
Literature Review of Machine-Learning Algorithms for Pressure Ulcer Prevention: Challenges and Opportunities

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Comparison with Previous Reviews
3. Methodology
- Identifying the purpose and intended goals of the review (Section 3).
- Search strategy (Section 3.1).
- Screening for inclusion (Section 3.2).
- Screening for exclusion (Section 3.3).
- Data extraction (Section 4).
- Analysis (Section 4)
- Discussion (Section 5).
- Writing the review.
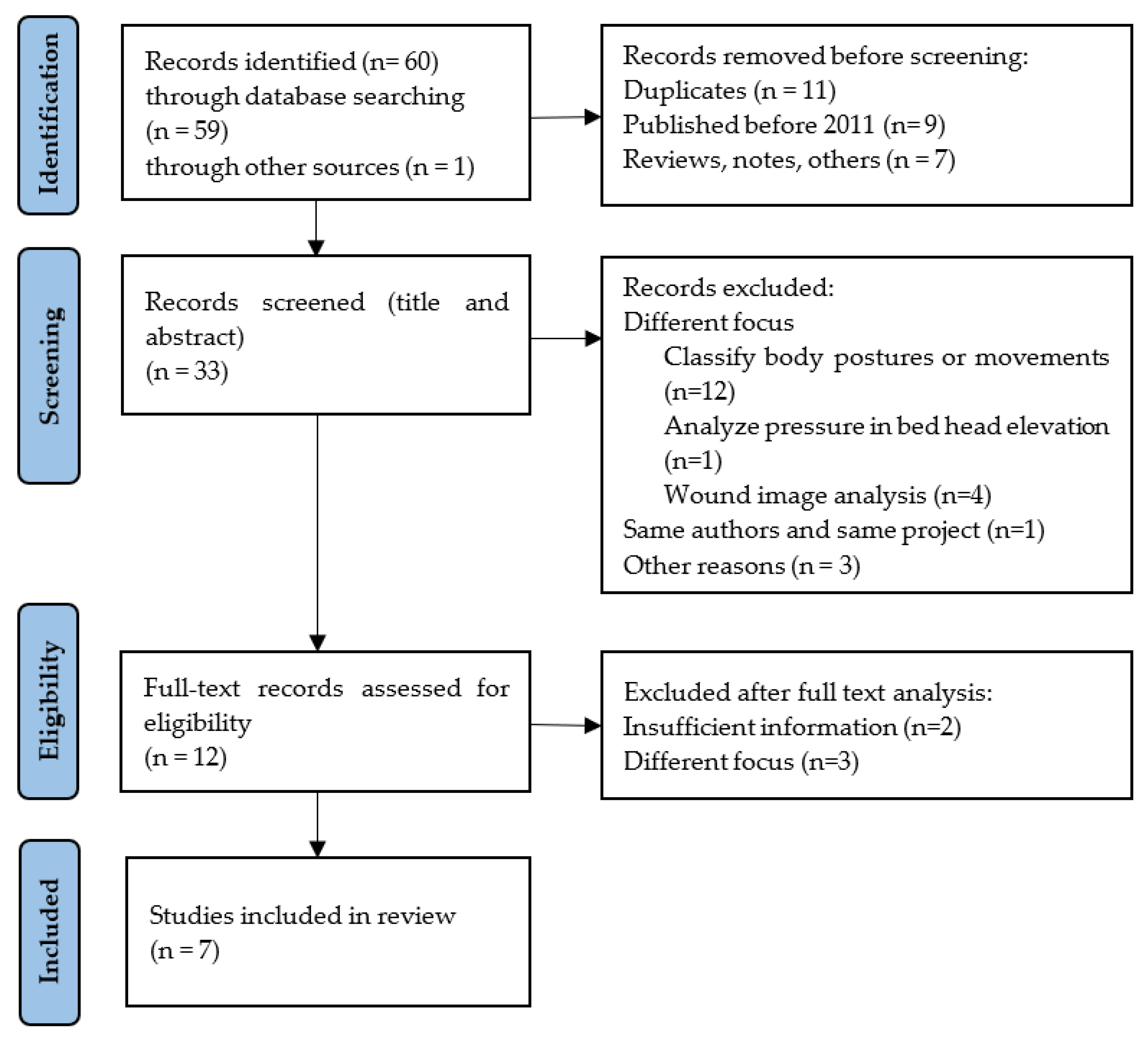
3.1. Search Strategy
3.2. Screening for Inclusion
3.3. Screening for Exclusion
3.4. Results
3.5. Characteristics of Included Studies
4. Data Extraction and Data Analysis
5. Discussion and Findings
6. Challenges and Opportunities
7. Strengths and Limitations of this Review
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bluestein, D.; Javaheri, A. Pressure ulcers: Prevention, evaluation, and management. Am. Fam. Physician 2008, 78, 1186–1194. [Google Scholar]
- Garcia, A.D.; Thomas, D.R. Assessment and management of chronic pressure ulcers in the elderly. Med. Clin. N. Am. 2006, 90, 925–944. [Google Scholar] [CrossRef] [PubMed]
- Haesler, E. (Ed.) National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. In Prevention and Treatment of Pressure Ulcers: Quick Reference Guide; Cambridge Media: Osborne Park, Australia, 2014. [Google Scholar]
- National Institute for Health and Care Excellence Pressure Ulcers. Quality Standard [QS89]. Available online: https://www.nice.org.uk/guidance/qs89 (accessed on 12 July 2021).
