
A Prospective Study of Long-Term Regenerative Endodontics Outcomes of Necrotic Immature Permanent Teeth: An 8-Year Follow-Up

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Procedures
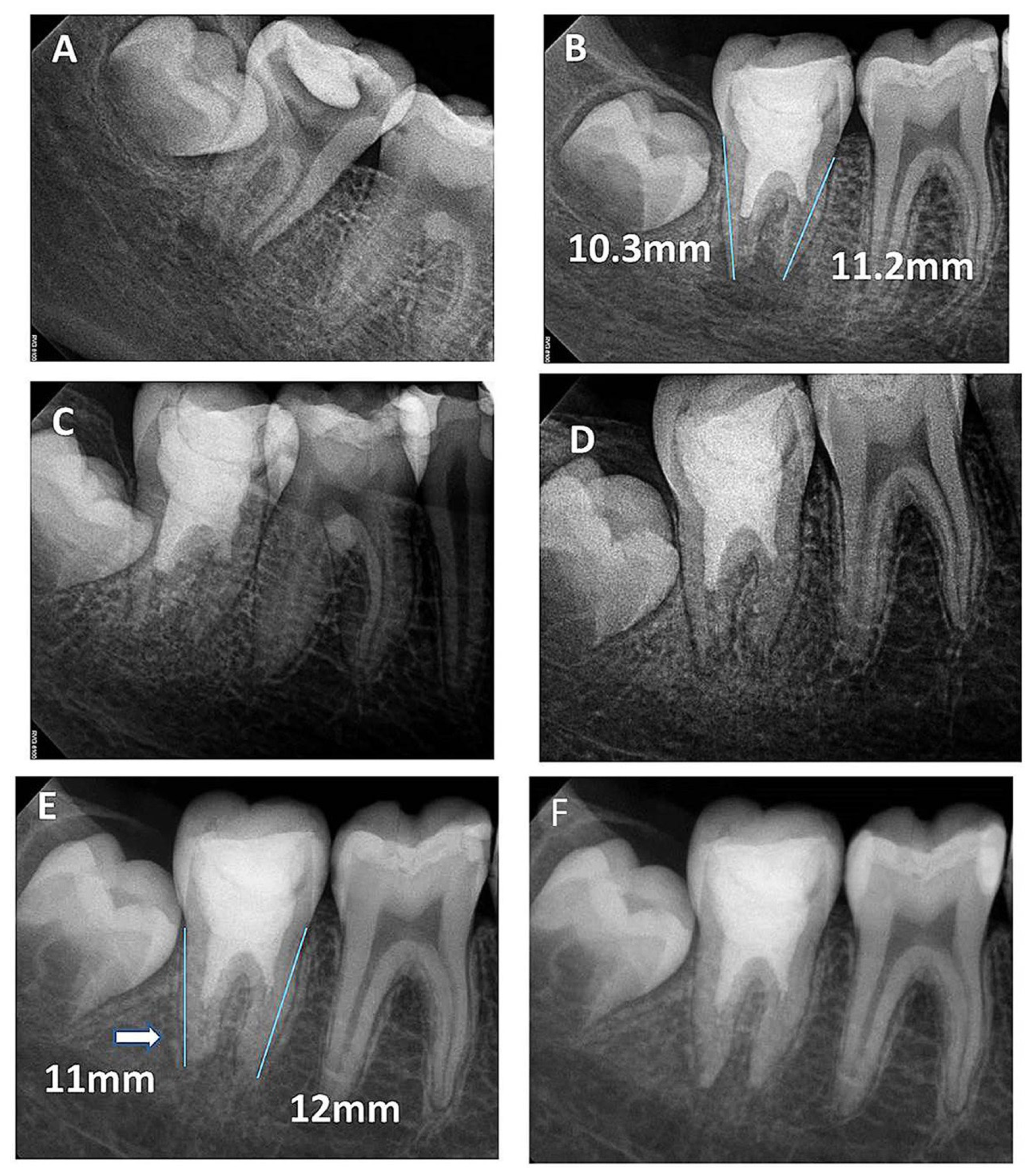
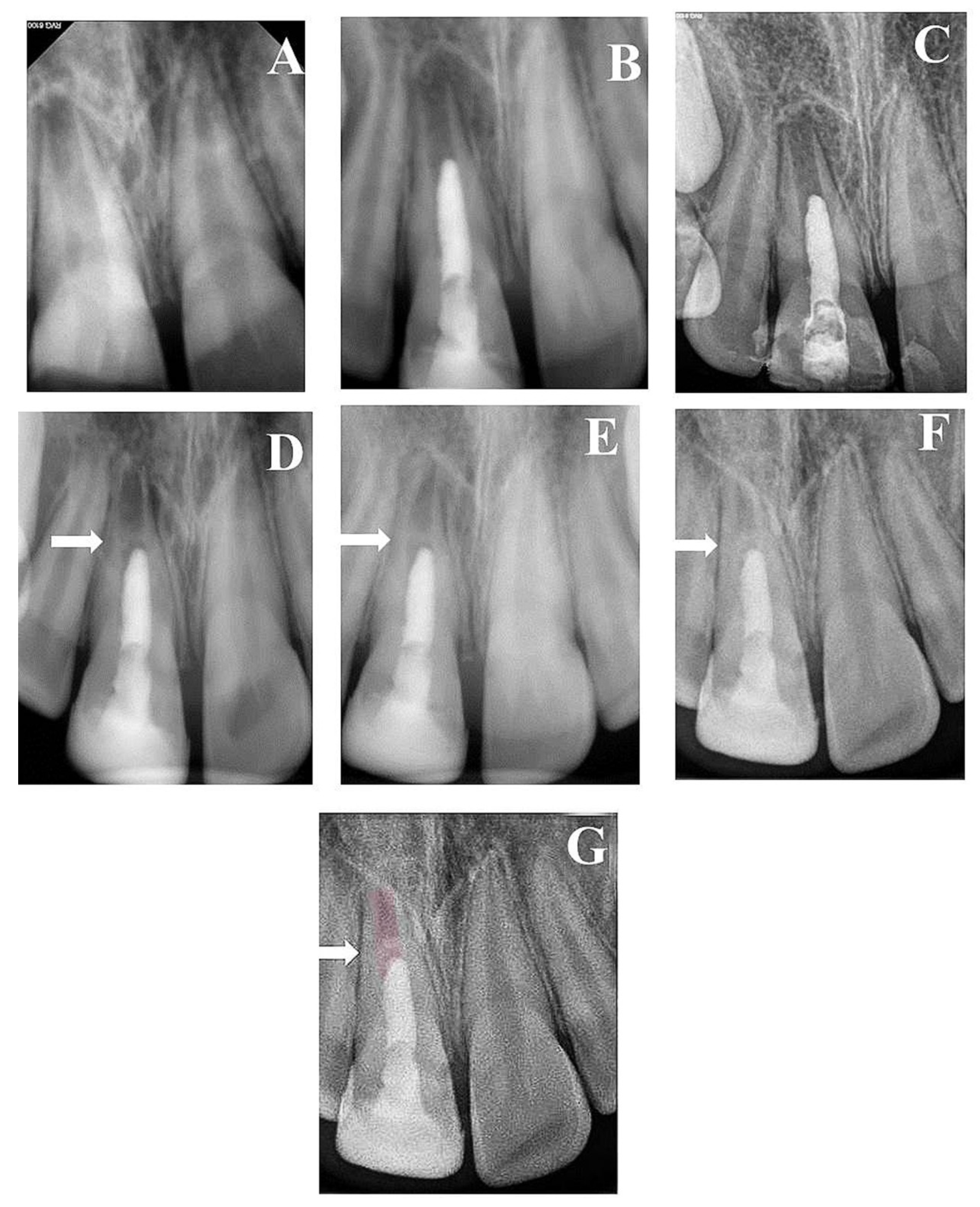
2.2. Quantitative Assessment
2.3. Qualitative Assessment
2.4. Statistical Analysis
3. Results
3.1. Quantitative Assessment
3.2. Qualitative Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cehreli, Z.C.; Isbitiren, B.; Sara, S.; Erbas, G. Regenerative Endodontic Treatment (Revascularization) of Immature Necrotic Molars Medicated with Calcium Hydroxide: A Case Series. J. Endod. 2011, 37, 1327–1330. [Google Scholar] [CrossRef]
- Rafter, M. Apexification: A review. Dent. Traumatol. 2005, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, V.; Baccetti, T.; Pace, R.; Pagavino, G. The use of MTA in teeth with necrotic pulps and open apices. Dent. Traumatol. 2002, 18, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Jyothi, M. Management of immature teeth—A paradigm shift from apexification to apexogenesis. Ann. Essences Dent. 2001, 2, 34–38. [Google Scholar]
- Torabinejad, M.; Abu-Tahun, I. Management of teeth with necrotic pulps and open apices. Endod. Top. 2010, 23, 105–130. [Google Scholar] [CrossRef]
- Jeeruphan, T.; Jantarat, J.; Yanpiset, K.; Suwannapan, L.; Khewsawai, P.; Hargreaves, K.M. Mahidol study 1: Comparison of radiographic and survival outcomes of immature teeth treated with either regenerative endodontic or apexification methods: A retrospective study. J. Endod. 2012, 38, 1330–1336. [Google Scholar] [CrossRef]
- Trope, M. Treatment of immature teeth with non-vital pulps and apical periodontitis. Endod. Top. 2006, 14, 51–59. [Google Scholar] [CrossRef]
- Wigler, R.; Kaufman, A.Y.; Lin, S.; Steinbock, N.; Hazan-Molina, H.; Torneck, C.D. Revascularization: A Treatment for Permanent Teeth with Necrotic Pulp and Incomplete Root Development. J. Endod. 2013, 39, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Östby, B.N. The Role of the Blood Clot in Endodontic Therapy an Experimental Histologic Study. Acta Odontol. Scand. 1961, 19, 323–353. [Google Scholar] [CrossRef]
