
Clinical Comparation of Extra-Short (4 mm) and Long (>8 mm) Dental Implants Placed in Mandibular Bone: A Systematic Review and Metanalysis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Focused Question
2.3. Implants Definition
2.4. Search Strategy
2.5. Eligibility Criteria and Study Selection Process
- Population: partially edentulous.
- Intervention: placement of extra-short 4 mm dental implants in the mandible
- Comparison: placement of long (>8 mm implants) in the mandible
- Outcomes: dental implant survival rate (primary outcome), marginal bone loss, biological complications (pain, exudate, peri-implant mucositis and peri-implantitis), and prosthetic complications (secondary outcome).
- Study design: RCTs and controlled clinical trials.
- Time: implants with follow-ups of 1–3 and 5 years
2.6. Data Synthesis
2.7. Assessments of the Risk of Bias
2.8. Statistical Analysis
2.9. Grading the Quality of Evidence
3. Results
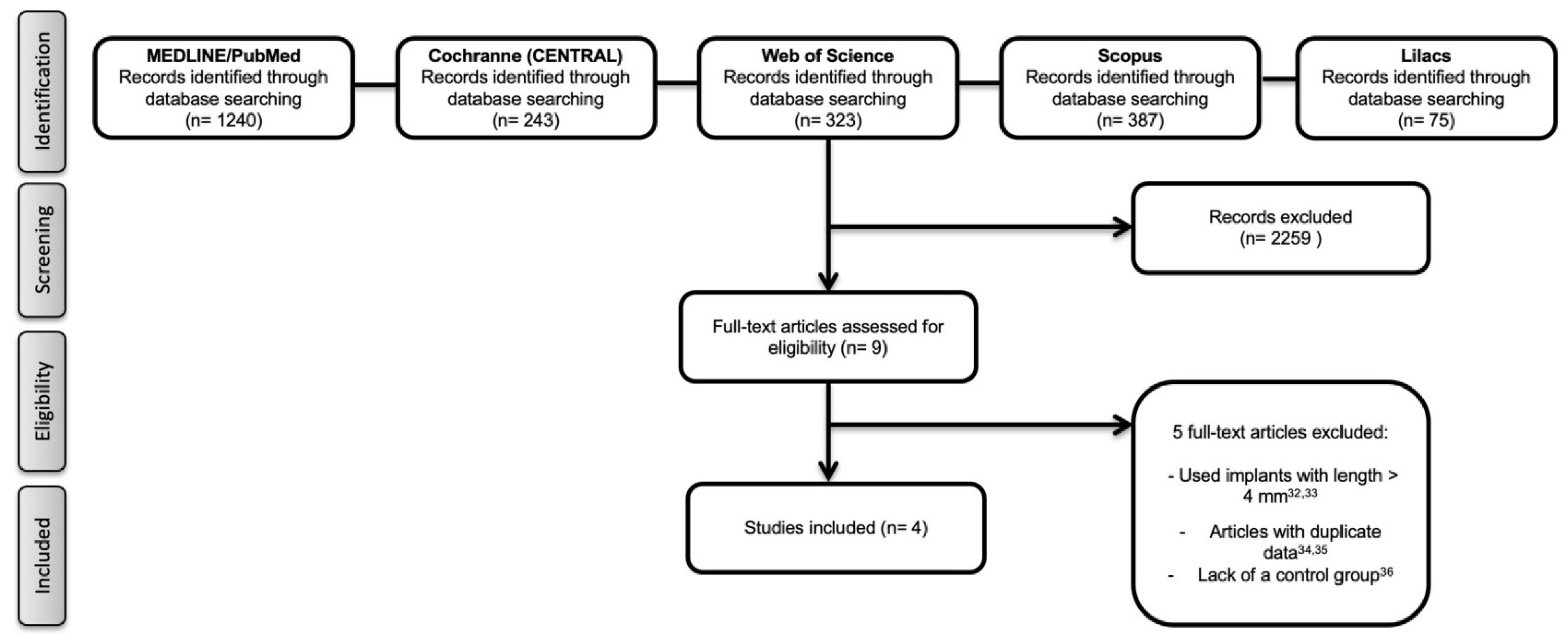
3.1. Literature Search
3.2. Study Characteristics
3.3. Meta-Analysis and Quality of Evidence
3.4. Biological Complications
3.5. Prosthetic Complications
3.6. Assessments of the Risk of Bias
4. Discussion
4.1. Summary of Evidence
4.2. Strengths and Limitations
4.3. Implications for Clinical Practice and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, C.-L.S. The impact of osseointegrated implants as an adjunct and alternative to conventional periodontal prosthesis. Compend. Contin. Educ. Dent. 2005, 26, 653. [Google Scholar]
- Pellegrini, G.; Francetti, L.; Barbaro, B.; Del Fabbro, M. Novel surfaces and osseointegration in implant dentistry. J. Investig. Clin. Dent. 2018, 9, e12349. [Google Scholar] [CrossRef]
- Alghamdi, H.S. Methods to Improve Osseointegration of Dental Implants in Low Quality (Type-IV) Bone: An Overview. J. Funct. Biomater. 2018, 9, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moraschini, V.; Poubel, L.D.C.; Ferreira, V.; Barboza, E.D.S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Ricci, M.; Tonelli, P.; Santini, S.; Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implant. Res. 2012, 24, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Orlando, B.; Cingano, L.; Marconcini, S.; Derchi, G.; Covani, U. A Randomized Clinical Trial to Evaluate and Compare Implants Placed in Augmented Versus Non-Augmented Extraction Sockets: 3-Year Results. J. Periodontol. 2012, 83, 836–846. [Google Scholar] [CrossRef]
- Aloy-Prósper, A.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M.A. The outcome of intraoral onlay block bone grafts on alveolar ridge augmentations: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e251–e258. [Google Scholar] [CrossRef] [PubMed]
- Younis, M.; Elshahat, A.; Elhabbaa, G.; Fareed, A.; Safe, I. Onlay Bone Graft Maintenance Using Guided Bone Regeneration, Platelet Rich Plasma, and Their Combination. J. Craniofac. Surg. 2014, 25, 2237–2240. [Google Scholar] [CrossRef] [PubMed]
- Cucchi, A.; Ghensi, P. Vertical Guided Bone Regeneration using Titanium-reinforced d-PTFE Membrane and Prehydrated Corticocancellous Bone Graft. Open Dent. J. 2014, 8, 194–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledano-Serrabona, J.; Sánchez-Garcés, M.Á.; Sánchez-Torres, A.; Gay-Escoda, C. Alveolar distraction osteogenesis for dental implant treatments of the vertical bone atrophy: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2018, 24, e70–e75. [Google Scholar] [CrossRef] [PubMed]