- Jaul, E. Assessment and Management of Pressure Ulcers in the Elderly. Drugs Aging 2010, 27, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, R.; Ostadabbas, S.; Faezipour, M.; Nourani, M.; Ng, V.; Tamil, L.; Bowling, A.; Behan, D.; Pompeo, M. A smart bed platform for monitoring & Ulcer prevention. In Proceedings of the 2011 4th International Conference on Biomedical Engineering and Informatics (BMEI), Shanghai, China, 15–17 October 2011; Volume 3, pp. 1362–1366. [Google Scholar] [CrossRef]
- Vázquez-Santacruz, E.; Cruz-Santos, W.; Gamboa-Zúñiga, M. Design and Implementation of an Intelligent System for Controlling a Robotic Hospital Bed for Patient Care Assistance. Comput. Y Sist. 2015, 19, 467–474. [Google Scholar] [CrossRef]
- Chen, H.-L.; Yu, S.-J.; Xu, Y.; Yu, S.-Q.; Zhang, J.-Q.; Zhao, J.-Y.; Liu, P.; Zhu, B. Artificial Neural Network: A Method for Prediction of Surgery-Related Pressure Injury in Cardiovascular Surgical Patients. J. Wound Ostomy Cont. Nurs. Off. Publ. Wound Ostomy Cont. Nurses Soc. 2018, 45, 26–30. [Google Scholar] [CrossRef]
- Cai, J.-Y.; Zha, M.-L.; Song, Y.-P.; Chen, H.-L. Predicting the Development of Surgery-Related Pressure Injury Using a Machine Learning Algorithm Model. J. Nurs. Res. 2020, 29, e135. [Google Scholar] [CrossRef] [PubMed]
- Alderden, J.; Pepper, G.A.; Wilson, A.; Whitney, J.D.; Richardson, S.; Butcher, R.; Jo, Y.; Cummins, M.R. Predicting Pressure Injury in Critical Care Patients: A Machine-Learning Model. Am. J. Crit. Care Off. Publ. Am. Assoc. Crit. Nurses 2018, 27, 461–468. [Google Scholar] [CrossRef]
- Srisrisawang, N.; Narupiyakul, L. Sleep Posture Recognition for Bedridden Patient. In Proceedings of the Mobile and Wireless Technology 2018; Kim, K.J., Kim, H., Eds.; Springer: Singapore, 2019; pp. 79–87. [Google Scholar]
- Huang, A.; Cao, J.; Zhang, H. Construction of patient service system based on QFD in internet of things. J. Supercomput. 2021, 77, 2155–2171. [Google Scholar] [CrossRef]
- Jiang, M.; Ma, Y.; Guo, S.; Jin, L.; Lv, L.; Han, L.; An, N. Using Machine Learning Technologies in Pressure Injury Management: Systematic Review. JMIR Med. Inform. 2021, 9, e25704. [Google Scholar] [CrossRef]
- Shi, C.; Dumville, J.C.; Cullum, N. Evaluating the development and validation of empirically-derived prognostic models for pressure ulcer risk assessment: A systematic review. Int. J. Nurs. Stud. 2019, 89, 88–103. [Google Scholar] [CrossRef] [Green Version]
- Tulloch, J.; Zamani, R.; Akrami, M. Machine Learning in the Prevention, Diagnosis and Management of Diabetic Foot Ulcers: A Systematic Review. IEEE Access 2020, 8, 198977–199000. [Google Scholar] [CrossRef]
- Marchione, F.G.; Araújo, L.M.Q.; Araújo, L.V. Approaches that use software to support the prevention of pressure ulcer: A systematic review. Int. J. Med. Inform. 2015, 84, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Araujo, S.M.; Sousa, P.; Dutra, I. Clinical Decision Support Systems for Pressure Ulcer Management: Systematic Review. JMIR Med. Inform. 2020, 8, e21621. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Barsocchi, P. Position Recognition to Support Bedsores Prevention. IEEE J. Biomed. Health Inform. 2013, 17, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Matar, G.; Lina, J.-M.; Kaddoum, G. Artificial Neural Network for in-Bed Posture Classification Using Bed-Sheet Pressure Sensors. IEEE J. Biomed. Health Inform. 2020, 24, 101–110. [Google Scholar] [CrossRef]
- Baran Pouyan, M.; Ostadabbas, S.; Nourani, M.; Pompeo, M. Classifying bed inclination using pressure images. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 6–30 August 2014; pp. 4663–4666. [Google Scholar] [CrossRef]
- Rodríguez, A.P.; Gil, D.; Nugent, C.; Quero, J.M. In-Bed Posture Classification from Pressure Mat Sensors for the Prevention of Pressure Ulcers Using Convolutional Neural Networks. In Proceedings of the Bioinformatics and Biomedical Engineering; Rojas, I., Valenzuela, O., Rojas, F., Herrera, L.J., Ortuño, F., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 338–349. [Google Scholar]
- Luo, S.; Zhao, C.; Fu, Y. An Intelligent Human Activity Recognition Method with Incremental Learning Capability for Bedridden Patients. In Proceedings of the 2018 15th International Conference on Control, Automation, Robotics and Vision (ICARCV), Singapore, 18–21 November 2018; pp. 1284–1289. [Google Scholar] [CrossRef]
- Kosuge, M.; Ishihara, Y.; Takahashi, M. Body pressure prediction for pressure ulcer prevention in a bed head elevation operation. Adv. Robot. 2021, 35, 181–193. [Google Scholar] [CrossRef]
