

Development of a CT-Compatible, Anthropomorphic Skull and Brain Phantom for Neurosurgical Planning, Training, and Simulation
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Phantom Requirements for Realistic Surgical Simulations
2.2. Computational Model
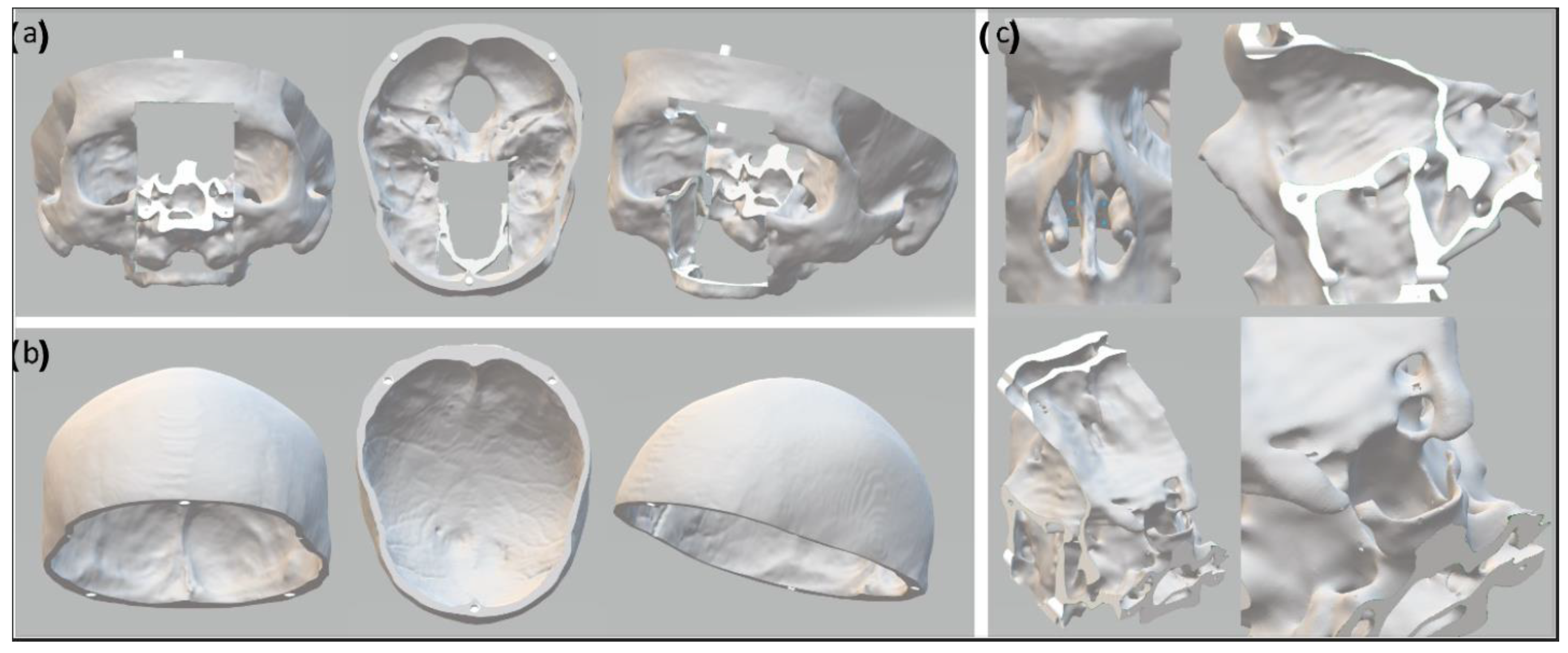
2.3. The Skull Phantom
2.4. The Brain Phantom
2.5. The Skull-Base Structures
2.6. Validation Step
3. Results
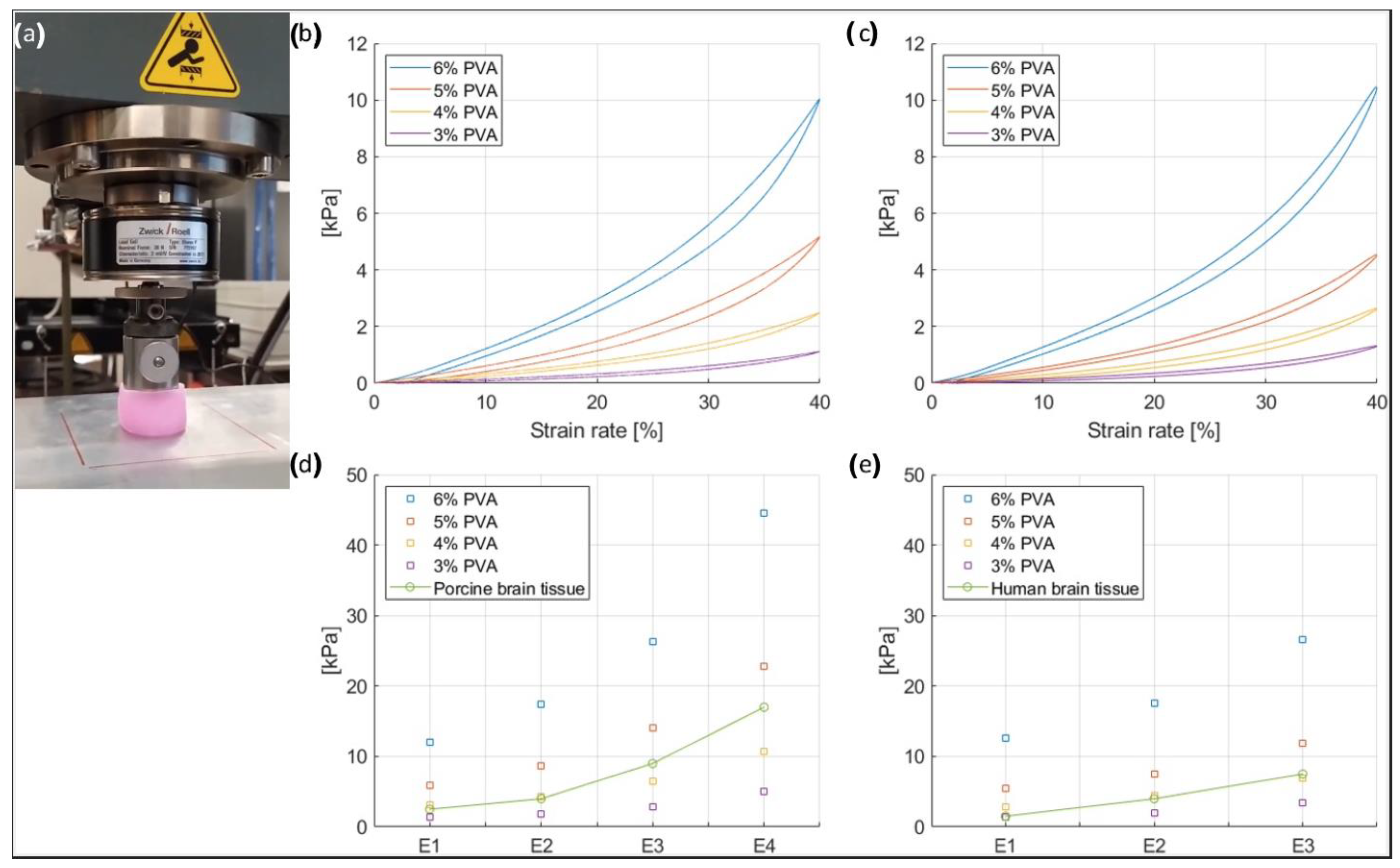
3.1. Mechanical Properties of the Brain Phantom
3.2. Radiodensity of the Skull and Brain Phantom
3.2.1. Radiodensity of the Skull Phantom
3.2.2. Radiodensity of the Brain Phantom
3.3. The Final Skull and Brain Phantom
3.4. Validation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Previous presentation
References
- Breimer, G.E.; Bodani, V.; Looi, T.; Drake, J.M. Design and evaluation of a new synthetic brain simulator for endoscopic third ventriculostomy. J. Neurosurg. Pediatr. 2015, 15, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Iop, A.; El-Hajj, V.G.; Gharios, M.; de Giorgio, A.; Monetti, F.M.; Edström, E.; Elmi-Terander, A.; Romero, M. Extended Reality in Neurosurgical Education: A Systematic Review. Sensors 2022, 22, 6067. [Google Scholar] [CrossRef] [PubMed]
- Lange, T.; Indelicato, D.J.; Rosen, J.M. Virtual Reality in Surgical Training. Surg. Oncol. Clin. N. Am. 2000, 9, 61–79. [Google Scholar] [CrossRef]
- Mirota, D.J.; Uneri, A.; Schafer, S.; Nithiananthan, S.; Reh, D.D.; Ishii, M.; Gallia, G.L.; Taylor, R.H.; Hager, G.D.; Siewerdsen, J.H. Evaluation of a System for High-Accuracy 3D Image-Based Registration of Endoscopic Video to C-Arm Cone-Beam CT for Image-Guided Skull Base Surgery. IEEE Trans. Med. Imaging 2013, 32, 1215–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibby, J.; Cvetko, S.; Javan, R.; Parr, R.; Gibby, W. Use of augmented reality for image-guided spine procedures. Eur. Spine J. 2020, 29, 1823–1832. [Google Scholar] [CrossRef]
- Chu, Y.; Yang, J.; Ma, S.; Ai, D.; Li, W.; Song, H.; Li, L.; Chen, D.; Chen, L.; Wang, Y. Registration and fusion quantification of augmented reality based nasal endoscopic surgery. Med. Image Anal. 2017, 42, 241–256. [Google Scholar] [CrossRef] [PubMed]
- Bong, J.H.; Song, H.-J.; Oh, Y.; Park, N.; Kim, H.; Park, S. Endoscopic navigation system with extended field of view using augmented reality technology. Int. J. Med. Robot. Comput. Assist. Surg. 2018, 14, e1886. [Google Scholar] [CrossRef]
