
Influence of Skin Marker Positioning and Their Combinations on Hip Joint Center Estimation Using the Functional Method

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Methods
2.3. Measurement Protocol
2.3.1. Anthropometric Data
2.3.2. Marker Placement
2.3.3. Data Acquisition
- − Static calibration for the predictive methods.
- − Dynamic calibration using a star-arc movement [23] for the functional method.
2.3.4. Data Processing
2.3.5. Estimate of the HJC by the Functional Method
2.3.6. Estimate of the HJC by the Predictive Method
2.4. Statistical Analysis
- − Mean norm (in mm) ± SD and range (max-min) for each combination.
- − Mean coordinates ± SD and range (max-min) in X, Y and Z of each combination.
- − Mean norms using the mean norms of each subject (in mm).
- − Mean SD of the norms using the mean SD of each subject.
- − Mean of the norm ranges using the mean ranges of each subject.
- − Mean coordinates (X, Y, Z) using the mean coordinates in X, Y, Z of each subject.
- − Mean SD of coordinates (X, Y, Z) using the mean SD in X, Y, Z of each subject.
- − Mean range of coordinates (X, Y, Z) using the mean range in X, Y, Z of each subject.
3. Results
3.1. Comparison of Combinations to Each Other Based on Their Norms
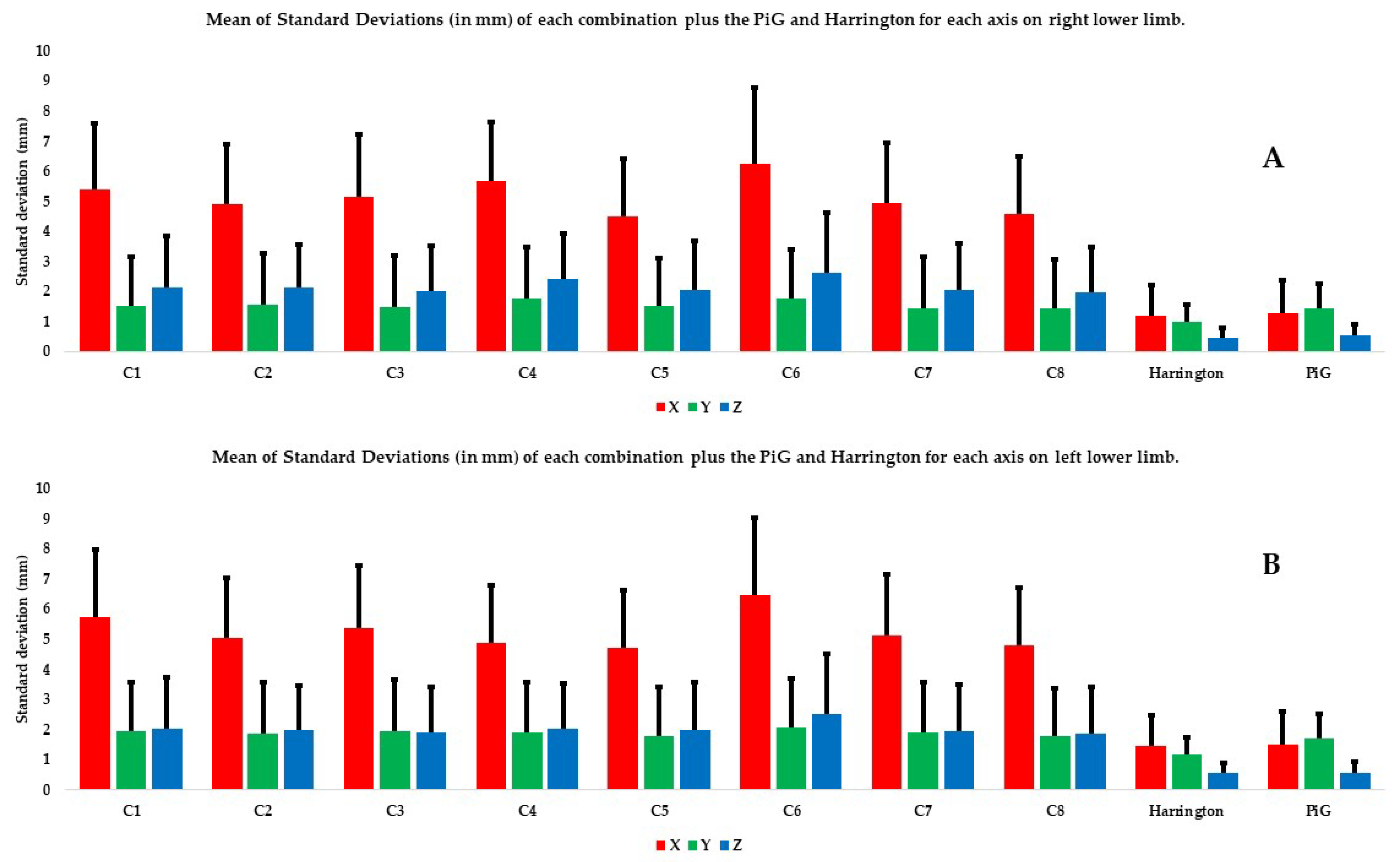
3.2. Comparison between Combinations Based on Their Coordinates on the Different Axes
3.3. Comparison with Predictive Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oppelt, K.; Hogan, A.; Stief, F.; Grützner, P.A.; Trinler, U. Movement Analysis in Orthopedics and Trauma Surgery—Measurement Systems and Clinical Applications. Z. Orthop. Unfallchirurgie 2020, 158, 304–317. [Google Scholar] [CrossRef] [PubMed]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E.; Gainey, J.; Gorton, G.; Cochran, G.V.B. Repeatability of Kinematic, Kinetic, and Electromyographic Data in Normal Adult Gait. J. Orthop. Res. 1989, 7, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Bouffard, V.; Begon, M.; Champagne, A.; Farhadnia, P.; Vendittoli, P.-A.; Lavigne, M.; Prince, F. Hip Joint Center Localisation: A Biomechanical Application to Hip Arthroplasty Population. World J. Orthop. 2012, 3, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Nantel, J.; Termoz, N.; Vendittoli, P.-A.; Lavigne, M.; Prince, F. Gait Patterns after Total Hip Arthroplasty and Surface Replacement Arthroplasty. Arch. Phys. Med. Rehabil. 2009, 90, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Lenaerts, G.; Bartels, W.; Gelaude, F.; Mulier, M.; Spaepen, A.; Van der Perre, G.; Jonkers, I. Subject-Specific Hip Geometry and Hip Joint Centre Location Affects Calculated Contact Forces at the Hip during Gait. J. Biomech. 2009, 42, 1246–1251. [Google Scholar] [CrossRef] [PubMed]
