
Postural Adjustments and Kinematic Index Finger Features in Frail Older Adults under Different Equilibrium Constraints

 , , and
, , and
Abstract
:1. Background
2. Methods
2.1. Study Design
2.2. Subjects
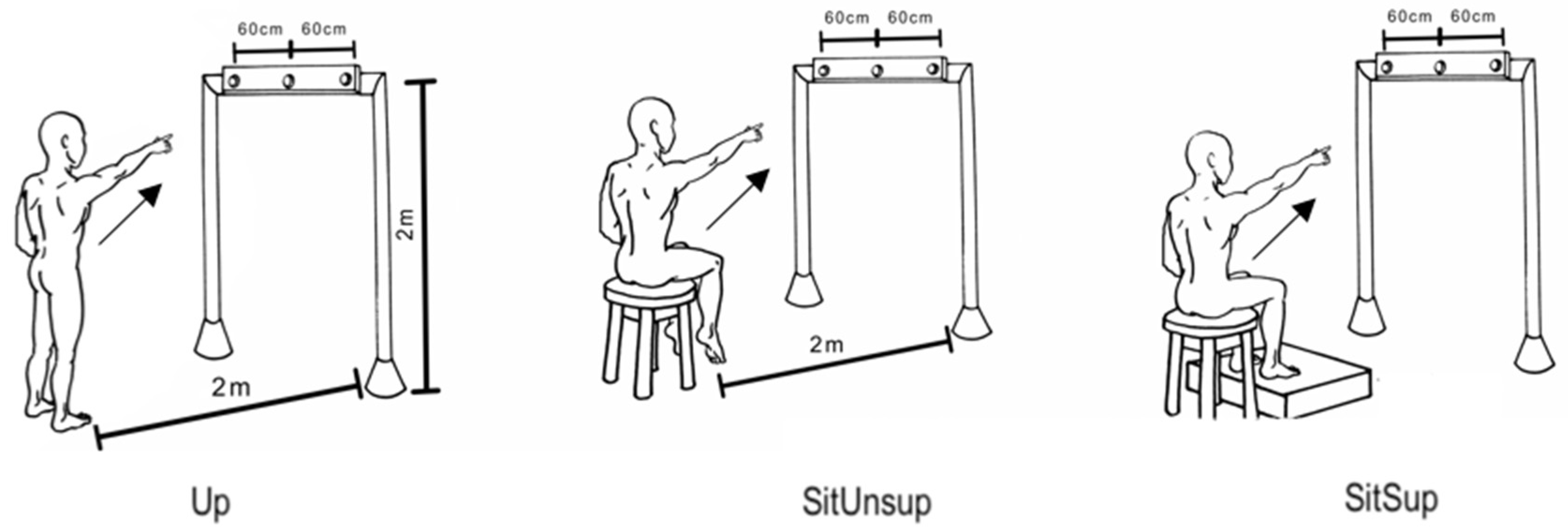
2.3. Experimental Setup and Protocol
2.4. Kinematic and Electromyographic Recording
2.5. Data Analysis
2.6. Kinematic Characteristics
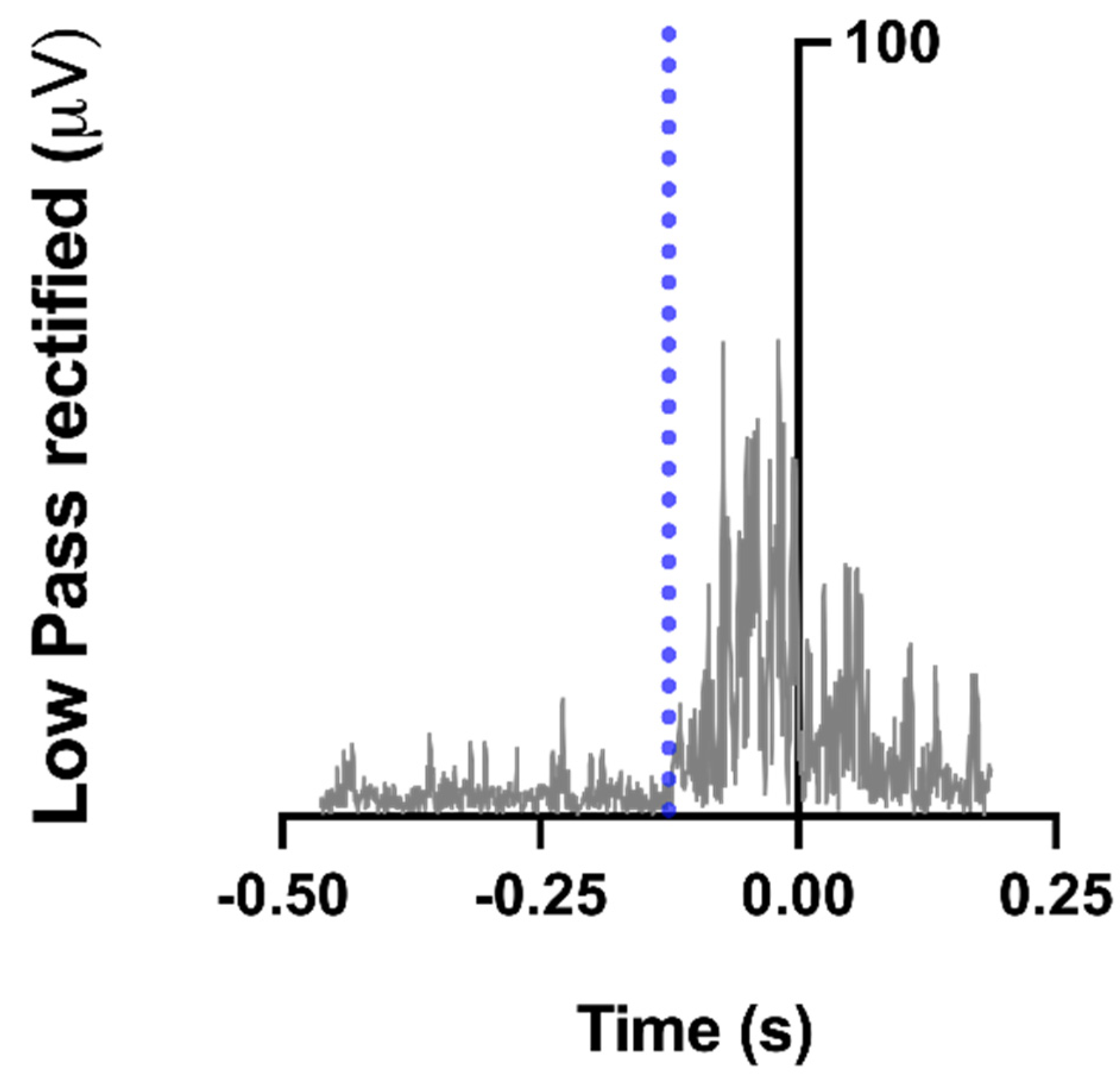
2.7. EMG Data
2.8. Statistical Analysis
3. Results
3.1. Kinematic Characteristics
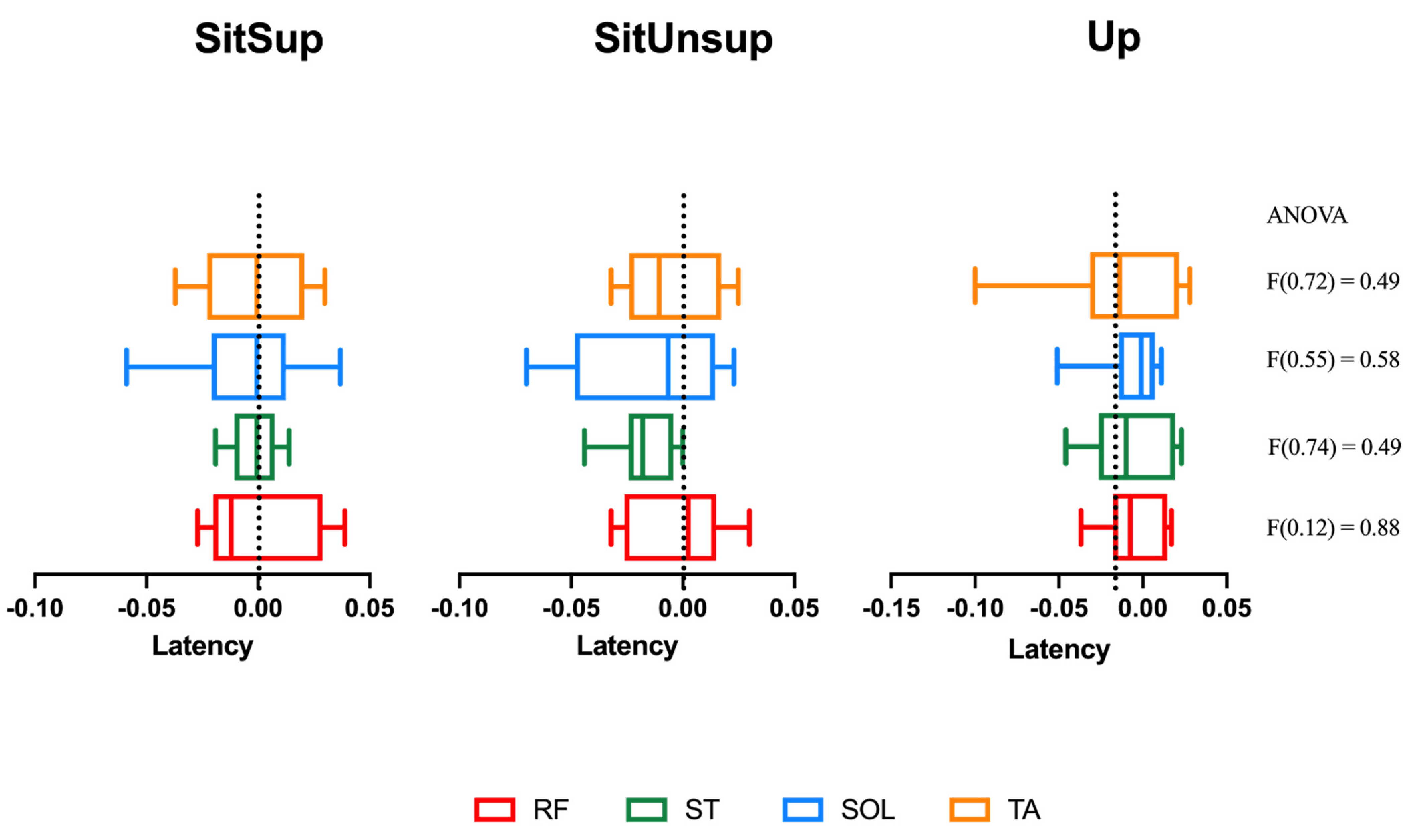
3.2. Muscle Activation Timing between Postures
3.3. Muscle Activation Magnitude in the APA Period between Postures
4. Discussion
4.1. Kinematic Features of the Upper Limb
4.2. Muscles Activation Features
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACC/MD | Acceleration time to total movement duration |
| AD | Ankle displacement |
| APAs | Anticipatory postural adjustments |
| COP | Center of pressure |
| CNS | Central nervous system |
| DEL | Deltoids anterior |
| EMG | Electromyographic |
| FOAs | Frail older adults |
| EMGi | Integrated EMG |
| MD | Movement duration |
| MV | Movement velocity |
| Fz | Reaction force |
| RT | Reaction time |
| RF | Rectus femoris |
| RMS | Root mean square |
| ST | Semitendinosus |
| Sit Sup | Sitting with support |
| SitUnsup | Sitting without support |
| SOL | Soleus |
| SD | Standard deviation |
| TA | Tibialis anterior |
| Up | Upright |
References
- Massion, J. Movement, posture and equilibrium: Interaction and coordination. Prog. Neurobiol. 1992, 38, 35–56. [Google Scholar] [CrossRef]
- Wolpert, D.M.; Flanagan, J.R. Motor prediction. Curr. Biol. 2001, 11, R729–R732. [Google Scholar] [CrossRef] [Green Version]
