
High-Resolution Imaging for the Analysis and Reconstruction of 3D Microenvironments for Regenerative Medicine: An Application-Focused Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
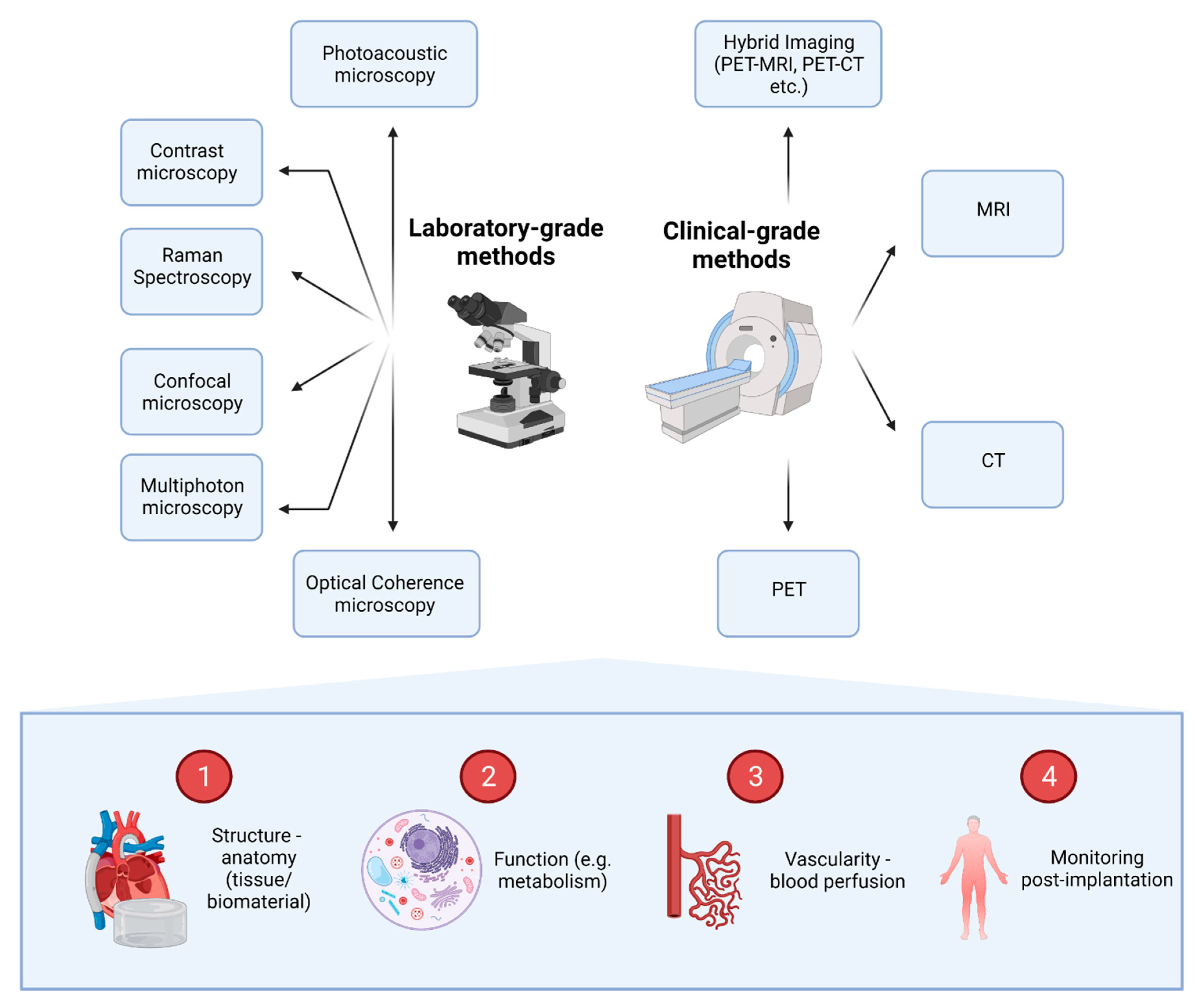
2. Overview of High-Resolution Imaging Techniques
2.1. Laboratory-Grade Methods
2.1.1. Contrast Microscopy
2.1.2. Confocal Microscopy
2.1.3. Multiphoton Microscopy
2.1.4. Optical Coherence Tomography
2.1.5. Photoacoustic Microscopy
2.1.6. Raman Spectroscopy
2.2. Clinical-Grade Methods
2.2.1. Computed Tomography (CT)
2.2.2. Magnetic Resonance Imaging (MRI)
2.2.3. PET and Hybrid Imaging
3. Tissue-Specific Applications
3.1. Cardiovascular Tissue Engineering
3.1.1. Engineered Heart Tissue Imaging
3.1.2. In Vivo Microscopy of the Heart
3.2. Musculoskeletal Tissue Engineering
3.2.1. Bone Tissue Engineering
3.2.2. Cartilage Tissue Engineering
3.3. Neural Tissue Engineering
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pigeot, S.; Klein, T.; Gullotta, F.; Dupard, S.J.; Garcia-Garcia, A.; García-García, A.; Prithiviraj, S.; Lorenzo, P.; Filippi, M.; Jaquiery, C.; et al. Manufacturing of human tissues as off-the-shelf grafts programmed to induce regeneration. Adv. Mater. 2021, 33, 2103737. [Google Scholar] [CrossRef] [PubMed]
- López-Martínez, S.; Rodríguez-Eguren, A.; de Miguel-Gómez, L.; Francés-Herrero, E.; Faus, E.; Díaz, A.; Ferrero, H.; Cervelló, I.; Pellicer, A. Bioengineered endometrial hydrogels with growth factors promote tissue regeneration and restore fertility in murine models. Acta Biomater. 2021, 135, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Kluzek, M.; Iuster, N.; Shimoni, E.; Kampf, N.; Klein, J. Cartilage-inspired, lipid-based boundary-lubricated hydrogels. Science 2020, 370, 335–338. [Google Scholar] [CrossRef]
- Wang, S.; Larina, I.V. High-Resolution Imaging Techniques in Tissue Engineering; Narayan, R.J., Ed.; Elsevier Ltd.: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Barthes, J.; Ozcelik, H.; Hindie, M.; Ndreu-Halil, A.; Hasan, A.; Vrana, N.E. Cell microenvironment engineering and monitoring for tissue engineering and regenerative medicine: The recent advances. BioMed Res. Int. 2014, 2014, 921905. [Google Scholar] [CrossRef] [PubMed]
- Klontzas, M.E.; Kakkos, G.A.; Papadakis, G.Z.; Marias, K.; Karantanas, A.H. Advanced clinical imaging for the evaluation of stem cell based therapies. Exp. Opin. Biol. Ther. 2021, 1253–1264. [Google Scholar] [CrossRef]
- Smith, L.E.; Smallwood, R.; Macneil, S. A comparison of imaging methodologies for 3D tissue engineering. Microsc. Res. Tech. 2010, 73, 1123–1133. [Google Scholar] [CrossRef]
