
Percutaneous versus Transcutaneous Electrical Stimulation of the Posterior Tibial Nerve in Idiopathic Overactive Bladder Syndrome with Urinary Incontinence in Adults: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.2. Data Sources
2.3. Data Collection and Analysis
3. Results
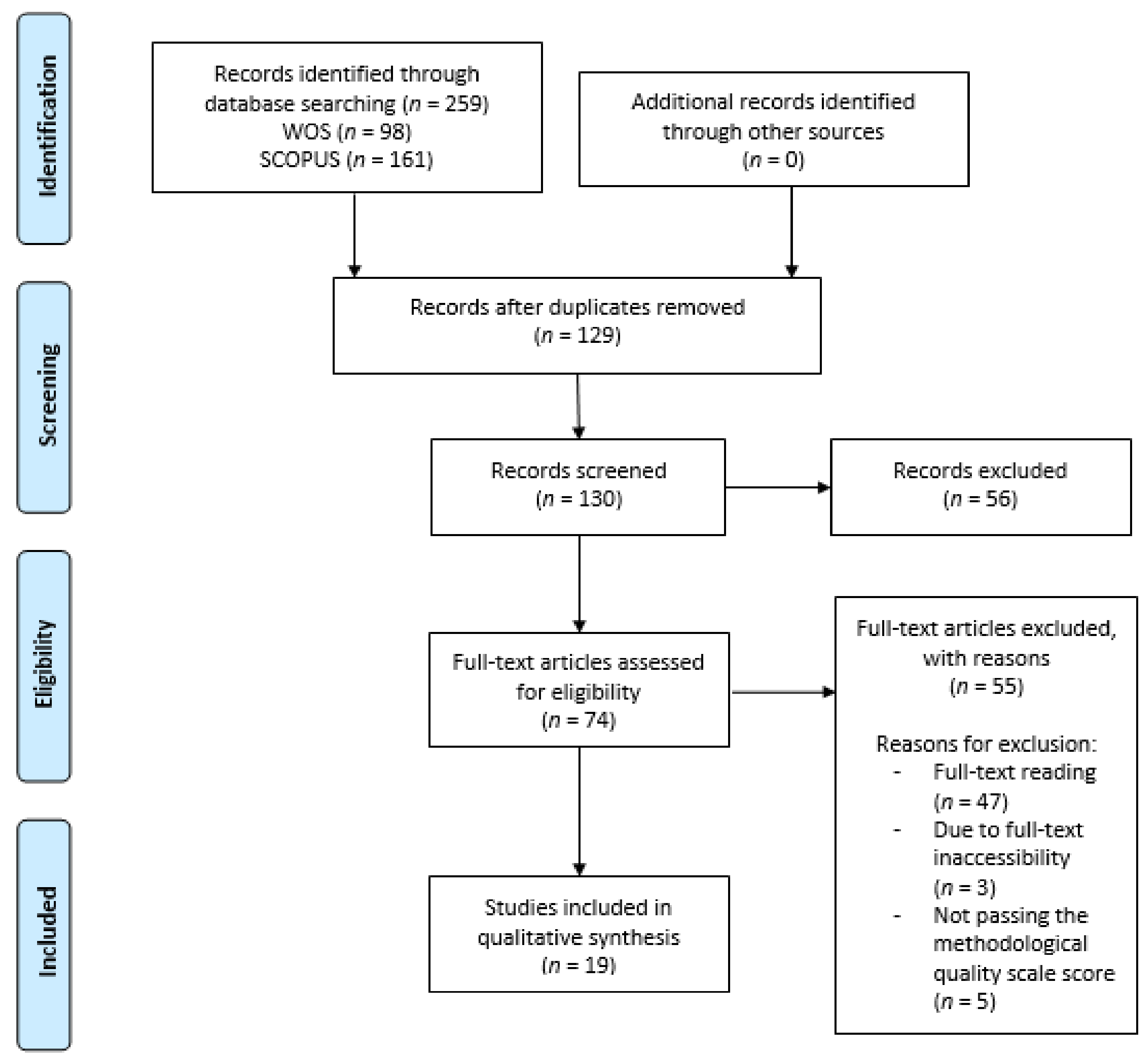
3.1. Literature Search
3.2. Summary of the Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- ICD-11-Mortality and Morbility Statistics. Available online: https://icd.who.int/browse11/l-m/en (accessed on 12 July 2021).