- Baghban, A.A.; Dehghani, A.; Ghanavati, F.; Zayeri, F.; Ghanavati, F. Comparing alveolar bone regeneration using Bio-Oss and autogenous bone grafts in humans: A systematic review and meta-analysis. Iran. Endod. J. 2009, 4, 125–130. [Google Scholar]
- Ghensi, P.; Stablum, W.; Bettio, E.; Soldini, M.; Tripi, T.; Soldini, C. Management of the exposure of a dense ptfe (d-PTFE) membrane in guided bone regeneration (GBR): A case report. Oral Implantol. 2017, 10, 335–342. [Google Scholar] [CrossRef]
- Lim, G.; Lin, G.-H.; Monje, A.; Chan, H.-L.; Wang, H.-L. Wound Healing Complications Following Guided Bone Regeneration for Ridge Augmentation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Fretwurst, T.; Wanner, L.; Nahles, S.; Raguse, J.; Stricker, A.; Metzger, M.; Nelson, K. A prospective study of factors influencing morbidity after iliac crest harvesting for oral onlay grafting. J. Cranio-Maxillofac. Surg. 2015, 43, 705–709. [Google Scholar] [CrossRef]
- Chiapasco, M.; Zaniboni, M. Failures in Jaw Reconstructive Surgery with Autogenous Onlay Bone Grafts for Pre-implant Purposes: Incidence, Prevention and Management of Complications. Oral Maxillofac. Surg. Clin. N. Am. 2011, 23, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Verardi, S.; Simion, M. Management of the exposure of e-PTFE membranes in guided bone regeneration. Pr. Proced. Aesthet. Dent. PPAD 2007, 19, 111–117. [Google Scholar]
- Garcia, J.; Dodge, A.; Luepke, P.; Wang, H.-L.; Kapila, Y.; Lin, G.-H. Effect of membrane exposure on guided bone regeneration: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoma, D.S.; Cha, J.-K.; Jung, U.-W. Treatment concepts for the posterior maxilla and mandible: Short implants versus long implants in augmented bone. J. Periodontal Implant. Sci. 2017, 47, 2–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravidà, A.; Wang, I.-C.; Barootchi, S.; Askar, H.; Tavelli, L.; Gargallo-Albiol, J.; Wang, H.-L. Meta-analysis of randomized clinical trials comparing clinical and patient-reported outcomes between extra-short (≤6 mm) and longer (≥10 mm) implants. J. Clin. Periodontol. 2018, 46, 118–142. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Lang, N.P.; Ricci, E.; Ferraioli, L.; Marchetti, C.; Botticelli, D. 6-mm-long implants loaded with fiber-reinforced composite resin-bonded fixed prostheses (FRCRBFDPs). A 5-year prospective study. Clin. Oral Implant. Res. 2017, 28, 1478–1483. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Katsoulis, J.; Koka, S.; Igarashi, K. Single versus splinted short implants at sinus augmented sites: A systematic review and meta-analysis. J. Stomatol. Oral Maxillofac. Surg. 2020, in press. [Google Scholar] [CrossRef]
- Bolle, C.; Felice, P.; Barausse, C.; Pistilli, V.; Trullenque-Eriksson, A.; Esposito, M. 4 mm long vs longer implants in augmented bone in posterior atrophic jaws: 1-year post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implant. 2018, 11, 31–47. [Google Scholar]
- Monje, A.; Fu, J.H.; Chan, H.L.; Suarez, F.; Galindo-Moreno, P.; Catena, A.; Wang, H.L. Do implant length and width matter for short dental implants (<10 mm)? A meta-analysis of prospective studies. J. Periodontol. 2013, 84, 1783–1791. [Google Scholar]