- Popescu, G.; Park, Y.K.; Choi, W.; Dasari, R.R.; Feld, M.S.; Badizadegan, K. Imaging red blood cell dynamics by quantitative phase microscopy. Blood Cells Mol. Dis. 2008, 41, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Zhou, R.; Mir, M.; Sevket Derin, M.; Scott Carney, P.; Goddard, L.L.; Popescu, G. White-light diffraction tomography of unlabelled live cells. Nat. Photonics 2014, 8, 256–263. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.K.; Best, C.A.; Badizadegan, K.; Dasari, R.R.; Feld, M.S.; Kuriabova, T.; Kuriabova, M.L.; Levine, A.J.; Popescu, G. Measurement of red blood cell mechanics during morphological changes. Proc. Natl. Acad. Sci. USA 2010, 107, 6731–6736. [Google Scholar] [CrossRef] [Green Version]
- Gillette, B.M.; Rossen, N.S.; Das, N.; Leong, D.; Wang, M.; Dugar, A.; Sia, S.K. Engineering extracellular matrix structure in 3D multiphase tissues. Biomaterials 2011, 32, 8067–8076. [Google Scholar] [CrossRef] [Green Version]
- Pampaloni, F.; Reynaud, E.G.; Stelzer, E.H.K. The third dimension bridges the gap between cell culture and live tissue. Nat. Rev. Mol. Cell Biol. 2007, 8, 839–845. [Google Scholar] [CrossRef]
- Krahn, K.N.; Bouten, C.V.C.; Van Tuijl, S.; Van Zandvoort, M.A.M.J.; Merkx, M. Fluorescently labeled collagen binding proteins allow specific visualization of collagen in tissues and live cell culture. Anal. Biochem. 2006, 350, 177–185. [Google Scholar] [CrossRef]
- Sahoo, S.; Cho-Hong, J.G.; Siew-Lok, T. Development of hybrid polymer scaffolds for potential applications in ligament and tendon tissue engineering. Biomed. Mater. 2007, 2, 169–173. [Google Scholar] [CrossRef] [Green Version]
- Moon, J.J.; Saik, J.E.; Poché, R.A.; Leslie-Barbick, J.E.; Lee, M.-H.; Smith, A.A.; Dickinson, M.E.; West, J.L. Biomimetic hydrogels with pro-angiogenic properties. Biomaterials 2010, 31, 3840–3847. [Google Scholar] [CrossRef] [Green Version]
- Klontzas, M.E.; Reakasame, S.; Silva, R.; Morais, J.C.F.; Vernardis, S.; MacFarlane, R.J.; Heliotis, H.M.; Tsiridis, E.; Panoskaltsis, N.; Boccaccini, A.R.; et al. Oxidized alginate hydrogels with the GHK peptide enhance cord blood mesenchymal stem cell osteogenesis: A paradigm for metabolomics-based evaluation of biomaterial design. Acta Biomater. 2019, 88, 224–240. [Google Scholar] [CrossRef]
- Larson, A.M. Multiphoton microscopy. Nat. Photonics 2011, 5. [Google Scholar] [CrossRef]
- Palikaras, K.; Tavernarakis, N. Multiphoton Fluorescence Light Microscopy; John Wiley & Sons: Chichester, UK, 2012. [Google Scholar]
- Monici, M. Cell and tissue autofluorescence research and diagnostic applications. Biotechnol. Ann. Rev. 2005, 11, 227–256. [Google Scholar]
- Dittmar, R.; Potier, E.; Van Zandvoort, M.; Ito, K. Assessment of cell viability in three-dimensional scaffolds using cellular auto-fluorescence. Tissue Eng. Part C 2012, 18, 198–204. [Google Scholar] [CrossRef] [Green Version]
