
Development and Evaluation of Psychometric Properties Regarding the Whole Person Health Scale for Employees of Hospital to Emphasize the Importance of Health Awareness of the Workers in the Hospital


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Measures
Recruitment Focus Group Participants to Develop and Validate Initial Questionnaire
2.3. Analysis
3. Results
3.1. Demographic Characteristics of the Participants
3.2. Item Analysis
3.3. Exploratory Factor Analysis and Reliability
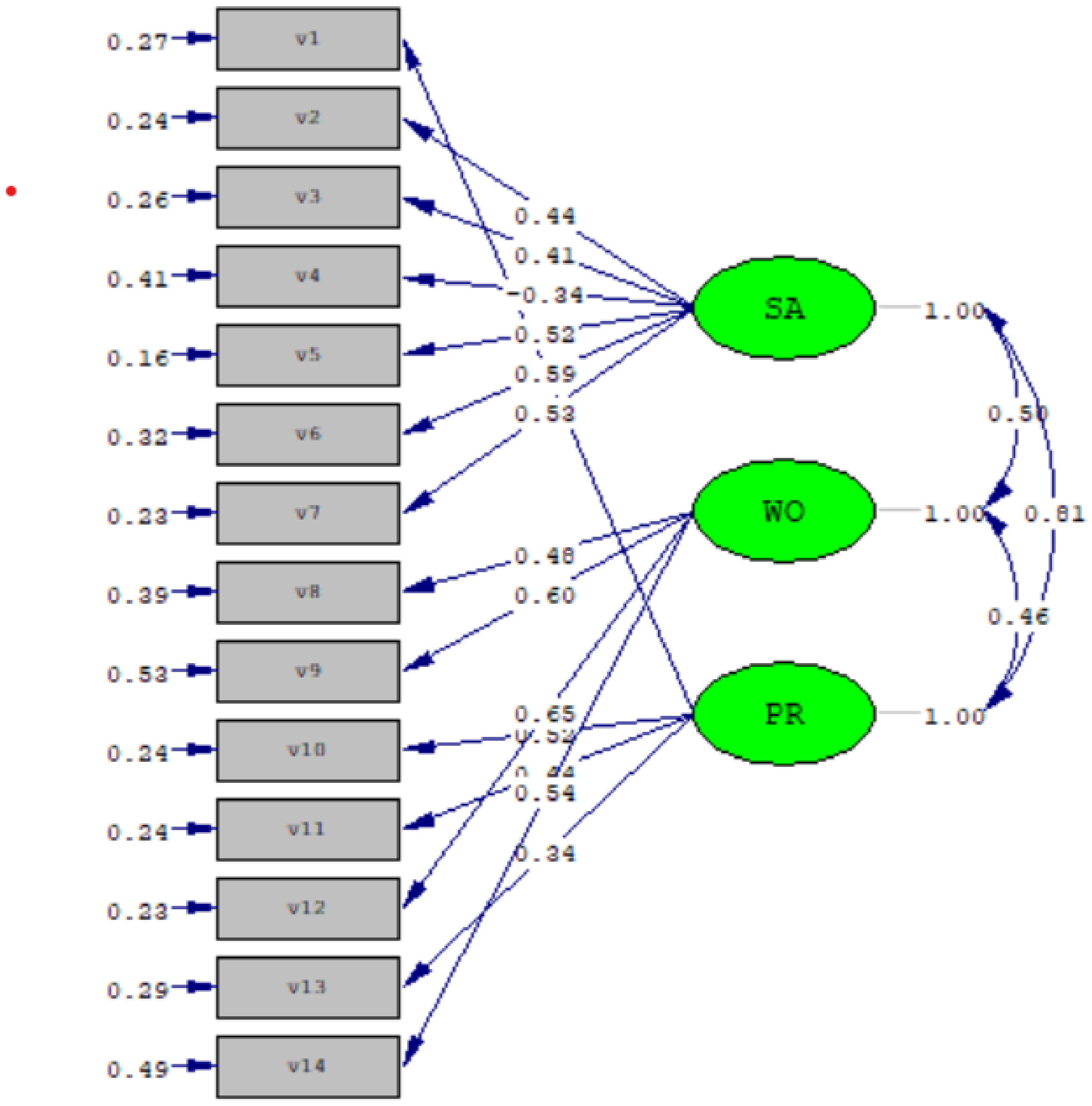
3.4. Confirmatory Factor Analysis for Construct Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Remains Firmly Committed to the Principles Set Out in the Preamble to the Constitution. 1946. Available online: https://www.who.int/about/who-we-are/constitution (accessed on 28 November 2020).