- Nagassa, R.G.; McMenamin, P.G.; Adams, J.W.; Quayle, M.R.; Rosenfeld, J.V. Advanced 3D printed model of middle cerebral artery aneurysms for neurosurgery simulation. 3D Print. Med. 2019, 5, 11. [Google Scholar] [CrossRef] [Green Version]
- Govsa, F.; Yagdi, T.; Ozer, M.A.; Eraslan, C.; Alagoz, A.K. Building 3D anatomical model of coiling of the internal carotid artery derived from CT angiographic data. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Hussain, R.; Lalande, A.; Marroquin, R.; Guigou, C.; Grayeli, A.B. Video-based augmented reality combining CT-scan and instrument position data to microscope view in middle ear surgery. Sci. Rep. 2020, 10, 6767. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, V.; Narayanan, P.; Rajagopalan, R.; Karuppiah, R.; Rahman, Z.A.A.; Wormald, P.-J.; Van Hasselt, C.A.; Waran, V. Endoscopic skull base training using 3D printed models with pre-existing pathology. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Cuello, J.F.; Saenz, A.; Liñares, J.M.; Martinez, P.; Ruiz, C.; Argañaraz, R.; Bailez, M.M.; Mantese, B. Low-Cost Stereotactic Brain Biopsy Simulation Model. World Neurosurg. 2020, 138, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.K.; Shih, A.J. Multi-modality gellan gum-based tissue-mimicking phantom with targeted mechanical, electrical, and thermal properties. Phys. Med. Biol. 2013, 58, 5511–5525. [Google Scholar] [CrossRef]
- Lai, M.; Skyrman, S.; Kor, F.; Homan, R.; Babic, D.; Edström, E.; Persson, O.; Burström, G.; Elmi-Terander, A.; Hendriks, B.H.W.; et al. Development of a CT-compatible anthropomorphic skull phantom for surgical planning, training, and simulation. In Proceedings of the 2021 SPIE Medical Imaging, San Diego, CA, USA, 14–18 February 2021; Volume 11601, pp. 43–52. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, H.H.L.; Siewerdsen, J.H.; Vescan, A.; Daly, M.J.; Prisman, E.; Irish, J.C. 3D Rapid Prototyping for Otolaryngology—Head and Neck Surgery: Applications in Image-Guidance, Surgical Simulation and Patient-Specific Modeling. PLoS ONE 2015, 10, e0136370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, M.A.; Duchesneau, P.M.; MacIntyre, W.J. White and Gray Matter of the Brain Differentiated by Computed Tomography. Radiology 1977, 122, 699–702. [Google Scholar] [CrossRef]
- Li, Z.; Ji, C.; Li, D.; Luo, R.; Wang, G.; Jiang, J. A comprehensive study on the mechanical properties of different regions of 8-week-old pediatric porcine brain under tension, shear, and compression at various strain rates. J. Biomech. 2020, 98, 109380. [Google Scholar] [CrossRef]