- Konig, K.; Schenke-Layland, K.; Riemann, I.; Stock, U.A. Multiphoton autofluorescence imaging of intratissue elastic fiber. Biomaterials 2005, 26, 495–500. [Google Scholar] [CrossRef]
- Campagnola, P. Second harmonic generation imaging microscopy: Applications to diseases diagnostics. Anal. Chem. 2011, 83, 3224–3231. [Google Scholar] [CrossRef] [Green Version]
- Akilbekova, D.; Bratlie, K.M. Quantitative characterization of collagen in the fibrotic capsule surrounding implanted polymeric microparticles through second harmonic generation imaging. PLoS ONE 2015, 10, e0130386. [Google Scholar] [CrossRef] [Green Version]
- Kabir, M.M.; Inavalli, V.V.G.K.; Lau, T.-Y.; Toussaint, K.C. Application of quantitative second-harmonic generation microscopy to dynamic conditions. Biomed. Opt. Exp. 2013, 4, 2546. [Google Scholar] [CrossRef] [Green Version]
- Raub, C.B.; Suresh, V.; Krasieva, T.; Lyubovitsky, J.; Mih, J.D.; Putnam, A.J.; Tromberg, B.J.; George, S.C. Noninvasive assessment of collagen gel microstructure and mechanics using multiphoton microscopy. Biophys. J. 2007, 92, 2212–2222. [Google Scholar] [CrossRef] [Green Version]
- Villa, M.M.; Wang, L.; Huang, J.; Rowe, D.W.; Wei, M. Visualizing osteogenesis in vivo within a cell-scaffold construct for bone tissue engineering using two-photon microscopy. Tissue Eng. Part C 2013, 19, 839–849. [Google Scholar] [CrossRef] [Green Version]
- Fujimoto, J.G.; Pitris, C.; Boppart, S.A.; Brezinski, M.E. Optical coherence tomography: An emerging technology for biomedical imaging and optical biopsy. Neoplasia 2000, 2, 9–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, X.; Graf, B.W.; Boppart, S.A. Imaging engineered tissues using structural and functional optical coherence tomography. J. Biophotonics 2009, 2, 643–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spoler, F.; Forst, M.; Marquardt, Y.; Hoeller, D.; Kurz, H.; Merk, H.; Abuzahra, F. High-resolution optical coherence tomography as a non-destructive monitoring tool for the engineering of skin equivalents. Skin Res. Technol. 2006, 12, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Yabushita, H.; Bouma, B.E.; Houser, S.L.; Thomas Aretz, H.; Jang, I.-K.; Schlendorf, K.H.; Kauffman, C.R.; Shishkov, M.; Kang, D.H.; Halpern, E.F.; et al. Characterization of human atherosclerosis by optical coherence tomography. Circulation 2002, 106, 1640–1645. [Google Scholar] [CrossRef]
- Tearney, G.J.; Brezinski, M.E.; Bouma, B.E.; Boppart, S.A.; Pitris, C.; Southern, J.F.; Fujimoto, J.G. In vivo endoscopic optical biopsy with optical coherence tomography. Science 1997, 276, 2037–2039. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, B.F.; Kennedy, K.M.; Sampson, D.D. A review of optical coherence elastography: Fundamentals, techniques and prospects. IEEE J. Sel. Top. Quantum Electron. 2014, 20, 272–288. [Google Scholar] [CrossRef]