- Kobashi, K.; Nitti, V.; Margolis, E.; Sand, P.; Siegel, S.; Khandwala, S.; Newman, D.; MacDiarmid, S.A.; Kan, F.; Michaud, E. A Prospective Study to Evaluate Efficacy Using the Nuro Percutaneous Tibial Neuromodulation System in Drug-Naïve Patients with Overactive Bladder Syndrome. Urology 2019, 131, 77–82. [Google Scholar] [CrossRef]
- Martin-Garcia, M.; Crampton, J. A single-blind, randomized controlled trial to valuate the effectiveness of transcutaneous tibial nerve stimulation (TTNS) in Overactive Bladder symptoms in women responders to percutaneous tibial nerve stimulation (PTNS). Physiotherapy 2019, 105, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Booth, J.; Connelly, L.; Dickson, S.; Duncan, F.; Lawrence, M. The effectiveness of transcutaneous tibial nerve stimulation (TTNS) for adults with overactive bladder syndrome: A systematic review. Neurol. Urodyn. 2018, 37, 528–541. [Google Scholar] [CrossRef] [Green Version]
- Leroux, P.A.; Brassart, E.; Lebdai, S.; Azzouzi, A.R.; Bigot, P.; Carrouget, J. Transcutaneous tibial nerve stimulation: 2 years follow-up outcomes in the management of anticholinergic refractory overactive bladder. World J. Urol. 2018, 36, 1455–1460. [Google Scholar] [CrossRef]
- Angulo, J.C.; Brenes, F.J.; Lizarraga, I.; Rejas, J.; Trillo, S.; Ochayta, D.; Arumi, D. Impacto del número de episodios diarios de incontinencia de urgencia en los resultados descritos por el paciente con vejiga hiperactiva. Actas Urol. Esp. 2016, 40, 173–182. [Google Scholar] [CrossRef]
- Milsom, I.; Coyne, K.S.; Nicholson, S.; Kvasz, M.; Chen, C.I.; Wein, A.J. Global prevalence and economic burden of urgency urinary incontinence: A systematic review. Eur. Urol. 2014, 65, 79–95. [Google Scholar] [CrossRef]
- Raju, R.; Linder, B.J. Evaluation and treatment of Overactive Bladder in Women. In Mayo Clinic Proceedings; Elsevier LTD: Amsterdam, The Netherlands, 2020; Volume 95, pp. 370–377. [Google Scholar]
- Valles-Antuña, C.; Pérez-Haro, M.L.; González-Ruiz de, L.C.; Quintás-Blanco, A.; Tamargo-Díaz, E.M.; García-Rodríguez, J.; San Martín-Blanco, A.; Fernandez-Gomez, J.M. Estimulación transcutánea del nervio tibial posterior en el tratamiento de la incontinecia urinaria de urgencia refractaria, de origen idiopático y neurogénico. Actas Urol. Esp. 2017, 41, 465–470. [Google Scholar] [CrossRef]
- Sousa-Fraguas, M.C.; Lastra-Barreira, D.; Blanco-Díaz, M. Neuromodulación periférica en el síndrome de vejiga hiperactiva en mujeres: Una revisión). Actas Urol. Esp. 2020, 45, 177–187. [Google Scholar] [CrossRef]
- Peters, K.M.; Carrico, D.J.; Wooldridge, L.S.; Miller, C.J.; MacDiarmid, S.A. Percutaneous tibial nerve stimulation for the long-term treatment of overactive bladder: 3-year results of the STEP study. J. Urol. 2013, 189, 2194–2201. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Grupo PRISMA. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Rev. Esp. Nutr. Hum. Diet. 2014, 18, 172–181. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cherghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Mosely, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Argimon Pallás, J.M.; Jimenez Villa, J. Metodos de Investigación Clinica y Epidemiológica, 3rd ed.; Elsevier: Barcelona, Spain, 2004. [Google Scholar]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; GØtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Strobe Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, 1628–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirez-García, I.; Blanco-Ratto, L.; Kauffmann, S.; Carralero-Martínez, A.; Sánchez, E. Efficacy of transcutaneous stimulation of the posterior tibial nerve compared to percutaneous stimulation in idiopathic overactive bladder syndrome: Randomized control trial. Neurourol. Urodyn. 2019, 38, 261–268. [Google Scholar] [CrossRef]
- Scaldazza, C.V.; Morosetti, C.; Giampieretti, R.; Lorenzetti, R.; Baroni, M. Percutaneous tibial nerve stimulation versus electrical stimulation with pelvic floor muscle training for overactive bladder syndrome in women: Results of a randomized controlled study. Int. Braz. J. Urol. 2017, 43, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preyer, O.; Umek, W.; Laml, T.; Bjelic-Radisic, V.; Gabriel, B.; Mittlboeck, M.; Hanzal, E. Percutaneous tibial nerve stimulation versus tolterodina for overactive bladder in women: A randomized controlled trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 191, 51–56. [Google Scholar] [CrossRef]
