
Quantitative Health Risk Assessment of the Chronic Inhalation of Chemical Compounds in Healthcare and Elderly Care Facilities


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hazard Identification and Compounds of Interest
2.2. Dose-Response Assessment
2.3. Exposure Assessment
2.4. Risk Characterization
3. Results
3.1. Organic Compounds Concentrations
3.2. Exposure Assessment
3.3. Deterministic Effects
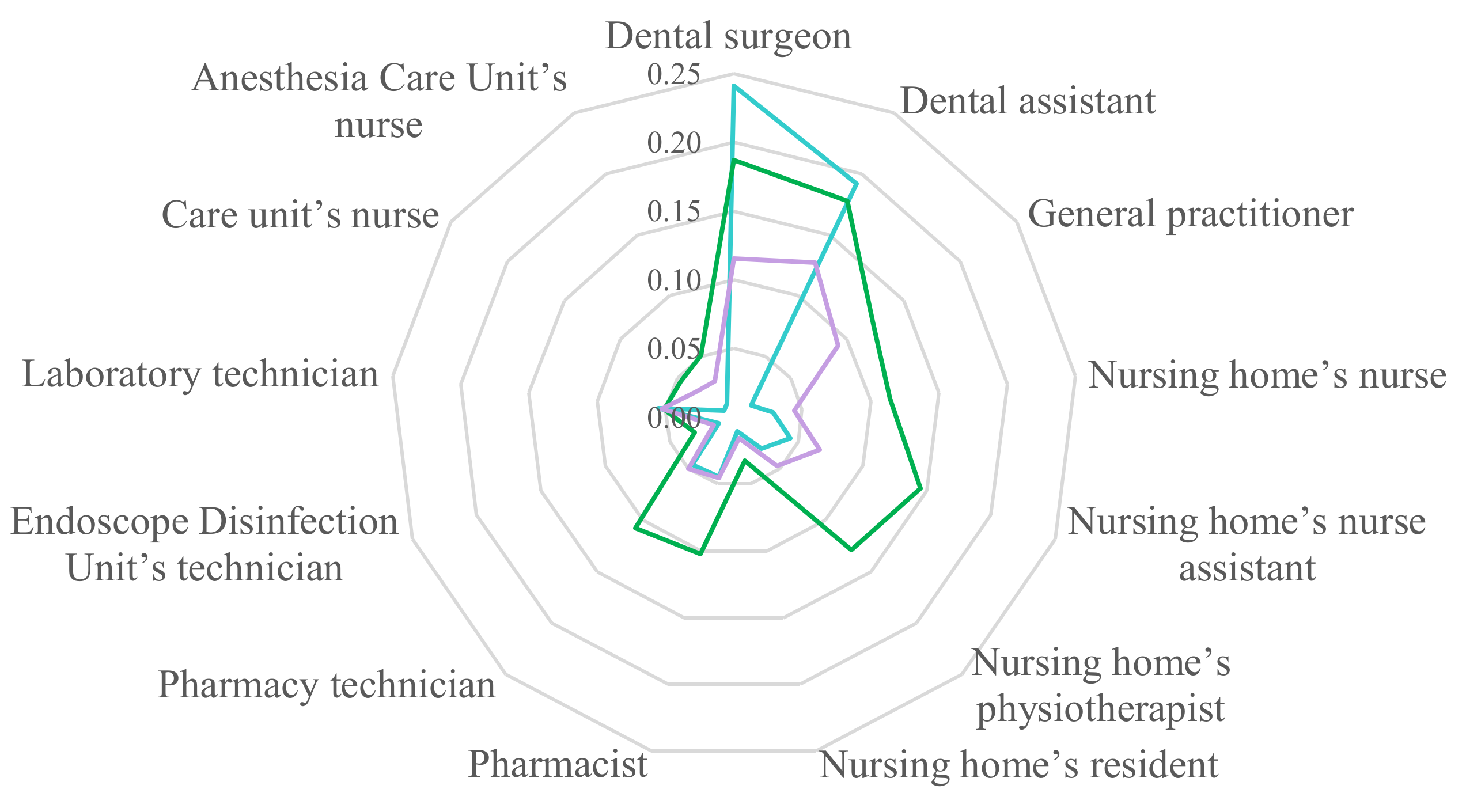
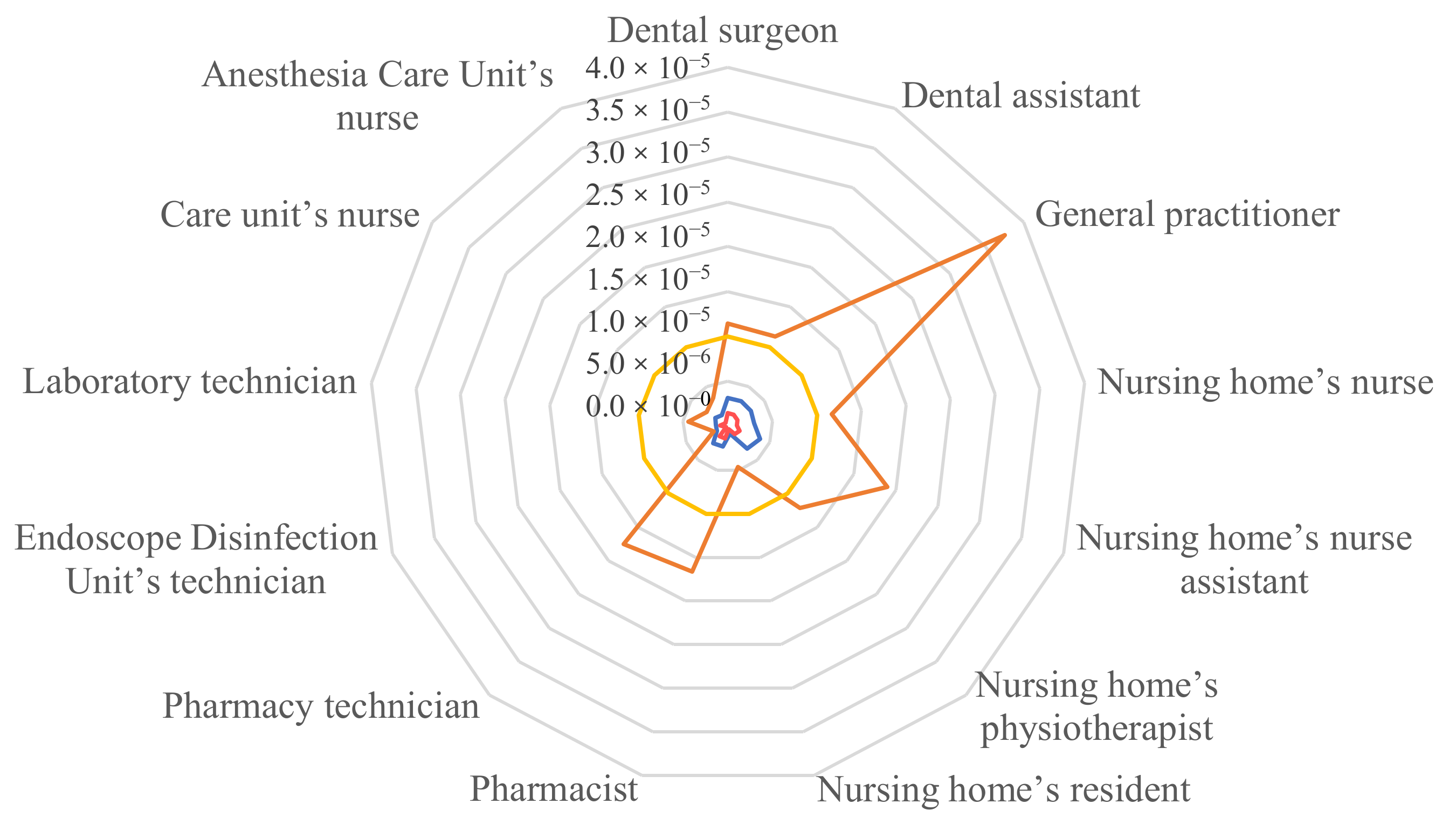
3.4. Stochastic Effects
4. Discussion
4.1. Methodology
4.2. Deterministic Effects
4.3. Stochastic Effects
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paciência, I.; Madureira, J.; Rufo, J.; Moreira, A.; Fernandes, E.; Fernandes, E.D.O. A Systematic Review of Evidence and Implications of Spatial and Seasonal Variations of Volatile Organic Compounds (VOC) in Indoor Human Environments. J. Toxicol. Environ. Health B Crit. Rev. 2016, 19, 47–64. [Google Scholar] [CrossRef] [PubMed]
- Le Cann, P.; Bonvallot, N.; Glorennec, P.; Deguen, S.; Goeury, C.; Le Bot, B. Indoor Environment and Children’s Health: Recent Developments in Chemical, Biological, Physical and Social Aspects. Int. J. Hyg. Environ. Health 2011, 215, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Sérafin, G.; Blondeau, P.; Mandin, C. Indoor Air Pollutant Health Prioritization in Office Buildings. Indoor Air 2021, 31, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, M.; Bonvallot, N.; Ramalho, O.; Mandin, C.; Wei, W.; Raffy, G.; Mercier, F.; Blanchard, O.; Le Bot, B.; Glorennec, P. Indoor Residential Exposure to Semivolatile Organic Compounds in France. Environ. Int. 2017, 109, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Fournier, K.; Glorennec, P.; Bonvallot, N. An Exposure-Based Framework for Grouping Pollutants for a Cumulative Risk Assessment Approach: Case Study of Indoor Semi-Volatile Organic Compounds. Environ. Res. 2014, 130, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Tsai, W.-T. An Overview of Health Hazards of Volatile Organic Compounds Regulated as Indoor Air Pollutants. Rev. Environ. Health 2019, 34, 81–89. [Google Scholar] [CrossRef]
- Matz, C.J.; Stieb, D.M.; Davis, K.; Egyed, M.; Rose, A.; Chou, B.; Brion, O. Effects of Age, Season, Gender and Urban-Rural Status on Time-Activity: Canadian Human Activity Pattern Survey 2 (CHAPS 2). Int. J. Environ. Res. Public Health 2014, 11, 2108–2124. [Google Scholar] [CrossRef] [Green Version]