- Ko, H.-J.; Tan, W.; Stack, R.; Boppart, S.A. Optical coherence elastography of engineered and developing tissue. Tissue Eng. 2006, 12, 63–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Singh, M.; Tran, T.T.; Leach, J.; Aglyamov, S.R.; Larina, I.V.; Martin, J.F.; Larin, K.V. Biomechanical assessment of myocardial infarction using optical coherence elastography. Biomed. Opt. Exp. 2018, 9, 728. [Google Scholar] [CrossRef]
- Veksler, B.; Kobzev, E.; Bonesi, M.; Meglinski, I. Application of optical coherence tomography for imaging of scaffold structure and micro-flows characterization. Laser Phys. Lett. 2008, 5, 236–239. [Google Scholar] [CrossRef]
- Mariampillai, A.; Standish, B.A.; Moriyama, E.H.; Khurana, M.; Munce, N.R.; Leung, M.K.K.; Jiang, J.; Cable, A.; Wilson, B.C.; Vitkin, A.; et al. Speckle variance detection of microvasculature using swept-source optical coherence tomography. Opt. Lett. 2008, 33, 1530. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.W.; Poché, R.A.; Saik, J.E.; Ali, S.; Wang, S.; Yosef, N.; Calderon, G.A.; Larry, S., Jr.; Vadakkan, T.G.; Larina, I.V.; et al. Improved angiogenesis in response to localized delivery of macrophage-recruiting molecules. PLoS ONE 2015, 10, e0131643. [Google Scholar] [CrossRef]
- Yao, J.; Wang, L.V. Photoacoustic microscopy. Laser Photonics Rev. 2012, 7, 758–778. [Google Scholar] [CrossRef]
- Zhang, Y.; Cai, X.; Choi, S.W.; Kim, C.; Wang, L.V.; Xia, Y. Chronic label-free volumetric photoacoustic microscopy of melanoma cells in three-dimensional porous scaffolds. Biomaterials 2010, 31, 8651–8658. [Google Scholar] [CrossRef] [Green Version]
- Cai, X.; Zhang, Y.; Li, L.; Choi, S.-W.; Matthew, R.M.; Yao, J.; Kim, C.; Xia, Y.; Wang, L.V. Investigation of neovascularization in three-dimensional porous scaffolds in vivo by a combination of multiscale photoacoustic microscopy and optical coherence tomography. Tissue Eng. Part C 2013, 19, 196–204. [Google Scholar] [CrossRef] [Green Version]
- Hu, S.; Wang, L.V. Optical-resolution photoacoustic microscopy: Auscultation of biological systems at the cellular level. Biophys. J. 2013, 105, 841–847. [Google Scholar] [CrossRef] [Green Version]
- Butler, H.J.; Ashton, L.; Bird, B.; Cinque, G.; Curtis, K.; Dorney, J.; Esmonde-White, K.; Fullwood, N.J.; Gardner, B.; Martin-Hirsch, P.L.; et al. Using Raman spectroscopy to characterize biological materials. Nat. Prot. 2016, 11, 664–687. [Google Scholar] [CrossRef] [Green Version]
- Swain, R.J.; Jell, G.; Stevens, M.M. Non-invasive analysis of cell cycle dynamics in single living cells with Raman micro-spectroscopy. J. Cell. Biochem. 2008, 104, 1427–1438. [Google Scholar] [CrossRef]
