
Engagement in Everyday Activities for Prevention of Stroke: Feasibility of an mHealth-Supported Program for People with TIA

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Engaging Everyday Activities and Lifestyle
1.2. Transient Ischemic Attack and Risk Factors for Stroke
1.3. Primary Healthcare and Policy
2. Materials and Methods
2.1. Design
2.2. Sample
2.3. The Make My Day Prevention Program
The Digital Platform
2.4. Data Collection
2.4.1. Feasibility Measures
2.4.2. Outcome Measures
2.5. Data Analysis
2.5.1. Analysis of Feasibility Data
2.5.2. Within-Case Analysis of Outcomes and Goal Achievement
3. Results
3.1. Feasibility of the Program and App
3.1.1. Acceptability of the App
3.1.2. Usability of the App
3.1.3. Acceptability of the Prevention Program as a Whole
Experiences of Participants at Risk
Experiences of Interventionists
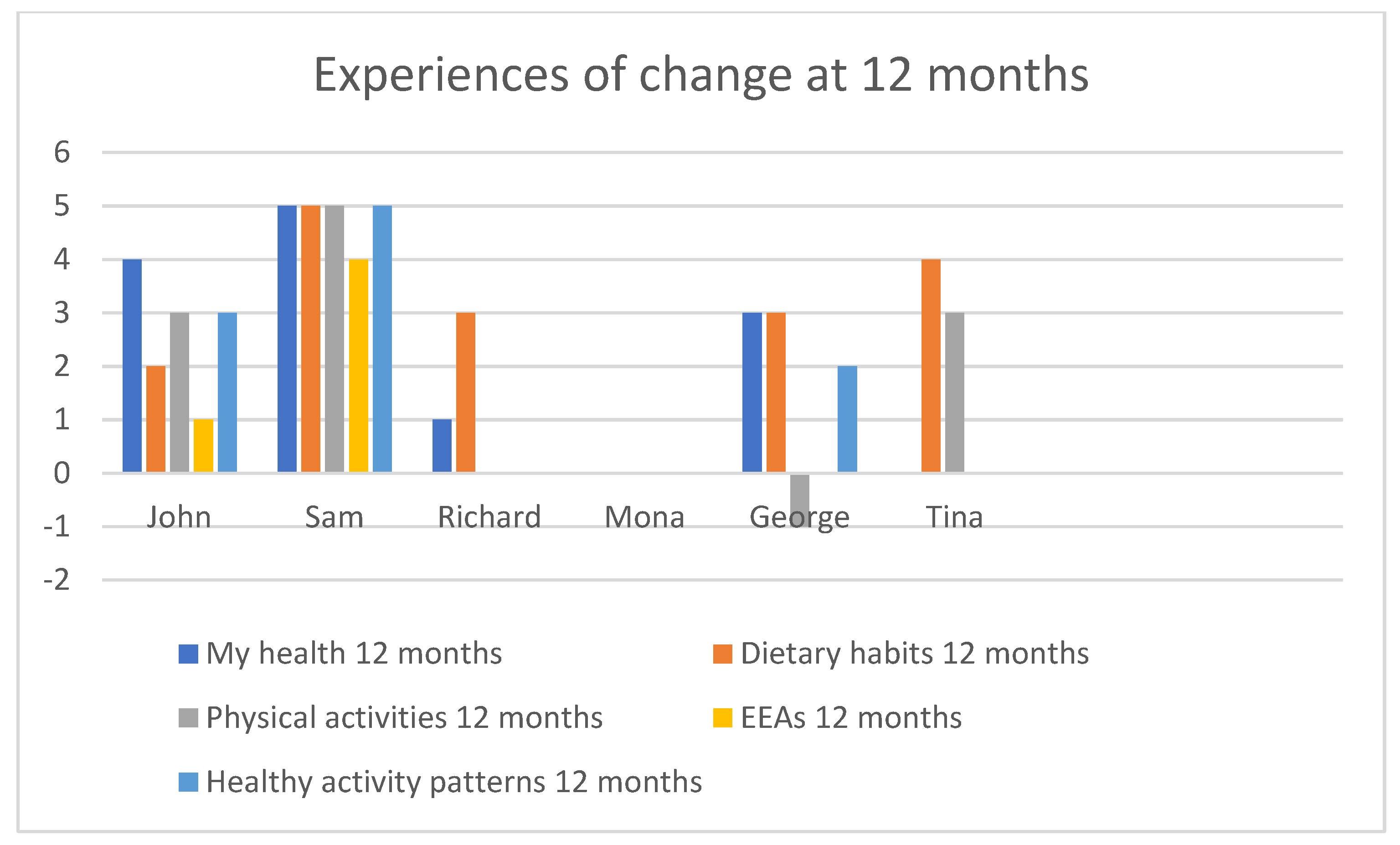
3.2. Risk for Stroke, Life Satisfaction, and Change Pre–Post-Intervention
4. Discussions
4.1. Methodological Limitations
4.2. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patomella, A.H.; Guidetti, S.; Malstam, E.; Eriksson, C.; Bergstrom, A.; Akesson, E.; Kottorp, A.; Asaba, E. Primary prevention of stroke: Randomised controlled pilot trial protocol on engaging everyday activities promoting health. BMJ Open 2019, 9, e031984. [Google Scholar] [CrossRef] [Green Version]
- Socialstyrelsen. Nationella Riktlinjer för Prevention och Behandling vid Ohälsosamma Levnadsvanor; Socialstyrelsen: Stockholm, Sweden, 2018; p. 79. [Google Scholar]
- Goldstein, L.B.; Bushnell, C.D.; Adams, R.J.; Appel, L.J.; Braun, L.T.; Chaturvedi, S.; Creager, M.A.; Culebras, A.; Eckel, R.H.; Hart, R.G.; et al. Guidelines for the primary prevention of stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011, 42, 517–584. [Google Scholar] [CrossRef] [PubMed]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef] [PubMed]
- Poulain, M.; Herm, A.; Pes, G. The Blue Zones: Areas of exceptional longevity around the world. Vienna Yearb. Popul. Res. 2013, 11, 87. [Google Scholar] [CrossRef]
- Michie, S.; Wood, C.E.; Johnston, M.; Abraham, C.; Francis, J.J.; Hardeman, W. Behaviour change techniques: The development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol Assess 2015, 19, 1–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonsson, H. A new direction in the conceptualization and categorization of occupation. J. Occup. Sci. 2008, 15, 3–8. [Google Scholar] [CrossRef]
- Asaba, E.; Bergström, A.; Patomella, A.-H.; Guidetti, S. Engaging occupations among persons at risk for stroke: A health paradox. Scand. J. Occup. Ther. 2020, 1–10. [Google Scholar] [CrossRef]
