
Impact of Nutrition Care Process Documentation in Obese Children and Adolescents with Metabolic Syndrome and/or Non-Alcoholic Fatty Liver Disease



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Participants
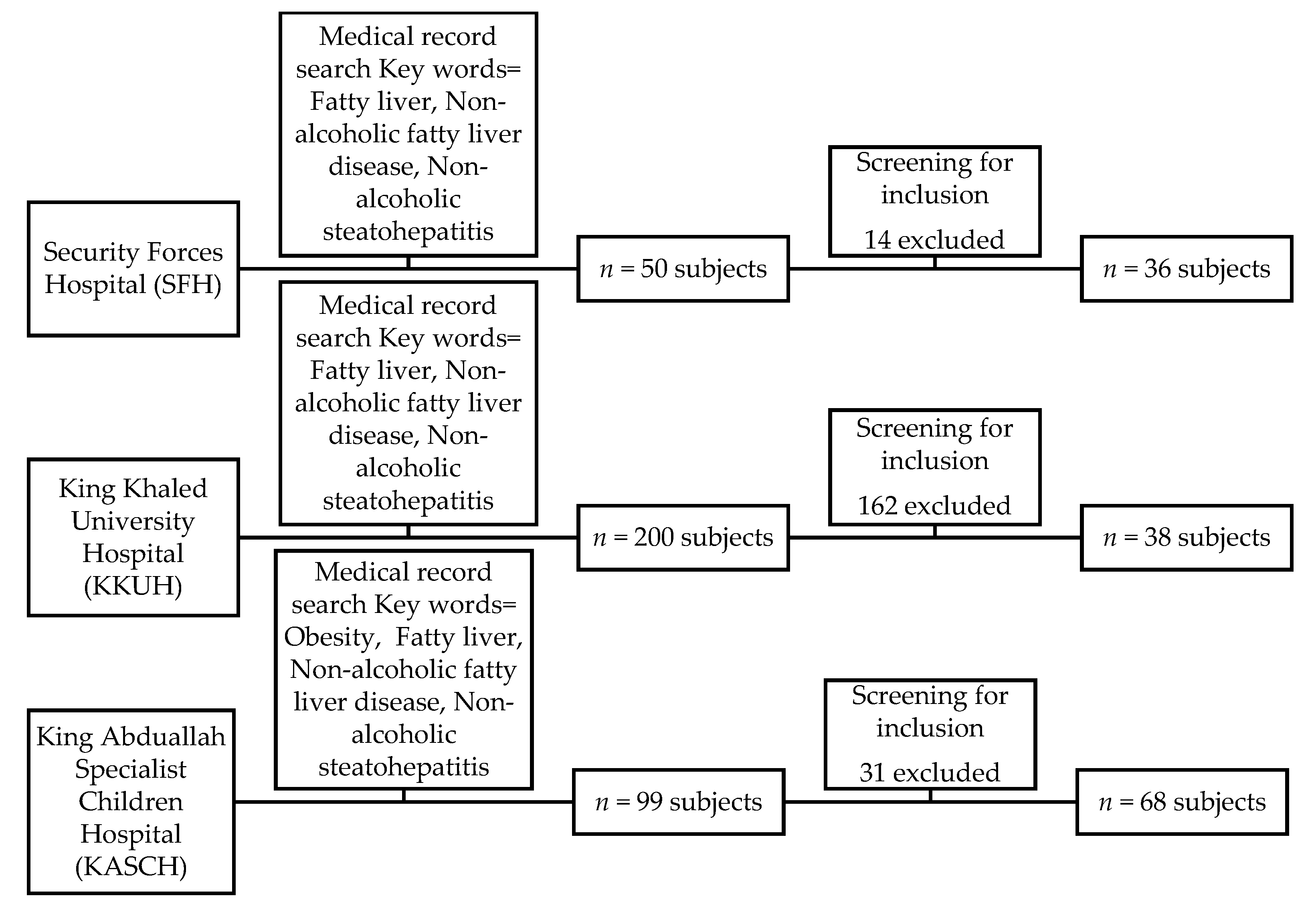
2.3. Hospital Medical Record Search
2.4. Sample Size and Sampling Technique
2.5. Study Parameters
2.5.1. Socio-Economic Data and Medical History
2.5.2. Obesity Parameters
2.5.3. Metabolic Syndrome Parameters
2.5.4. NAFLD Parameters
2.5.5. Assessing the Quality of Dietitians’ Documentation
2.5.6. Achievement Parameters of Nutritional Goals
2.6. Statistical Analysis
3. Results
3.1. Study Subjects’ Demographic Data and Baseline Characteristics
3.2. Audit of the NCP Documentation
3.3. Correlation between Dietitian Documentation Audit Scores and Achievement of the Nutritional Goals
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Edwards, M.; Moczygemba, J. Reducing Medical Errors Through Better Documentation. Health Care Manag. 2004, 23, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, K.C.; Sensmeier, J. Technological Approach to Enhancing Patient Safety. 2002. Available online: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.475.4937&rep=rep1&type=pdf2002 (accessed on 11 March 2020).