- Jell, G.; Notingher, I.; Tsigkou, O.; Notingher, P.; Polak, J.M.; Hench, L.L.; Stevens, M.M. Bioactive glass-induced osteoblast differentiation: A noninvasive spectroscopic study. J. Biomed. Mater. Res. Part A 2008, 86, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Perlaki, C.M.; Liu, Q.; Lim, M. Raman spectroscopy based techniques in tissue engineering-an overview. Appl. Spectrosc. Rev. 2014, 49, 513–532. [Google Scholar] [CrossRef]
- Bertoluzza, A.; Fagnano, C.; Tinti, A.; Morelli, M.A.; Tosi, M.R.; Maggi, G.; Marchetti, P.G. Raman and infrared spectroscopic study of the molecular characterization of the biocompatibility of prosthetic biomaterials. J. Raman Spectrosc. 1994, 25, 109–114. [Google Scholar] [CrossRef]
- Kunstar, A.; Leferink, A.M.; Okagbare, P.I.; Morris, M.D.; Roessler, B.J.; Otto, C.; Karperien, M.; van Blitterswijk, C.A.; Moroni, L.; van Apeldoorn, A.A. Label-free Raman monitoring of extracellular matrix formation in three-dimensional polymeric scaffolds. J. R. Soc. Interface 2013, 10, 20130464. [Google Scholar] [CrossRef]
- Klontzas, M.E.; Papadakis, G.Z.; Marias, K.; Karantanas, A.H. Musculoskeletal trauma imaging in the era of novel molecular methods and artificial intelligence. Injury 2020, 51, 2748–2756. [Google Scholar] [CrossRef]
- Klontzas, M.E.; Karantanas, A.H. MR imaging of artificial musculoskeletal tissues: Bridging the gap between basic science and clinical reality. Hell. J. Radiol. 2019, 5, 38–49. [Google Scholar]
- Zhu, N.; Chen, X.; Chapman, D. A brief review of visualization techniques for nerve tissue engineering applications. J. Biomim. Biomater. Tissue Eng. 2010, 7, 81–99. [Google Scholar] [CrossRef]
- Mendes, L.F.; Katagiri, H.; Tam, W.L.; Chai, Y.C.; Geris, L.; Roberts, S.J.; Luyten, F.P. Advancing osteochondral tissue engineering: Bone morphogenetic protein, transforming growth factor, and fibroblast growth factor signaling drive ordered differentiation of periosteal cells resulting in stable cartilage and bone formation in vivo. Stem Cell Res. Ther. 2018, 9, 42. [Google Scholar] [CrossRef]
- Karantanas, A.H. What’s new in the use of MRI in the orthopaedic trauma patient? Injury 2014, 45, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Rutland, J.W.; Delman, B.N.; Gill, C.M.; Zhu, C.; Shrivastava, R.K.; Balchandani, P. Emerging use of ultra-high-field 7T MRI in the study of intracranial vascularity: State of the field and future directions. AJNR Am. J. Neuroradiol. 2020, 41, 2–9. [Google Scholar] [CrossRef]
- Ladd, M.E.; Bachert, P.; Meyerspeer, M.; Moser, E.; Nagel, A.M.; Norris, D.G.; Schmitter, S.; Speck, O.; Straub, S.; Zaiss, M. Pros and cons of ultra-high-field MRI/MRS for human application. Prog. Nucl. Magn. Reson. Spectrosc. 2018, 109, 1–50. [Google Scholar] [CrossRef]
- Schaefer, P.W.; Grant, P.E.; Gonzalez, R.G. Diffusion-weighted MR imaging of the brain. Radiology 2000, 217, 331–345. [Google Scholar] [CrossRef]