- Abulseoud, A.; Moussa, A.; Abdelfattah, G.; Ibrain, I.; Saba, E.; Hassouna, M. Transcutaneous posterior tibial nerve electrostimulation with low dose trospium chloride: Could it be used as a second line treatment of overactive bladder in females. Neurourol. Urodyn. 2018, 37, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Seth, J.H.; Gonzales, G.; Haslam, C.; Pakzad, M.; Vashisht, A.; Sahai, A.; Knowles, C.; Tucker, A.; Panicker, J. Feasibility of using a novel non-invasive ambulatory tibial nerve stimulation device for the home-based treatment of overactive bladder symptoms. Transl. Androl. Urol. 2018, 7, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Welk, B.; Mckibbon, M. A randomized, controlled trial of transcutaneous tibial nerve stimulation to treat overactive bladder and neurogenic bladder patients. Can. Urol. Assoc. J. 2020, 14, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Tudor, K.I.; Seth, J.H.; Liechti, M.D.; Ochulor, J.; Gonzales, G.; Haslm, C.; Fox, Z.; Pakzad, M.; Panicker, J.N. Outcomes following percutaneous tibial nerve stimulation (PTNS) treatment for neurogenic and idiopathic overactive bladder. Clin. Auton. Res. 2020, 30, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Mallmann, S.; Ferla, L.; Rodrigues, M.P.; Paiva, L.L.; Sanches, P.R.S.; Ferreira, C.F.; Ramos, J.G.L. Comparison of parasacral transcutaneous electrical stimulation and transcutaneous posterior tibial nerve stimulation in women with overactive bladder syndrome: A randomized clinical trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 250, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Salatzki, J.; Liechti, M.D.; Spanudakis, E.; Gonzalez, G.; Baldwin, J.; Haslam, C.; Pakzad, M.; Panicker, J.N. Factors influencing return for maintenance treatment with percutaneous tibial nerve stimulation for the management of the overactive bladder. BJU Int. 2019, 123, 20–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moratalla Charcos, L.M.; Planelles Gómez, J.; García Mora, B.; Santamaria Navarro, C.; Vidal Moreno, J.F. Efficacy and satisfaction with transcutaneous electrostimulation of the posterior tibial nerve in overactive bladder syndrome. J. Clin. Urol. 2018, 11, 331–338. [Google Scholar] [CrossRef]
- Palmer, C.; Farhan, B.; Nguyen, N.; Ghoniem, G. Clinical outcomes of percutaneous tibial nerve stimulation in elderly patients with overactive bladder. Arab. J. Urol. 2019, 17, 10–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wibisono, E.; Rahardjo, H.E. Effectiveness of Short Term Percutaneous Tibial Nerve Stimulation for Non-neurogenic Overactive Bladder Syndrome in adults: A Meta-analysis. Acta Med. Indones. 2015, 47, 188–200. [Google Scholar]
- Tutolo, M.; Ammirati, E.; van der Aa, F. What is New in Neuromodulation for Overactive Bladder? In European Urology Focus; Elsevier B.V.: Amsterdam, The Netherlands, 2018; Volume 4, pp. 49–53. [Google Scholar]
- Lo, C.W.; Wu, M.Y.; Yang, S.S.D.; Jaw, F.S.; Chang, S.J. Comparing the efficacy of onabotulinumtoxinA, sacral neuromodulation, and peripheral tibial nerve stimulation as third line treatment for the management of overactive bladder symptoms in adults: Systematic review and network meta-analysis. Toxins 2020, 12, 128. [Google Scholar] [CrossRef] [Green Version]
- Veeratterapillay, R.; Lavin, V.; Thorpe, A.; Harding, C. Posterior tibial nerve stimulation in adults with overactive bladder syndrome: A systematic review of the literature. J. Clin. Urol. 2016, 9, 120–127. [Google Scholar] [CrossRef]
- Wang, M.; Jian, Z.; Ma, Y.; Jin, X.; Li, H.; Wang, K. Percutaneous tibial nerve stimulation for overacttive bladder syndrome: A systematic review and meta-analysis. Int. Urogynecol. J. 2020, 31, 2457–2471. [Google Scholar]


{kind=link}
| Databases | Search Strategy |
|---|---|
| WOS (February–March 2021) (years 2015/2020) | I. (“Transcutaneous Electric Nerve Stimulation” OR “Therapy, Percutaneous Neuromodulation” OR “Electrical Neuromodulation, Percutaneous”) AND adult AND (“Urinary Incontinence” OR “Urinary Bladder, Overactive”) AND (“tibial nerve” OR “Posterior tibial nerve”). II. (“Transcutaneous electrical nerve stimulation” OR “Transcutaneous tibial nerve stimulation” OR “transcutaneous stimulation tibial nerve”) AND adult AND (“overactive bladder” OR “detrusor activity” OR “urinary incontinence”). III. (“percutaneous tibial nerve stimulation” OR “PTNS”) AND adult AND (“overactive bladder” OR “detrusor activity” OR “urinary incontinence”). |
| Scopus (February–March 2021) (years 2015/2020) | I. (“Transcutaneous Electric Nerve Stimulation” OR “Therapy, Percutaneous Neuromodulation” OR “Electrical Neuromodulation, Percutaneous”) AND adult AND (“Urinary Incontinence” OR “Urinary Bladder, Overactive”) AND (“tibial nerve” OR “Posterior tibial nerve”). II. (“Transcutaneous electrical nerve stimulation” OR “Transcutaneous tibial nerve stimulation” OR “transcutaneous stimulation tibial nerve”) AND adult AND (“overactive bladder” OR “detrusor activity” OR “urinary incontinence”). III. (“percutaneous tibial nerve stimulation” OR “PTNS”) AND adult AND (“overactive bladder” OR “detrusor activity” OR “urinary incontinence”). |
| Author/s | Study Design | Study Population | Sample Size | Intervention | Follow-Up | Randomization |
| Ramírez-García I., et al., 2019 [17] | RCT | OAB and OD | n = 68 (46 W and 22 M) (34 per G) Mean age (MA): 59.6 ± 27.4 kg. Symptom duration: 1–56 years with mean of 5.1. | Grupo A(GA) (intervention)→ TTNS Grupo B (GB) (control)→ PTNS | 12 weeks | Online 1:1 Randomization Sequence“Sealed Envelope Lt. 2015” |