- Lenaerts, G.; Mulier, M.; Spaepen, A.; Van der Perre, G.; Jonkers, I. Aberrant Pelvis and Hip Kinematics Impair Hip Loading before and after Total Hip Replacement. Gait Posture 2009, 30, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Sangeux, M.; Pillet, H.; Skalli, W. Which Method of Hip Joint Centre Localisation Should Be Used in Gait Analysis? Gait Posture 2014, 40, 20–25. [Google Scholar] [CrossRef]
- Stagni, R.; Leardini, A.; Cappozzo, A.; Grazia Benedetti, M.; Cappello, A. Effects of Hip Joint Centre Mislocation on Gait Analysis Results. J. Biomech. 2000, 33, 1479–1487. [Google Scholar] [CrossRef]
- Ehrig, R.M.; Heller, M.O.; Kratzenstein, S.; Duda, G.N.; Trepczynski, A.; Taylor, W.R. The SCoRE Residual: A Quality Index to Assess the Accuracy of Joint Estimations. J. Biomech. 2011, 44, 1400–1404. [Google Scholar] [CrossRef]
- Ehrig, R.M.; Taylor, W.R.; Duda, G.N.; Heller, M.O. A Survey of Formal Methods for Determining the Centre of Rotation of Ball Joints. J. Biomech. 2006, 39, 2798–2809. [Google Scholar] [CrossRef]
- Fiorentino, N.M.; Kutschke, M.J.; Atkins, P.R.; Foreman, K.B.; Kapron, A.L.; Anderson, A.E. Accuracy of Functional and Predictive Methods to Calculate the Hip Joint Center in Young Non-Pathologic Asymptomatic Adults with Dual Fluoroscopy as a Reference Standard. Ann. Biomed. Eng. 2016, 44, 2168–2180. [Google Scholar] [CrossRef]
- Kainz, H.; Carty, C.P.; Modenese, L.; Boyd, R.N.; Lloyd, D.G. Estimation of the Hip Joint Centre in Human Motion Analysis: A Systematic Review. Clin. Biomech. 2015, 30, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Kainz, H.; Hajek, M.; Modenese, L.; Saxby, D.J.; Lloyd, D.G.; Carty, C.P. Reliability of Functional and Predictive Methods to Estimate the Hip Joint Centre in Human Motion Analysis in Healthy Adults. Gait Posture 2017, 53, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Leboeuf, F.; Baker, R.; Barré, A.; Reay, J.; Jones, R.; Sangeux, M. The Conventional Gait Model, an Open-Source Implementation That Reproduces the Past but Prepares for the Future. Gait Posture 2019, 69, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Pillet, H.; Sangeux, M.; Hausselle, J.; El Rachkidi, R.; Skalli, W. A Reference Method for the Evaluation of Femoral Head Joint Center Location Technique Based on External Markers. Gait Posture 2014, 39, 655–658. [Google Scholar] [CrossRef]
- Sangeux, M. On the Implementation of Predictive Methods to Locate the Hip Joint Centres. Gait Posture 2015, 42, 402–405. [Google Scholar] [CrossRef]
- Lalevée, M.; Martinez, L.; Rey, B.; Beldame, J.; Matsoukis, J.; Poirier, T.; Brunel, H.; Van Driessche, S.; Noé, N.; Billuart, F. Gait Analysis after Total Hip Arthroplasty by Direct Minimally Invasive Anterolateral Approach: A Controlled Study. Orthop. Traumatol. Surg. Res. 2022, 109, 103521. [Google Scholar] [CrossRef]
- Martinez, L.; Noé, N.; Beldame, J.; Matsoukis, J.; Poirier, T.; Brunel, H.; Van Driessche, S.; Lalevée, M.; Billuart, F. Quantitative Gait Analysis after Total Hip Arthroplasty through a Minimally Invasive Direct Anterior Approach: A Case Control Study. Orthop. Traumatol. Surg. Res. 2022, 108, 103214. [Google Scholar] [CrossRef]
