format of the self-administered Lequesne–Algofunctional index in patients with knee and hip osteoarthritis. Osteoarthr. Cartil. 1998, 6, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, M.-H.; Lin, Y.-S.; Yang, R.-C.; Lee, C.-L. A comparison of various therapeutic exercises on the functional status of patients with knee osteoarthritis. Semin. Arthritis Rheum. 2003, 32, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Petterson, S.C.; Mizner, R.L.; Stevens, J.E.; Raisis, L.; Bodenstab, A.; Newcomb, W.; Snyder-Mackler, L. Improved function from progressive strengthening interventions after total knee arthroplasty: A randomized clinical trial with an imbedded prospective cohort. Arthritis Care Res. 2009, 61, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Stevens-Lapsley, J.E.; Balter, J.E.; Wolfe, P.; Eckhoff, D.G.; Schwartz, R.S.; Schenkman, M.; Kohrt, W.M. Relationship between intensity of quadriceps muscle neuromuscular electrical stimulation and strength recovery after total knee arthroplasty. Phys. Ther. 2012, 92, 1187–1196. [Google Scholar] [CrossRef]
- Thomas, A.C.; Stevens-Lapsley, J.E. Importance of attenuating quadriceps activation deficits after total knee arthroplasty. Exerc. Sport Sci. Rev. 2012, 40, 95. [Google Scholar] [CrossRef] [Green Version]
- Schache, M.B.; McClelland, J.A.; Webster, K.E. Lower limb strength following total knee arthroplasty: A systematic review. Knee 2014, 21, 12–20. [Google Scholar] [CrossRef]
- McClelland, J.A.; Webster, K.E.; Feller, J.A. Gait analysis of patients following total knee replacement: A systematic review. Knee 2007, 14, 253–263. [Google Scholar] [CrossRef]
- Mizner, R.L.; Petterson, S.C.; Snyder-Mackler, L. Quadriceps strength and the time course of functional recovery after total knee arthroplasty. J. Orthop. Sports Phys. Ther. 2005, 35, 424–436. [Google Scholar] [CrossRef] [Green Version]
- Rossi, M.D.; Hasson, S.; Kohia, M.; Pineda, E.; Bryan, W. Mobility and perceived function after total knee arthroplasty. J. Arthroplast. 2006, 21, 6–12. [Google Scholar] [CrossRef]
- Wang, J.; Xie, Y.; Wang, L.; Lei, L.; Liao, P.; Wang, S.; Gao, Y.; Chen, Y.; Xu, F.; Zhang, C. Hip abductor strength–based exercise therapy in treating women with moderate-to-severe knee osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2020, 34, 160–169. [Google Scholar] [CrossRef]
- Gottschall, J.S.; Okita, N.; Sheehan, R.C. Muscle activity patterns of the tensor fascia latae and adductor longus for ramp and stair walking. J. Electromyogr. Kinesiol. 2012, 22, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.T.; Zarro, V.; Bosacco, S.; Israelite, C. Quantitative gait analysis after unilateral or bilateral total knee replacement. J. Bone Jt. Surg. Am. Vol. 1987, 69, 1340–1345. [Google Scholar]