| Scaldazza C.V., et al., 2017 [18] | RCT | W with OAB | n = 60 W (30 per G) MA: 58.5 years (38–72) | GA→ EMS vaginal + exercises GB→ PTNS | 1 m post-treatment. | Online randomization GraphPad QuickCalcs software |
| Preyer O., et al., 2015 [19] | RCT Pilot study | W with OAB, with no previous PTNS or anticholinergic treatment | n = 36 W (18 per G) GA: MA = 57.4 ± 9.5 GB: MA = 55.8 ± 16.2 | GA→PTNS GB→ Tolterodine | 3 m (baseline/1–3 m) | 1:1 adapted randomization method (computer assistant) |
| Abulseoud A., et al., 2018 [20] | RCT | W with OAB and OD, and behavioral treatment failure | n = 30 W (15 per G) G 1: MA = 48 ± 16.42 G 2: MA = 48.13 ± 10.80 | G 1: TTNS + placebo bottle identical to G 2. G 2: TTNS + Trospium Chloride | 8 Weeks | 1:1 by random number table |
| Martín-García M. & Cramptom J. 2019 [3] | RCT | W with non-neurogenic OAB who responded to PTNS initial treatment of 12 weeks | n = 24 W (12 per G) G PTNS: MA = 58 ± 10 G TTNS: MA = 54 ± 12 | Maintenance G PTNS G TTNS | 6 m Evaluation: baseline (post-treatment with 12 weeks PTNS), at 6 weeks, 3 m and 6 m | 1:1 via sealed, opaque envelopes with numbered sequences |
| Seth J.H., et al., 2018 [21] | Randomized pilot trial | M/W with OAB after treatment with ineffective conservative therapy | n = 48 (24 multiple sclerosis and 24 Idiopathic OAB) G 1 (daily treatment): MA = 46.4(32–73), 18 W/6 M, 20 UI G 2 (weekly treatment): MA = 46.9(20–81), 20 W/4 M, 18 UI | TTNS G 1: 1 session/day G 2: 1 session/week | 12 weeks, with evaluation at 4, 8 and 12 weeks | Stratified method by sealed envelopes |
| Welk B., et al., 2020 [22] | RCT | W with OAB, neurological diseases with urinary urgency with or without UI | n = 50. MA (73%, 22/30); 10% (3/30) used spontaneous voiding catheter G TTNS→ n = 26; MA = 62 (54–68) GS → n = 24; MA = 53 (46–64) | G TTNS→ TTNS. Increasing amplitude to maximum tolerance or flexion of the big toe GS→ TTNS. Constant amplitude | 12 weeks | 1:1 by random number generator |
| Tudor K.I., et al.020 [23] | Experimental study of two groups related retrospective | Neurological or idiopathic OAB refractory to 1st line treatments | n = 74 (52 W/22 M), MA = 56.0 (25.2, 59.8). 49 (66.2%)→ neurogenic OAB 25 (33.8%) → idiopathic OAB | PTNS + drug | 12 weeks | Without randomization |
| Mallman S., et al., 2020 [24] | RCT | W with OAB | n = 50 (25 per G) MA = 61.48 ± 10.10 | G transcutaneous sacral EMS G TTNS | 6 weeks | Sequence generated in 2 G by WinPEPI version 11.63 |
| Author/s | Variables | Results | Conclusions | Adverse Effects and Limitations | Met Quality | |
| Ramírez-García I., et al., 2019 [17] | Difference day and night urination Mean voiding volume Number of urgencies and UI Quality of life | At the beginning/12 weeks. GA: n = 34/GB: n = 34 Differences by protocol: GA: n = 32 /GB: n = 29. Post intervention differences: GA: n = 34/GB: n = 34. Difference adjustment with 95% confidence interval Quality of life I-QoL: GA (21.5 p), GB (22.1 p) (P < 0.001) | Both techniques improve symptoms and quality of life Treatment adherence (P = 0.236). | No serious adverse effects Study carried out to measure differences between groups. High cost. | 7/10 | |
| Scaldazza C.V., et al., 2017 [18] | Number of voiding in 24 h Number of UUI episodes Nocturia Quality of life (OAB-q SF) Bladder urgency perception (PPIU-S) Perception of global improvement (PGI-I) | Number of daily voiding → GA→ P = 0.0620; GB→ P = 0.0307; Difference between groups (DG)→ P = 0.3758 Number of UUI episodes →GA: P = 0.1293; GB→ P = 0.0009; DG: P = 0.0251 Nocturia→ GA: P = 0.1683; GB→ P = 0.0201; DG: P = 0.049 Voiding volume→ GA: P = 0.0048; GB→ P = 0.0003; DG: P = 0.0222 OAB-q SF: 6 items: GA: P = 0.0420; GB: P < 0.0001; DG: P = 0.0172. 13 items: GA: P = 0.0420; GB: P < 0.0001; DG: P = 0.0295 PPIU-S: GA: P = 0.1014; GB: P = 0.0001; DG P = 0.0459 PGI-I→ GA: P = 0.0415; GB: P = 0.0415 | PTNS 1st line treatment (efficacy, minimally invasive) | Without significant side effects | 6/10 | |
| Preyer O., et al., 2015 [19] | Differences in number of voids in 24 h between both groups (voiding diaries). Number of UI episodes Quality of life (QoL-VAS) | n = 16 per group Number of voids→ without significant decrease 1–3 m in both G (P = 0.13), DGNS (P = 0.96). No significant differences in number at the beginning and post treatment (P = 0.79) Quality of life (QoL-VAS)→ depends on the initial values, in GB mean values are lower than GA in 1–3 m Increase in both G 1 and 3 m, without significant changes (P = 0.07) Number of UI episodes in 24 hours→ depends on the number episodes at the beginning of treatment (P = 0.0001). NSDG pre/post treatment (P = 0.89). Significant changes in 3 m (baseline/1 m) (P = 0.03) | Both are effective treatments: decrease in number of UI episodes, but not in urinary frequency. PTNS has fewer side effects. | The first 4 weeks mainly GB→ dry mouth and dizziness. 9 participants (3 m) GA→ pain in puncture area. 3 participants (3 m). Small sample size and standard deviations greater than expected, which could be due to a type II error; no blinding | 6/10 | |