- Harrington, M.E.; Zavatsky, A.B.; Lawson, S.E.M.; Yuan, Z.; Theologis, T.N. Prediction of the Hip Joint Centre in Adults, Children, and Patients with Cerebral Palsy Based on Magnetic Resonance Imaging. J. Biomech. 2007, 40, 595–602. [Google Scholar] [CrossRef]
- Assi, A.; Sauret, C.; Massaad, A.; Bakouny, Z.; Pillet, H.; Skalli, W.; Ghanem, I. Validation of Hip Joint Center Localization Methods during Gait Analysis Using 3D EOS Imaging in Typically Developing and Cerebral Palsy Children. Gait Posture 2016, 48, 30–35. [Google Scholar] [CrossRef]
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A Gait Analysis Data Collection and Reduction Technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Baker, R.; Leboeuf, F.; Reay, J.; Sangeux, M. The Conventional Gait Model—Success and Limitations. In Handbook of Human Motion; Springer International Publishing: Cham, Switzerland, 2018; pp. 489–508. ISBN 978-3-319-14417-7. [Google Scholar]
- Camomilla, V.; Cereatti, A.; Vannozzi, G.; Cappozzo, A. An Optimized Protocol for Hip Joint Centre Determination Using the Functional Method. J. Biomech. 2006, 39, 1096–1106. [Google Scholar] [CrossRef]
- Hara, R.; Sangeux, M.; Baker, R.; McGinley, J. Quantification of Pelvic Soft Tissue Artifact in Multiple Static Positions. Gait Posture 2014, 39, 712–717. [Google Scholar] [CrossRef]
- Kratzenstein, S.; Kornaropoulos, E.I.; Ehrig, R.M.; Heller, M.O.; Pöpplau, B.M.; Taylor, W.R. Effective Marker Placement for Functional Identification of the Centre of Rotation at the Hip. Gait Posture 2012, 36, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Heller, M.O.; Kratzenstein, S.; Ehrig, R.M.; Wassilew, G.; Duda, G.N.; Taylor, W.R. The Weighted Optimal Common Shape Technique Improves Identification of the Hip Joint Center of Rotation in Vivo. J. Orthop. Res. 2011, 29, 1470–1475. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.R.; Ehrig, R.M.; Duda, G.N.; Schell, H.; Seebeck, P.; Heller, M.O. On the Influence of Soft Tissue Coverage in the Determination of Bone Kinematics Using Skin Markers. J. Orthop. Res. 2005, 23, 726–734. [Google Scholar] [CrossRef]
- Begon, M.; Monnet, T.; Lacouture, P. Effects of Movement for Estimating the Hip Joint Centre. Gait Posture 2007, 25, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Hara, R.; McGinley, J.; Briggs, C.; Baker, R.; Sangeux, M. Predicting the Location of the Hip Joint Centres, Impact of Age Group and Sex. Sci. Rep. 2016, 6, 37707. [Google Scholar] [CrossRef]
- Fiorentino, N.M.; Atkins, P.R.; Kutschke, M.J.; Foreman, K.B.; Anderson, A.E. In-Vivo Quantification of Dynamic Hip Joint Center Errors and Soft Tissue Artifact. Gait Posture 2016, 50, 246–251. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD (min–max) | |
|---|---|
| Number | 41 |
| Age (years) | 22.7 ± 5.69 (19–45) |
| Sex (Male (M)/Female (F)) | 20/21 |
| Height (cm) | 172 ± 0.09 (168–182) |