- Ewles, L.; Simnett, I. Promoting Health: A Practical Guide; Baillière Tindall: Edinburgh, UK; New York, NY, USA, 2010. [Google Scholar]
- Last, J.M. A Dictionary of Public Health; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Kiefer, R.A. An integrative review of the concept of well-being. Holist. Nurs. Pract. 2008, 22, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Montano, D.; Reeske, A.; Franke, F.; Hüffmeier, J. Leadership, followers’ mental health and job performance in organizations: A comprehensive meta-analysis from an occupational health perspective. J. Organ. Behav. 2017, 38, 327–350. [Google Scholar] [CrossRef]
- Maslach, C. Understanding burnout: Definition issues in analyzing a complex phenomenon. In Job Stress and Burnout: Research, Theory, and Intervention Perspectives; Paine, W.S., Ed.; Sage: Beverly Hills, CA, USA, 1981; pp. 29–40. [Google Scholar]
- Healy, C.M.; McKay, M.F. Nursing stress: The effects of coping strategies and job satisfaction in a sample of Australian. J. Adv. Nurs. 2000, 31, 681–688. [Google Scholar] [CrossRef] [PubMed]
- McGowan, B. Self-reported stress and its effects on nurses. Nurs. Stand. 2001, 15, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Siu, O.L. Predictors of job satisfaction and absenteeism in two samples of Hong Kong nurses. J. Adv. Nurs. 2002, 40, 218–229. [Google Scholar] [CrossRef] [PubMed]
- Garretson, S. Nurse to patient ratios in American health care. Nurs. Stand. 2004, 19, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.L. It alleviates health cares “healing crisis”. Nurs. Manag. 2002, 33, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.J.; Kim, O.; Kim, S.; Kim, M.S.; Choi, J.A.; Kim, B.; Dan, H.; Jung, H. Factors affecting physical and mental fatigue among female hospital nurses: The Korea nurses’ health study. Healthcare 2021, 9, 201. [Google Scholar] [CrossRef] [PubMed]
- Muthuri, R.N.D.K.; Senkubuge, F.; Hongoro, C. Predictors of Health-Related Quality of Life among Healthcare Workers in the Context of Health System Strengthening in Kenya. Healthcare 2021, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Bringsén, Å.; Ejlertsson, G.; Andersson, I.H. Flow situations during everyday practice in a medical hospital ward. Results from a study based on the experience sampling method. BMC Nurs. 2011, 10, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. Psychol. Assess. 1995, 7, 309–319. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Nursing Research 9th, Measurement and Data Quality; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Strickland, O.L. Using factor analysis for validity assessment: Practical considerations. J. Nurs. Meas. 2003, 11, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Li, P.Y.; Chen, H.W.; Yang, Y.C.; Tsai, L.Y.; Lai, M.L.; Bridge, D.T.; Fang, C.K. Using the demoralization scale for the early detection of demoralization in health professionals. Educ. Res. 2011, 2, 1648–1653. [Google Scholar]
- Fang, C.K.; Li, P.Y.; Lai, M.L.; Lin, M.H.; Bridge, D.T.; Chen, H.W. Establishing a ‘Physician’s Spiritual Well-being Scale’ and testing its reliability and validity. J. Med. Ethics 2011, 37, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, T.A. Current methodological considerations in exploratory and confirmatory Factor Analysis. J Psychol. Assess. 2011, 29, 304–321. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Item | N (%) | Mean | SD | |
|---|---|---|---|---|
| Age (years) | 37.6 | ± | 10.7 | |
| Work experience (years) | 11.8 | ± | 9.8 | |
| Gender | ||||
| Male | 102 (11.9) | |||
| Female | 752 (88.1) | |||
| Working department | ||||
| Doctor | 33 (3.9) | |||
| Nurse | 501 (58.7) | |||
| Medical technician | 129 (15.1) | |||
| Administrator | 135 (15.8) | |||
| Other | 46 (5.4) | |||
| No answer | 10 (1.1) |
| Questionaire Items | Mean | SD | Skewness | Kurtosis | t | 95% Confidence Interval | Correlation | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Statistic | Std. Error | Statistic | Std. Error | Lower | Upper | with Total Score | ||||
