
Novel Adiposity and Biochemical–Anthropometric Indices to Identify Cardiometabolic Risk and Metabolic Syndrome in Mexican Adults


Abstract
:1. Introduction
2. Materials and Methods
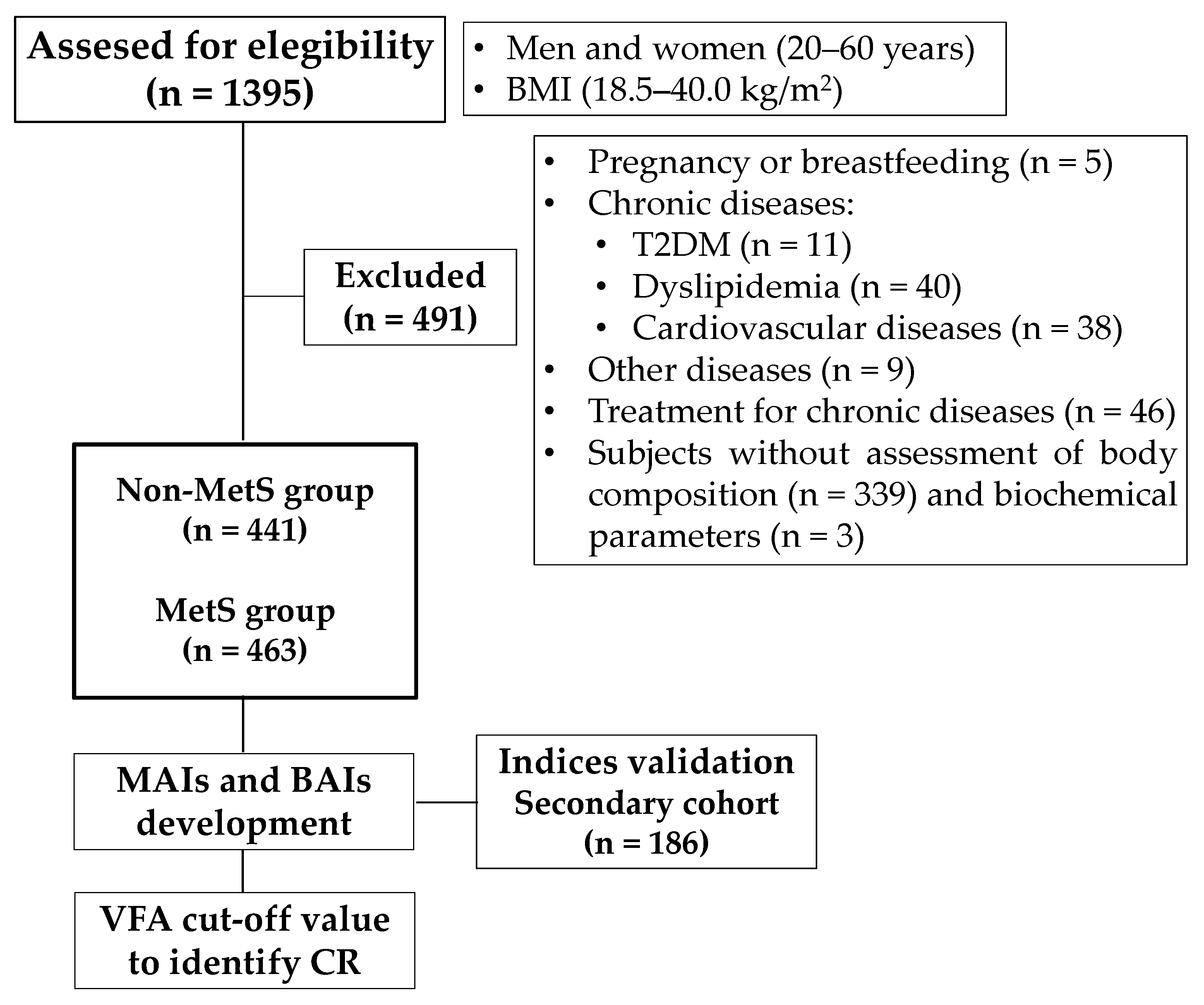
2.1. Subjects
2.2. Data Collection
2.2.1. Clinical Evaluation
2.2.2. Anthropometric and Body Composition Assessment
2.2.3. Biochemical Assays
2.2.4. Anthropometric, Adiposity, and Insulin Resistance Indexes
2.2.5. Metabolic Syndrome Diagnosis
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
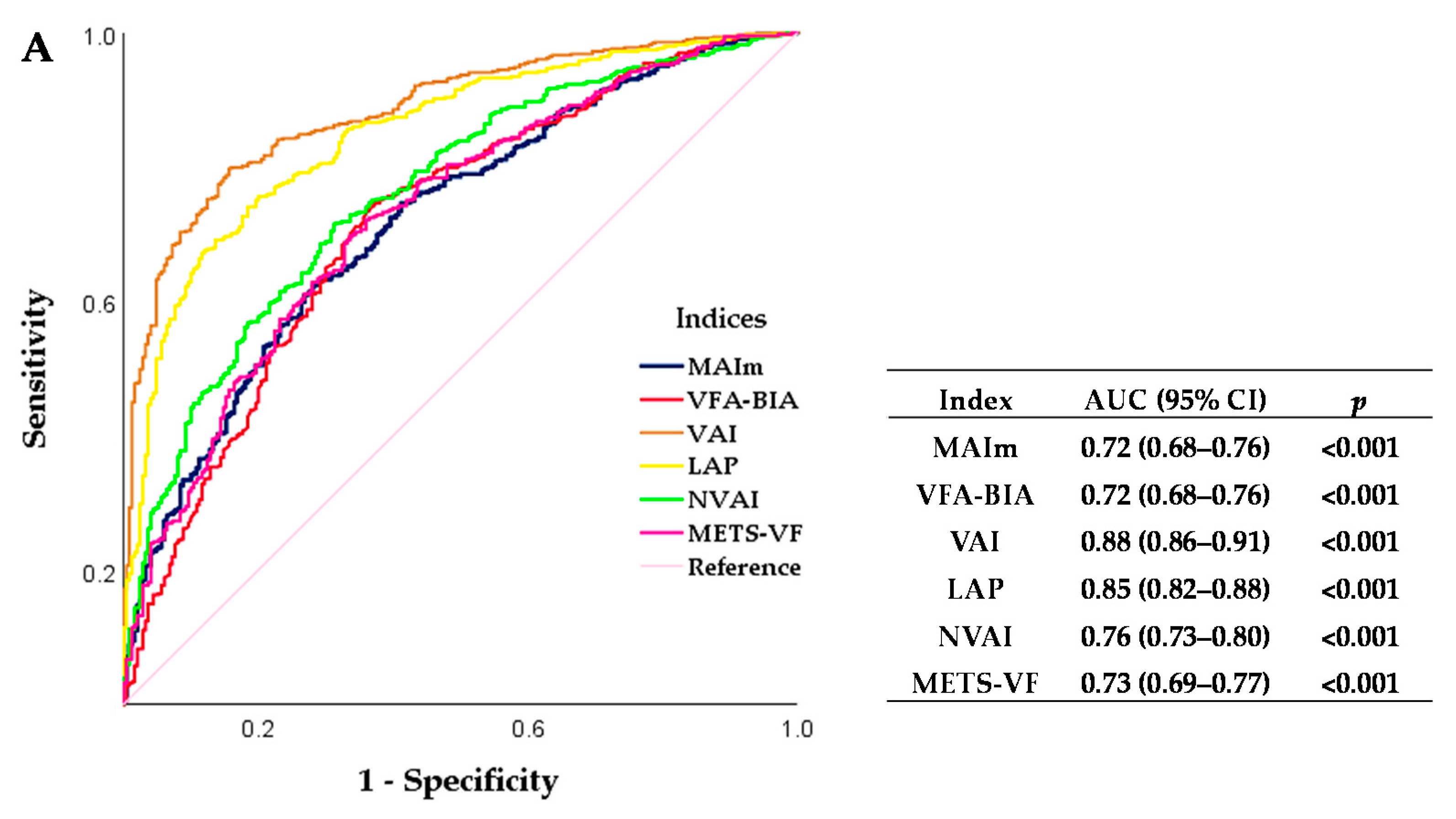
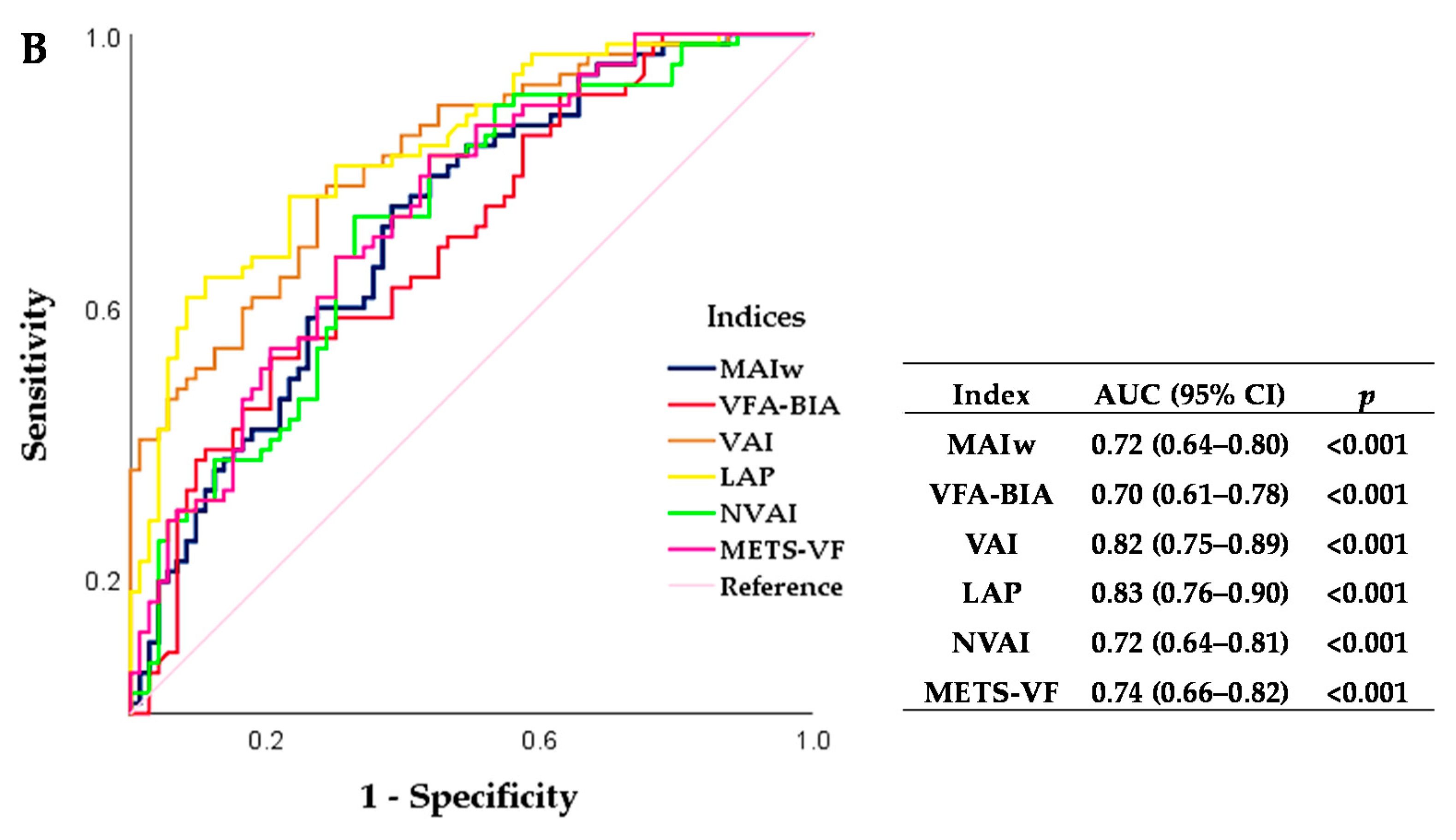
3.2. Mexican Adiposity Indices to Identify Cardiometabolic Risk Associated with Visceral Adipose Tissue Accumulation in Mexican Adults
3.3. The Cut-Off Values for the Visceral Fat Area as Assessed by Bioelectrical Impedance Analysis to Identify Cardiometabolic Risk in Mexican Adults
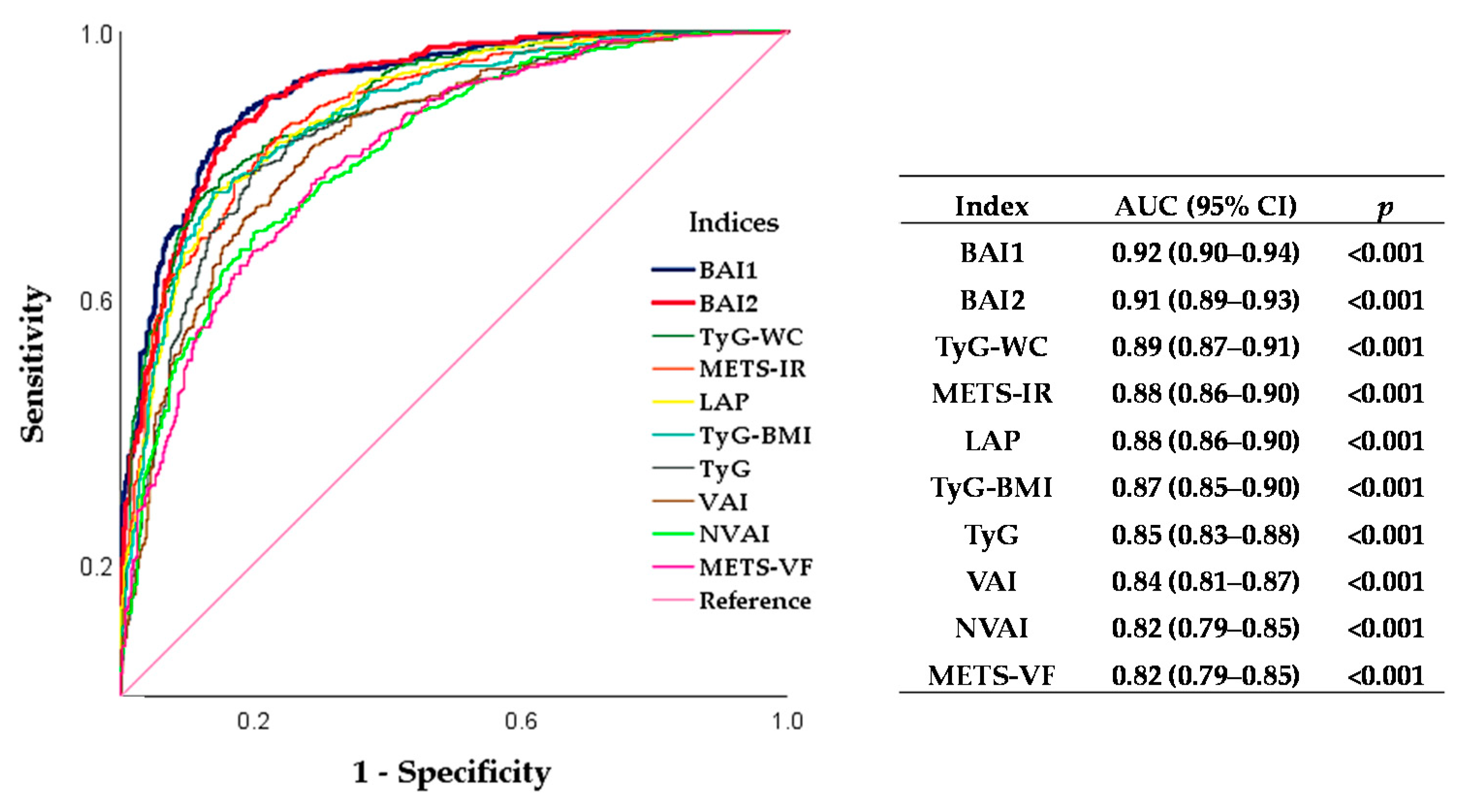
3.4. Biochemical–Anthropometric Indices to Identify Metabolic Syndrome in Mexican Adults
4. Discussion
4.1. Sex-Specific Mexican Adiposity Indices and Visceral Fat Area Cut-Off Value Assessed by Bioelectrical Impedance Analysis to Identify Cardiometabolic Risk Associated with Visceral Adipose Tissue Accumulation in Mexican Adults
4.2. Biochemical–Anthropometric Indices to Identify Metabolic Syndrome
4.3. Advantages and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neeland, I.J.; Ross, R.; Despres, J.P.; Matsuzawa, Y.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Lancet Diabetes Endocrinol. 2019, 7, 715–725. [Google Scholar] [CrossRef]
- Elffers, T.W.; de Mutsert, R.; Lamb, H.J.; de Roos, A.; Willems van Dijk, K.; Rosendaal, F.R.; Jukema, J.W.; Trompet, S. Body fat distribution, in particular visceral fat, is associated with cardiometabolic risk factors in obese women. PLoS ONE 2017, 12, e0185403. [Google Scholar] [CrossRef] [Green Version]