| Mass (kg) | 64.80 ± 10.9 (59.45–83.56) |
| Body mass index (kg/m2) | 21.91 ± 2.76 (19.12–24.77) |
| Segment | Number of Markers | Marker Name | Anatomical Landmark |
|---|---|---|---|
| Pelvis | 2 (4 on both sides) | ASIS | Anterosuperior iliac spine [21] |
| PSIS | Posterosuperior iliac spine [21] | ||
| Thigh | 11 (22 on both sides) | GTR | Greater trochanter [21] |
| THIAP | Proximally from the belly of the rectus femoris = AI in Kratzenstein et al. [25] | ||
| THIAD | Anterolateral area of the distal thigh = AII in Kratzenstein et al. [25] | ||
| THILP | Proximally along the tensor fascia lata = LI in Kratzenstein et al. [25] | ||
| THILD | Distally along the tensor fascia lata = LII in Kratzenstein et al. [25] | ||
| THIPP | Proximal to the belly of the biceps femoris and semitendinosus = PI in Kratzenstein et al. [25] | ||
| THIPD | Distal to the belly of the biceps femoris and semitendinosus = PII in Kratzenstein et al. [25] | ||
| THI | Right side: inferior third of lateral portion of thigh Left side: superior third of lateral portion of thigh | ||
| KNE | Lateral femoral condyle [21] | ||
| PAT | Middle of superior edge of patella [21] | ||
| MKNE | Medial femoral condyle [21] |
| Name of Combination | Markers Included | Potential Clinical Benefit |
|---|---|---|
| C1 = all the markers | All the markers | Will using all the markers improve the accuracy of the HJC estimate compared to predictive methods? |
| C2 = markers on the bony landmarks | GTR MKNE KNE + pelvis | Simplify method by using only bone markers (easily palpable) |
| C3 = proximal and distal posterior markers | GTR MKNE KNE + pelvis THIPP THIPD | Simplify method by using only the lateral, anterior, or posterior skin markers |
| C4 = lateral markers | GTR MKNE KNE + pelvis THILP THILD | |
| C5 = proximal and distal anterior markers | GTR MKNE KNE + pelvis THIAP THIAD | |
| C6 = proximal and distal anterior markers without the pelvis markers | GTR MKNE KNE THIAP THIAD | Potentially useful if the pelvic bony landmarks cannot be palpated (too much soft tissue on the bony landmarks) |
| C7 = anterior distal and posterior proximal markers | GTR MKNE KNE + pelvis THIAD THIPP | The THIAP, THIAD, THIPP, and THIPD markers are located in the corresponding regions on the muscle bellies (anterior: quadriceps; posterior: hamstrings). These locations are easier to palpate but could be affected by STA |
| C8 = anterior proximal and posterior distal markers | GTR MKNE KNE + pelvis THIAP THIPD |
| p value range of the norm for each combination in the right lower limb | p value range of the norm for each combination in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | P | ||||||||||||||||||||
| p value mean of the norm for each combination in the right lower limb | p value mean of the norm for each combination in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | P | ||||||||||||||||||||