- Clark, F.; Azen, S.P.; Zemke, R.; Jackson, J.; Carlson, M.; Mandel, D.; Hay, J.; Josephson, K.; Cherry, B.; Hessel, C.; et al. Occupational therapy for independent-living older adults. A randomized controlled trial. JAMA 1997, 278, 1321–1326. [Google Scholar] [CrossRef] [PubMed]
- Clark, F.; Jackson, J.; Carlson, M.; Chou, C.P.; Cherry, B.J.; Jordan-Marsh, M.; Knight, B.G.; Mandel, D.; Blanchard, J.; Granger, D.A.; et al. Effectiveness of a lifestyle intervention in promoting the well-being of independently living older people: Results of the Well Elderly 2 Randomised Controlled Trial. J. Epidemiol. Community Health 2012, 66, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Mountain, G.; Windle, G.; Hind, D.; Walters, S.; Keertharuth, A.; Chatters, R.; Sprange, K.; Craig, C.; Cook, S.; Lee, E.; et al. A preventative lifestyle intervention for older adults (lifestyle matters): A randomised controlled trial. Age Ageing 2017, 46, 627–634. [Google Scholar] [CrossRef] [Green Version]
- Loef, M.; Walach, H. The combined effects of healthy lifestyle behaviors on all cause mortality: A systematic review and meta-analysis. Prev. Med. 2012, 55, 163–170. [Google Scholar] [CrossRef]
- Barbaresko, J.; Rienks, J.; Nothlings, U. Lifestyle Indices and Cardiovascular Disease Risk: A Meta-analysis. Am. J. Prev. Med. 2018, 55, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.; Carlson, M.; Mandel, D.; Zemke, R.; Clark, F. Occupation in lifestyle redesign: The Well Elderly Study Occupational Therapy Program. Am. J. Occup. 1998, 52, 326–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, M.; Asaba, E.; Duncan, E.; Elf, M.; Eriksson, G.; Faulkner, J.; Guidetti, S.; Johansson, B.; Kruuse, C.; Lambrick, D.; et al. Stroke secondary prevention, a non-surgical and non-pharmacological consensus definition: Results of a Delphi study. BMC Res. Notes 2019, 12, 823. [Google Scholar] [CrossRef] [Green Version]
- Easton, J.D.; Saver, J.L.; Albers, G.W.; Alberts, M.J.; Chaturvedi, S.; Feldmann, E.; Hatsukami, T.S.; Higashida, R.T.; Johnston, S.C.; Kidwell, C.S.; et al. Definition and evaluation of transient ischemic attack: A scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke 2009, 40, 2276–2293. [Google Scholar] [CrossRef] [Green Version]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef]
- Buchwald, F. TIA in the Swedish Stroke Register (Riksstroke). Aspects on Diagnostic Validation, Risk Factors, Investigations, and Therapies. Ph.D. Thesis, Faculty of Medicine, Lund University, Lund, Sweden, 2018. [Google Scholar]