- Huang, G.T.-J.; Sonoyama, W.; Liu, Y.; Liu, H.; Wang, S.; Shi, S. The Hidden Treasure in Apical Papilla: The Potential Role in Pulp/Dentin Regeneration and BioRoot Engineering. J. Endod. 2008, 34, 645–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estefan, B.S.; El Batouty, K.M.; Nagy, M.M.; Diogenes, A. Influence of Age and Apical Diameter on the Success of Endodontic Regeneration Procedures. J. Endod. 2016, 42, 1620–1625. [Google Scholar] [CrossRef]
- Chen, X.; Bao, Z.-F.; Liu, Y.; Liu, M.; Jin, X.-Q.; Xu, X.-B. Regenerative Endodontic Treatment of an Immature Permanent Tooth at an Early Stage of Root Development: A Case Report. J. Endod. 2013, 39, 719–722. [Google Scholar] [CrossRef] [PubMed]
- Ding, R.Y.; Cheung, G.S.-P.; Chen, J.; Yin, X.; Wang, Q.Q.; Zhang, C. Pulp Revascularization of Immature Teeth With Apical Periodontitis: A Clinical Study. J. Endod. 2009, 35, 745–749. [Google Scholar] [CrossRef]
- Nagy, M.M.; Tawfik, H.E.; Hashem, A.A.R.; Abu-Seida, A.M. Regenerative potential of immature permanent teeth with necrotic pulps after different regenerative protocols. J. Endod. 2014, 40, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Kontakiotis, E.G.; Filippatos, C.G.; Agrafioti, A. Levels of Evidence for the Outcome of Regenerative Endodontic Therapy. J. Endod. 2014, 40, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; Nosrat, A.; Verma, P.; Udochukwu, O. Regenerative Endodontic Treatment or Mineral Trioxide Aggregate Apical Plug in Teeth with Necrotic Pulps and Open Apices: A Systematic Review and Meta-analysis. J. Endod. 2017, 43, 1806–1820. [Google Scholar] [CrossRef] [PubMed]
- López, F.U.; Kopper, P.M.P.; Cucco, C.; Bona, A.D.; de Figueiredo, J.A.P.; Vier-Pelisser, F.V. Accuracy of cone-beam computed tomography and periapical radiography in apical periodontitis diagnosis. J. Endod. 2014, 40, 2057–2060. [Google Scholar] [CrossRef] [PubMed]
- Cvek, M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study. Dent. Traumatol. 1992, 8, 45–55. [Google Scholar] [CrossRef]