| p value SD of the norm for each combination in the right lower limb | p value SD of the norm for each combination in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | PiG | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | P | ||||||||||||||||||||
| Red: p > 0.001; Green = p < 0.001. p = Plug-in Gait; H = Harrington | |||||||||||||||||||||
| p value SD of X coordinates in the right lower limb | p value SD of X coordinates in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | P | ||||||||||||||||||||
| p value SD of Y coordinates in the right lower limb | p value SD of Y coordinates in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | P | ||||||||||||||||||||
| p value SD of Z coordinates in the right lower limb | p value SD of Z coordinates in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | P | ||||||||||||||||||||
| Red: p > 0.001; Green = p < 0.001. p = Plug-in Gait; H = Harrington | |||||||||||||||||||||
| p value range of X coordinates in the right lower limb | p value range of X coordinates in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | P | ||||||||||||||||||||
| p value range of Y coordinates in the right lower limb | p value range of Y coordinates in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | P | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| p value range of Z coordinates in the right lower limb | p value range of Z coordinates in the left lower limb | ||||||||||||||||||||
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | H | P | ||
| C1 | C1 | ||||||||||||||||||||
| C2 | C2 | ||||||||||||||||||||
| C3 | C3 | ||||||||||||||||||||
| C4 | C4 | ||||||||||||||||||||
| C5 | C5 | ||||||||||||||||||||
| C6 | C6 | ||||||||||||||||||||
| C7 | C7 | ||||||||||||||||||||
| C8 | C8 | ||||||||||||||||||||
| H | H | ||||||||||||||||||||
| P | P | ||||||||||||||||||||
| Red: p > 0.001; Green = p < 0.001. p = Plug-in Gait; H = Harrington | |||||||||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez, L.; Lalevée, M.; Poirier, T.; Brunel, H.; Matsoukis, J.; Van Driessche, S.; Billuart, F. Influence of Skin Marker Positioning and Their Combinations on Hip Joint Center Estimation Using the Functional Method. Bioengineering 2024, 11, 297. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering11030297
Martinez L, Lalevée M, Poirier T, Brunel H, Matsoukis J, Van Driessche S, Billuart F. Influence of Skin Marker Positioning and Their Combinations on Hip Joint Center Estimation Using the Functional Method. Bioengineering. 2024; 11(3):297. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering11030297
Chicago/Turabian StyleMartinez, Lucas, Matthieu Lalevée, Thomas Poirier, Helena Brunel, Jean Matsoukis, Stéphane Van Driessche, and Fabien Billuart. 2024. "Influence of Skin Marker Positioning and Their Combinations on Hip Joint Center Estimation Using the Functional Method" Bioengineering 11, no. 3: 297. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering11030297