- Lee, H.J.; Hwang, S.H.; Lee, S.M.; Lim, Y.G.; Park, K.S. Estimation of Body Postures on Bed Using Unconstrained ECG Measurements. IEEE J. Biomed. Health Inform. 2013, 17, 985–993. [Google Scholar] [CrossRef]
- Hung, Y.-W.; Chiu, Y.; Jou, Y.-C.; Chen, W.-H.; Cheng, K.-S. Bed posture classification based on artificial neural network using fuzzy c-means and latent semantic analysis. J. Chin. Inst. Eng. 2015, 38, 415–425. [Google Scholar] [CrossRef]
- Veredas, F.J.; Mesa, H.; Morente, L. Efficient detection of wound-bed and peripheral skin with statistical colour models. Med. Biol. Eng. Comput. 2015, 53, 345–359. [Google Scholar] [CrossRef]
- Zoppo, G.; Marrone, F.; Pittarello, M.; Farina, M.; Uberti, A.; Demarchi, D.; Secco, J.; Corinto, F.; Ricci, E. AI technology for remote clinical assessment and monitoring. J. Wound Care 2020, 29, 692–706. [Google Scholar] [CrossRef] [PubMed]
- Orciuoli, F.; Orciuoli, F.J.; Peduto, A. A Mobile Clinical DSS based on Augmented Reality and Deep Learning for the home cares of patients afflicted by bedsores. Procedia Comput. Sci. 2020, 175, 181–188. [Google Scholar] [CrossRef]
- Kavitha, I.; Suganthi, S.S.; Ramakrishnan, S. Analysis of Chronic Wound Images Using Factorization Based Segmentation and Machine Learning Methods. In Proceedings of the 2017 International Conference on Computational Biology and Bioinformatics; Association for Computing Machinery: New York, NY, USA, 2017; pp. 74–78. [Google Scholar] [CrossRef]


{kind=link}
| Review | Year | Focus | Studies | Timespan |
|---|---|---|---|---|
| [13] | 2021 | Analyze the use of ML technologies in PU management, identify their strengths and weaknesses. | 32 | 2007–2020 |
| [14] | 2019 | Describe empirically derived models (risk assessment tools) for predicting pressure-ulcer risk, assess the predictive performance of these models, and evaluate their clinical impact in reducing PU incidence. | 24 | 1996–2017 |
| [15] | 2020 | Understand and compare the applications of ML in the care of diabetic foot-ulcer patients and compare their diagnostic and prognostic accuracy. | 37 | 2010–2020 |
| [16] | 2015 | Identify the state of art of the approaches that use software that provides relevant information based on monitoring a patient’s risk factor, to assist health professionals in PU prevention support. | 36 | 1989–2014 |
| [17] | 2020 | Identify the outcomes from nurses when using support systems on clinical decision-making for PU management. | 16 | 1995–2017 |
| Review | Analysis/Results | Identified Opportunities and Future Research |
|---|---|---|
| [13] | Studies were classified and organized into three groups: 12 (38%) reported using ML technologies to develop predictive models to identify risk factors, 11 (34%) reported using them in posture detection and recognition, and 9 (28%) reported using them in image analysis for tissue classification and measurement of PU wounds. | Apply these technologies on a large scale with clinical data to further verify and improve their effectiveness, as well as to improve methodological quality. The prevention of PU was studied under different approaches; however, they are related and should be studied together. For example: ML technologies on predictive model and posture recognition need feedback from PU wound image analysis to improve their performance. |
| [14] | The characteristics of the included studies and models are summarized, and performance (discrimination and calibration) measurement statistics are combined for relevant models. | Validate the prognostic models for predicting ulcer risk and evaluate the clinical impact of empirically derived models. |
| [15] | Whilst varying across several ML algorithms, all studies reported at least 90% accuracy. Applications where ML had positive effects on diabetic foot-ulcer data analysis and outcomes include image segmentation and classification, raw data analysis, and risk assessment. | For the development of more applicable ML algorithms, future research should compare the use of ML applications with current standards for care, health economic analyses, and large-scale data collection. |