- Bouisset, S.; Zattara, M. Biomechanical study of the programming of anticipatory postural adjustments associated with voluntary movement. J. Biomech. 1987, 20, 735–742. [Google Scholar] [CrossRef]
- Callegari, B.; Saunier, G.; Duarte, M.B.; da Silva Almeida, G.C.; Amorim, C.F.; Mourey, F.; Pozzo, T.; da Silva Souza, G. Anticipatory postural adjustments and kinematic arm features when postural stability is manipulated. PeerJ 2018, 6, e4309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertucco, M.; Cesari, P. Does movement planning follow Fitts’ law? Scaling anticipatory postural adjustments with movement speed and accuracy. Neuroscience 2010, 171, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Woollacott, M.H. Age-Related Changes in Posture and Movement. J. Gerontol. 1993, 48, 56–60. [Google Scholar] [CrossRef]
- Bleuse, S.; Cassim, F.; Blatt, J.-L.; Labyt, E.; Derambure, P.; Guieu, J.-D.; Defebvre, L. Effect of age on anticipatory postural adjustments in unilateral arm movement. Gait Posture 2006, 24, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Kanekar, N.; Aruin, A.S.; Kanekar, N.; Aruin, A. The effect of aging on anticipatory postural control. Exp. Brain Res. 2014, 232, 1127–1136. [Google Scholar] [CrossRef] [Green Version]
- Woollacott, M.H. Age-related changes in anticipatory postural adjustments associated with arm movements. J. Gerontol. Med. Sci. 1988, 43, M205–M213. [Google Scholar]
- Inglin, B.; Woollacott, M. Age-related changes in anticipatory postural adjustments associated with arm movements. J Gerontol. 1988, 43, 105–113. [Google Scholar] [CrossRef]