- Banchs, F.; Trope, M. Revascularization of Immature Permanent Teeth with Apical Periodontitis: New Treatment Protocol? J. Endod. 2004, 30, 196–200. [Google Scholar] [CrossRef]
- Khoshkhounejad, M.; Shokouhinejad, N.; Pirmoazen, S. Regenerative endodontic treatment: Report of two cases with different clinical management and outcomes. J. Dent. 2015, 12, 460. [Google Scholar]
- Bose, R.; Nummikoski, P.; Hargreaves, K. A Retrospective Evaluation of Radiographic Outcomes in Immature Teeth with Necrotic Root Canal Systems Treated with Regenerative Endodontic Procedures. J. Endod. 2009, 35, 1343–1349. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, M.S.M.; Barletta, F.B.; Fontanella, V.R.C.; Vanni, J.R. Canal transportation after root canal instrumentation: A comparative study with computed tomography. J. Endod. 2007, 33, 962–965. [Google Scholar] [CrossRef]
- Zeid, S.T.H.A.; Shafie, L.A. The influence of asymmetric cross section of rotary instrument on root canal geometry using cone-beam computed tomography. Egypt. Dent. J. 2014, 60, 1053–1060. [Google Scholar]
- Mente, J.; Hage, N.; Pfefferle, T.; Koch, M.J.; Dreyhaupt, J.; Staehle, H.J.; Friedman, S. Mineral Trioxide Aggregate Apical Plugs in Teeth with Open Apical Foramina: A Retrospective Analysis of Treatment Outcome. J. Endod. 2009, 35, 1354–1358. [Google Scholar] [CrossRef]
- Albuquerque, M.T.P.; Nagata, J.Y.; Soares, A.D.J.; Zaia, A.A. Pulp revascularization: An alternative treatment to the apexification of immature teeth. RGO—Rev. Gaúcha Odontol. 2014, 62, 401–410. [Google Scholar] [CrossRef] [Green Version]
- Shah, N.; Logani, A.; Bhaskar, U.; Aggarwal, V. Efficacy of Revascularization to Induce Apexification/Apexogensis in Infected, Nonvital, Immature Teeth: A Pilot Clinical Study. J. Endod. 2008, 34, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Windley, W., III; Teixeira, F.; Levin, L.; Sigurdsson, A.; Trope, M. Disinfection of immature teeth with a triple antibiotic paste. J. Endod. 2005, 31, 439–443. [Google Scholar] [CrossRef] [Green Version]