- Tamura, M.; Unno, K.; Yonezawa, S.; Hattori, K.; Nakashima, E.; Tsukada, H.; Nakajima, M.; Oku, N. In vivo trafficking of endothelial progenitor cells their possible involvement in the tumor neovascularization. Life Sci. 2004, 75, 575–584. [Google Scholar] [CrossRef]
- Collignon, A.M.; Lesieur, J.; Anizan, N.; Azzouna, R.B.; Poliard, A.; Gorin, C.; Letourneur, D.; Chaussain, C.; Rouzet, F.; Rochefort, G.Y. Early angiogenesis detected by PET imaging with 64Cu-NODAGA-RGD is predictive of bone critical defect repair. Acta Biomater. 2018, 82, 111–121. [Google Scholar] [CrossRef]
- Tzatzalos, E.; Abilez, O.J.; Shukla, P.; Wu, J.C. Engineered heart tissues and induced pluripotent stem cells: Macro- and microstructures for disease modeling, drug screening, and translational studies. Adv. Drug Deliv. Rev. 2016, 96, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Stein, J.M.; Mummery, C.L.; Bellin, M. Engineered models of the human heart: Directions and challenges. Stem Cell Rep. 2021, 16, 2049–2057. [Google Scholar] [CrossRef] [PubMed]
- Van Meer, B.J.; Tertoolen, L.G.J.; Mummery, C.L. Concise review: Measuring physiological responses of human pluripotent stem cell derived cardiomyocytes to drugs and disease. Stem Cells 2016, 34, 2008–2015. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, W.H.; Melnychenko, I.; Wasmeier, G.; Didié, M.; Naito, H.; Nixdorff, U.; Hess, A.; Budinsky, L.; Brune, K.; Michaelis, B. Engineered heart tissue grafts improve systolic and diastolic function in infarcted rat hearts. Nat. Med. 2006, 12, 452–458. [Google Scholar] [CrossRef]
- Riegler, J.; Tiburcy, M.; Ebert, A.; Tzatzalos, E.; Raaz, U.; Abilez, O.J.; Shen, Q.; Kooreman, N.G.; Neofytou, E.; Chen, V.C.; et al. Human engineered heart muscles engraft and survive long term in a rodent myocardial infarction model. Circ. Res. 2015, 117, 720–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, X.; Riegler, J.; Tiburcy, M.; Zhao, X.; Chour, T.; Ndoye, B.; Nguyen, M.; Adams, J.; Ameen, M.; Denney, T.S., Jr.; et al. Magnetic resonance imaging of cardiac strain pattern following transplantation of human tissue engineered heart muscles. Circ. Cardiovasc. Imaging 2016, 9, e004731. [Google Scholar] [CrossRef] [Green Version]
- Vaghela, R.; Arkudas, A.; Horch, R.E.; Hessenauer, M. Actually seeing what is going on—Intravital microscopy in tissue engineering. Front. Eng. Biotechnol. 2021, 9, 627462. [Google Scholar] [CrossRef]
- Vinegoni, C.; Aguirre, A.D.; Lee, S.; Weissleder, R. Imaging the beating heart in the mouse using intravital microscopy techniques. Nat. Prot. 2015, 10, 1802–1819. [Google Scholar] [CrossRef] [Green Version]
- Aguirre, A.D.; Vinegoni, C.; Sebas, M.; Weissleder, R. Intravital imaging of cardiac function at the single-cell level. Proc. Natl. Acad. Sci. USA 2014, 111, 11257–11262. [Google Scholar] [CrossRef] [Green Version]