- Chao, E.; Laughman, R.; Stauffer, R. Biomechanical gait evaluation of pre and postoperative total knee replacement patients. Arch. Orthop. Trauma. Surg. 1980, 97, 309–317. [Google Scholar] [CrossRef]
- Lee, T.H.; Tsuchida, T.; Kitahara, H.; Moriya, H. Gait analysis before and after unilateral total knee arthroplasty. Study using a linear regression model of normal controls—Women without arthropathy. J. Orthop. Sci. 1999, 4, 13–21. [Google Scholar] [CrossRef]
- Mattsson, E.; Olsson, E.; Broström, L.-Å. Assessment of walking before and after unicompartmental knee arthroplasty. A comparison of different methods. Scand. J. Rehabil. Med. 1990, 22, 45. [Google Scholar] [PubMed]


{kind=link}
| Exercise | Dosage |
|---|---|
| Warm up (AROM) | 10 min |
| Supine extension bridge with thera-band | 3 sets of 20 at a RPE 5~7 |
| Sideway walking with thera-band | 3 sets of 20 steps at a RPE 5~7 |
| Standing hip adduction with thera-band | 3 sets of 20 at a RPE 5~7 |
| Clamshell (Hip external rotation) with thera-band | 3 sets of 20 at a RPE 5~7 |
| Exercise | Dosage |
|---|---|
| Warm up (AROM) | 10 min |
| Seated knee extension with thera-band | 4 sets of 20 at a RPE 5~7 |
| Supine straight leg raise with thera-band | 4 sets of 20 at a RPE 5~7 |
| Quarter wall squat with thera-band | 4 sets of 20 at a RPE 5~7 |
| Characteristic | All Patients | Hip Group | Quadriceps Group | Control Group | p Value |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||
| Sex (Men/Women) | 8(16.4%)/47(83.6%) | 3(15.8%)/16(84.2%) | 3(15%)/17(85%) | 3(18.8%)/13(81.3%) | 0.952 (chi-Square test) |
| Age (years) | 72.80 ± 5.47 | 72.84 ± 7.03 | 72.50 ± 4.73 | 73.13 | 0.945 |
| Height (cm) | 154.76 ± 5.64 | 155.07 ± 5.86 | 154.28 ± 5.25 | 155.00 ± 6.17 | 0.894 |
| Weight (kg/m2) | 60.65 ± 5.00 | 60.58 ± 5.02 | 61.05 ± 5.50 | 60.25 ± 4.61 | 0.893 |
| BMI (kg/m2) | 37.47 ± 2.76 | 37.19 ± 2.59 | 37.60 ± 3.03 | 37.62 ± 2.75 | 0.868 |
| Outcome Measure | Hip Group | Quadriceps Group | Control | F | p | Post Hoc |
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||||
| Flexion ROM | ||||||
| Baseline | 114.42 ± 10.52 | 115.15 ± 9.33 | 117 ± 5.79 | 0.378 | 0.687 | |
| 4 week f/w | 118.32 ± 9.39 | 120.4 ± 7.25 | 118.44 ± 5.66 | 5.8 | 0.005 * | B > C |
| 8 week f/w | 119.53 ± 9.19 | 121.45 ± 6.73 | 118.56 ± 5.64 | 9.274 | 0.001 * | A, B > C |
| 12 week f/w | 119.84 ± 8.82 | 122.7 ± 6.4 | 118.88 ± 5.62 | 11.006 | 0.001 * | A, B > C |
| Time × Group | 3.382 | 0.004 * | ||||
| Extension ROM | ||||||
| Baseline | 10.37 ± 5.6 | 8.1 ± 3.58 | 9.13 ± 3.09 | 1.371 | 0.263 | |
| 4 week f/w | 8.58 ± 4.76 | 6.8 ± 2.72 | 8.19 ± 2.56 | 1.509 | 0.231 | |
| 8 week f/w | 7.79 ± 4.41 | 6.2 ± 2.3 | 8 ± 2.65 | 4.776 | 0.013 * | A, B > C |
| 12 week f/w | 7.84 ± 4.11 | 6.1 ± 2.33 | 7.63 ± 2.6 | 2.604 | 0.084 | |