- Johnston, S.C.; Gress, D.R.; Browner, W.S.; Sidney, S. Short-term prognosis after emergency department diagnosis of TIA. JAMA 2000, 284, 2901–2906. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Krishnamurthi, R.; Bhattacharjee, R.; Parmar, P.; Theadom, A.; Hussein, T.; Purohit, M.; Hume, P.; Abbott, M.; Rush, E. New strategy to reduce the global burden of stroke. Stroke 2015, 46, 1740–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lennon, O.; Blake, C.; Booth, J.; Pollock, A.; Lawrence, M. Interventions for behaviour change and self-management in stroke secondary prevention: Protocol for an overview of reviews. Syst. Rev. 2018, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, M.; Pringle, J.; Kerr, S.; Booth, J.; Govan, L.; Roberts, N.J. Multimodal secondary prevention behavioral interventions for TIA and stroke: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0120902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patomella, A.H.; Mickols, G.; Asaba, E.; Nilsson, G.; Friden, C.; Kottorp, A.; Bertilson, B.C.; Tham, K. General practitioners’ reasoning on risk screening and primary prevention of stroke—A focus group study. BMC Fam. Pr. 2018, 19, 190. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Rexrode, K.M.; Spiegelman, D.; Logroscino, G.; Manson, J.E.; Rimm, E.B. Primary prevention of stroke by healthy lifestyle. Circulation 2008, 118, 947–954. [Google Scholar] [CrossRef] [Green Version]
- Eakin, E.G.; Glasgow, R.E.; Riley, K.M. Review of primary care-based physical activity intervention studies: Effectiveness and implications for practice and future research. In Database of Abstracts of Reviews of Effects (DARE): Quality-Assessed Reviews [Internet]; Centre for Reviews and Dissemination (UK): York, UK, 2000. [Google Scholar]
- Weiss, E.C.; Galuska, D.A.; Khan, L.K.; Gillespie, C.; Serdula, M.K. Weight regain in US adults who experienced substantial weight loss, 1999–2002. Am. J. Prev. Med. 2007, 33, 34–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, C.K.; Ariyarathna, N.; Islam, S.M.; Thiagalingam, A.; Redfern, J. mHealth in Cardiovascular Health Care. Heart Lung Circ. 2016, 25, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phy. 2016, 13, 127. [Google Scholar] [CrossRef] [Green Version]
- Vellipuram, A.R.; Rodriguez, G.; Rawla, P.; Maud, A.; Cruz-Flores, S.; Khatri, R. Lifestyle Interventions to Prevent Cardiovascular Events After Stroke and Transient Ischemic Attack. Curr. Cardiol. Rep. 2019, 21, 44. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M.; Medical Research Council, G. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Cathain, A.; Hoddinott, P.; Lewin, S.; Thomas, K.; Young, B.; Adamson, J.; Jansen, Y.; Mills, N.; Moore, G.; Donovan, J. Maximising the impact of qualitative research in feasibility studies for randomised controlled trials: Guidance for researchers. Trials 2015, 16, 32. [Google Scholar] [CrossRef]
- Yin, R.K. Case Study Research and Applications: Design and Methods; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- National Stroke Association. Stroke Risk Score Card. Available online: https://www.stroke.org/stroke-risk-scorecard-2018/ (accessed on 24 April 2021).