- Rokn, A.R.; Monzavi, A.; Panjnoush, M.; Hashemi, H.M.; Dds, M.J.K.; Bitaraf, T. Comparing 4-mm dental implants to longer implants placed in augmented bones in the atrophic posterior mandibles: One-year results of a randomized controlled trial. Clin. Implant. Dent. Relat. Res. 2018, 20, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.A.; Ferro-Alves, M.L.; Okamoto, R.; Mendonça, M.R.; Pellizzer, E.P. Short dental implants versus standard dental implants placed in the posterior jaws: A systematic review and meta-analysis. J. Dent. 2016, 47, 8–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Cannizzaro, G.; Felice, P.; Buti, J.; Leone, M.; Ferri, V.; Esposito, M. Immediate loading of fixed cross-arch prostheses supported by flapless-placed supershort or long implants: 1-year results from a randomised controlled trial. Eur. J. Oral Implant. 2015, 8, 27–36. [Google Scholar]
- Gastaldi, G.; Felice, P.; Pistilli, R.; Barausse, C.; Trullenque-Eriksson, A.; Esposito, M. Short implants as an alternative to crestal sinus lift: A 3-year multicentre randomised controlled trial. Eur. J. Oral Implant. 2017, 10, 391–400. [Google Scholar]
- Esposito, M.; Zucchelli, G.; Barausse, C.; Pistilli, R.; Trullenque-Eriksson, A.; Felice, P. Four mm-long versus longer implants in augmented bone in atrophic posterior jaws: 4-month post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implant. 2016, 9, 393–409. [Google Scholar]
- Esposito, M.; Barausse, C.; Pistilli, R.; Checchi, V.; Diazzi, M.; Gatto, M.R.; Felice, P. Posterior jaws rehabilitated with partial prostheses supported by 4.0 × 4.0 mm or by longer implants: Four-month post-loading data from a randomised controlled trial. Eur. J. Oral Implant. 2015, 8, 221–230. [Google Scholar]
- Slotte, C.; Grønningsaeter, A.; Halmøy, A.-M.; Öhrnell, L.-O.; Mordenfeld, A.; Isaksson, S.; Johansson, L.-Å. Four-Millimeter-Long Posterior-Mandible Implants: 5-Year Outcomes of a Prospective Multicenter Study. Clin. Implant. Dent. Relat. Res. 2014, 17, e385–e395. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; López Torres, J.A.; Dard, M.; Javed, F.; Pérez-Albacete Martínez, C.; Maté Sánchez de Val, J.E. Evaluation of extrashort 4-mm implants in mandibular edentulous patients with reduced bone height in comparison with standard implants: A 12-month results. Clin. Oral Implant. Res. 2016, 27, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Felice, P.; Checchi, L.; Barausse, C.; Pistilli, R.; Sammartino, G.; Masi, I.; Ippolito, D.R.; Esposito, M. Posterior jaws rehabilitated with partial prostheses supported by 4.0 × 4.0 mm or by longer implants: One-year post-loading results from a multicenter randomised controlled trial. Eur. J. Oral Implant. 2016, 9, 35–45. [Google Scholar]
