
Aggressions on Social Networks: What Are the Implications for Healthcare Providers? An Exploratory Research

 , , , and
, , , and {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
- -
- Presence of at least one noun/adjective/adverb with a negative connotation (e.g., coldness, insensibility)
- -
- Presence of threats/swear words
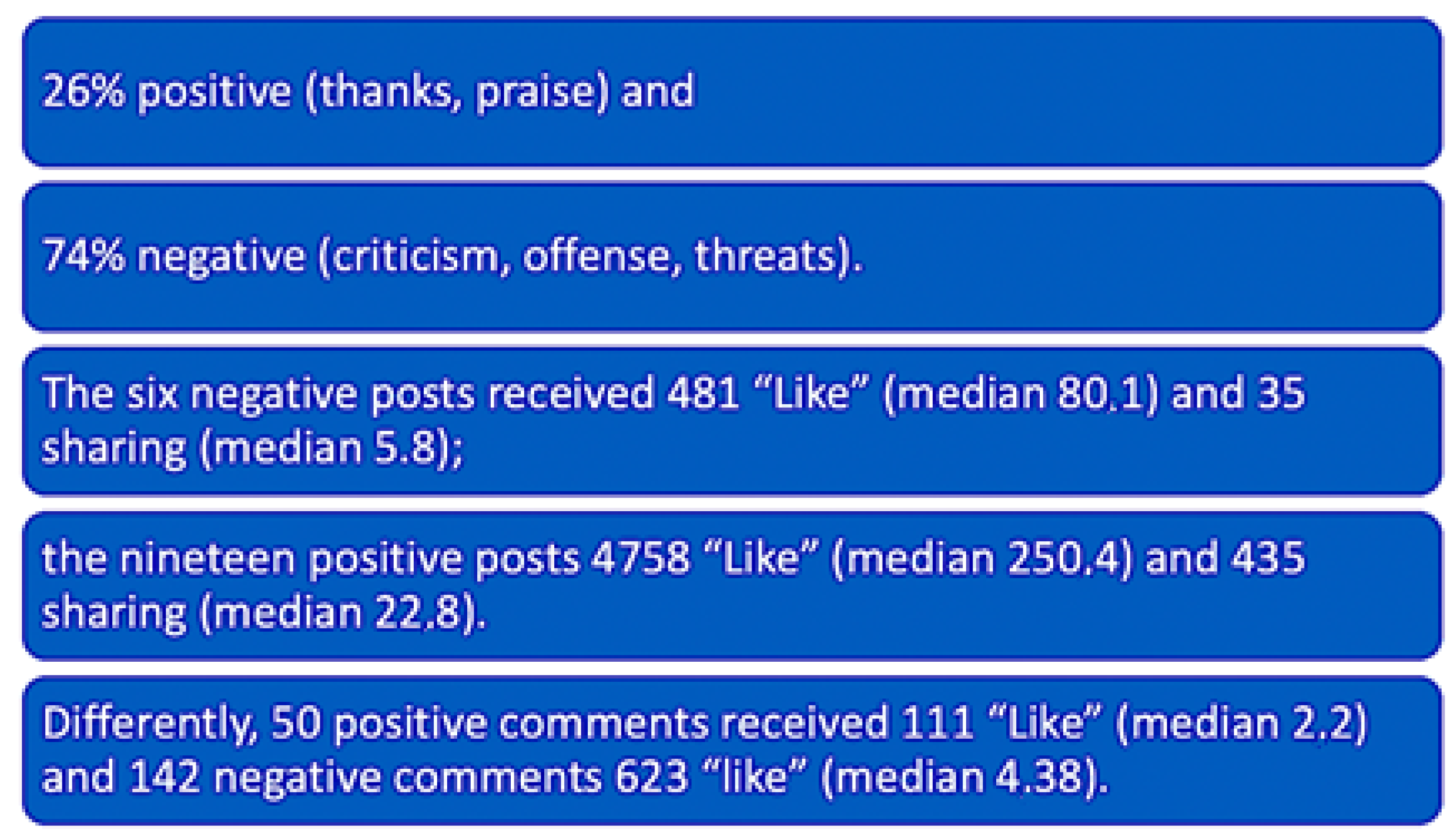
3. Results
- 1
- lack of adequate and functional structures
- 2
- negative point of view (POV) of users towards some departments
- 3
- positive POV towards other departments.
4. Discussion
- (a)
- the facilitation of the process of reporting the act of violence;
- (b)
- the collection of data and their analysis;
- (c)
- (1)
- Adequate accountability mechanism by governments against perpetrators of violence against health personnel;
- (2)
- Accurate and systematic data collection on violent incidents in relation to the pandemic to document the phenomenon across the globe;
- (3)
- Effective information campaigns to keep the public informed and stop misinformation related to COVID-19 contamination;
- (4)
- Close cooperation between local/state authorities, health professionals’ organizations and other relevant health actors, as well as media organizations, to denounce and prevent the problem of violence [34].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raccomandazione per Prevenire gli Atti di Violenza a Danno Degli Operatori Sanitari. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_721_allegato.pdf (accessed on 23 June 2021).