- Prochaska, J.O.; Redding, C.A.; Evers, K.E. The transtheoretical model and stages of change. In Health Behavoiur: Theory, Research and, Practice, 5th ed.; Jossey-Bass/Wiley: San Francisco, CA, USA, 2015; pp. 125–148. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Deijle, I.A.; Van Schaik, S.M.; Van Wegen, E.E.; Weinstein, H.C.; Kwakkel, G.; Van den Berg-Vos, R.M. Lifestyle Interventions to Prevent Cardiovascular Events After Stroke and Transient Ischemic Attack: Systematic Review and Meta-Analysis. Stroke 2017, 48, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Strecher, V.J.; Seijts, G.H.; Kok, G.J.; Latham, G.P.; Glasgow, R.; DeVellis, B.; Meertens, R.M.; Bulger, D.W. Goal setting as a strategy for health behavior change. Health Educ. Q. 1995, 22, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Bryan, R.L.; Kreuter, M.W.; Brownson, R.C. Integrating adult learning principles into training for public health practice. Health Promot. Pract. 2009, 10, 557–563. [Google Scholar] [CrossRef]
- Gardner, B. A review and analysis of the use of ‘habit’ in understanding, predicting and influencing health-related behaviour. Health Psychol. Rev. 2015, 9, 277–295. [Google Scholar] [CrossRef] [Green Version]
- Hall, A.K.; Stellefson, M.; Bernhardt, J.M. Healthy Aging 2.0: The potential of new media and technology. Prev.Chronic. Dis. 2012, 9, E67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, D.R.; Chair, S.Y.; Chan, S.W.; Astin, F.; Davidson, P.M.; Ski, C.F. Motivational interviewing: A useful approach to improving cardiovascular health? J. Clin. Nurs. 2011, 20, 1236. [Google Scholar] [CrossRef]
- Law, M.; Baptiste, S.; McColl, M.; Opzoomer, A.; Polatajko, H.; Pollock, N. The Canadian occupational performance measure: An outcome measure for occupational therapy. Can. J. Occup. 1990, 57, 82–87. [Google Scholar] [CrossRef]
- Kroese, F.M.; Adriaanse, M.A.; De Ridder, D.T. Boosters, anyone? Exploring the added value of booster sessions in a self-management intervention. Health Educ. Res. 2012, 27, 825–833. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.F.; Sidani, S. Effectiveness of Diabetes Self-management Education Intervention Elements: A Meta-analysis. Can. J. Diabetes 2009, 33, 18–26. [Google Scholar] [CrossRef]
- Wu, S.; Chalder, T.; Anderson, K.E.; Gillespie, D.; Macleod, M.R.; Mead, G.E. Development of a psychological intervention for fatigue after stroke. PLoS ONE 2017, 12, e0183286. [Google Scholar] [CrossRef] [Green Version]
- Mälstam, E.; Asaba, E.; Åkesson, E.; Guidetti, S.; Patomella, A.-H. ‘Weaving lifestyle habits’: Complex pathways to health for persons at risk for stroke. Scand. J. Occup. Ther. 2021, 1–13. [Google Scholar] [CrossRef]
- Burstrom, K.; Johannesson, M.; Diderichsen, F. Swedish population health-related quality of life results using the EQ-5D. Qual. Life Res. 2001, 10, 621–635. [Google Scholar] [CrossRef]