- Papaspyridakos, P.; De Souza, A.; Vazouras, K.; Gholami, H.; Pagni, S.; Weber, H. Survival rates of short dental implants (≤6 mm) compared with implants longer than 6 mm in posterior jaw areas: A meta-analysis. Clin. Oral Implant. Res. 2018, 29, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Malchiodi, L.; Giacomazzi, E.; Cucchi, A.; Ricciotti, G.; Caricasulo, R.; Bertossi, D.; Gherlone, E. Relationship Between Crestal Bone Levels and Crown-to-Implant Ratio of Ultra-Short Implants with a Microrough Surface: A Prospective Study With 48 Months of Follow-Up. J. Oral Implant. 2019, 45, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant. Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hingsammer, L.; Pommer, B.; Hunger, S.; Stehrer, R.; Watzek, G.; Insua, A. Influence of implant length and associated parameters upon biomechanical forces in finite element analyses: A systematic review. Implant. Dent. 2019, 28, 296–305. [Google Scholar] [CrossRef]
- Ravidà, A.; Saleh, M.H.A.; Muriel, M.C.; Maska, B.; Wang, H.L. Biological and technical complications of splinted or nonsplinted dental implants: A decision tree for selection. Implant. Dent. 2018, 27, 89–94. [Google Scholar] [CrossRef]
- Garaicoa-Pazmiño, C.; Del Amo, F.S.-L.; Monje, A.; Catena, A.; Ortega-Oller, I.; Galindo-Moreno, P.; Wang, H.-L. Influence of Crown/Implant Ratio on Marginal Bone Loss: A Systematic Review. J. Periodontol. 2014, 85, 1214–1221. [Google Scholar] [CrossRef]
- Nunes, M.; Almeida, R.F.; Felino, A.C.; Malo, P.; de Araújo Nobre, M. The Influence of Crown-to-Implant Ratio on Short Implant Marginal Bone Loss. Int. J. Oral Maxillofac. Implant. 2016, 31, 1156–1163. [Google Scholar] [CrossRef]
- Vazouras, K.; De Souza, A.B.; Gholami, H.; Papaspyridakos, P.; Pagni, S.; Weber, H.-P. Effect of time in function on the predictability of short dental implants (≤6 mm): A meta-analysis. J. Oral Rehabil. 2019, 47, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Barboza, E.D.P. Success of dental implants in smokers and non-smokers: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Smoking and dental implants: A systematic review and meta-analysis. J. Dent. 2015, 43, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Alfadda, S.A. Current Evidence on Dental Implants Outcomes in Smokers and Nonsmokers: A Systematic Review and Meta-Analysis. J. Oral Implantol. 2018, 44, 390–399. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Study Design No. of Participants | Follow-Up (Months) | Implant Location | No. of Implants Implant Brand Surface Type | Implant Size (Diameter × Length) | Loading Protocol | No. of Smokers | Primary Stability (Ncm or ISQ) | Implant Survival Rate (No. of Failures) | Marginal Bone Loss (Mean ± SD) (mm) | Prosthetic Complication (No. of Failures) | Biological Complications | Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Felice et al., 2016 | RCT (parallel) 150 | 12 | PM M | SI: 78 TwinKon Rough CI: 47 TwinKon Rough | SI: 4.0 × 4.0 LI: 4.0 × 8.5, 10, 11.5, 13 | Delayed | SI: 20 LI: 12 | >25 Ncm | SI: 96% (3) LI: 97.3% (2) | SI: 0.53 ± 0.23 LI: 0.57 ± 0.33 | SI: 97.3% (2) LI: 97.3% (2) | SI: 4 LI: 2 | This study indicated that 4.0 × 4.0 mm implants, one year after loading, achieved similar results to 8.5 × 4.0 mm long or longer implants in the presence of adequate bone volumes. |
| Calvo-Guitrado et al., 2016 | CCT 60 | 12 | PM M | SI: 40 Strauman Rough LI: 20 Strauman Rough | SI: 4.1 × 4.0 LI: 4.1 × 10 | Delayed | NR | >25 Ncm | SI: 97.5% (1) LI: 100% (0) | SI: 0.71 ± 0.11 LI: 0.89 ± 0.23 | SI: 100% (0) LI: 100% (0) | NR | Extra-short dental implants supporting single crowns or FDP are a feasible treatment option with radiographic and clinical success rates similar to longer implants for patients with compromised ridges |