| Abulseoud A., et al., 2018 [20] | Brief OAB Symptom Score (OABSS) Short form of incontinence impact questionnaire (IIQ-7) | OABSS → post-treatment G (P < 0.001) and G 2 (P = 0.024) IIQ-7 → (G1: P = 0.002; G 2: P = 0.001). Pre- treatment min 50 points (good quality of life), post-treatment 20 (6 G 1 and 14 G 2). Pre- treatment→ severe OAB symptoms in 26 patients (12 G 1 and 14 G 2), post-treatment 4 (G 1). Cystometric volume → post-treatment (G1: P = 0.026; G 2: P = 0.001), G 2 (P = 0.034) | TTNS is tolerable and effective when combined with Trospium Chloride. Better results without side effects. | Without side effects Limitation: need for another group with sodium chloride treatment without TTNS. Longer follow-up studies needed. | 8/10 | |
| Martín-García M. & Cramptom J. 2019 [3] | Urinary frequency Number of urgency episodes Number of UUI episodes Severity of symptoms Quality of life (HRQoL) | Urinary frequency G TTNS→ decreasing from the beginning/6 m: 8.5 (1.9) vs 7.7 (2.8), (P = 0.373).; G PTNS→ during the study (P = 0.242), increasing from 7.3 (4.7) to 8.7 (2.4) at 6 m P = 0.208. Number of UUI episodes in 24 h: G TTNS→ (P = 0.900); G PTNS→ (P = 0.655) Number of urgency episodes in 24 h: G TTNS→ Friedman test (P = 0.038). Wilconxon test: significant increase baseline/ 6 Weeks: 1.7 (2.8) vs 3.2 (3.6), (P = 0.044); and baseline/3 m: 1.7 (2.8) vs 2.5 (2.6 (P = 0.011). Without significant changes baseline/6 m: 1.7 (2.8) vs 2.0 (1.4) (P = 0.325); G PTNS→ (P = 0.883) Severity of symptoms → G TTNS→ (P = 0.584); G PTNS→ (P = 0.854) Quality of life HRQoL→ G TTNS→ (P = 0.676); G PTNS→ (P = 0.948) | Application of bilateral TTNS is an effective and tolerable treatment for the maintenance of benefits in OAB symptoms with previous PTNS therapy For maintenance: PTNS, regular visit for consultation; Home TTNS | TTNS without side effects. PTNS → 3 minor episodes of needle insertion bleeding (2 participants); 1 episode of discomfort/ pain over the needle area | 7/10 | |
| Seth J.H., et al., 2018 [21] | Quality of life (ICIQ-OAB) and (ICIQ-LUTqol) Part A for severity of symptoms and Part B for patient discomfort. 3-day voiding diary → urinary frequency in 24 h; number of UI episodes. | Quality of life → improvements in ICIQ-OAB score and ICIQ-LUTSqol score between the beginning and during 12 week treatments in both G. Daily treatment → part A - ICIQ-OAB → means improved between the beginning and 12 weeks from 9.3 (2.5) to 7.5 (3.1) Part B — ICIQ-OAB → from 29.6 (8.1) to 25.6 (9.5) Part A — ICIQ-LUTSqol→ from 51 (12.8) to 44.2 (13.1) Part B — ICIQ-LUTSqol → from 130.3 (43.7) to 105.5 (57.8) Weekly treatment→ part A - ICIQ-OAB→ week 12 from 9.1 (1.9) to 5.9 (1.7) Part B — ICIQ-OAB → from 29.7 (5.9) to 19.1 (8.5) Part A — ICIQ-LUTSqol → from 44.9 (9.0) to 35.9 (8.8) Part B — ICIQ-LUTSqol→ from 102.1 (40.1) to 63.9 (42.8) Urinary frequency in 24 h → Daily treatment → from 10.8 to 8.2 at 12 weeks Weekly treatment→ from 12.2 to 9.5 at 12 weeks Number of UI episodes → Daily treatment → from 2.8 to 1.6 at 12 weeks. Weekly treatment → from 2.3 to 0.9 at 12 weeks | Safe treatment. Low frequency stimulation (1 Hz) improves quality of life and symptoms of voiding diaries (daily/weekly) Neurological patients respond more frequently to treatment (65%) versus patients with idiopathic OAB (36%). No significant differences in tolerability between G | No significant complications during treatment or in satisfaction surveys 5 patients said therapy was uncomfortable and did not continue the treatment No significant safety problems. One patient developed skin redness in the area of stimulation Limitations: high dropout rate (in relation to device, lack of improvement, or local discomfort) | 5/10 | |
| Welk B., et al., 2020 [22] | Questionnaire (PPBC) Compress weight in 24 h, for UI 3-day voiding diary→ Urinary frequency and functional capacity in 24 h Quality of life (OAB-q SF, in G with OAB) Neurological patients → (NBSS), (Qualiveen-SF) | PPBC→ 13% (3/24) of sham patients and 15 (4/26) of TTNS treatment were considered responders (P = 0.77) Marginal mean of the end of the PPBC score was 3.3 (2.8–3.7) for TTNS vs 2.9 (2.5–3.4) for simulated (P = 0.30) Compress weight in 24 h→ NSDG (P = 0.64) Functional capacity → NSDG(P = 0.12) Urinary frequency in 24 h → NSDG(P = 0.32) OAB-qSF Questionnaire → NSDG in symptom discomfort (P = 0.82) and quality of life (P = 0.29) NBSS→ NSDG (P = 0.16) Qualiveen-SF→ NSDG (P = 0.85) Global assessment of improvement → NSDG (P = 0.27) | TTNS does not display greater efficacy in patient perception of OAB symptoms and objective parameters evaluated | With no adverse effects during the study Limitation in results generality, most had UI and had failed with pharmacological therapy. Small sample | 8/10 | |