- Sato, F.; Maeda, N.; Yamada, T.; Namazui, H.; Fukuda, S.; Natsukawa, T.; Nagao, H.; Murai, J.; Masuda, S.; Tanaka, Y.; et al. Association of Epicardial, Visceral, and Subcutaneous Fat With Cardiometabolic Diseases. Circ. J. 2018, 82, 502–508. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.V.; Murthy, V.L.; Abbasi, S.A.; Blankstein, R.; Kwong, R.Y.; Goldfine, A.B.; Jerosch-Herold, M.; Lima, J.A.; Ding, J.; Allison, M.A. Visceral adiposity and the risk of metabolic syndrome across body mass index: The MESA Study. JACC Cardiovasc. Imaging 2014, 7, 1221–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuster, A.; Patlas, M.; Pinthus, J.H.; Mourtzakis, M. The clinical importance of visceral adiposity: A critical review of methods for visceral adipose tissue analysis. Br. J. Radiol. 2012, 85, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Examination Committee of Criteria for ‘Obesity Disease’ in Japan; Japan Society for the Study of Obesity. New criteria for ‘obesity disease’ in Japan. Circ. J. 2002, 66, 987–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kammar-García, A.; Hernández-Hernández, M.E.; López-Moreno, P.; Ortíz-Bueno, A.M.; Martínez-Montaño, M.L.C. Risk and diagnosis of the metabolic syndrome in apparently healthy young adults by means of the waist-height. Rev. Med. Hosp. Gen. Méx. 2019, 82, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Gonzalez, D.; Miranda-Lora, A.; Klunder-Klunder, M.; Queipo-Garcia, G.; Bustos-Esquivel, M.; Paez-Villa, M.; Villanueva-Ortega, E.; Chavez-Requena, I.; Laresgoiti-Servitje, E.; Garibay-Nieto, N. Diagnostic Performance of Waist Circumference Measurements for Predicting Cardiometabolic Risk in Mexican Children. Endocr. Pract. 2016, 22, 1170–1176. [Google Scholar] [CrossRef]
- Wall-Medrano, A.; Ramos-Jimenez, A.; Hernandez-Torres, R.P.; Villalobos-Molina, R.; Tapia-Pancardo, D.C.; Jimenez-Flores, J.R.; Mendez-Cruz, A.R.; Murguia-Romero, M.; Gallardo-Ortiz, I.A.; Urquidez-Romero, R. Cardiometabolic risk in young adults from northern Mexico: Revisiting body mass index and waist-circumference as predictors. BMC Public Health 2016, 16, 236. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A.; AlkaMeSy Study, G. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920–922. [Google Scholar] [CrossRef] [Green Version]