| [16] | Most of the approaches use sensors to monitor the patient’s exposure to pressure, temperature, and humidity to generate reports regarding the intensity of each one of these risk factors, as well as the patient’s position in bed. Some approaches perform automated management of the risk factors using ventilation tubes and mattresses with porous cells to decrease the body’s temperature and cause movable cells to automatically redistribute the pressure over the body. | Perform randomized control trials to verify which approaches are effective to reduce PU incidence and to verify which information provided by each of the approach is relevant to health professionals to support them on PU prevention. |
| [17] | All the analyzed studies describe knowledge-based systems that assessed the effects on clinical decision-making, clinical effects secondary to clinical decision support system use, or factors that influenced the use, or intention to use, clinical decision support systems by health professionals and the success of their implementation in nursing practice. | Carry out studies that prioritize better adoption and interaction of nurses with clinical decision support systems, as well as studies with a representative sample of healthcare professionals. |
| Item | Description |
|---|---|
| Year of publication | Year of publication |
| Country | Country/territory |
| Document type | Document type (article, conference paper, book chapter) |
| Aim | Main goal of the proposed system |
| AI algorithm | AI-based algorithm used in the proposed system |
| Input | Input variables |
| Predictive model | Details of the predictive model |
| Results and findings | Summary of the main results and findings |
| Study | Year | Country | Type | Summary/Aim |
|---|---|---|---|---|
| [6] | 2011 | USA | Conference paper | Collect information from several sensors incorporated into the bed, analyze the data to create a time-stamped, whole-body pressure distribution map, and command the bed’s actuators to periodically adjust its surface profile to redistribute pressure over the entire body. Predictions are used for issuing an early warning (alert) flag indicating the existence of high risk of developing an ulcer and control command/data for pressure redistribution around high-risk limbs. |
| [7] | 2015 | Mexico | Journal article | Program a sequence of movements of a robotic bed that are executed automatically through electric actuators in response to the pressure distribution of a patient on the bed. |
| [8] | 2018 | China | Journal article | Develop an artificial neural network (ANN) model for predicting surgery-related pressure injury (SRPI) in cardiovascular surgical patients. Four risk factors were included in the ANN model: length of surgery, disease category, age, and corticosteroids. The ANN model had a moderate prediction value for SRPI. |
| [9] | 2020 | China | Journal article | Predict SRPI in cardiovascular surgical patients. An ML model using the XGBoost algorithm is used for SRPI prediction in patients undergoing cardiovascular surgery. As potential risk factors, they use demographic characteristics, SRPI information, and others. They find that the most important predictors are duration of surgery, patient weight, duration of the cardiopulmonary bypass procedure, patient age, and disease category. |
| [10] | 2018 | USA | Journal article | Develop a model for predicting risk of PU among surgical critical care patients. A random forest model is used to predict stage 1, stage 2, and greater injuries, by using the testing set to evaluate classifier performance. |
| [11] | 2019 | Thailand | Conference paper | Design a system to relieve the work for the caretaker of a bedridden patient, consisting of three parts: sleep data collection where a computer, connected to Kinect, will continuously monitor the patient; sleep posture analysis, which will determine the postures of the patient; and sleep notification part which will notify users of the current state of the patient. Three ML algorithms were applied to compare their performance: decision tree (DT), neural network (NN), and support vector machine (SVM). |
| [12] | 2020 | China | Journal article | Construct a patient service system based on quality function deployment (QFD) in the IoT environment. With the support of IoT technology, a deep-learning algorithm and a QFD method were used to build a patient service model to achieve detection and nursing reminders of patients’ physical conditions. |
| Study | Participants | Algorithm | Inputs | Type of Results | Findings |
|---|---|---|---|---|---|