- Pershad, Y.; Hangge, P.T.; Albadawi, H.; Oklu, R. Social Medicine: Twitter in Healthcare. J. Clin. Med. 2018, 7, 121. [Google Scholar] [CrossRef] [Green Version]
- Van Hee, C.; Jacobs, G.; Emmery, C.; Desmet, B.; Lefever, E.; Verhoeven, B.; De Pauw, G.; Daelemans, W.; Hoste, V. Automatic detection of cyberbullying in social media text. PLoS ONE 2018, 13, e0203794. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Strategy and Plan of Action on Hate Speech. May 2019. Available online: https://www.un.org/en/genocideprevention/documents/advising-and-mobilizing/Action_plan_on_hate_speech_EN.pdf (accessed on 23 June 2021).
- Deirmenjian, J.M. Stalking in cyberspace. J. Am. Acad. Psychiatry Law 1999, 27, 407–413. [Google Scholar] [PubMed]
- Legge 14 agosto 2020, n. 113. Disposizioni in Materia di Sicurezza per gli Esercenti le Professioni Sanitarie e Socio-Sanitarie nell’esercizio delle Proprie Funzioni. Available online: https://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=76120 (accessed on 23 June 2021).
- Larkin, H. Navigating attacks against health care workers in the COVID-19 era. JAMA 2021, 325, 1822–1824. [Google Scholar] [CrossRef] [PubMed]
- Guarini, A.; Menin, D.; Menabò, L.; Brighi, A. RPC Teacher-Based Program for Improving Coping Strategies to Deal with Cyberbullying. Int. J. Environ. Res. Public Health 2019, 16, 948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.; Park, M. Effects of nursing organisational culture on face-to-face bullying and cyberbullying in the workplace. J. Clin. Nurs. 2019, 28, 2577–2588. [Google Scholar] [CrossRef]
- Farley, S.; Coyne, I.; Sprigg, C.; Axtell, C.; Subramanian, G. Exploring the impact of workplace cyberbullying on trainee doctors. Med. Educ. 2015, 49, 436–443. [Google Scholar] [CrossRef]
- Granstra, K. Nurse Against Nurse: Horizontal Bullying in the Nursing Profession. J. Healthc. Manag. 2015, 60, 249–257. [Google Scholar] [CrossRef]
- Park, M.; Choi, J.S. Effects of workplace cyberbullying on nurses’ symptom experience and turnover intention. J. Nurs. Manag. 2019, 27, 1108–1115. [Google Scholar] [CrossRef]
- Huesch, M.D.; Currid-Halkett, E.; Doctor, J.N. Public hospital quality report awareness: Evidence from National and Californian Internet searches and social media mentions. BMJ Open 2014, 4, e004417. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.A.; Sap, M.; Schwartz, A.; Town, R.; Baker, T.; Ungar, L.; Merchant, R.M. Twitter sentiment predicts affordable care act marketplace enrollment. J. Med. Internet Res. 2015, 17, e51. [Google Scholar] [CrossRef] [Green Version]
- Glover, M.; Khalilzadeh, O.; Choy, G.; Prabhakar, A.M.; Pandharipande, P.V.; Gazelle, G.S. Hospital evaluations by social media: A comparative analysis of Facebook ratings among performance outliers. J. Gen. Intern. Med. 2015, 30, 1440–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, B.C.; Paul, M.J.; Sarkar, U.; Trikalinos, T.A.; Dredze, M. A large-scale quantitative analysis of latent factors and sentiment in online doctor reviews. J. Am. Med. Inform. Assoc. 2014, 21, 1098–1103. [Google Scholar] [CrossRef] [PubMed]
- Greaves, F.; Laverty, A.A.; Cano, D.R.; Moilanen, K.; Pulman, S.; Darzi, A.; Millett, C. Tweets about hospital quality: A mixed methods study. BMJ Qual. Saf. 2014, 23, 838–846. [Google Scholar] [CrossRef] [Green Version]
- Verhoef, L.M.; Van de Belt, T.H.; Engelen, L.J.P.G.; Kool, R.B. Social media and rating sites as tools to understanding quality of care: A scoping review. J. Med. Internet Res. 2014, 16, e56. [Google Scholar] [CrossRef]
- McCaughey, D.; Baumgardner, C.; Gaudes, A.; LaRochelle, D.; Wu, K.J.; Raichura, T. Best practices in social media: Utilizing a value matrix to assess social media’s impact on health care. Soc. Sci. Comput. Rev. 2014, 32, 575–589. [Google Scholar] [CrossRef] [Green Version]
- Timian, A.; Rupcic, S.; Kachnowski, S.; Luisi, P. Do patients “like” good care? measuring hospital quality via Facebook. Am. J. Med. Qual. 2013, 28, 374–382. [Google Scholar] [CrossRef]
- Rozenblum, R.; Bates, D.W. Patient-centred healthcare, social media and the internet: The perfect storm? BMJ Qual. Saf. 2013, 22, 183–186. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, N.; Forsyth, D.; Tappin, D.; Catley, B. Conceptualizing workplace cyberbullying: Toward a definition for research and practice in nursing. J. Nurs. Manag. 2018, 26, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the Framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 2–3. [Google Scholar] [CrossRef] [Green Version]
- Joint Commission International, Physical and Verbal Violence against Health Care Workers, Sentinel Event Alert, Issue 59, 17 April 2018. Available online: https://www.jointcommission.org/-/media/documents/office-quality-and-patient-safety/sea_59_workplace_violence_4_13_18_final.pdf?db=web&hash=9E659237DBAF28F07982817322B99FFB (accessed on 2 April 2020).