- Kamper, S.J.; Maher, C.G.; Mackay, G. Global rating of change scales: A review of strengths and weaknesses and considerations for design. J. Man. Manip. 2009, 17, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Charmaz, K. Constructing Grounded Theory; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Bowen, D.J.; Kreuter, M.; Spring, B.; Cofta-Woerpel, L.; Linnan, L.; Weiner, D.; Bakken, S.; Kaplan, C.P.; Squiers, L.; Fabrizio, C.; et al. How we design feasibility studies. Am. J. Prev. Med. 2009, 36, 452–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, A.N.; Lachman, M.E. Behavior Change with Fitness Technology in Sedentary Adults: A Review of the Evidence for Increasing Physical Activity. Front. Public Health 2016, 4, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greaves, C.J.; Sheppard, K.E.; Abraham, C.; Hardeman, W.; Roden, M.; Evans, P.H.; Schwarz, P.; Group, I.S. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011, 11, 119. [Google Scholar] [CrossRef] [PubMed]
- Kamwesiga, J.T.; Tham, K.; Guidetti, S. Experiences of using mobile phones in everyday life among persons with stroke and their families in Uganda–a qualitative study. Disabil. Rehabil. 2017, 39, 438–449. [Google Scholar] [CrossRef] [Green Version]
- Bartels, S.L.; van Knippenberg, R.J.M.; Dassen, F.C.M.; Asaba, E.; Patomella, A.H.; Malinowsky, C.; Verhey, F.R.J.; de Vugt, M.E. A narrative synthesis systematic review of digital self-monitoring interventions for middle-aged and older adults. Internet Interv. 2019, 18, 100283. [Google Scholar] [CrossRef]
- Jackson, S.E.; Steptoe, A.; Wardle, J. The influence of partner’s behavior on health behavior change: The English Longitudinal Study of Ageing. JAMA Intern. Med. 2015, 175, 385–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillsdon, M.; Thorogood, M.; White, I.; Foster, C. Advising people to take more exercise is ineffective: A randomized controlled trial of physical activity promotion in primary care. Int. J. Epidemiol. 2002, 31, 808–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller-Riemenschneider, F.; Reinhold, T.; Nocon, M.; Willich, S.N. Long-term effectiveness of interventions promoting physical activity: A systematic review. Prev. Med. 2008, 47, 354–368. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| John | Sam | Richard | Mona | George | Tina | |
|---|---|---|---|---|---|---|
| High stroke risk factors according to the stroke risk score card [34] | ||||||
| Hypertension > 140/90 (Medicating Y/N) | Y (Y) | Y (Y) | Y (Y) | C (Y) | C (Y) | Y (Y) |
| Overweight a (BMI) | Y (31) | Y (27) | Y (29) | Y (27) | Y (26) | Y (28) |
| Atrial fibrillation | N | N | N | N | N | N |
| Smoker | Y | N | N | N | N | N |
| Hypolipidemia | N | Y | N | N | N | N |
| Diabetes | N | N | N | N | N | N |
| Irregular physical exercise (self-reported aerobic exercise minutes/week b) | Y (80) | Y (60) | Y (180) | Y (180) | Y (0) | Y (0) |
| Family history of stroke | Y | Not sure | Y | Y | N | N |
| No. of high-risk factors according to the stroke risk score card [34] | 5 | 4 | 4 | 3 | 2 * | 3 |
| Self-perceived stroke risk (1–10) | 6 | 4 | Missing data | 6 | 1 | 5 |
| Motivation for change | High | High | Moderate | High | High | High |
| EQ5D − VAS 0 = worst imaginable health 100 = best imaginable health | 78 | 50 | 60 | 80 | 75 | 99 |
| 1: Risk for stroke and engaging everyday activities |
| 2: Physical activity |
| 3: Dietary habits |
| 4: Activity balance and stress |
| 5: Sustainable health and goal setting |