- Yiou, E.; Kanekar, N.; Aruin, A.; Yiou, E.; Caderby, T.; Delafontaine, A.; Fourcade, P.; Honeine, J.-L.; Greve, J.M.D.A.; Alonso, A.C.; et al. Adaptability of anticipatory postural adjustments associated with voluntary movement. Front. Hum. Neurosci. 2017, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Kubicki, A.; Bonnetblanc, F.; Petrement, G.; Ballay, Y.; Mourey, F. Delayed postural control during self-generated perturbations in the frail older adults. Clin. Interv. Aging 2012, 7, 65–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubicki, A.; Bonnetblanc, F.; Petrement, G.; Mourey, F. Motor-prediction improvements after virtual rehabilitation in geriatrics: Frail patients reveal different learning curves for movement and postural control. Neurophysiol. Clin. Neurophysiol. 2014, 44, 109–118. [Google Scholar] [CrossRef]
- Davis, D.H.J.; Rockwood, M.R.H.; Mitnitski, A.B.; Rockwood, K. Impairments in mobility and balance in relation to frailty. Arch. Gerontol. Geriatr. 2011, 53, 79–83. [Google Scholar] [CrossRef]
- Aruin, A.; Shiratori, T. Anticipatory postural adjustments while sitting: The effects of different leg supports. Exp. Brain Res. 2003, 151, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Nakazawa, K.; Shimizu, E.; Shimoyama, I. Anticipatory postural adjustments modify the movement-related potentials of upper extremity voluntary movement. Gait Posture 2008, 27, 97–102. [Google Scholar] [CrossRef]