- Nancarrow, S.A.; Booth, A.; Ariss, S.; Smith, T.; Enderby, P.; Roots, A. Ten principles of good interdisciplinary teamwork. Hum. Resour. Health 2013, 11, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biesemeier, C.; Chima, C.S. Computerized patient record: Are we prepared for our future practice? J. Am. Diet. Assoc. 1997, 97, 1099–1104. [Google Scholar] [CrossRef]
- Lacey, K.; Pritchett, E. Nutrition care process and model: ADA adopts road map to quality care and outcomes management. J. Acad. Nutr. Diet. 2003, 103, 1061–1072. [Google Scholar] [CrossRef]
- Andersen, D.; Baird, S.; Bates, T.; Chapel, D.L.; Cline, A.D.; Ganesh, S.N.; Garner, M.; Grant, B.L.; Hamilton, K.K.; Jablonski, K.; et al. Academy of Nutrition and Dietetics: Revised 2017 Standards of Practice in Nutrition Care and Standards of Professional Performance for Registered Dietitian Nutritionists. J. Acad. Nutr. Diet. 2018, 118, 132–140.e15. [Google Scholar] [CrossRef] [Green Version]
- Lövestam, E.; Orrevall, Y.; Koochek, A.; Karlström, B.; Andersson, A. Evaluation of Nutrition Care Process documentation in electronic patient records: Need of improvement. Nutr. Diet. 2014, 72, 74–80. [Google Scholar] [CrossRef]
- Kaur, J. A Comprehensive Review on Metabolic Syndrome. Cardiol. Res. Pr. 2014, 2014, 1–21. [Google Scholar] [CrossRef]
- Lee, A.M.; Gurka, M.J.; DeBoer, M.D. Trends in Metabolic Syndrome Severity and Lifestyle Factors Among Adolescents. Pediatrics 2016, 137, e20153177. [Google Scholar] [CrossRef] [Green Version]
- Cook, S.; Weitzman, M.; Auinger, P.; Nguyen, M.; Dietz, W.H. Prevalence of a metabolic syndrome phenotype in adolescents: Findings from the third National Health and Nutrition Examination Survey, 1988–1994. Arch. Pediatr. Adolesc. Med. 2003, 157, 821–827. [Google Scholar] [CrossRef] [Green Version]
- Kapil, U.; Kaur, S. Prevalence of Pediatrics Metabolic Syndrome (PMS) Amongst Children in the Age Group of 6–18 Years Belonging to High Income Group Residing in National Capital Territory (NCT) of Delhi. Indian J. Pediatr. 2010, 77, 1041. [Google Scholar] [CrossRef] [Green Version]
- Alberti KG, M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; National Heart, Lung, And Blood Institute; American Heart Association; World Heart Federation; International. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Marchesini, G.; Bugianesi, E.; Forlani, G.; Cerrelli, F.; Lenzi, M.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; Melchionda, N.; et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003, 37, 917–923. [Google Scholar] [CrossRef]
- Vos, M.B.; Abrams, S.H.; Barlow, S.E.; Caprio, S.; Daniels, S.R.; Kohli, R.; Xanthakos, S.A. NASPGHAN clinical practice guideline for the diagnosis and treatment of nonalcoholic fatty liver disease in children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). J. Pediatr. Gastroenterol. Nutr. 2017, 64, 319. [Google Scholar] [PubMed] [Green Version]
- Hoelscher, D.M.; Kirk, S.; Ritchie, L.; Cunningham-Sabo, L.; Academy Positions Committee. Position of the Academy of Nutrition and Dietetics: Interventions for the Prevention and Treatment of Pediatric Overweight and Obesity. J. Acad. Nutr. Diet. 2013, 113, 1375–1394. [Google Scholar] [CrossRef] [PubMed]
- Steinberger, J. Progress and challenges in metabolic syndrome in children and adolescents: A scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular Nursing; and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2009, 119, 628–647. [Google Scholar]
- Chalasani, N.; Younossi, Z.M.; LaVine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.R.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatol. 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Lenth, R.V. Java Applets for Power And Sample Size. 2006. Available online: http://www.stat.uiowa.edu/~rlenth/Power (accessed on 1 February 2020).