- Kahn, H.S. The “lipid accumulation product” performs better than the body mass index for recognizing cardiovascular risk: A population-based comparison. BMC Cardiovasc. Disord. 2005, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Bello-Chavolla, O.Y.; Almeda-Valdes, P.; Gomez-Velasco, D.; Viveros-Ruiz, T.; Cruz-Bautista, I.; Romo-Romo, A.; Sanchez-Lazaro, D.; Meza-Oviedo, D.; Vargas-Vazquez, A.; Campos, O.A.; et al. METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes. Eur. J. Endocrinol. 2018, 178, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Er, L.K.; Wu, S.; Chou, H.H.; Hsu, L.A.; Teng, M.S.; Sun, Y.C.; Ko, Y.L. Triglyceride Glucose-Body Mass Index Is a Simple and Clinically Useful Surrogate Marker for Insulin Resistance in Nondiabetic Individuals. PLoS ONE 2016, 11, e0149731. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendia, L.E.; Rodriguez-Moran, M.; Guerrero-Romero, F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab. Syndr. Relat. Disord. 2008, 6, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.K.; Cho, A.R.; Kwon, Y.J.; Lee, H.S.; Lee, J.W. Derivation and validation of a new visceral adiposity index for predicting visceral obesity and cardiometabolic risk in a Korean population. PLoS ONE 2018, 13, e0203787. [Google Scholar] [CrossRef] [PubMed]
- Bello-Chavolla, O.Y.; Antonio-Villa, N.E.; Vargas-Vazquez, A.; Viveros-Ruiz, T.L.; Almeda-Valdes, P.; Gomez-Velasco, D.; Mehta, R.; Elias-Lopez, D.; Cruz-Bautista, I.; Roldan-Valadez, E.; et al. Metabolic Score for Visceral Fat (METS-VF), a novel estimator of intra-abdominal fat content and cardio-metabolic health. Clin. Nutr. 2020, 39, 1613–1621. [Google Scholar] [CrossRef]
- Barquera, S.; Rivera, J.A. Obesity in Mexico: Rapid epidemiological transition and food industry interference in health policies. Lancet Diabetes Endocrinol. 2020, 8, 746–747. [Google Scholar] [CrossRef]