- Ueno, T.; Kim, P.; McGrath, M.M.; Yeung, M.Y.; Shimizu, T.; Jung, K.; Sayegh, H.; Chandraker, A.K.; Abdi, R.; Yun, S.H. Live images of donor dendritic cells trafficking Via CX3CR1 pathway. Front. Immunol. 2016, 7, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Witte, T.-M.; Fratila-Apachitei, L.E.; Zadpoor, A.A.; Peppas, N.A. Bone tissue engineering via growth factor delivery: From scaffolds to complex matrices. Regen. Biomater. 2018, 5, 197–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalande, C.; Miraux, S.; Derkaoui, S.M.; Mornet, S.; Bareille, R.; Fricain, J.C.; Franconi, J.M.; Visage, C.L.; Letourneur, D.; Amédée, J.; et al. Magnetic resonance imaging tracking of human adipose derived stromal cells within three-dimensional scaffolds for bone tissue engineering. Eur. Cells Mater. 2011, 21, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Klontzas, M.E.; Karantanas, A.H. Considerations on the use of ferumoxytol-enhanced MRI for tracking stem cell implants in cartilage defects. Radiology 2020, 294, 238–239. [Google Scholar] [CrossRef]
- Theruvath, A.J.; Nejadnik, H.; Lenkov, O.; Yerneni, K.; Li, K.; Kuntz, L.; Wolterman, C.; Tuebel, J.; Burgkart, R.; Liang, T.; et al. Tracking stem cell implants in cartilage defects of minipigs by using ferumoxytol-enhanced MRI. Radiology 2019, 292, 129–137. [Google Scholar] [CrossRef]
- Allenby, M.C.; Okutsu, N.; Brailey, K.; Guasch, J.; Zhang, Q.; Panoskaltsis, N.; Mantalaris, A. A spatiotemporal microenvironment model to improve design of a 3D bioreactor for red cell production. Tissue Eng. Part A 2021. [Google Scholar] [CrossRef]
- Ma, Y.J.; Jerban, S.; Jang, H.; Chang, D.; Chang, E.Y.; Du, J. Quantitative Ultrashort Echo Time (UTE) magnetic resonance imaging of bone: An update. Front. Endocrinol. 2020, 11, 567417. [Google Scholar] [CrossRef]
- Lin, E.; Alessio, A. What are the basic concepts of temporal, contrast, and spatial resolution in cardiac CT? J. Cardiovasc. Comput. Tomogr. 2009, 3, 403–408. [Google Scholar] [CrossRef] [Green Version]
- Subhawong, T.K.; Fishman, E.K.; Swart, J.E.; Carrino, J.A.; Attar, S.; Fayad, M. Soft-tissue masses and masslike conditions: What does CT add to diagnosis and management? AJR Am. J. Roentgenol. 2010, 194, 1559–1567. [Google Scholar] [CrossRef] [Green Version]
- Gaustad, J.V.; Brurberg, K.G.; Simonsen, T.G.; Mollatt, C.S.; Rofstad, E.K. Tumor vascularity assessed by magnetic resonance imaging and intravital microscopy imaging. Neoplasia 2008, 10, 354–362. [Google Scholar] [CrossRef] [Green Version]
- Naraghi, A.; White, L.M. MRI of labral and chondral lesions of the hip. AJR Am. J. Roentgenol. 2015, 205, 479–490. [Google Scholar] [CrossRef]