- Schweizer, C.; Edwards, R.D.; Bayer-Oglesby, L.; Gauderman, W.J.; Ilacqua, V.; Juhani Jantunen, M.; Lai, H.K.; Nieuwenhuijsen, M.; Künzli, N. Indoor Time-Microenvironment-Activity Patterns in Seven Regions of Europe. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 170–181. [Google Scholar] [CrossRef] [Green Version]
- Bessonneau, V.; Mosqueron, L.; Berrubé, A.; Mukensturm, G.; Buffet-Bataillon, S.; Gangneux, J.-P.; Thomas, O. VOC Contamination in Hospital, from Stationary Sampling of a Large Panel of Compounds, in View of Healthcare Workers and Patients Exposure Assessment. PLoS ONE 2013, 8, e55535. [Google Scholar] [CrossRef]
- Zabiegała, B. Organic Compounds in Indoor Environments. Pol. J. Environ. Stud. 2006, 15, 383–393. [Google Scholar]
- Almeida-Silva, M.; Wolterbeek, H.; Almeida, S. Elderly Exposure to Indoor Air Pollutants. Atmos. Environ. 2014, 85, 54–63. [Google Scholar] [CrossRef]
- Hong, Y.-J.; Huang, Y.-C.; Lee, I.-L.; Chiang, C.-M.; Lin, C.; Jeng, H.A. Assessment of Volatile Organic Compounds and Particulate Matter in a Dental Clinic and Health Risks to Clinic Personnel. J. Environ. Sci. Health A Tox Hazard Subst. Environ. Eng. 2015, 50, 1205–1214. [Google Scholar] [CrossRef]
- Hwang, S.H.; Roh, J.; Park, W.M. Evaluation of PM10, CO2, Airborne Bacteria, TVOCs, and Formaldehyde in Facilities for Susceptible Populations in South Korea. Environ. Pollut. 2018, 242, 700–708. [Google Scholar] [CrossRef]
- National Toxicology Program. Final Report on Carcinogens Background Document for Formaldehyde. Rep. Carcinog. Backgr. Doc. 2010, 10-5981, i-512. [Google Scholar]
- Baurès, E.; Blanchard, O.; Mercier, F.; Surget, E.; Le Cann, P.; Rivier, A.; Gangneux, J.-P.; Florentin, A. Indoor Air Quality in Two French Hospitals: Measurement of Chemical and Microbiological Contaminants. Sci. Total Environ. 2018, 642, 168–179. [Google Scholar] [CrossRef]
- Baudet, A.; Baurès, E.; Guegan, H.; Blanchard, O.; Guillaso, M.; Le Cann, P.; Gangneux, J.-P.; Florentin, A. Indoor Air Quality in Healthcare and Care Facilities: Chemical Pollutants and Microbiological Contaminants. Atmosphere 2021, 12, 1337. [Google Scholar] [CrossRef]
- Berrubé, A.; Mosqueron, L.; Cavereau, D.; Gangneux, J.-P.; Thomas, O. Méthodologie d’évaluation Semi-Quantitative Du Risque Chimique En Établissement de Soins. Environ. Risques St. 2013, 12, 508–520. [Google Scholar] [CrossRef]