- Boyraz, M.; Hatipoğlu, N.; Sari, E.; Akcay, A.; Taskin, N.; Korkut, U.; Akcay, T. Non-alcoholic fatty liver disease in obese children and the relationship between metabolic syndrome criteria. Obes. Res. Clin. Pr. 2014, 8, e356–e363. [Google Scholar] [CrossRef]
- Falkner, B.; Daniels, S.R. Summary of the fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Hypertension 2004, 44, 387–388. [Google Scholar] [CrossRef] [Green Version]
- Hickman, T.B.; Briefel, R.R.; Carroll, M.D.; Rifkind, B.M.; Cleeman, J.I.; Maurer, K.R.; Johnson, C.L. Distributions and trends of serum lipid levels among United States children and adolescents ages 4-19 years: Data from the Third National Health and Nutrition Examination Survey. Prev Med. 1998, 27, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Joseph, A.; Saverymuttu, S. Ultrasound in the assessment of diffuse parenchymal liver disease. Clin. Radiol. 1991, 44, 219–221. [Google Scholar] [CrossRef]
- Patton, H.M.; Yates, K.; Unalp-Arida, A.; Behling, C.A.; Huang, T.T.-K.; Rosenthal, P.; Sanyal, A.J.; Schwimmer, J.B.; LaVine, J.E. Association Between Metabolic Syndrome and Liver Histology Among Children With Nonalcoholic Fatty Liver Disease. Am. J. Gastroenterol. 2010, 105, 2093–2102. [Google Scholar] [CrossRef] [Green Version]
- Lövestam, E.; Orrevall, Y.; Koochek, A.; Karlström, B.; Andersson, A. Evaluation of a Nutrition Care Process-based audit instrument, the Diet-NCP-Audit, for documentation of dietetic care in medical records. Scand. J. Caring Sci. 2013, 28, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Howse, E.; Bailey, J. Resistance to documentation—A nursing research issue. Int. J. Nurs. Stud. 1992, 29, 371–380. [Google Scholar] [CrossRef]
- Alkhaldy, A.A.; Allahyani, M.N.; Alghamdi, N.A.; Jeddawi, A.K.; Malibary, R.M.; Al-Othman, A.M. Status of nutrition care process implementation in hospitals in Jeddah, Saudi Arabia. Clin. Nutr. ESPEN 2020, 36, 53–59. [Google Scholar] [CrossRef]
- Memmer, D. Implementation and Practical Application of the Nutrition Care Process in the Dialysis Unit. J. Ren. Nutr. 2013, 23, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Murphy, W.J.; Yadrick, M.M.; Steiber, A.L.; Mohan, V.; Papoutsakis, C. Academy of Nutrition and Dietetics Health Informatics Infrastructure (ANDHII): A pilot study on the documentation of the Nutrition Care Process and the usability of ANDHII by registered dietitian nutritionists. J. Acad. Nutr. Diet. 2018, 118, 1966–1974. [Google Scholar] [CrossRef] [PubMed]
- Becker, P.; Lusk, B.; Walker, F.; Gallagher, J.W. The Design and Implementation of an Electronic Medical Record Template Using Standardized Language and the Nutrition Care Process. J. Am. Diet. Assoc. 2009, 109, A9. [Google Scholar] [CrossRef]
- Urquhart, C.; Currell, R.; Grant, M.J.; Hardiker, N.R. Nursing record systems: Effects on nursing practice and healthcare outcomes. Cochrane Database Syst. Rev. 2009, CD002099. [Google Scholar] [CrossRef] [PubMed]