- Campos-Nonato, I.; Aguilar-Salinas, C.A.; Mendoza-Herrera, K.; Pedroza-Tobías, A.; Rojas, R.; Barquera, S. Prevalence and Trends of Metabolic Syndrome in Mexican Adults: Data of the National Health and Nutrition Surveys 2006 and 2016; Research Square: Durham, NC, USA, 2020. [Google Scholar]
- Knopfholz, J.; Disserol, C.C.; Pierin, A.J.; Schirr, F.L.; Streisky, L.; Takito, L.L.; Massucheto Ledesma, P.; Faria-Neto, J.R.; Olandoski, M.; da Cunha, C.L.; et al. Validation of the friedewald formula in patients with metabolic syndrome. Cholesterol 2014, 2014, 261878. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, Y.; Nakagawa, T.; Yamamoto, S.; Takahashi, Y.; Yokoyama, T.; Mizoue, T.; Noda, M. Visceral fat area cutoff for the detection of multiple risk factors of metabolic syndrome in Japanese: The Hitachi Health Study. Obesity 2012, 20, 1744–1749. [Google Scholar] [CrossRef]
- Gutierrez-Solis, A.L.; Datta Banik, S.; Mendez-Gonzalez, R.M. Prevalence of Metabolic Syndrome in Mexico: A Systematic Review and Meta-Analysis. Metab. Syndr. Relat. Disord. 2018, 16, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F.; Clegg, D.J. The sexual dimorphism of obesity. Mol. Cell. Endocrinol. 2015, 402, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.; Kim, Y.J.; Oh, S.W.; Lee, C.M.; Choi, H.C.; Joh, H.K.; Oh, B.; Hwang, S.S.; Kim, S.J.; Kwon, O.D. Cut-Off Values for Visceral Fat Area Identifying Korean Adults at Risk for Metabolic Syndrome. Korean J. Fam. Med. 2018, 39, 239–246. [Google Scholar] [CrossRef]
- Santosa, S.; Jensen, M.D. The Sexual Dimorphism of Lipid Kinetics in Humans. Front. Endocrinol. 2015, 6, 103. [Google Scholar] [CrossRef] [Green Version]
- Anderson, L.A.; McTernan, P.G.; Barnett, A.H.; Kumar, S. The effects of androgens and estrogens on preadipocyte proliferation in human adipose tissue: Influence of gender and site. J. Clin. Endocrinol. Metab. 2001, 86, 5045–5051. [Google Scholar] [CrossRef]
- Lemieux, I.; Pascot, A.; Tchernof, A.; Bergeron, J.; Prud’homme, D.; Bouchard, C.; Despres, J.P. Visceral adipose tissue and low-density lipoprotein particle size in middle-aged versus young men. Metabolism 1999, 48, 1322–1327. [Google Scholar] [CrossRef]