- Forte, A.E.; Galvan, S.; Manieri, F.; Rodriguez y Baena, F.; Dini, D. A composite hydrogel for brain tissue phantoms. Mater. Des. 2016, 112, 227–238. [Google Scholar] [CrossRef] [Green Version]
- Skyrman, S.; Lai, M.; Edström, E.; Burström, G.; Förander, P.; Homan, R.; Kor, F.; Holthuizen, R.; Hendriks, B.H.W.; Persson, O.; et al. Augmented reality navigation for cranial biopsy and external ventricular drain insertion. Neurosurg. Focus 2021, 51, E7. [Google Scholar] [CrossRef]
- Dho, Y.-S.; Lee, D.; Ha, T.; Ji, S.Y.; Kim, K.M.; Kang, H.; Kim, M.-S.; Kim, J.W.; Cho, W.-S.; Kim, Y.H.; et al. Clinical application of patient-specific 3D printing brain tumor model production system for neurosurgery. Sci. Rep. 2021, 11, 7005. [Google Scholar] [CrossRef]
- Kunimatsu, A.; Kunimatsu, N. Skull Base Tumors and Tumor-Like Lesions: A Pictorial Review. Pol. J. Radiol. 2017, 82, 398–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almefty, K.; Pravdenkova, S.; Colli, B.O.; Al-Mefty, O.; Gokden, M. Chordoma and chondrosarcoma: Similar, but quite different, skull base tumors. Cancer 2007, 110, 2467–2477. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.W.; Lee, D.Y.; Pang, C.H.; Kim, J.E.; Park, C.-K.; Lee, D.; Park, S.J.; Cho, W.-S. Clinical application of 3D virtual and printed models for cerebrovascular diseases. Clin. Neurol. Neurosurg. 2021, 206, 106719. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.; Shan, C.; Babic, D.; Homan, R.; Terander, A.E.; Edstrom, E.; Persson, O.; Burstrom, G.; de With, P.H.N. Image fusion on the endoscopic view for endo-nasal skull-base surgery. In Proceedings of the 2019 SPIE Medical Imaging, San Diego, CA, USA, 8 March 2019; p. 48. [Google Scholar] [CrossRef]
- Lai, M.; Shan, C.; de With, P.H.N. Hand-eye camera calibration with an optical tracking system. In Proceedings of the 12th International Conference on Distributed Smart Cameras, Eindhoven, The Netherlands, 3–4 September 2018. [Google Scholar] [CrossRef]
- Lai, M.; Skyrman, S.; Shan, C.; Babic, D.; Homan, R.; Edström, E.; Persson, O.; Burström, G.; Elmi-Terander, A.; Hendriks, B.H.W.; et al. Fusion of augmented reality imaging with the endoscopic view for endonasal skull base surgery; a novel application for surgical navigation based on intraoperative cone beam computed tomography and optical tracking. PLoS ONE 2020, 15, e0227312. [Google Scholar] [CrossRef] [Green Version]