| Tudor K.I., et al., 2020 [23] | ICIQ-OAB questionnaire and ICIQ-LUTSqol 3-day voiding diary → urgency and severity of UI | 64 (86%) completed 12 weeks. Significant improvements at 12 weeks of treatment in ICIQ-OAB ICIQ-LUTSqol, change in urinary frequency over 24 h and severity of UI in bladder diary G neurogenic VH→ ICIQ-OAB (P = 0.04); ICIQ-LUTSqol (P = 0.05) [in ICIQ-OAB, odds ratio (IC 95%) 0,93 (0,87, 0,99), P = 0,03], severity of UI [in bladder diary, odds ratio (IC 95%) 0.05 (0.01, 0.63), P = 0.02] and QoL [IUTQ-LUTSqol, odds ratio (IC 95%) 0.98 (0.96, 0.99), P = 0.007] at 12 weeks | PTNS is a possible alternative treatment in patients with neurological disease and with ineffective or intolerable 1st line treatment | No adverse effects. 5 patients had mild discomfort at the needle insertion area Lack of blinding, lack of a placebo or control group, and lack of urodynamic assessment before treatment Not validated questionnaires in patients with neurogenic OAB | 5/10 | |
| Mallman S., et al., 2020 [24] | Quality of life: KHQ Severity of UI: ISI Discomfort due to OAB symptoms: OAB-V8 | NSDG (P > 0.005) OAB-V8: (6 weeks P = 0.0019) G TPNS/G transcutaneous sacral EMS KHQ e ISI: NSDG | Both therapies are effective and safe for the treatment of women with OAB, UUI, and MUI | No side effects | 6/10 | |
| Author/s | Study Design | Study Population | Sample Size | Intervention | Follow-Up | |
| Salatzki J., et al., 2019 [25] | Cross-sectional (cohort) | Positive response to PTNS treatments (10–12 weeks) | n = 83 PTNS-SEQ G 1: n = 28 G 2: n = 24 G 3: n = 31 | G 1→ non-responders; no maintenance therapy G 2→ responders; possibility of maintenance therapy: they did not do it G 3→ responders who underwent maintenance therapy | 18 weeks | |
| Leroux P.A., et al., 2018 [5] | Prospective | Idiopathic or refractory OAB to anticholinergic treatment | n = 97 treated with TTNS 20 (21%) M; 77 (79%) W MA = 58.4 ± 16.6 | TTNS | 24 m | |
| Moratalla-Charcos L.M., et al., 2018 [26] | Pilot study Prospective | OAB with or without OD/UI, without success in pharmacological treatment or dropout due to adverse effects | n = 45: 38 W and 7 M. MA = 66.6 ± 10.5 (41–83). OD: 53.3%. | TTNS | 12 weeks | |
| Palmer C., et al 2019 [27] | Retrospective | >65 with idiopathic OAB, after treatment with PTNS | n = 52: 23 M (44.3%); 29 W (55.8%). MA = 75.75 (65 to 93); BMI = 26.33 (17.4 to 43.9) kg/m2 | PTNS | 12 weeks | |
| Author/s | Variables | Results | Conclusions | Adverse Effects and Limitations | Met Quality | |
| Salatzki J., et al., 2019 [25] | ICIQ-OAB→ UI in OAB ICIQ-LUT→ OAB symptoms. 3-day voiding diary PTNS-SEQ questionnaire→ variables observation to return to maintenance | Groups 2 and 3→ improvements compared to G 1. Patients with idiopathic or non-neurogenic OAB → significant improvement vs neurogenic OAB (P = 0.048). Group 3→ return to treatment after 39–204 days; significant improvements in nocturia (ICIQ-LUT, P = 0.036) and voiding diary (P = 0.046) To identify variables back to maintenance, (nocturia in 3 days/daytime urinary frequency/ number of UUI episodes), ICIQ- OAB, ICIQ-LUT→successful to distinguish between G 2 and 3 (Chi-squared 11.23, P = 0.047) PTNS-SEQ(P = 0.039)→ + 75% of cases. Increase in the categories “lack of treatment effect” — greater probability of belonging to G 2. Alternatives found to treatment of PTNS in PTNS-SEQ: (PTNS n = 28; PTNS home n = 20; PTNS in medicine clinic n = 20) | 12 weeks of PTNS→ safe and effective treatment for OAB. A beneficial response with PTNS in nocturia was a factor to return to maintenance. The voiding diary offers more objective results for the evaluation of the treatment | No side effects Limitations: small sample size; difference in number of participants between G; results only applicable to public health. | 21/22 | |
| Leroux P.A., et al., 2018 [5] | Questionnaire effectiveness USP and USP-OAB Treatment discontinuity and adverse effects Comorbidities Drugs during treatment follow-up | 3 (3%) died of unknown cause/10 were lost at follow-up TTNS persistence and predictive factors → mean follow-up = 39.3 (25–65) m; mean persistence TTNS 8.3 (1–40 m). persistence = 12 m/28 patients (29%) e = 18 m/16 patients (16%) Discontinuity risk factors → At 3 m = 24 (28,9%) abandonment TTNS. Baseline score USP-OAB > 11 predictor of early treatment failure (P = 0.014) (univariate analysis) | TTNS treatment for refractory OAB. Few patients continued long-term therapy, probably due to a decrease in efficacy over time. | No adverse effects or pain Limitation: loss in follow-up during the study, and lack of placebo group, and objective urodynamic data | 17/22 | |