- Ministère de L’écologie, du Développement; Durable et de L’énergie. DGS/EA1/DGPR/2014/307:Note D’Information Relative Aux Modalités de Sélection des Substances Chimiques et de Choix des Valeurs Toxicologiques de Référence Pour Mener les Évaluations des Risques Sanitaires Dans le Cadre des Études D’Impact et de La Gestion des Sites et Sols Pollués; Ministère de L’écologie, du Développement; Durable et de L’énergie: Paris, France, 2014. [Google Scholar]
- Mathieu-Huart, A.; De Lentdecker, C.; Rivière, G.; Sissoko, F.; Rousselle, C. Valeurs sanitaires de référence (VR) de l’Agence nationale de sécurité sanitaire de l’alimentation, de l’environnement et du travail (ANSES). Arch. Mal. Prof. Environ. 2014, 75, 292–301. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. U.S. EPA. Exposure Factors Handbook 2011 Edition (Final Report); EPA/600/R-09/052F; U.S. Environmental Protection Agency: Washington, DC, USA, 2011. [Google Scholar]
- Jakoubovitch, S. Les Emplois Du Temps Des Médecins Généralistes. EtudesRésultats Dir. Rech. Études Évalua. Stat. 2012, 797, 1–8. [Google Scholar]
- Coppalle, A.; Beaudeau, P.; Delmas, V. Le Transfert Extérieur/Intérieur Des Polluants Atmosphériques: Approches Statistiques et Physiques Utiles Pour Le Calcul de l’exposition Des Populations. Pollut. Atmos. 2002, 2268-3798, 407–419. [Google Scholar] [CrossRef] [Green Version]
- Mandin, C.; Trantallidi, M.; Cattaneo, A.; Canha, N.; Mihucz, V.G.; Szigeti, T.; Mabilia, R.; Perreca, E.; Spinazzè, A.; Fossati, S.; et al. Assessment of Indoor Air Quality in Office Buildings across Europe—The OFFICAIR Study. Sci. Total Environ. 2017, 579, 169–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dallongeville, A.; Costet, N.; Zmirou-Navier, D.; Le Bot, B.; Chevrier, C.; Deguen, S.; Annesi-Maesano, I.; Blanchard, O. Volatile and Semi-Volatile Organic Compounds of Respiratory Health Relevance in French Dwellings. Indoor Air 2016, 26, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Wolkoff, P.; Nielsen, G.D. Effects by Inhalation of Abundant Fragrances in Indoor Air—An Overview. Environ. Int. 2017, 101, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Wakayama, T.; Ito, Y.; Sakai, K.; Miyake, M.; Shibata, E.; Ohno, H.; Kamijima, M. Comprehensive Review of 2-ethyl-1-hexanol as an Indoor Air Pollutant. J. Occup. Health 2019, 61, 19–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruno, P.; Caselli, M.; de Gennaro, G.; Iacobellis, S.; Tutino, M. Monitoring of Volatile Organic Compounds in Non-Residential Indoor Environments. Indoor Air 2008, 18, 250–256. [Google Scholar] [CrossRef]