- Thiong’O, G.M.; Bernstein, M.; Drake, J.M. 3D printing in neurosurgery education: A review. 3D Print. Med. 2021, 7, 9. [Google Scholar] [CrossRef]
- Chawla, S.; Devi, S.; Calvachi, P.; Gormley, W.B.; Rueda-Esteban, R. Evaluation of simulation models in neurosurgical training according to face, content, and construct validity: A systematic review. Acta Neurochir. 2022, 164, 947–966. [Google Scholar] [CrossRef]
- Grillo, F.W.; Souza, V.H.; Matsuda, R.H.; Rondinoni, C.; Pavan, T.Z.; Baffa, O.; Machado, H.R.; Carneiro, A.A.O. Patient-specific neurosurgical phantom: Assessment of visual quality, accuracy, and scaling effects. 3D Print. Med. 2018, 4, 3. [Google Scholar] [CrossRef]
- Craven, C.; Baxter, D.; Cooke, M.; Carline, L.; Alberti, S.J.M.M.; Beard, J.; Murphy, M. Development of a modelled anatomical replica for training young neurosurgeons. Br. J. Neurosurg. 2014, 28, 707–712. [Google Scholar] [CrossRef]
- Waran, V.; Narayanan, V.; Karuppiah, R.; Owen, S.L.F.; Aziz, T. Utility of multimaterial 3D printers in creating models with pathological entities to enhance the training experience of neurosurgeons: Technical note. J. Neurosurg. 2014, 120, 489–492. [Google Scholar] [CrossRef]
- Saleh, Y.; Piper, R.; Richard, M.; Jeyaretna, S.; Cosker, T. Designing a 3D Printed Model of the Skull-Base: A Collaboration Between Clinicians and Industry. J. Med. Educ. Curric. Dev. 2022, 9, 238212052210807. [Google Scholar] [CrossRef]
- Guo, X.-Y.; He, Z.-Q.; Duan, H.; Lin, F.-H.; Zhang, G.-H.; Zhang, X.-H.; Chen, Z.-H.; Sai, K.; Jiang, X.-B.; Wang, Z.-N.; et al. The utility of 3-dimensional-printed models for skull base meningioma surgery. Ann. Transl. Med. 2020, 8, 370. [Google Scholar] [CrossRef] [PubMed]
- Levi, D.; Rampa, F.; Barbieri, C.; Pricca, P.; Franzini, A.; Pezzotta, S. True 3D reconstruction for planning of surgery on malformed skulls. Child’s Nerv. Syst. 2002, 18, 705–706. [Google Scholar] [CrossRef]
- Byvaltsev, V.; Polkin, R.; Bereznyak, D.; Giers, M.B.; Hernandez, P.A.; Shepelev, V.; Aliyev, M. 3D-printed cranial models simulating operative field depth for microvascular training in neurosurgery. Surg. Neurol. Int. 2021, 12, 213. [Google Scholar] [CrossRef] [PubMed]
- Mashiko, T.; Otani, K.; Kawano, R.; Konno, T.; Kaneko, N.; Ito, Y.; Watanabe, E. Development of Three-Dimensional Hollow Elastic Model for Cerebral Aneurysm Clipping Simulation Enabling Rapid and Low Cost Prototyping. World Neurosurg. 2015, 83, 351–361. [Google Scholar] [CrossRef]