| Moratalla-Charcos L.M., et al., 2018 [26] | 3-day voiding diary → Urinary frequency, nocturia, number of urgency episodes, number of UUI episodes, maximum voiding volume OABQ-SF Subjective improvements Satisfaction level | n = 39/45(86.6%)→ completed 12 weeks treatment Significant differences before and after treatment (P < 0.05) in urinary frequency, nocturia, number of urgency episodes, number of UUI episodes, maximum voiding volume. OABq-SF: P > 0.05. Statistically significant differences in GOD vs OAB Treatment satisfaction→ patients with mellitus diabetes (P = 0.043), in diabetes W (P = 0.042). In ordinal regression with 4 independent variables: number of vaginal deliveries (P = 0.011); psychiatric history (P = 0.001) were significant. Group with OD→ better satisfaction by increasing the number of vaginal deliveries and lower satisfaction for W and patients with diabetes. In ordinal regression with 3 independent variables: number of vaginal deliveries (P = 0.05) was significant | OAB treatment with TTNS is an effective, safe, minimally invasive and well tolerated therapy. In this study, all variables improved significantly compared to baseline. | Adverse effect: mild pain on plantar flexion, but no cases of dermatitis Limitation: lack of completion of voiding diaries, the OABQ-SF questionnaire, and subjective improvements, in addition to lack of a control group | 17/22 | |
| Palmer C., et al 2019 [27] | OAB-V8 → OAB symptoms 3-day voiding diary Global impression of patient satisfaction (GIPS) | n = 21 (39%) used combination therapy during PTNS After PTNS→ 37 patients (70%) reported symptom improvements; 7 used anticholinergic, 6 used ß3 adrenoceptor agonist, 5 received intravesical injections of onabotulinumtoxnA, and 2 underwent sacral neuromodulation Mean old age→ n = 13, 1 or 2 medical comorbidities; n = 10, 3, or 4 medical comorbidities; n = 6 + 5. n = 20 W (69%) used anticholinergic treatments before PTNS; n = 11 W (38%) used combination therapy during PTNS | Effectiveness and viability of the PTNS technique for the treatment of OAB in elderly patients is observed, being able to choose as a 2nd line treatment. Decrease in the use of anticholinergics by PTNS therapy | Retrospective descriptive study, small sample size which could influence the results. More objective measures should have been used to determine the success of the treatment, such as voiding diary parameters or urodynamic parameters | 13/22 | |
| Author/s | Study Design | Number and Design of Studies | Study Participants | Inerventions | Variables | Results | Conclusions and Limitations |
|---|---|---|---|---|---|---|---|
| Wibison E., et al., 2015 [28] | Meta-analysis | 16 studies 11 RCTs 5 non-comparative prospective studies | Participants with non-neurogenic OAB n = 787 480; PTNS 108; antimuscarinics 63 combined therapy 136 sham or placebo treatment More W than M (10/16 W) | PTNS vs sham treatment PTNS vs antimuscarinics PTNS in non-comparative studies | Percentage of responders or patients with positive response Voiding diary parameters (urinary frequency; nocturia; UI and voiding volume) | PTNS vs sham procedure Urinary frequency and UI episodes PTNS vs antimuscarinics PTNS in comparative studies | PTNS therapy is effective for the short-term treatment of OAB, with greater efficacy than with sham treatment, and comparable with antimuscarinic drugs (but with fewer adverse effects). However, multimodal therapy was found to be more effective PTNS could be a maintenance therapy due to its safety and durability Dose, duration, frequency, pulse of PTNS, duration of study follow-up and demographic characteristics of the subjects were highly variable in the studies included |
| Booth J., et al., 2018 [4] | Systematic review | 13 articles 10 RCTs 3 prospective studies | >18 years old with OAB with MUI n = 629 → 473 (70%) W and 176 (28%) M, 16 (2%) gender is unknown 36 (18%) →sham treatment 142 (56%) →anticholinergic; 26 (10%)→ pelvic floor and bladder training 9 (4%) → sacral EMS or without treatment | Durability: 4–12 weeks (mean: 7.6 ± 3.6). Total number of sessions 5–90 (mean 21.6 ± 2.3) 30 min/individual session, except 3 of 20 min. 3 studies with daily stimulation, 7 studies with 2 times/week and 2 studies with 1 time/week | Urinary urgency symptoms Urinary frequency Nocturia Number of UI episodes Quality of life Adverse effects Urodynamic changes | Changes in voiding diary Score in OAB symptoms Effectiveness of TTNS Observational studies→ 3/3 General combined result→ 9/13 | All studies observed improvements with TTNS treatment. It is safe and tolerable, due to this factor, its low cost, its ease of application and the possibility of self-administration by the patient, more studies are necessary to show its use as a 2nd line treatment |
| Tutolo M., et al., 2018 [29] | Systematic review | 9 articles, all RCTs | Patients with OAB treated by SNM or PTNS | SNM and PTNS PTNS: 4 RCTs→ 388 patients PTNS vs Tolterodine → 3 m (94% W) PTNS vs sham therapy → 3 m PTNS vs placebo → 12 weeks PTNS vs vaginal electrical stimulation→ 12 weeks | Number of UI episodes and severity Number of compress in 24 h Urinary frequency Voiding volume Urinary urgency | PTNS efficacy PTNS safety | There are no high-quality studies able to guide professionals to choose between different treatments. This study shows that sacral stimulation and PTNS are safe and effective. SNM has more long-lasting effects, while PTNS needs to have maintenance treatment Limitations: number of results due to the impossibility of evaluator and patient blinding in the studies |