- U.S. EPA. Provisional Peer-Reviewed Toxicity Values for 2-Ethylhexanol (CASRN 104-76-7); U.S. EPA: Washington, DC, USA, 2019; p. 166. [Google Scholar]
- Langer, S.; Ramalho, O.; Derbez, M.; Ribéron, J.; Kirchner, S.; Mandin, C. Indoor Environmental Quality in French Dwellings and Building Characteristics. Atmos. Environ. 2016, 128, 82–91. [Google Scholar] [CrossRef]
- Pelletier, M.; Glorennec, P.; Mandin, C.; Le Bot, B.; Ramalho, O.; Mercier, F.; Bonvallot, N. Chemical-by-Chemical and Cumulative Risk Assessment of Residential Indoor Exposure to Semivolatile Organic Compounds in France. Environ. Int. 2018, 117, 22–32. [Google Scholar] [CrossRef]
- Billionnet, C.; Gay, E.; Kirchner, S.; Leynaert, B.; Annesi-Maesano, I. Quantitative Assessments of Indoor Air Pollution and Respiratory Health in a Population-Based Sample of French Dwellings. Environ. Res. 2011, 111, 425–434. [Google Scholar] [CrossRef]
- Zhang, H.; Ji, Y.; Wu, Z.; Peng, L.; Bao, J.; Peng, Z.; Li, H. Atmospheric Volatile Halogenated Hydrocarbons in Air Pollution Episodes in an Urban Area of Beijing: Characterization, Health Risk Assessment and Sources Apportionment. Sci. Total Environ. 2022, 806, 150283. [Google Scholar] [CrossRef]
- National Toxicology Program. Naphthalene. Rep. Carcinog. 2011, 12, 276–278. [Google Scholar]
- Huff, J.; Chan, P.; Melnick, R. Clarifying Carcinogenicity of Ethylbenzene. Regul. Toxicol. Pharmacol. 2010, 58, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Johnson, G.T.; Harbison, S.C.; McCluskey, J.D.; Harbison, R.D. Characterization of Cancer Risk from Airborne Benzene Exposure. Regul. Toxicol. Pharmacol. 2009, 55, 361–366. [Google Scholar] [CrossRef]
- Kang, M.-S.; Hong, J.-R.; Gil, H.-W.; Yang, J.-O.; Lee, E.-Y.; Hong, S.-Y.; Jun, Y.-T.; Son, B.-S. Benzene and Toluene Concentrations in a Hemodialysis Room in a Medium Sized South Korean City. Korean J. Intern. Med. 2008, 23, 111–115. [Google Scholar] [CrossRef]
- AFSSET. Risques Sanitaires Liés à La Présence de Formaldéhyde Dans Les Environnements Intérieurs Et Extérieurs Toxicité Du Formaldéhyde; Agence Française de Sécurité Sanitaire De L’Environnement Et Du Travail: Paris, France, 2008; p. 5. [Google Scholar]