| Rokn et al., 2018 | RCT (parallel) 11 | 12 | PM M | SI: 25 Strauman Rough LI: 22 Strauman Rough | SI: 4.1 × 4.0 LI: 4.1 × 8.0, 10 | Delayed | NR | NR | SI: 100% (0) LI: 100% (0) | SI: 0.30 ± 0.34 LI: 0.47 ± 0.54 | SI: 100% (0) LI: 100% (0) | SI: 0 LI: 8 | This study showed that 4 mm dental implants and longer implants provided acceptable outcomes up to 1 year after loading |
| Bolle et al., 2018 | RCT (parallel) 80 | 12 | PM M | SI: 43 TwinKon Rough LI: 46 TwinKon Rough | SI: 4.0, 4.5 × 4.0 LI: 4.0 × 8.5, 10, 11.5, 13 | Delayed | SI: 2 LI: 8 | >25 Ncm | SI: 88.4% (5) LI: 82.7% (8) | SI: 0.57± 0.16 LI: 0.75 ± 0.23 | SI: 95% (2) LI: 84.7% (6) | SI: 6 LI: 23 | This study showed that, one year after loading, 4.0 mm long implants achieved similar results than longer implants and were affected by fewer complications. |
| Outcomes | Anticipated Absolute Effects * (95% CI) | Relative Effect (95% CI) | No of Participants (Studies) | Certainty of the Evidence (GRADE) | Comments | |
|---|---|---|---|---|---|---|
| Risk with Extra-Short 4 mm Dental Implants | Risk with Long Implants | |||||
| Implant survival rate Follow up: mean 12 months | 1.000 per 1.000 | 870 per 1.000 (370 to 1.000) | RR 0.87 (0.37 to 2.03) | 436 (4 RCTs) | ⨁⨁⨁⨁ HIGH | Nonsignificant effect |
| Marginal bone loss Follow up: mean 12 months | The mean marginal bone loss was 0.52 mm | MD 0.13 204 lower (0.29 lower to 0.07 lower) | 436 (4 RCTs) | ⨁⨁⨁◯ MODERATE a,b | Significant effect | |
| Authors (Year) | Adequate Sequence Generation | Allocation Concealment | Blinding | Incomplete Outcome Data Addressed | Selective Outcome Reporting | Free of Other Souces of Bias | Estimated Potential Risk of Bias |
|---|---|---|---|---|---|---|---|
| Felice et al., 2016 | Yes | Unclear | Yes | Yes | Yes | Yes | Moderate risk |
| Calvo-Guirado et al., 2016 | Yes | Unclear | Yes | Yes | Yes | Yes | Moderate Risk |
| Rokn et al., 2018 | Yes | Yes | Yes | Yes | Yes | Yes | Low risk |
| Bolle et al., 2018 | Yes | Yes | Yes | Yes | Yes | Yes | Low Risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moraschini, V.; Mourão, C.F.d.A.B.; Montemezzi, P.; Kischinhevsky, I.C.C.; de Almeida, D.C.F.; Javid, K.; Shibli, J.A.; Granjeiro, J.M.; Calasans-Maia, M.D. Clinical Comparation of Extra-Short (4 mm) and Long (>8 mm) Dental Implants Placed in Mandibular Bone: A Systematic Review and Metanalysis. Healthcare 2021, 9, 315. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030315
Moraschini V, Mourão CFdAB, Montemezzi P, Kischinhevsky ICC, de Almeida DCF, Javid K, Shibli JA, Granjeiro JM, Calasans-Maia MD. Clinical Comparation of Extra-Short (4 mm) and Long (>8 mm) Dental Implants Placed in Mandibular Bone: A Systematic Review and Metanalysis. Healthcare. 2021; 9(3):315. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030315
Chicago/Turabian StyleMoraschini, Vittorio, Carlos Fernando de Almeida Barros Mourão, Pietro Montemezzi, Ingrid Chaves Cavalcante Kischinhevsky, Daniel Costa Ferreira de Almeida, Kayvon Javid, Jamil Awad Shibli, José Mauro Granjeiro, and Monica Diuana Calasans-Maia. 2021. "Clinical Comparation of Extra-Short (4 mm) and Long (>8 mm) Dental Implants Placed in Mandibular Bone: A Systematic Review and Metanalysis" Healthcare 9, no. 3: 315. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030315