| Total score of scale | 38.7 | 5.6 | ||||||||
| Q 1. | 3.2 | 0.6 | −0.36 | 0.084 | 0.082 | 0.167 | −1.33 | −0.16 | 0.03 | 0.47 ** |
| Q 2. | 3.0 | 0.7 | −0.318 | 0.084 | 0.295 | 0.167 | −19.56 ** | −1.51 | −1.23 | 0.67 ** |
| Q 3. | 3.2 | 0.7 | −0.436 | 0.084 | 0.023 | 0.167 | −16.27 ** | −1.50 | −1.17 | 0.58 ** |
| Q 4. | 2.1 | 0.7 | 0.025 | 0.084 | −0.741 | 0.167 | 2.05 * | 0.01 | 0.41 | 0.66 ** |
| Q 5. | 2.9 | 0.7 | −0.301 | 0.084 | 0.273 | 0.167 | −18.69 ** | −1.53 | −1.23 | 0.71 ** |
| Q 6. | 2.6 | 0.8 | −0.155 | 0.084 | −0.469 | 0.167 | −24.06 ** | −1.96 | −1.67 | 0.67 ** |
| Q 7. | 2.8 | 0.7 | −0.120 | 0.084 | −0.324 | 0.167 | −28.34 ** | −1.68 | −1.46 | 0.66 ** |
| Q 8. | 3.1 | 0.8 | −0.718 | 0.084 | 0.346 | 0.167 | −19.59 ** | −1.08 | −0.88 | 0.63 ** |
| Q 9. | 2.5 | 0.9 | −0.258 | 0.084 | −0.901 | 0.167 | −26.07 ** | −1.47 | −1.27 | 0.55 ** |
| Q 10. | 2.7 | 0.7 | −0.247 | 0.084 | −0.068 | 0.167 | −9.36 ** | −0.59 | −0.38 | 0.69 ** |
| Q 11. | 2.7 | 0.7 | −0.141 | 0.084 | −0.096 | 0.167 | −5.32 ** | −0.36 | −0.17 | 0.60 ** |
| Q 12. | 2.6 | 0.8 | −0.470 | 0.084 | −0.357 | 0.167 | −26.54 ** | −1.28 | −1.11 | 0.62 ** |
| Q 13. | 2.8 | 0.6 | −0.203 | 0.084 | 0.153 | 0.167 | −1.70 | −0.18 | 0.01 | 0.46 ** |
| Q 14. | 2.5 | 0.9 | −0.159 | 0.084 | −0.746 | 0.167 | −25.72 ** | −1.37 | −1.18 | 0.55 ** |
| Questionaire Items | Factor Loading | ||
|---|---|---|---|
| I | II | III | |
| Factor 1: Hospital circumstance and system | |||
| 2. My working environment and equipment are suitable | 0.558 | ||
| 3. The medical resources at my hospital are sufficient | 0.628 | ||
| 4. I can get meaning from the feedback from my patients | 0.594 | ||
| 5. I can adapt to the hospital system | 0.688 | ||
| 6. My salary is sufficient | 0.771 | ||
| 7. The welfare provided by the hospital is enough | 0.787 | ||
| Factor 2: Workload and harm | |||
| 8. I need to leave my job | 0.640 | ||
| 9. The workforce in my department is insufficient | 0.733 | ||
| 12. My workload is too heavy | 0.821 | ||
| 14. I am at risk of occupational injuries | 0.743 | ||
| Factor 3: Professional and interpersonal interaction | |||
| 1. I interact well with my colleagues | 0.624 | ||
| 10. I am well balanced in all aspects of my body, mind, and soul | 0.592 | ||
| 11. My opinions are heard by others | 0.722 | ||
| 13. My professional skillset is utilized | 0.736 | ||
| Components | Mean | SD | Cronbach’s α | Correlation between 3 Factors and Total Score a |
|---|---|---|---|---|
| Total score of the scale | 38.7 | 5.6 | 0.82 | |
| Factor 1: Hospital circumstance and system | 16.7 | 2.5 | 0.78 | 0.82 ** |
| Factor 2: Workload and harm | 10.6 | 2.6 | 0.74 | 0.73 ** |
| Factor 3: Professional and interpersonal interaction | 11.4 | 1.9 | 0.64 | 0.74 ** |
| Three-Factor Model | X2/df | GFI | AGFI | NNFI | NFI | CFI | IFI | RFI | PNFI | PGFI |
|---|---|---|---|---|---|---|---|---|---|---|
| Scale | 539/105 = 5.1 | 0.93 | 0.90 | 0.95 | 0.95 | 0.96 | 0.96 | 0.94 | 0.77 | 0.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.-J.; Pi, S.-H.; Fang, C.-K.; Wu, T.-Y. Development and Evaluation of Psychometric Properties Regarding the Whole Person Health Scale for Employees of Hospital to Emphasize the Importance of Health Awareness of the Workers in the Hospital. Healthcare 2021, 9, 610. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050610
Liu C-J, Pi S-H, Fang C-K, Wu T-Y. Development and Evaluation of Psychometric Properties Regarding the Whole Person Health Scale for Employees of Hospital to Emphasize the Importance of Health Awareness of the Workers in the Hospital. Healthcare. 2021; 9(5):610. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050610
Chicago/Turabian StyleLiu, Chih-Ju, Shih-Hsuan Pi, Chun-Kai Fang, and Te-Yu Wu. 2021. "Development and Evaluation of Psychometric Properties Regarding the Whole Person Health Scale for Employees of Hospital to Emphasize the Importance of Health Awareness of the Workers in the Hospital" Healthcare 9, no. 5: 610. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050610