- HCSP. Valeurs Repères D’aide à La Gestion de la Qualité de L’air Intérieur—Le Formaldéhyde; Haut Conseil de la Santé Publique: Paris, France, 2019. [Google Scholar]
- Canha, N.; Mandin, C.; Ramalho, O.; Wyart, G.; Ribéron, J.; Dassonville, C.; Hänninen, O.; Almeida, S.M.; Derbez, M. Assessment of Ventilation and Indoor Air Pollutants in Nursery and Elementary Schools in France. Indoor Air 2016, 26, 350–365. [Google Scholar] [CrossRef]
- Sarigiannis, D.A.; Karakitsios, S.P.; Gotti, A.; Liakos, I.L.; Katsoyiannis, A. Exposure to Major Volatile Organic Compounds and Carbonyls in European Indoor Environments and Associated Health Risk. Environ. Int. 2011, 37, 743–765. [Google Scholar] [CrossRef]
- Cheng, Z.; Li, B.; Yu, W.; Wang, H.; Zhang, T.; Xiong, J.; Bu, Z. Risk Assessment of Inhalation Exposure to VOCs in Dwellings in Chongqing, China. Toxicol. Res. 2017, 7, 59–72. [Google Scholar] [CrossRef] [Green Version]
- Alamri, S.H.; Ali, N.; Ali Albar, H.M.S.; Rashid, M.I.; Rajeh, N.; Ali Qutub, M.M.; Malarvannan, G. Polycyclic Aromatic Hydrocarbons in Indoor Dust Collected during the COVID-19 Pandemic Lockdown in Saudi Arabia: Status, Sources and Human Health Risks. Int. J. Environ. Res. Public Health 2021, 18, 2743. [Google Scholar] [CrossRef]
- Edwards, L.; Rutter, G.; Iverson, L.; Wilson, L.; Chadha, T.S.; Wilkinson, P.; Milojevic, A. Personal Exposure Monitoring of PM2.5 among US Diplomats in Kathmandu during the COVID-19 Lockdown, March to June 2020. Sci. Total Environ. 2021, 772, 144836. [Google Scholar] [CrossRef]
- Mor, S.; Kumar, S.; Singh, T.; Dogra, S.; Pandey, V.; Ravindra, K. Impact of COVID-19 Lockdown on Air Quality in Chandigarh, India: Understanding the Emission Sources during Controlled Anthropogenic Activities. Chemosphere 2021, 263, 127978. [Google Scholar] [CrossRef]
- Ministère des Solidarités et de la Santé. Ministère des Solidarités et de la Santé Recommandations En Matière d’aération, de Ventilation, de Climatisation et de Chauffage En Période D’épidémie de COVID-19 2020; Ministère des Solidarités et de la Santé: Paris, France, 2020; pp. 1–9. [Google Scholar]
- Derruau, S.; Bouchet, J.; Nassif, A.; Baudet, A.; Yasukawa, K.; Lorimier, S.; Prêcheur, I.; Bloch-Zupan, A.; Pellat, B.; Chardin, H.; et al. COVID-19 and Dentistry in 72 Questions: An Overview of the Literature. J. Clin. Med. 2021, 10, 779. [Google Scholar] [CrossRef]