- Robinovitch, S.N.; Feldman, F.; Yang, Y. Erratam: Video capture of the circumstances of falls in elderly people residing in long-term care: An observational study. Lancet 2013, 381, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older AdultsEvidence for a Phenotype. J. Gerontol. Ser. A 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Santos, M.J.; Kanekar, N.; Aruin, A.S. The role of anticipatory postural adjustments in compensatory control of posture: 1. Electromyographic analysis. J. Electromyogr. Kinesiol. 2010, 20, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Woollacott, M.H.; Manchester, D.L. Anticipatory postural adjustments in older adults: Are changes in response characteristics due to changes in strategy? J. Gerontol. 1993, 48, M64–M70. [Google Scholar] [CrossRef] [PubMed]
- Berret, B.; Bonnetblanc, F.; Papaxanthis, C.; Pozzo, T. Modular control of pointing beyond arm’s length. J. Neurosci. 2009, 29, 191–205. [Google Scholar] [CrossRef] [PubMed]
- Fautrelle, L.; Prablanc, C.; Berret, B.; Ballay, Y.; Bonnetblanc, F. Pointing to double-step visual stimuli from a standing position: Very short latency (express) corrections are observed in upper and lower limbs and may not require cortical involvement. Neuroscience 2010, 169, 697–705. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| FOA (n = 10) | |
|---|---|
| Sex | 10 M |
| Age (years) | 72.7 ± 1.42 |
| Height (cm) | 167.5 ± 0.71 |
| Weight (kg) | 68.3 ± 7.30 |
| Physical Activity | 8 sedentary 2 insufficiently active |
| Berg Balance Scale | 43.00 ± 5.01 (39; 46) |
| Posture | Reaction Time (ms) | Movement Duration (ms) | Velocity (m/s) | Acceleration Time/ Movement Duration |
|---|---|---|---|---|
| SitSup | 532.87 (44.51) | 747.84 (39.85) | 3.47 (0.5) | 0.36 (0.04) |
| SitUnsup | 568.65 (44.34) | 772.00 (65.28) | 3.62 (0.4) | 0.37 (0.04) |
| Up | 571.41 (3.13) | 760.99 (25.68) | 3.08 (0.3) | 0.36 (0.03) |