- Ritchie, S.A.; Connell, J.M. The link between abdominal obesity, metabolic syndrome and cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 319–326. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Bray, G.A.; Greenway, F.L.; Johnson, W.D.; Newton, R.L., Jr.; Ravussin, E.; Ryan, D.H.; Bouchard, C. Ethnic-specific BMI and waist circumference thresholds. Obesity 2011, 19, 1272–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pekgor, S.; Duran, C.; Berberoglu, U.; Eryilmaz, M.A. The Role of Visceral Adiposity Index Levels in Predicting the Presence of Metabolic Syndrome and Insulin Resistance in Overweight and Obese Patients. Metab. Syndr. Relat. Disord. 2019, 17, 296–302. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C.; Pitrone, M.; Galluzzo, A. Cut-off points of the visceral adiposity index (VAI) identifying a visceral adipose dysfunction associated with cardiometabolic risk in a Caucasian Sicilian population. Lipids Health Dis. 2011, 10, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bermúdez, V.J.; Salazar, J.; Añez, R.; Rivas-Ríos, J.R.; Chávez-Castillo, M.; Torres, W.; Núñez, V.; Mejías, J.; Wilches-Durán, S.; Cerda, M.; et al. Optimal cutoff for visceral adiposity index in a Venezuelan population: Results from the Maracaibo City Metabolic Syndrome Prevalence Study. Rev. Argent. Endocrinol. Metab. 2017, 54, 176–183. [Google Scholar] [CrossRef]
- Li, R.; Li, Q.; Cui, M.; Yin, Z.; Li, L.; Zhong, T.; Huo, Y.; Xie, P. Clinical surrogate markers for predicting metabolic syndrome in middle-aged and elderly Chinese. J. Diabetes Investig. 2018, 9, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Shin, K.A.; Kim, Y.J. Usefulness Of Surrogate Markers Of Body Fat Distribution For Predicting Metabolic Syndrome In Middle-Aged And Older Korean Populations. Diabetes Metab. Syndr. Obes. 2019, 12, 2251–2259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tellechea, M.L.; Aranguren, F.; Martinez-Larrad, M.T.; Serrano-Rios, M.; Taverna, M.J.; Frechtel, G.D. Ability of lipid accumulation product to identify metabolic syndrome in healthy men from Buenos Aires. Diabetes Care 2009, 32, e85. [Google Scholar] [CrossRef] [Green Version]