- Hoshino, E.; Kurihara-Ando, N.; Sato, I.; Uematsu, H.; Sato, M.; Kota, K.; Iwaku, M. In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline. Int. Endod. J. 1996, 29, 125–130. [Google Scholar] [CrossRef]
- Akgun, O.M.; Altun, C.; Guven, G. Use of triple antibiotic paste as a disinfectant for a traumatized immature tooth with a periapical lesion: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, e62–e65. [Google Scholar] [CrossRef] [PubMed]
- Ruparel, N.B.; Teixeira, F.B.; Ferraz, C.; Diogenes, A. Direct Effect of Intracanal Medicaments on Survival of Stem Cells of the Apical Papilla. J. Endod. 2012, 38, 1372–1375. [Google Scholar] [CrossRef]
- Sabrah, A.H.A.; Yassen, G.H.; Liu, W.-C.; Goebel, W.S.; Gregory, R.L.; Platt, J.A. The effect of diluted triple and double antibiotic pastes on dental pulp stem cells and established Enterococcus faecalis biofilm. Clin. Oral Investig. 2015, 19, 2059–2066. [Google Scholar] [CrossRef] [Green Version]
- Segura-Egea, J.J.; Gould, K.; Şen, B.H.; Jonasson, P.; Cotti, E.; Mazzoni, A.; Sunay, H.; Tjäderhane, L.; Dummer, P. European Society of Endodontology position statement: The use of antibiotics in endodontics. Int. Endod. J. 2018, 51, 20–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadi, Z.; Abbott, P.V. On the local applications of antibiotics and antibiotic-based agents in endodontics and dental traumatology. Int. Endod. J. 2009, 42, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Jung, I.-Y.; Lee, S.-J.; Hargreaves, K.M. Biologically based treatment of immature permanent teeth with pulpal necrosis: A case series. J. Endod. 2008, 34, 876–887. [Google Scholar] [CrossRef]
- Chen, M.Y.-H.; Chen, K.-L.; Chen, C.-A.; Tayebaty, F.; Rosenberg, P.A.; Lin, L.M. Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures. Int. Endod. J. 2012, 45, 294–305. [Google Scholar] [CrossRef] [PubMed]
- American Association of Endodontists: Clinical Considerations for a Regenerative Procedure. 2016. Available online: https://wwwaaeorg/uploadedfiles/publications_and_research/research/currentregenerativeendodonticconsiderationspdf (accessed on 30 May 2021).