| ANOVA (p-value) | (F(2.37) = 0.11) | (F(0.65) = 0.052) | (F(2.39) = 0.11) | (F(0.49) = 0.61) |
| Posture | TA (%) | SOL (%) | RF (%) | ST (%) |
|---|---|---|---|---|
| SitSup | 14.59 (10.19) | −8.14 (3.20) | 11.99 (5.71) | 8.84 (5.95) |
| SitUnsup | 18.51 (27.891) | −6.04 (3.76) | 10.45 (5.03) | 31.53 (13.99) * |
| Up | 13.01 (7.96) | −7.75 (3.73) | 7.98 (4.19) | 9.83 (4.76) |
| ANOVA (p-value) | (F(0.25) = 0.77) | (F(0.98) = 0.38) | (F(1.62) = 0.21) | (F(19.43) < 0.0000) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Callegari, B.; Kubicki, A.; Saunier, G.; Duarte, M.B.; Almeida, G.C.d.S.; Alves, B.M.O.; Amorim, C.F.; Garcez, D.R.; Souza, G.d.S.; Mourey, F. Postural Adjustments and Kinematic Index Finger Features in Frail Older Adults under Different Equilibrium Constraints. Healthcare 2021, 9, 921. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9080921
Callegari B, Kubicki A, Saunier G, Duarte MB, Almeida GCdS, Alves BMO, Amorim CF, Garcez DR, Souza GdS, Mourey F. Postural Adjustments and Kinematic Index Finger Features in Frail Older Adults under Different Equilibrium Constraints. Healthcare. 2021; 9(8):921. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9080921
Chicago/Turabian StyleCallegari, Bianca, Alexandre Kubicki, Ghislain Saunier, Manuela Brito Duarte, Gizele Cristina da Silva Almeida, Bruno Mazziotti Oliveira Alves, César Ferreira Amorim, Daniela Rosa Garcez, Givago da Silva Souza, and France Mourey. 2021. "Postural Adjustments and Kinematic Index Finger Features in Frail Older Adults under Different Equilibrium Constraints" Healthcare 9, no. 8: 921. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9080921