- Okosun, I.S.; Okosun, B.; Lyn, R.; Airhihenbuwa, C. Surrogate indexes of insulin resistance and risk of metabolic syndrome in non-Hispanic White, non-Hispanic Black and Mexican American. Diabetes Metab. Syndr. 2020, 14, 3–9. [Google Scholar] [CrossRef]
- Mendoza-González, C. Guías del Instituto Nacional de Cardiología “Ignacio Chávez” para el tratamiento de la hipertensión arterial sistémica. Arch. Cardiol. Mex. 2006, 76, 279–284. [Google Scholar]
- Nagai, M.; Komiya, H.; Mori, Y.; Ohta, T.; Kasahara, Y.; Ikeda, Y. Development of a new method for estimating visceral fat area with multi-frequency bioelectrical impedance. Tohoku J. Exp. Med. 2008, 214, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Gao, B.; Liu, Y.; Ding, C.; Liu, S.; Chen, X.; Bian, X. Comparison of visceral fat area measured by CT and bioelectrical impedance analysis in Chinese patients with gastric cancer: A cross-sectional study. BMJ Open 2020, 10, e036335. [Google Scholar] [CrossRef]
- Lee, D.-H.; Park, K.S.; Ahn, S.; Ku, E.J.; Jung, K.Y.; Kim, Y.J.; Kim, K.M.; Moon, J.H.; Choi, S.H.; Park, K.S.; et al. Comparison of Abdominal Visceral Adipose Tissue Area Measured by Computed Tomography with That Estimated by Bioelectrical Impedance Analysis Method in Korean Subjects. Nutrients 2015, 7, 10513–10524. [Google Scholar] [CrossRef] [Green Version]
- Omura-Ohata, Y.; Son, C.; Makino, H.; Koezuka, R.; Tochiya, M.; Tamanaha, T.; Kishimoto, I.; Hosoda, K. Efficacy of visceral fat estimation by dual bioelectrical impedance analysis in detecting cardiovascular risk factors in patients with type 2 diabetes. Cardiovasc. Diabetol. 2019, 18, 137. [Google Scholar] [CrossRef] [Green Version]
- Qin, Q.; Yang, Y.; Chen, J.; Jiang, Y.; Li, A.; Huang, M.; Dong, Y.; Wang, S.; Ding, S. Bioelectrical impedance analysis versus quantitative computer tomography and anthropometry for the assessment of body composition parameters in China. Sci. Rep. 2021, 11, 11076. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Non-MetS n = 441 | MetS n = 463 | p |