- Liu, Y.; Gao, Q.; Du, S.; Chen, Z.; Fu, J.; Chen, B.; Liu, Z.; He, Y. Fabrication of cerebral aneurysm simulator with a desktop 3D printer. Sci. Rep. 2017, 7, srep44301. [Google Scholar] [CrossRef] [Green Version]
- Iida, H.; Hori, Y.; Ishida, K.; Imabayashi, E.; Matsuda, H.; Takahashi, M.; Maruno, H.; Yamamoto, A.; Koshino, K.; Enmi, J.; et al. Three-dimensional brain phantom containing bone and grey matter structures with a realistic head contour. Ann. Nucl. Med. 2012, 27, 25–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhuang, Y.-D.; Zhou, M.-C.; Liu, S.-C.; Wu, J.-F.; Wang, R.; Chen, C.-M. Effectiveness of personalized 3D printed models for patient education in degenerative lumbar disease. Patient Educ. Couns. 2019, 102, 1875–1881. [Google Scholar] [CrossRef]
- van de Belt, T.H.; Nijmeijer, H.; Grim, D.; Engelen, L.J.L.P.G.; Vreeken, R.; van Gelder, M.M.H.J.; ter Laan, M. Patient-Specific Actual-Size Three-Dimensional Printed Models for Patient Education in Glioma Treatment: First Experiences. World Neurosurg. 2018, 117, e99–e105. [Google Scholar] [CrossRef]
- Akkus, Z.; Galimzianova, A.; Hoogi, A.; Rubin, D.L.; Erickson, B.J. Deep Learning for Brain MRI Segmentation: State of the Art and Future Directions. J. Digit. Imaging 2017, 30, 449–459. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, M.; Skyrman, S.; Kor, F.; Homan, R.; El-Hajj, V.G.; Babic, D.; Edström, E.; Elmi-Terander, A.; Hendriks, B.H.W.; de With, P.H.N. Development of a CT-Compatible, Anthropomorphic Skull and Brain Phantom for Neurosurgical Planning, Training, and Simulation. Bioengineering 2022, 9, 537. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9100537
Lai M, Skyrman S, Kor F, Homan R, El-Hajj VG, Babic D, Edström E, Elmi-Terander A, Hendriks BHW, de With PHN. Development of a CT-Compatible, Anthropomorphic Skull and Brain Phantom for Neurosurgical Planning, Training, and Simulation. Bioengineering. 2022; 9(10):537. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9100537
Chicago/Turabian StyleLai, Marco, Simon Skyrman, Flip Kor, Robert Homan, Victor Gabriel El-Hajj, Drazenko Babic, Erik Edström, Adrian Elmi-Terander, Benno H. W. Hendriks, and Peter H. N. de With. 2022. "Development of a CT-Compatible, Anthropomorphic Skull and Brain Phantom for Neurosurgical Planning, Training, and Simulation" Bioengineering 9, no. 10: 537. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9100537