- Schmid, M.R.; Nötzli, H.P.; Zanetti, M.; Wyss, T.F.; Hodler, J. Cartilage lesions in the hip: Diagnostic effectiveness of MR arthrography. Radiology 2003, 226, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Jungmann, P.M.; Baum, T.; Bauer, J.S.; Karampinos, D.C.; Erdle, B.; Link, T.B.; Li, X.; Trattnig, S.; Rummeny, E.J.; Woertler, K. Cartilage repair surgery: Outcome evaluation by using noninvasive cartilage biomarkers based on quantitative MRI techniques? BioMed Res. Int. 2014, 2014, 840170. [Google Scholar] [CrossRef]
- Kondo, S.; Nakagawa, Y.; Mizuno, M.; Katagiri, K.; Tsuji, K.; Kiuchi, S.; Ono, H.; Muneta, T.; Koga, H.; Sekiya, I. Transplantation of aggregates of autologous synovial mesenchymal stem cells for treatment of cartilage defects in the femoral condyle and the femoral groove in microminipigs. Am. J. Sport Med. 2019, 47, 2338–2347. [Google Scholar] [CrossRef]
- Perdikakis, E.; Karachalios, T.; Katonis, P.; Karantanas, A. Comparison of MR-arthrography and MDCT-arthrography for detection of labral and articular cartilage hip pathology. Skelet. Radiol. 2011, 40, 1441–1447. [Google Scholar] [CrossRef]
- Doblado, L.R.; Martínez-Ramos, C.; Pradas, M.M. Biomaterials for neural tissue engineering. Front. Nanotechnol. 2021, 3, 643507. [Google Scholar] [CrossRef]
- Greve, F.; Frerker, S.; Bittermann, A.G.; Burkhardt, C.; Hierlemann, A.; Hall, H. Molecular design and characterization of the neuron-microelectrode array interface. Biomaterials 2007, 28, 5246–5258. [Google Scholar] [CrossRef]
- Lagali, N.; Griffith, M.; Fagerholm, P.; Merrett, K.; Huynh, M.; Munger, R. Innervation of tissue-engineered recombinant human collagen-based corneal substitutes: A comparative in vivo confocal microscopy study. Investig. Ophthalmol. Vis. Sci. 2008, 49, 3895–3902. [Google Scholar] [CrossRef]
- Bonse, U.; Busch, F. X-ray computed microtomography (μCT) using synchrotron radiation (SR). Prog. Biophys. Mol. Biol. 1996, 65, 133–169. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klontzas, M.E.; Protonotarios, A. High-Resolution Imaging for the Analysis and Reconstruction of 3D Microenvironments for Regenerative Medicine: An Application-Focused Review. Bioengineering 2021, 8, 182. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8110182
Klontzas ME, Protonotarios A. High-Resolution Imaging for the Analysis and Reconstruction of 3D Microenvironments for Regenerative Medicine: An Application-Focused Review. Bioengineering. 2021; 8(11):182. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8110182
Chicago/Turabian StyleKlontzas, Michail E., and Alexandros Protonotarios. 2021. "High-Resolution Imaging for the Analysis and Reconstruction of 3D Microenvironments for Regenerative Medicine: An Application-Focused Review" Bioengineering 8, no. 11: 182. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8110182