|---|---|---|---|
| Age (years) | 32.0 ± 7.6 | 34.9 ± 8.2 | <0.001 |
| Male (%) | 353 (80.0) | 410 (88.6) | <0.001 |
| BMI (kg/m2) | 25.8 ± 3.4 | 29.9 ± 3.7 | <0.001 |
| WHtR | 0.5 ± 0.1 | 0.6 ± 0.1 | <0.001 |
| WC (cm) | 89.1 ± 8.8 | 100.1 ± 9.0 | <0.001 |
| VFA (cm2) | 89.2 ± 31.4 | 121.8 ± 30.5 | <0.001 |
| Total body fat (kg) | 18.6 ± 7.0 | 26.5 ± 7.6 | <0.001 |
| Body fat percentage (%) | 25.1 ± 7.4 | 30.6 ± 6.5 | <0.001 |
| Free fat mass (kg) | 54.6 ± 8.3 | 59.2 ± 8.4 | <0.001 |
| Skeletal muscle mass (kg) | 30.9 ± 5.1 | 33.6 ± 5.0 | <0.001 |
| Systolic BP (mmHg) | 118.3 ± 11.7 | 128.5 ± 14.0 | <0.001 |
| Diastolic BP (mmHg) | 73.7 ± 8.8 | 81.5 ± 10.2 | <0.001 |
| MBP (mmHg) | 88.6 ± 8.5 | 97.2 ± 10.3 | <0.001 |
| FBG (mg/dL) | 89.9 ± 10.5 | 99.6 ± 12.5 | <0.001 |
| Total cholesterol (mg/dL) | 175.9 ± 33.9 | 191.0 ± 33.3 | <0.001 |
| HDL-c (mg/dL) | 40.3 ± 9.1 | 33.7 ± 6.9 | <0.001 |
| LDL-c (mg/dL) | 110.1 ± 28.5 | 113.9 ± 31.3 | 0.058 |
| VLDL-c (mg/dL) | 25.5 ± 13.1 | 43.7 ± 18.9 | <0.001 |
| TG (mg/dL) | 127.3 ± 65.2 | 218.6 ± 94.5 | <0.001 |
| VAI | 1.8 (1.3) | 3.7 (2.5) | <0.001 |
| LAP | 37.2 ± 23.2 | 87.9 ± 43.2 | <0.001 |
| NVAI | 0.7 (0.5) | 1.0 (0.1) | <0.001 |
| METS-VF | 6.4 ± 0.6 | 7.0 ± 0.4 | <0.001 |
| TyG | 8.5 ± 0.5 | 9.2 ± 0.5 | <0.001 |
| TyG–BMI | 220.7 ± 32.7 | 274.5 ± 35.1 | <0.001 |
| TyG–WC | 760.1 ± 97.6 | 921.2 ± 94.6 | <0.001 |
| METS-IR | 40.4 ± 6.5 | 51.5 ± 7.3 | <0.001 |
| MetS components, N (%) | |||
| Elevated WC | 128 (29.0) | 378 (81.6) | <0.001 |
| Elevated BP | 73 (16.6) | 284 (61.3) | <0.001 |
| Reduced HDL-c level | 237 (53.7) | 418 (90.3) | <0.001 |
| Elevated FBG level | 54 (12.2) | 256 (55.3) | <0.001 |
| Elevated TG level | 103 (23.4) | 359 (77.5) | <0.001 |
| Variable | Non-Standardized Coefficient B | Standardized Coefficient β | Significance | t | R2 | F | p |
|---|---|---|---|---|---|---|---|
| MAIm | 0.83 | 1877.23 | <0.001 | ||||
| Body weight * WC (kg * cm) | 0.02 | 0.95 | <0.001 | 61.02 | |||