- Kirchner, S.; Arenes, J.-F.; Cochet, C.; Derbez, M.; Duboudin, C.; Elias, P.; Gregoire, A. Campagne Nationale Logements: État de La Qualité de L’air Dans Les Logements Français. Rapport Final, Observatoire de La Qualité de L’air Intérieur; OQAI: Paris, France, 2007; p. 183. [Google Scholar]
- HCSP. COVID-19: Aération, Ventilation et Mesure Du CO2 Dans Les ERP; Haut Conseil de la Santé Publique: Paris, France, 2021. [Google Scholar]



{kind=link}
{kind=link}
| Organic Compound | |
|---|---|
| Volatile Organic Compounds (VOCs) (36) | |
| Aromatic hydrocarbons (9) | benzene, ethylbenzene, styrene, toluene, o-xylene, mp-xylenes, 1,2,4-trimethylbenzene, naphthalene, phenol |
| Aliphatic hydrocarbons (3) | n-decane, n-undecane, n-heptane |
| Halogenated hydrocarbons (7) | 1,1,1-trichloroethane, 1,4-dichlorobenzene, trichloroethylene, tetrachloroethylene, bromodichloromethane, tribromomethane, trichloromethane |
| Alcohols (4) | 2-ethyl-1-hexanol, ethanol, isopropanol, n-propanol |
| Ketones (2) | acetone, 2-butanone |
| Terpenes (1) | limonene |
| Ethers (3) | ether, 2-ethoxyethanol, 2-butoxyethanol |
| Aldehydes (7) | formaldehyde, acetaldehyde, propionaldehyde, butyraldehyde, isovaleraldehyde, valeraldehyde, hexaldehyde |
| Semi-volatile organic compounds (SVOCs) (13) | |
| Phthalates (6) | di(2-ethylhexyl)phthalate (DEHP), diethylphthalate (DEP), dibutylphthalate (DBP), diisobutyltphthalate (DiBP), benzylbutylphthalate (BBP), diisononylphthalate (DiNP) |
| Musk (2) | tonalide, galaxolide |
| Pyrethroids (5) | cyfluthrine, cypermethrine, deltamethrine, permethrine, tetramethrine |
| Facilities (Number) | Rooms | Sampling Period |
|---|---|---|
| Hospitals (2) | Patient room Reception hall Parasitology and mycology laboratory Plaster cast room Post-anesthesia care unit Nursing care room Flexible endoscope disinfection unit | Summer 2014 Winter 2015 |
| Dental offices (2) | Sterilization room Waiting room Treatment room | Summer 2018 Winter 2019 |
| General practitioner offices (2) | Waiting room Consulting room | |
| Pharmacies (2) | Commercial space Storage room | |
| Nursing homes (4) | Resident’s bedroom Common room (refectory or lounge) |
| Exposure Scenarios | Number of Respondents | Number of Days Worked per Week | Number of Weeks Worked per Year | Mean Daily Time Spent in the Different Premises (Hours) |
|---|---|---|---|---|
| Dental surgeon | 3 (questionnaire) | 4.2 | 47.0 | Treatment room: 7.0 Sterilization room: 0.2 Waiting room: 0.0 Other rooms: 0.7 |