- Weddle, D.O.; Tu, N.S.; Guzik, C.J.; Ramakrishnan, V. Positive Association between Dietetics Recommendations and Achievement of Enteral Nutrition Outcomes of Care. J. Am. Diet. Assoc. 1995, 95, 753–758. [Google Scholar] [CrossRef]
- Bruun, L.I.; Bosaeus, I.; Bergstad, L.; Nygaard, K. Prevalence of malnutrition in surgical patients: Evaluation of nutritional support and documentation. Clin. Nutr. 1999, 18, 141–147. [Google Scholar] [CrossRef]
- Wakeham, M.; Christensen, M.; Manzi, J.; Kuhn, E.M.; Scanlon, M.; Goday, P.S.; Mikhailov, T.A. Registered dietitians making a difference: Early medical record documentation of estimated energy requirement in critically ill children is associated with higher daily energy intake and with use of the enteral route. J. Acad. Nutr. Diet. 2013, 113, 1311–1316. [Google Scholar] [CrossRef] [PubMed]
- Funk, K.L.; Ayton, C.M. Improving Malnutrition Documentation Enhances Reimbursement. J. Am. Diet. Assoc. 1995, 95, 468–475. [Google Scholar] [CrossRef]


{kind=link}
| Are the Following Statements Consistent with the Medical Record Reviewed? Answer in Accordance with the Scoring Scale, and with Support of the Associated Manual. Scoring Items 1–12: Yes = 2 p, Partly = 1 p, No = 0 p; Scoring items 13–14: Yes = 1 p, Partly = 0.5 p, No = 0 p | ||||
|---|---|---|---|---|
| Item No. | Question | Score | ||
| 1. | One or more nutrition problems have been identified and prioritized | 0 | 1 | 2 |
| 2. | Possible etiology related to one or more nutrition problems is documented | 0 | 1 | 2 |
| 3. | The documentation refers to signs and/or symptoms related to one or more nutrition problems | 0 | 1 | 2 |
| 4. | The documentation includes relationship between problem, etiology and signs/symptoms | 0 | 1 | 2 |
| 5. | The documentation includes a nutrition prescription | 0 | 1 | 2 |
| 6. | The documentation includes taken or planned interventions, alternatively a comment explaining why interventions were not taken | 0 | 1 | 2 |
| 7. | The documentation includes evidence for the choice of taken or planned interventions, alternatively the decision of not taking any interventions | 0 | 1 | 2 |
| 8. | The documentation includes one or more goals for the intervention | 0 | 1 | 2 |
| 9. | The documentation includes information of whether a follow-up appointment is planned, alternatively whether the patient is discharged | 0 | 1 | 2 |
| 10. | The documentation includes a plan for how to perform the monitoring and evaluation, alternatively an explanation of why no monitoring and evaluation was planned | 0 | 1 | 2 |
| 11. | The structure of the note follows the assessment-diagnosis-intervention-monitoring/evaluation format | 0 | 1 | 2 |
| 12. | The language in the record is clear and may not lead to misunderstandings | 0 | 1 | 2 |
| 13. | All included information is relevant for understanding the patient’s nutritional status, problem, and situation | 0 | 0.5 | 1 |
| 14. | All relevant information included in the assessment part gets the response in the intervention part | 0 | 1.5 | 1 |