| [6] | NA simulation | SVM | Pressure map (sensor matrix in the bed), level of moisture, temperature, mobility/activity, and blood pressure. | Recognize body posture and predict the risk associated with various limbs and the whole body. Alert caregivers to intervene at an early stage. | This system augments the ability of a care giver, allowing them to provide better care to more patients in less time (without clinical evaluation). |
| [7] | - | SVM | Pressure map from sensor array. | Recognize body posture (four positions) and program a sequence of movements of a robotic bed. | |
| [8] | 149 | ANN | Length of surgery, disease category, age, and perioperative corticosteroid administration. | Predict SRPI in cardiovascular surgical patients. | Findings indicate that surgery duration was the most important risk factor for a SRPI. |
| [9] | 149 | XGBoost | Electronic health records: demographic characteristics (age, gender, weight, and disease category), SRPI information (number of ulcers, ulcer severity, anatomical location, corticosteroid information included administration, type of drug used, drug dosage, and frequency of drug administration), and risk factors (use of vasoactive drugs, experiencing hypotensive periods, hemoglobin level, albumin level, and use of corticosteroids). | Predict SRPI in cardiovascular surgical patients. | The most important variables based on the mean decrease accuracy were, in descending order: duration of surgery, body weight, duration of cardiopulmonary bypass procedure, age, and disease category. |
| [10] | 6376 | RF | Electronic health records: hypotension, level of consciousness (Glasgow Coma Scale), delirium, oxygenation, severity of illness, temperature, vasopressor medication received, body mass index at admission, laboratory value (albumin, creatinine, glucose, hemoglobin, lactate, prealbumin), surgical time. | Predict SRPI in surgical critical care patients. | Variables deemed most important in the algorithm were, in descending order: body mass index, hemoglobin level, creatinine level, time required for surgery, and age. |
| [11] | NN SVM DT | Patients’ movement captured through Kinect. Input data represents the body joints of the patient. | Recognize body posture. Alert caregivers to intervene when the patient is absent or when he or she stays too long in the same position. | NN performs better. | |
| [12] | NA simulation | Deep learning | Firstly, the personal information of the elderly or patients is logged in; secondly, the physiological parameters of the human body are automatically collected, and the physiological signals of the elderly or patients are collected by sensors. | The monitoring terminal send out a warning of abnormal physiological indicators. | If a nurse can look after four patients in the traditional way, with the Service System, he or she can look after six or more patients. Reduce the incidence of a bedsore (22.6% to 4.1%) and increase the average patrol from 30 min to 2 h. |
| Study | Algorithm | Goal | Training | Testing | Accuracy |
|---|---|---|---|---|---|
| [6] | SVM | Posture recognition and predict the risk associated | - | - | 97.7% |
| [7] | SVM | Posture recognition and bed movements | - | - | 99.7% |
| [8] | ANN | Predict surgery-related pressure injury | 73.2% | 26.8% | 81.5% |
| [9] | XGBoost | Predict surgery-related pressure injury | - | - | 80.6% |
| [10] | RF | Predict surgery-related pressure injury | 67% | 33% | 79% |
| [11] | NN | Posture recognition and alerts | - | - | 100% |
| SVM | Posture recognition and alerts | - | - | 100% | |
| DT | Posture recognition and alerts | - | - | 93.3% | |
| [12] | Deep Learning | Send out a warning of abnormal physiological indicators | - | - | 98.53% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro, F.; Fidalgo, F.; Silva, A.; Metrôlho, J.; Santos, O.; Dionisio, R. Literature Review of Machine-Learning Algorithms for Pressure Ulcer Prevention: Challenges and Opportunities. Informatics 2021, 8, 76. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics8040076
Ribeiro F, Fidalgo F, Silva A, Metrôlho J, Santos O, Dionisio R. Literature Review of Machine-Learning Algorithms for Pressure Ulcer Prevention: Challenges and Opportunities. Informatics. 2021; 8(4):76. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics8040076
Chicago/Turabian StyleRibeiro, Fernando, Filipe Fidalgo, Arlindo Silva, José Metrôlho, Osvaldo Santos, and Rogério Dionisio. 2021. "Literature Review of Machine-Learning Algorithms for Pressure Ulcer Prevention: Challenges and Opportunities" Informatics 8, no. 4: 76. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics8040076