| Height (cm) | −2.10 | −0.36 | <0.001 | −23.10 | |||
| MAIw | 0.86 | 409.46 | <0.001 | ||||
| Body weight * WC (kg * cm) | 0.02 | 0.92 | <0.001 | 28.32 | |||
| Height (cm) | −1.60 | −0.21 | <0.001 | −6.52 |
| Cut-Off | Sensitivity (%) | Specificity (%) | AUC | 95% CI | p | |
|---|---|---|---|---|---|---|
| 0.71 | (0.67–0.74) | <0.001 | ||||
| VFA (cm2) | 95.1 | 73.7 | 59.2 | |||
| 100.3 | 66.8 | 64.4 | ||||
| 105.1 | 58.7 | 69.0 |
| Variable | Standardized Coefficient β | Wald Statistic | p | OR | 95% CI | p |
|---|---|---|---|---|---|---|
| BAI1 | <0.001 | |||||
| TyG | 3.18 | 157.01 | <0.001 | 23.99 | (14.59–39.43) | |
| BMI (kg/m2) | 0.29 | 83.47 | <0.001 | 1.34 | (1.25–1.42) | |
| MBP (mmHg) | 0.08 | 46.57 | <0.001 | 1.08 | (1.06–1.10) | |
| BAI2 | <0.001 | |||||
| TyG | 3.20 | 162.20 | <0.001 | 24.46 | (14.96–40.01) | |
| VFA (cm2) | 0.03 | 79.21 | <0.001 | 1.03 | (1.02–1.04) | |
| MBP (mmHg) | 0.08 | 51.12 | <0.001 | 1.08 | (1.06–1.11) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Carrillo, P.L.; Aguirre-Tostado, P.I.; Macías-Cervantes, M.H.; Alegría-Torres, J.A.; Luevano-Contreras, C. Novel Adiposity and Biochemical–Anthropometric Indices to Identify Cardiometabolic Risk and Metabolic Syndrome in Mexican Adults. Healthcare 2021, 9, 1561. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9111561
Rodríguez-Carrillo PL, Aguirre-Tostado PI, Macías-Cervantes MH, Alegría-Torres JA, Luevano-Contreras C. Novel Adiposity and Biochemical–Anthropometric Indices to Identify Cardiometabolic Risk and Metabolic Syndrome in Mexican Adults. Healthcare. 2021; 9(11):1561. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9111561
Chicago/Turabian StyleRodríguez-Carrillo, Patricia Lizett, Priscila Irene Aguirre-Tostado, Maciste H. Macías-Cervantes, Jorge Alejandro Alegría-Torres, and Claudia Luevano-Contreras. 2021. "Novel Adiposity and Biochemical–Anthropometric Indices to Identify Cardiometabolic Risk and Metabolic Syndrome in Mexican Adults" Healthcare 9, no. 11: 1561. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9111561