| Total score (max 26) | Final Score: ……………. | |||
| Disease Group | NAFLD Diagnosis Method | Stage of NAFLD | ||||
|---|---|---|---|---|---|---|
| Ultrasound N (%) | Liver Biopsy N (%) | CT N (%) | Mild N (%) | Moderate N (%) | Advance N (%) | |
| Group II Obese with non-alcoholic fatty liver disease | 71 (95.9%) | 3 (4.1%) | 0 (0.0%) | 69 (94.5%) | 1 (1.4%) | 3 (4.1%) |
| Group IV Obese with metabolic syndrome and non-alcoholic fatty liver disease | 20 (95.2%) | 0 (0.0%) | 1 (4.8%) | 21 (100%) | 0 (0.0%) | 0 (0.0%) |
| Disease Parameters | Group I | Group II | Group III | Group IV | p-Value |
|---|---|---|---|---|---|
| (n = 37) | (n = 74) | (n = 10) | (n = 21) | ||
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| Body mass index (kg/m2) | 30.47 ± 6.49 | 34.46 ± 8.03 | 31.55 ± 4.61 | 34.83 ± 6.68 | 0.039 ** |
| Systolic blood pressure (mmHg) | 118.27 ± 8.44 | 121.58 ± 14.99 | 116.10 ± 13.28 | 129.71 ± 16.43 | 0.012 ** |
| Diastolic blood pressure (mmHg) | 66.49 ± 8.97 | 69.57 ± 9.8 | 67.40 ± 9.29 | 72.05 ± 8.80 | 0.152 |
| Triglycerides (mmol/L) | 0.98 ± 0.44 | 1.33 ± 0.85 | 1.08 ± 0.36 | 1.56 ± 0.69 | 0.50 |
| Total cholesterol (mmol/L) | 4.34 ± 0.68 | 4.19 ± 0.86 | 4.32 ± 1.08 | 4.70 ± 0.97 | 0.173 |
| High-density lipoprotein (mmol/L) | 1.13 ± 0.22 | 1.31 ± 0.88 | 1.00 ± 0.23 | 1.10 ± 0.40 | 0.360 |
| Low-density lipoprotein (mmol/L) | 2.81 ± 0.64 | 2.54 ± 0.71 | 3.11 ± 1.12 | 2.91 ± 0.82 | 0.68 |
| Insulin (mIU/L) | 18.71 ± 15.91 | 25.71 ± 13.37 | N/A * | 33.11 ± 18.32 | 0.308 |
| Fasting blood glucose (mmol/L) | 4.90 ± 0.43 | 5.69 ± 3.47 | 5.18 ± 0.58 | 9.26 ± 6.51 | 0.006 ** |
| Alanine aminotransferase (U/L) | 24.97 ± 14.39 | 46.84 ± 59.15 | 30.50 ± 17.59 | 52.74 ± 32.75 | 0.110 |
| Aspartate aminotransferase (U/L) | 24.93 ± 7.86 | 36.46 ± 38.52 | 30.83 ± 11.58 | 32.46 ± 16.18 | 0.373 |
| Alkaline phosphatase (U/L) | 250.34 ± 66.32 | 182.61 ± 87.07 | 269.14 ± 28.29 | 178.55 ± 88.25 | <0.001 ** |
| Gamma-glutamyltransferase (U/L) | N/A * | 42.91 ± 109.77 | N/A * | 38.05 ± 27.57 | 0.460 |
| Bilirubin (umol/L) | 6.69 ± 3.49 | 13.31 ± 41.00 | 6.97 ± 2.27 | 7.84 ± 3.36 | 0.741 |
| Prothrombin time (seconds) | 10.84 ± 0.48 | 11.97 ± 2.19 | 11.50 ± 0.57 | 13.17 ± 4.35 | 0.358 |
| C-reactive protein (mg/L) | 27.00 ± 35.36 | 13.87 ± 31.47 | N/A * | 13.51 ± 14.19 | 0.844 |
| Hospital | Audit Results | p-Value | ||
|---|---|---|---|---|
| Level A (Total Score = 20–26) | Level B (Total Score = 13–19) | Level C (Total Score = 0–13) | ||
| n (%) | n (%) | n (%) | ||
| Hospital A (n = 36) | 25 (69.4%) | 9 (25%) | 2 (5.6%) | <0.001 * |
| Hospital B (n = 8) | 2 (25%) | 3 (37.5%) | 3 (37.5%) | |
| Hospital C (n = 14) | 0 (0%) | 9 (64.3%) | 5 (35.7%) | |
| Total (n = 58) | 27 (46.6%) | 21 (36.2%) | 10 (17.2%) | |
| Disease Parameters | Reported Dietitian Documentation | No Reported Dietitian Documentation | p-Value |
|---|---|---|---|
| n = 58 | n = 84 | ||
| Mean ± SD | Mean ± SD | ||