| Time × Group | 2.291 | 0.041 * | ||||
| WOMAC-P | ||||||
| Baseline | 12.32 ± 2.42 | 12.75 ± 2.78 | 12.19 ± 2.56 | 0.239 | 0.788 | |
| 4 week f/w | 8.21 ± 4.14 | 10.1 ± 2.97 | 11.25 ± 1.91 | 6.547 | 0.003 * | A > C |
| 8 week f/w | 8.37 ± 2.56 | 9.6 ± 2.41 | 11 ± 2.12 | 11.474 | 0.001 * | A, B > C |
| 12 week f/w | 8.05 ± 3.2 | 9.8 ± 2.39 | 10.69 ± 2.15 | 7.677 | 0.001 * | A > C |
| Time × Group | 3.493 | 0.004 * | ||||
| WOMAC-F | ||||||
| Baseline | 41.89 ± 5.36 | 45.1 ± 7.13 | 45.31 ± 4.78 | 1.931 | 0.155 | |
| 4 week f/w | 33.74 ± 8.93 | 38.2 ± 6.38 | 43.56 ± 3.75 | 8.464 | 0.001 * | A, B > C |
| 8 week f/w | 33.32 ± 8.49 | 37.35 ± 5.94 | 41.5 ± 4.32 | 5.767 | 0.006 * | A > C |
| 12 week f/w | 32.05 ± 8.76 | 36.75 ± 5.32 | 40.31 ± 4.84 | 5.499 | 0.007 * | A > C |
| Time × Group | 1.456 | 0.201 |
| Outcome Measure | Hip | Quadriceps | Control | F | p | Post Hoc |
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||||
| AST | ||||||
| Baseline | 15.72 ± 3.98 | 16.13 ± 4.99 | 14.24 ± 3.18 | 0.977 | 0.383 | |
| 4 week f/w | 12.17 ± 2.66 | 14.26 ± 3.54 | 13.76 ± 2.85 | 7.684 | 0.001 * | A > B, C |
| 8 week f/w | 11.68 ± 3.3 | 14.31 ± 3.53 | 13.67 ± 2.51 | 10.470 | 0.001 * | A > B, C |
| 12 week f/w | 11.17 ± 2.69 | 14.46 ± 3.8 | 13.23 ± 2.6 | 13.336 | 0.001 * | A > B, C |
| Time × Group | 3.999 | 0.001 * | ||||
| FTSST | ||||||
| Baseline | 15.25 ± 3.16 | 16.25 ± 3.64 | 14.49 ± 2.8 | 1.326 | 0.274 | |
| 4 week f/w | 13.25 ± 2.6 | 13.12 ± 2.76 | 13.92 ± 2.29 | 13.595 | 0.001 * | A, B > C |
| 8 week f/w | 12.58 ± 2.58 | 12.77 ± 1.99 | 13.79 ± 2.01 | 11.074 | 0.001 * | A, B > C |
| 12 week f/w | 12.69 ± 2.7 | 13.26 ± 2.32 | 13.29 ± 1.97 | 4.09 | 0.022 * | A, B > C |
| Time × Group | 4.699 | 0.001 * | ||||
| TUG | ||||||
| Baseline | 14.19 ± 2.37 | 15.44 ± 3.13 | 15.38 ± 3.1 | 1.122 | 0.333 | |
| 4 week f/w | 11.09 ± 2.29 | 12.7 ± 2.79 | 14.76 ± 2.27 | 16.737 | 0.001 * | A, B > C |
| 8 week f/w | 10.68 ± 2.36 | 12.46 ± 2.74 | 14.52 ± 2.41 | 16.769 | 0.001 * | A, B > C |
| 12 week f/w | 10.34 ± 2.3 | 12.31 ± 2.63 | 14.47 ± 2.27 | 24.661 | 0.001 * | A, B > C |
| Time × Group | 4.394 | 0.001 * | ||||
| 6MWT | ||||||
| Baseline | 285.54 ± 98.57 | 244.54 ± 93.71 | 240.31 ± 51.72 | 1.568 | 0.218 | |
| 4 week f/w | 341.81 ± 109.11 | 295.55 ± 86.63 * | 245.43 ± 50.22 | 9.994 | 0.001 * | A, B > C |
| 8 week f/w | 351.91 ± 100.6 | 289.1 ± 89.3 * | 247.62 ± 52.86 | 6.74 | 0.002 * | A, B > C |
| 12 week f/w | 346.67 ± 101.95 | 284.6 ± 87.04 * | 252.93 ± 51.9 * | 5.67 | 0.006 * | A > C |
| Time × Group | 4.209 | 0.001 * | ||||
| SLS | ||||||
| Baseline | 5.68 ± 2.51 | 7.37 ± 1.95 | 6.48 ± 2.93 | 2.312 | 0.109 | |
| 4 week f/w | 8.56 ± 3.16 | 8.08 ± 1.89 | 6.56 ± 2.94 | 14.374 | 0.001 * | A > B, C |
| 8 week f/w | 9.83 ± 3.57 | 8.15 ± 1.94 | 6.32 ± 2.94 | 11.817 | 0.001 * | A > B, C |