- Law, A.S. Considerations for regeneration procedures. Pediatr. Dent. 2013, 35, 141–152. [Google Scholar] [CrossRef]
- Shivashankar, V.Y.; Johns, D.A.; Maroli, R.K.; Sekar, M.; Chandrasekaran, R.; Karthikeyan, S.; Renganathan, S.K. Comparison of the effect of PRP, PRF and induced bleeding in the revascularization of teeth with necrotic pulp and open apex: A triple blind randomized clinical trial. J. Clin. Diagn. Res. 2017, 11, ZC34. [Google Scholar] [PubMed]
- Alagl, A.; Bedi, S.; Hassan, K.; AlHumaid, J. Use of platelet-rich plasma for regeneration in non-vital immature permanent teeth: Clinical and cone-beam computed tomography evaluatio. J. Int. Med. Res. 2017, 45, 583–593. [Google Scholar] [CrossRef]
- Staffoli, S.; Plotino, G.; Torrijos, B.G.N.; Grande, N.M.; Bossù, M.; Gambarini, G.; Polimeni, A. Regenerative Endodontic Procedures Using Contemporary Endodontic Materials. Materials 2019, 12, 908. [Google Scholar] [CrossRef] [Green Version]
- Meschi, N.; EzEldeen, M.; Garcia, A.E.T.; Jacobs, R.; Lambrechts, P. A Retrospective Case Series in Regenerative Endodontics: Trend Analysis Based on Clinical Evaluation and 2- and 3-dimensional Radiology. J. Endod. 2018, 44, 1517–1525. [Google Scholar] [CrossRef]
- Huang, G.T.J. A paradigm shift in endodontic management of immature teeth: Conservation of stem cells for regeneration. J. Dent. 2008, 36, 379–386. [Google Scholar] [CrossRef]
- Orstavik, D.; Qvist, V.; Stoltze, K. A multivariate analysis of the outcome of endodontic treatment. Eur. J. Oral Sci. 2004, 112, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.; Andreasen, F.M.; Bergenholtz, G.; Andreasen, J.O.; Norén, J.G. Incidence of pulp necrosis subsequent to pulp canal obliteration from trauma of permanent incisors. J. Endod. 1996, 22, 557–560. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Gender | Age in Years | Tooth | Etiology | Preoperative Root Length in mm | Preoperative Dentin Thickness in mm | Preoperative Apical Canal Width in mm | Length of the Follow Up | Resolution of Periapical Lesion in Month | Sensitivity Test at the 3rd Year Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 9 | 11 | Trauma | 11.088 | 0.405 | 0.63 | 2 years | No lesion | NA |
| 2 | Male | 9 | 21 | Trauma | 10.48 | 0.477 | 1.021 | 3 years | 6 | No respond |
| 3 | Male | 9 | 11 | Trauma | 12.562 | 0.584 | 1.53 | 3 years | 6 | Respond |
| 4 | Male | 9 | 21 | Trauma | 12.36 | 0.44 | 1.1 | 3 years | 6 | Respond |
| 5 | Male | 10 | 11 | Trauma | 14.014 | 0.81 | 0.92 | 3 years | 6 | No respond |
| 6 | Male | 11 | 21 | Trauma | 14.38 | 0.78 | 0.9 | 2 years | 6 | NA |
| 7 | Female | 8 | 21 | Trauma | 10.01 | 0.36 | 1.02 | 3 years | 6 | No respond |