- Fooody, M.; Samara, M.; Caribring, P. A review of cyberbulling and suggestions for online psychological therapy. Internet Interv. 2015, 2, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Ning, H.; Dhelim, S.; Bouras, M.A.; Khelloufi, A.; Ullah, A. Cyber-syndrome and its formation, classification, recovery and prevention. IEEE Access 2018, 6, 35501–35511. [Google Scholar] [CrossRef]
- Norton, P.; Costa, V.; Teixeira, J.; Azevedo, A.; Roma-Torres, A.; Amaro, J.; Cunha, L. Prevalence and determinants of bullying among healthcare workers in Portugal. Workplace Health Saf. 2017, 65, 188–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkins, J.B.; Brownstein, J.S.; Tuli, G.; Runels, T.; Broecker, K.; Nsoesie, E.O.; McIver, D.J.; Rozenblum, R.; Wright, A.; Bourgeois, F.T.; et al. Measuring patient-perceived quality of care in US hospitals using Twitter. BMJ Qual. Saf. 2016, 25, 404–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clari, M.; Conti, A.; Scacchi, A.; Scattaglia, M.; Dimonte, V.; Gianino, M.M. Prevalence of Workplace Sexual Violence against Healthcare Workers Providing Home Care: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8807. [Google Scholar] [CrossRef]
- Li, Y.L.; Li, R.Q.; Qiu, D.; Xiao, S.Y. Prevalence of Workplace Physical Violence against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binmadi, N.O.; Alblowi, J.A. Prevalence and policy of occupational violence against oral healthcare workers: Systematic review and meta-analysis. BMC Oral Health 2019, 19, 279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devi, S. COVID-19 exacerbates violence against health workers. Lancet 2020, 396, 658. [Google Scholar] [CrossRef]
- McKay, D.; Heisler, M.; Mishori, R.; Catton, H.; Kloiber, O. Attacks against health-care personnel must stop, especially as the world fights COVID-19. Lancet 2020, 395, 1743–1745. [Google Scholar] [CrossRef]
- Scopetti, M.; Santurro, A.; Tartaglia, R.; Frati, P.; Fineschi, V. Expanding frontiers of risk management: Care safety in nursing home during COVID-19 pandemic. Int. J. Qual. Health Care 2021, 33, mzaa085. [Google Scholar] [CrossRef]
- Dong, R.; Li, L.; Zhang, Q.; Cai, G. Information diffusion on social media during natural disaster. IEEE Trans. Comput. Soc. Syst. 2018, 5, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.C.; Hindle, A.; Stroulia, E. Latent Dirichlet allocation: Extracting topics from software engineering data. In The Art and Science of Analyzing Software Data 2014; Morgan Kaufmann Publishers: Burlington, MA, USA, 2015; pp. 139–159. [Google Scholar]
- Liu, B. Sentiment analysis and opinion mining. Synth. Lect. Hum. Lang. Technol. 2012, 5, 1–184. [Google Scholar] [CrossRef] [Green Version]
- Canini, K.R.; Shi, L.; Griffiths, T.L. Online inference of topics with latent Dirichlet allocation. Proceedings of the 12th International Conference on Artificial Intelligence and Statistics (AISTATS) 2009, Clearwater Beach, Florida, USA. J. Mach. Learn. Res. 2009, 5, 65–72. [Google Scholar]
- Caraka, R.E.; Hafianti, S.; Hidayati, S.; Wilie, B.; Muztahid, M.R. Identifying indicators of household indebtedness by provinces. Ninth Res. Dive Dev. Househ Vulnerability 2019, 9, 10–15. [Google Scholar]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Regina, M.; Mancini, A.; Falli, F.; Fineschi, V.; Ramacciati, N.; Frati, P.; Tartaglia, R. Aggressions on Social Networks: What Are the Implications for Healthcare Providers? An Exploratory Research. Healthcare 2021, 9, 811. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070811
La Regina M, Mancini A, Falli F, Fineschi V, Ramacciati N, Frati P, Tartaglia R. Aggressions on Social Networks: What Are the Implications for Healthcare Providers? An Exploratory Research. Healthcare. 2021; 9(7):811. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070811
Chicago/Turabian StyleLa Regina, Micaela, Arianna Mancini, Francesco Falli, Vittorio Fineschi, Nicola Ramacciati, Paola Frati, and Riccardo Tartaglia. 2021. "Aggressions on Social Networks: What Are the Implications for Healthcare Providers? An Exploratory Research" Healthcare 9, no. 7: 811. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070811