| Change in body mass index (kg/m2) * | −1.25 ± 2.97 | −1.07 ± 1.78 | 0.724 |
| Change in systolic blood pressure mmHg | −1.62 ± 14.82 | −1.73 ± 13.96 | 0.971 |
| Change in diastolic blood pressure mmHg | −0.86 ± 10.88 | −1.79 ± 10.34 | 0.677 |
| Change in triglycerides (mmol/L) | −0.03 ± 0.46 | 0.01 ± 0.0.77 | 0.854 |
| Change in total cholesterol (mmol/L) | 0.04 ± 0.70 | 0.31 ± 0.99 | 0.275 |
| Change in high-density lipoprotein (mmol/L) | 0.03 ± 0.24 | 0.34 ± 1.30 | 0.261 |
| Change in low-density lipoprotein (mmol/L) | 0.04 ± 0.67 | 0.09 ± 0.47 | 0.734 |
| Change in fasting blood glucose (mmol/L) | 0.59 ± 3.43 | 0.34 ± 3.28 | 0.869 |
| Change in alanine aminotransferase (U/L) | −2.87 ± 40.76 | 8.00 ± 24.39 | 0.261 |
| Change in aspartate aminotransferase (U/L) | −1.38 ± 23.04 | 4.87 ± 21.81 | 0.346 |
| Change in alkaline phosphatase (U/L) | 2.35 ± 54.77 | −8.29 ± 70.92 | 0.569 |
| Change in gamma-glutamyl transferase (U/L) | −7.08 ± 26.06 | 5.25 ± 16.14 | 0.135 |
| Change in bilirubin (umol/L) | −6.52 ± 30.93 | −15.76 ± 57.46 | 0.499 |
| Change in prothrombin time (seconds) | −1.80 ± 2.07 | −1.03 ± 2.01 | 0.574 |
| Disease Parameters | Level A (Total Score = 20–26) | Level B (Total Score = 13–19) | Level C (Total Score = 0–13) | p-Value |
|---|---|---|---|---|
| n = 27 | n = 21 | n = 10 | ||
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Change in body mass index (kg/m2) * | −1.56 ± 3.54 | −0.39 ± 1.53 | −2.10 ± 3.18 | 0.579 |
| Change in systolic blood pressure (mmHg) | −5.43 ± 14.29 | 4.23 ± 12.51 | −1.13 ± 18.11 | 0.453 |
| Change in diastolic blood pressure (mmHg) | −5.48 ± 8.11 | 3.54 ± 9.59 | 4.13 ± 14.83 | 0.218 |
| Change in triglycerides (mmol/L) | −0.08 ± 0.54 | −0.04 ± 0.47 | 0.08 ± 0.23 | 0.542 |
| Change in total cholesterol (mmol/L) | 0.06 ± 0.69 | 0.44 ± 0.60 | −0.58 ± 0.42 | 0.119 |
| Change in high-density lipoprotein (mmol/L) | 0.04 ± 0.29 | 0.09 ± 0.21 | −0.06 ± 0.07 | 0.215 |
| Change in low-density lipoprotein (mmol/L) | 0.06 ± 0.62 | 0.41 ± 0.67 | −0.55 ± 0.38 | 0.103 |
| Change in fasting blood glucose (mmol/L) | −0.03 ± 0.41 | −0.79 ± 1.67 | 6.50 ± 8.34 | 0.777 |
| Change in alanine aminotransferase (U/L) | −2.15 ± 10.74 | 1.79 ± 23.38 | −22.33 ± 121.16 | 0.364 |
| Change in aspartate aminotransferase (U/L) | −2.00 ± 17.86 | 1.17 ± 8.94 | −8.67 ± 64.44 | 0.452 |
| Change in alkaline phosphatase (U/L) | −11.33 ± 53.24 | −0.09 ± 38.49 | 52.33 ± 98.08 | 0.182 |
| Change in bilirubin (umol/L) | −0.13 ± 2.51 | −0.12 ± 1.70 | −49.20 ± 85.68 | 0.420 |
| Disease Parameters | Change from Baseline to 6 Months * | Change from 6 Months to 12 Months * | Change from Baseline to 12 Months * | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Group I | ||||||
| Change in body mass index | −0.275 | 0.241 | −0.445 | 0.084 | −0.315 | 0.188 |
| Group II | ||||||
| Change in body mass index | −0.298 | 0.322 | −0.761 ** | 0.007 | −0.326 | 0.301 |
| Change in alanine aminotransferase | 0.299 | 0.471 | 0.632 | 0.368 | 0.006 | 0.989 |