| Lo C.W., et al., 2020 [30] | Systematic review and meta-analysis | 17 articles, all of them RCTs | Most patients with refractory OAB or patients who have tried 1st or 2nd line of treatment | Treatment with OnabotulinumtoxinA, SNM, and PTNS Heterogeneity between study designs, participants, follow-up, evaluated parameters, OnabotulinumtoxinA dose, and PTNS and SNM protocols | Quality of life Number of UUI episodes in 24 h Urinary frequency in 24 h improvement >50% of symptoms Nocturia Complications | Urinary frequency per day→ 9/17 Number of UI episodes per day→ 7/17 Improvement of 50% or more in symptoms at 12 weeks →8/17 | The three modalities are effective and better than placebo for OAB treatment. At 12 weeks, SNM had greater efficacy in UI and urinary frequency, while OnabotulinumtoxinA had more complications Lack of enough data to conduct a meta-analysis in quality of life, urgency, UUI episodes/day, maximum bladder capacity and nocturia 4 studies rated as high risk of bias in the category of ’outcome measurement’ because the self-report results could have been influenced by the placebo effect. Heterogeneity between studies made it difficult to clarify the results |
| Veeratterapillav R., et al., 2016 [31] | Systematic review | 20 studies 6 RCTs 14 controlled clinical trials, prospective cohort studies, and retrospective series | Patients with OAB treated by PTNS and other comparative therapies. | PTNS vs pharmacological treatment PTNS vs placebo PTNS vs sham treatment Follow-up durability varied Different inclusion criteria and definitions of therapy “success” complicated the comparison | Urinary frequency Urinary urgency Nocturia UUI episodes Quality of life Urodynamic study | PTNS urodynamic results and PTNS clinical result PTNS vs anticholinergic therapy PTNS safety and other therapies PTNS cost | PTNS success changed due to informed symptoms by the patient (improvements in frequency and urgency), clinical evaluations (OAB and QoL questionnaires, voiding diary), and observation of aerodynamic variables. Hence, treatment was successful between 54.5% and 79.5% at 12 weeks and 15% and 71% in 1–3 years The studies suggested that PTNS efficacy is better with anticholinergic as a unique treatment, but there was limited evidence of combination therapy efficacy |
| Wang M., et al., 2020 [32] | Systematic review and meta-analysis | 28 articles, 12 RCTs 16 observational studies | 246 patients with OAB symptoms treated by PTNS and other comparative therapies | 30 min PTNS for 12 weeks in 6/2 studies, the rest of studies had different protocols PTNS vs Tolterodine PTNS vs PTNS + sham treatment PTNS vs TTNS | 3-day voiding diary (urinary frequency/day, nocturia/day, number of UUI episodes/day, number of UI episodes, daytime urination frequency/day, voiding volume and urodynamic data) Response rate | Urinary frequency/day → 10/28. Nocturia/día → 13/28 Number of UUI and UI episodes /day → 8/28 and 10/28 Urination frequency /day → 7/28 Voiding volume /day → 8/28 Urodynamic data Treatment response rate → 17/28 Comparison with other therapies | PTNS therapy was shown to be effective and safe for OAB treatment Limitations: heterogeneity of the studies included, however, a subgroup analysis was performed to observe that this factor was due to the study design. Second, evaluation of the improvements and success of the variable was done unconsciously Severe side effects: the most common was pain in the puncture area |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agost-González, A.; Escobio-Prieto, I.; Pareja-Leal, A.M.; Casuso-Holgado, M.J.; Blanco-Diaz, M.; Albornoz-Cabello, M. Percutaneous versus Transcutaneous Electrical Stimulation of the Posterior Tibial Nerve in Idiopathic Overactive Bladder Syndrome with Urinary Incontinence in Adults: A Systematic Review. Healthcare 2021, 9, 879. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070879
Agost-González A, Escobio-Prieto I, Pareja-Leal AM, Casuso-Holgado MJ, Blanco-Diaz M, Albornoz-Cabello M. Percutaneous versus Transcutaneous Electrical Stimulation of the Posterior Tibial Nerve in Idiopathic Overactive Bladder Syndrome with Urinary Incontinence in Adults: A Systematic Review. Healthcare. 2021; 9(7):879. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070879
Chicago/Turabian StyleAgost-González, Aida, Isabel Escobio-Prieto, Azahara M. Pareja-Leal, María Jesús Casuso-Holgado, María Blanco-Diaz, and Manuel Albornoz-Cabello. 2021. "Percutaneous versus Transcutaneous Electrical Stimulation of the Posterior Tibial Nerve in Idiopathic Overactive Bladder Syndrome with Urinary Incontinence in Adults: A Systematic Review" Healthcare 9, no. 7: 879. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070879