| Dental assistant | 3 (questionnaire) | 4.0 | 45.0 | Treatment room: 5.5 Sterilization room: 0.7 Waiting room: 0.2 Other rooms: 2.5 |
| General practitioner | 2161 (national survey data [21]) | 5.0 | 46.7 | Consulting room: 10.0 Other rooms: 1.4 |
| Nursing home’s nurse | 2 (questionnaire) | 3.0 | 47.0 | Common room: 1.7 Resident’s room: 6.0 Other rooms: 4.3 |
| Nursing home’s nurse assistant | 2 (questionnaire) | 3.0 | 47.0 | Common room: 3.0 Resident’s room: 7.0 Other rooms: 1.0 |
| Nursing home’s physiotherapist | 1 (questionnaire) | 5.0 | 44.0 | Common room: 0.0 Resident’s room: 3.0 Other rooms: 4.5 |
| Nursing home’s resident | 1 (questionnaire) | 7.0 | 52.0 | Common room: 0.5 Resident’s room: 23.0 Other rooms: 0.5 |
| Pharmacist | 1 (questionnaire) | 5.0 | 47.0 | Commercial space: 5.0 Storage room: 2.0 |
| Pharmacy technician | 1 (questionnaire) | 5.0 | 47.0 | Commercial space: 6.5 Storage room: 1.0 |
| Endoscope Disinfection Unit’s technician | 5 (observational data) | 5.0 | 44.0 | Flexible Endoscope Disinfection Unit: 5.0 Other rooms: 3.3 |
| Laboratory technician | 5 (observational data) | 5.0 | 44.0 | Laboratory: 3.8 Other rooms: 4.5 |
| Care unit’s nurse | 5 (observational data) | 5.0 | 44.0 | Nursing Care Room: 3.0 Patient Room: 4.0 Other rooms: 1.3 |
| Anesthesia Care Unit’s nurse | 5 (observational data) | 5.0 | 44.0 | Post-Anesthesia Care Unit: 6.0 Other rooms: 2.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colas, A.; Baudet, A.; Le Cann, P.; Blanchard, O.; Gangneux, J.-P.; Baurès, E.; Florentin, A. Quantitative Health Risk Assessment of the Chronic Inhalation of Chemical Compounds in Healthcare and Elderly Care Facilities. Toxics 2022, 10, 141. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics10030141
Colas A, Baudet A, Le Cann P, Blanchard O, Gangneux J-P, Baurès E, Florentin A. Quantitative Health Risk Assessment of the Chronic Inhalation of Chemical Compounds in Healthcare and Elderly Care Facilities. Toxics. 2022; 10(3):141. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics10030141
Chicago/Turabian StyleColas, Anaïs, Alexandre Baudet, Pierre Le Cann, Olivier Blanchard, Jean-Pierre Gangneux, Estelle Baurès, and Arnaud Florentin. 2022. "Quantitative Health Risk Assessment of the Chronic Inhalation of Chemical Compounds in Healthcare and Elderly Care Facilities" Toxics 10, no. 3: 141. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics10030141