| Change in aspartate aminotransferase | 0.427 | 0.292 | −0.800 | 0.200 | 0.291 | 0.485 |
| Change in alkaline phosphatase | −0.275 | 0.509 | 0.400 | 0.600 | −0.790 ** | 0.02 |
| Change in gamma-glutamyl transferase | −0.090 | 0.848 | NA *** | NA *** | −0.116 | 0.827 |
| Change in bilirubin | −0.299 | 0.471 | NA *** | NA *** | 0.240 | 0.568 |
| Group III | ||||||
| Change in body mass index | 0.019 | 0.968 | 0.316 | 0.684 | 0.316 | 0.684 |
| Change in systolic blood pressure | 0.561 | 0.190 | −0.821 | 0.089 | 0.526 | 0.362 |
| Change in diastolic blood pressure | 0.661 | 0.106 | −0.821 | 0.089 | −0.205 | 0.741 |
| Change in total cholesterol | NA *** | NA *** | NA *** | NA *** | 0.500 | 0.667 |
| Change in high-density lipoprotein | NA *** | NA *** | NA *** | NA *** | 0.500 | 0.667 |
| Change in low-density lipoprotein | NA *** | NA *** | NA *** | NA *** | 0.500 | 0.667 |
| Group IV | ||||||
| Change in body mass index | −0.410 | 0.273 | 0.180 | 0.699 | 0.054 | 0.908 |
| Change in systolic blood pressure | 0.030 | 0.933 | −0.631 | 0.129 | −0.627 | 0.132 |
| Change in diastolic blood pressure | 0.027 | 0.940 | 0.711 | 0.074 | −0.100 | 0.831 |
| Change in triglycerides | −0.616 | 0.269 | NA *** | NA *** | −0.559 | 0.192 |
| Change in total cholesterol | −0.872 | 0.054 | −0.866 | 0.333 | 0.577 | 0.175 |
| Change in high-density lipoprotein | −0.616 | 0.269 | 0.866 | 0.333 | 0.667 | 0.102 |
| Change in low-density lipoprotein | −0.718 | 0.172 | −0.866 | 0.333 | 0.739 | 0.58 |
| Change in fasting blood glucose | 0.500 | 0.667 | NA *** | NA *** | NA *** | NA *** |
| Change in alanine aminotransferase | −0.500 | 0.667 | NA *** | NA *** | −0.414 | 0.355 |
| Change in aspartate aminotransferase | −0.500 | 0.667 | −0.500 | 0.667 | −0.414 | 0.355 |
| Change in alkaline phosphatase | −0.500 | 0.667 | −0.500 | 0.667 | 0.036 | 0.939 |
| Change in gamma-glutamyl transferase | 0.500 | 0.667 | −0.500 | 0.667 | −0.029 | 0.957 |
| Change in bilirubin | NA *** | NA *** | −0.500 | 0.667 | −0.234 | 0.613 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mujlli, G.; Aldisi, D.; Aljuraiban, G.S.; Abulmeaty, M.M.A. Impact of Nutrition Care Process Documentation in Obese Children and Adolescents with Metabolic Syndrome and/or Non-Alcoholic Fatty Liver Disease. Healthcare 2021, 9, 188. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9020188
Mujlli G, Aldisi D, Aljuraiban GS, Abulmeaty MMA. Impact of Nutrition Care Process Documentation in Obese Children and Adolescents with Metabolic Syndrome and/or Non-Alcoholic Fatty Liver Disease. Healthcare. 2021; 9(2):188. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9020188
Chicago/Turabian StyleMujlli, Gadah, Dara Aldisi, Ghadeer S. Aljuraiban, and Mahmoud M. A. Abulmeaty. 2021. "Impact of Nutrition Care Process Documentation in Obese Children and Adolescents with Metabolic Syndrome and/or Non-Alcoholic Fatty Liver Disease" Healthcare 9, no. 2: 188. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9020188