| 6: Booster session: Identity, resources, and self-management |
| Participant | Goal Achievement (%) | Participation in EEAs (%) | Physical Activity (%) | Dietary Habits (%) | Stress (%) | Total (%) |
|---|---|---|---|---|---|---|
| John | 97 | 96 | 97 | 99 | 97 | 97.2 |
| Sam | 0 | 59 | 87 | 66 | 62 | 54.8 |
| Richard | 54 | 79 | 87 | 89 | 66 | 75 |
| Mona | 73 | 73 | 73 | 73 | 73 | 73 |
| George | 94 | 90 | 90 | 94 | 90 | 91.6 |
| Tina | 100 | 97 | 100 | 100 | 100 | 99.4 |
| Mean | 69.7 | 82.3 | 89 | 86.8 | 81.3 | 81.8 |
| Participant | Goal 1 (Goal Achievement in %) | Goal 2 (Goal Achievement in %) | Goal 3 (Goal Achievement in %) |
|---|---|---|---|
| John | Keep a healthy weight (76%) | Daily light exercise, i.e., walking 6 K per day (56%) | Swimming 5 times a week (85%) |
| Sam | Implement new sleeping routines—go to bed at latest 11 p.m. (no valid number) | Eat vegetables with each meal (no valid number) | Physical exercise 3 times a week (no valid number) |
| Richard | Eat vegetables with each supper (65%) | Light exercise of at least 20 min/day (35%) | Reduce the intake of snacks and cakes (69%) |
| Mona | 20 min daily walking (11%) | Go to the gym once a week (dancing once a week) (44%) | Eat at least two portions of vegetables per day (48%) |
| George | Go to the gym twice a week (55%) | Eat more fruits (taking lunch walks twice a week) (35%) | Eat more vegetables (42%) |
| Tina | Walk 10 K per week (running 3 times/week) (76%) | Eat at least one fruit per day (96%) | Eat at least one portion of vegetables/day (92%) |
| Factors Effecting Health | Baseline (n = 6) | Follow-Up (n = 6) | 12 Months Follow-Up (n = 5) |
|---|---|---|---|
| Stroke risk factors | |||
| No. of participants with hypertension > 140/90 (medicating) | 4 (6) | 2 (6) | 1 (5 b) |
| No. of participants with overweight a | 6 | 5 | 4 |
| No. of participants with atrial fibrillation | 0 | 0 | 0 |
| No. of smokers | 1 | 1 | 1 |
| No. of participants with hypolipidemia | 1 | 1 | 1 |
| No. of participants with diabetes | 0 | 0 | 0 |
| No. of participants with irregular physical exercise c | 6 | 1 | 3 |
| Median number of high-risk factors (range) | 3.5 (2–5) | 1 (0–3) | 1 (0–2) |
| Quality of life (EQ-5D-VAS 0–100): mean; SD | 73.7; 17.0 | 88.8; 11.7 | 82.0; 14.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patomella, A.-H.; Farias, L.; Eriksson, C.; Guidetti, S.; Asaba, E. Engagement in Everyday Activities for Prevention of Stroke: Feasibility of an mHealth-Supported Program for People with TIA. Healthcare 2021, 9, 968. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9080968
Patomella A-H, Farias L, Eriksson C, Guidetti S, Asaba E. Engagement in Everyday Activities for Prevention of Stroke: Feasibility of an mHealth-Supported Program for People with TIA. Healthcare. 2021; 9(8):968. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9080968
Chicago/Turabian StylePatomella, Ann-Helen, Lisette Farias, Christina Eriksson, Susanne Guidetti, and Eric Asaba. 2021. "Engagement in Everyday Activities for Prevention of Stroke: Feasibility of an mHealth-Supported Program for People with TIA" Healthcare 9, no. 8: 968. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9080968