| 12 week f/w | 9.7 ± 3.82 | 7.85 ± 2.18 | 6.95 ± 2.93 | 7.837 | 0.001 * | A > B, C |
| Time × Group | 8.381 | 0.001 * |
| Outcome Measure | Hip | Quadriceps | Control | F | p | Post Hoc |
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||||
| Stride (cm) | ||||||
| Baseline | 87.94 ± 10.20 | 87.58 ± 13.45 | 85.37 ± 8.48 | 0.268 | 0.766 | |
| 4 week f/w | 94.85 ± 13.00 | 90.65 ± 10.37 | 85.82 ± 8.82 | 24.768 | 0.024 * | A > C |
| 8 week f/w | 97.59 ± 13.14 | 90.85 ± 10.29 | 86.15 ± 8.52 | 5.902 | 0.005 * | A > C |
| 12 week f/w | 97.24 ± 10.46 | 90.70 ± 10.24 | 87.16 ± 8.94 | 7.304 | 0.002 * | A > B,C |
| Time × Group | 1.730 | 0.122 | ||||
| Single-stance(%) | ||||||
| Baseline | 31.71 ± 3.03 | 31.98 ± 2.30 | 31.64 ± 2.40 | 0.086 | 0.918 | |
| 4 week f/w | 34.37 ± 3.21 | 32.67 ± 2.45 | 31.81 ± 2.48 | 10.225 | 0.001 * | A > B,C |
| 8 week f/w | 35.31 ± 3.78 | 32.44 ± 2.42 | 31.81 ± 2.58 | 12.574 | 0.001 * | A > B,C |
| 12 week f/w | 34.99 ± 3.36 | 32.60 ± 2.39 | 32.23 ± 2.31 | 12.155 | 0.001 * | A > B,C |
| Time × Group | 3.933 | 0.001 * | ||||
| Double-stance(%) | ||||||
| Baseline | 33.37 ± 2.41 | 32.74 ± 4.28 | 33.69 ± 3.68 | 0.343 | 0.711 | |
| 4 week f/w | 29.62 ± 3.61 | 31.76 ± 3.75 | 33.69 ± 3.38 | 12.702 | 0.001 * | A > B,C |
| 8 week f/w | 28.75 ± 4.32 | 31.88 ± 3.67 | 33.51 ± 3.22 | 11.999 | 0.001 * | A > B,C |
| 12 week f/w | 28.90 ± 3.53 | 31.98 ± 3.83 | 33.24 ± 3.14 | 14.983 | 0.001 * | A > B,C |
| Time × Group | 4.462 | 0.001 * | ||||
| Speed (m/s) | ||||||
| Baseline | 0.82 ± 0.12 | 0.82 ± 0.11 | 0.80 ± 0.10 | 0.257 | 0.774 | |
| 4 week f/w | 0.93 ± 0.11 | 0.93 ± 0.11 | 0.81 ± 0.09 | 10.619 | 0.001 * | A,B > C |
| 8 week f/w | 0.97 ± 0.11 | 0.96 ± 0.11 | 0.81 ± 0.09 | 18.006 | 0.001 * | A,B > C |
| 12 week f/w | 0.96 ± 0.11 | 0.98 ± 0.12 | 0.82 ± 0.09 | 14.179 | 0.001 * | A,B > C |
| Time × Group | 4.270 | 0.001 * | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Do, K.; Yim, J. Effects of Muscle Strengthening around the Hip on Pain, Physical Function, and Gait in Elderly Patients with Total Knee Arthroplasty: A Randomized Controlled Trial. Healthcare 2020, 8, 489. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040489
Do K, Yim J. Effects of Muscle Strengthening around the Hip on Pain, Physical Function, and Gait in Elderly Patients with Total Knee Arthroplasty: A Randomized Controlled Trial. Healthcare. 2020; 8(4):489. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040489
Chicago/Turabian StyleDo, KwangSun, and JongEun Yim. 2020. "Effects of Muscle Strengthening around the Hip on Pain, Physical Function, and Gait in Elderly Patients with Total Knee Arthroplasty: A Randomized Controlled Trial" Healthcare 8, no. 4: 489. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040489