| 8 | Female | 8 | 47 | Caries | 10.51 | 0.41 | 1.28 | 2 years | 9 | NA |
| 9 | Male | 11 | 21 | Trauma | 10.34 | 0.79 | 2.32 | 8 years | 6 | Respond |
| 10 | Male | 11 | 11 | Trauma | 10.02 | 0.51 | 1.85 | 8 years | 6 | Respond |
| 11 | Male | 11 | 11 | Trauma | 10.375 | 0.56 | 1.68 | 8 years | 6 | No Respond |
| 12 | Male | 11 | 11 | Trauma | 10.05 | 0.56 | 1.13 | 8 years | 9 | Respond |
| 13 | Male | 11 | 11 | Trauma | 9.356 | 0.39 | 1.14 | 8 years | 6 | No respond |
| 14 | Male | 13 | 31 | Trauma | 9.40 | 0.31 | 1.233 | 8 years | 6 | No respond |
| 15 | Male | 11 | 21 | Trauma | 9.338 | 0.38 | 1.15 | 8 years | 9 | Respond |
| 16 | Male | 9 | 35 | Caries | 9.40 | 0.31 | 1.16 | 8 years | 6 | Respond |
| 17 | Male | 11 | 21 | Trauma | 9.401 | 0.36 | 1.23 | 12 months | 6 | NA |
| 18 | Male | 10 | 21 | Trauma | 9.8 | 0.514 | 1.279 | 12 months | No lesion | NA |
| 19 | Male | 10 | 11 | Trauma | 10.2 | 0.534 | 1.321 | 12 months | No lesion | NA |
| 20 | Female | 8 | 37 | Caries | 10.477 | 0.78 | 1.214 | 12 months | No lesion | NA |
| 21 | Male | 10 | 21 | Trauma | 9.56 | 0.419 | 0.923 | 12 months | No lesion | NA |
| 22 | Male | 9 | 21 | Trauma | 10.023 | 0.465 | 1.13 | 12 months | 6 | NA |
| 23 | Male | 8 | 16 | Caries | 9.401 | 0.402 | 1.24 | 12 months | 6 | NA |
| Follow-Up Time | Median at Each Follow-Up Time (mm) | ||
|---|---|---|---|
| Root Length | Apical Canal Width | Dentin Wall Thickness | |
| Preoperative | 10.36 | 1.14 | 0.48 |
| 6th Month | 10.47 | 1.15 | 0.72 |
| 12th Month | 10.64 | 1.28 | 0.74 |
| 2nd Year | 10.79 | 1.29 | 0.76 |
| 3rd Year | 10.92 | 0.65 | 0.86 |
| 8th Year | 11.4 | 0.24 | 0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu Zeid, S.T.; Alamoudi, R.A.; Alothmani, O.S.; Mokeem Saleh, A.A.; Siddiqui, A.Y. A Prospective Study of Long-Term Regenerative Endodontics Outcomes of Necrotic Immature Permanent Teeth: An 8-Year Follow-Up. Healthcare 2021, 9, 1670. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121670
Abu Zeid ST, Alamoudi RA, Alothmani OS, Mokeem Saleh AA, Siddiqui AY. A Prospective Study of Long-Term Regenerative Endodontics Outcomes of Necrotic Immature Permanent Teeth: An 8-Year Follow-Up. Healthcare. 2021; 9(12):1670. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121670
Chicago/Turabian StyleAbu Zeid, Sawsan T., Ruaa A. Alamoudi, Osama S. Alothmani, Abeer A. Mokeem Saleh, and Amna Y. Siddiqui. 2021. "A Prospective Study of Long-Term Regenerative Endodontics Outcomes of Necrotic Immature Permanent Teeth: An 8-Year Follow-Up" Healthcare 9, no. 12: 1670. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121670