
Clinical Performance Evaluation of a Hyaluronic Acid Dental Gel for the Treatment of Traumatic Ulcers in Patients with Fixed Orthodontic Appliances: A Randomized Controlled Trial
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Settings
2.3. Study Population
- (1)
- aged between 6 and 18 years;
- (2)
- a malocclusion that necessitates the use of a fixed orthodontic appliance (rapid palatal expander, slow mandibular expander, partial fixed, traditional fixed one arch appliance, or both arches);
- (3)
- good general health (ASA status I);
- (4)
- patients with good oral health (FMPS and FMBS < 20%);
- (5)
- absence of caries;
- (6)
- periodontal health (absence of periodontal pockets > 4 mm with bleeding on probing, excluding a pseudopocket from the trade-in in progress);
- (7)
- patients and parents willing and able to cooperate in all aspects of the protocol;
- (8)
- written informed consent to treatment signed by parents (when underage) and participation in the clinical trial.
- (1)
- use of drugs that could interact with the wound healing process;
- (2)
- smokers;
- (3)
- previous history of diseases of the mucous membranes of the oral cavity, in particular, recurrent aphthous stomatitis, ulcers, bullous, or erosive diseases;
- (4)
- a history of skin or systemic diseases that may also have evidence in the oral cavity;
- (5)
- presence of oral ulcerations of unknown etiology, non-traumatic;
- (6)
- pregnancy and breastfeeding;
- (7)
- a history of hypersensitivity or allergy to the materials or drugs used in the study;
- (8)
- presence of auxiliary extraoral appliances, which could cause additional injuries during the treatment.
2.4. Intervention
2.5. Sample Size Calculation
2.5.1. Randomization (Random Number Generation, Allocation Concealment, and Implementation)
2.5.2. Blinding
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kvam, E.; Bondevik, O.; Gjerdet, N.R. Traumatic ulcers and pain in adults during orthodontic treatment. Community Dent. Oral Epidemiol. 1989, 17, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Kvam, E.; Gjerdet, N.R.; Bondevik, O. Traumatic ulcers and pain during orthodontic treatment. Community Dent. Oral Epidemiol. 1987, 15, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Shaw, W.C.; Addy, M.; Griffiths, S.; Price, C. Chlorhexidine and traumatic ulcers in orthodontic patients. Eur. J. Orthod. 1984, 6, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Baricevic, M.; Mravak-Stipetic, M.; Majstorovic, M.; Baranovic, M.; Baricevic, D.; Loncar, B. Oral mucosal lesions during orthodontic treatment. Int. J. Paediatr. Dent. 2011, 21, 96–102. [Google Scholar] [CrossRef]
- Kluemper, G.; Hiser, D.; Rayens, M.; Jay, M. Efficacy of a wax containing benzocaine in the relief of oral mucosal pain caused by orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 359–365. [Google Scholar] [CrossRef]
- Rennick, L.A.; Campbell, P.M.; Naidu, A.; Taylor, R.W.; Buschang, P.H. Effectiveness of a novel topical powder on the treatment of traumatic oral ulcers in orthodontic patients: A randomized controlled trial. Angle Orthod. 2016, 86, 351–357. [Google Scholar] [CrossRef] [Green Version]
- Leiva-Cala, C.; Lorenzo-Pouso, A.I.; Centenera-Centenera, B.; López-Palafox, J.; Gándara-Vila, P.; García-García, A.; Pérez-Sayáns, M. Clinical efficacy of an Aloe Vera gel versus a 0.12% chlorhexidine gel in preventing traumatic ulcers in patients with fixed orthodontic appliances: A double-blind randomized clinical trial. Odontology 2020, 108, 470–478. [Google Scholar] [CrossRef]
- Lee, M.; Han, S.H.; Choi, W.J.; Chung, K.H.; Lee, J.W. Hyaluronic acid dressing (Healoderm) in the treatment of diabetic foot ulcer: A prospective, randomized, placebo-controlled, single-center study. Wound Repair. Regen. 2016, 24, 581–588. [Google Scholar] [CrossRef]
- Casale, M.; Moffa, A.; Vella, P.; Rinaldi, V.; Lopez, M.A.; Grimaldi, V.; Salvinelli, F. Systematic review: The efficacy of topical hyaluronic acid on oral ulcers. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. 2), 63–69. [Google Scholar]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef]
- Shwethashree, M.; George, P.S.; Prakash, B.; Smitha, M.; Shabadi, N.; Murthy, M.N.; Gopi, A. Prevalence of oral diseases among school children of mysuru and chamarajanagar districts, Karnataka, India. Clin. Epidemiol. Glob. Health 2020, 8, 725–727. [Google Scholar] [CrossRef]
- Garala, K.; Joshi, P.; Shah, M.; Ramkishan, A.; Patel, J. Formulation and evaluation of periodontal in situ gel. Int. J. Pharm. Investig. 2013, 3, 29–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valentino, A.; Conte, R.; De Luca, I.; Di Cristo, F.; Peluso, G.; Bosetti, M.; Calarco, A. Thermo-Responsive Gel Containing Hydroxytyrosol-Chitosan Nanoparticles (Hyt@tgel) Counteracts the Increase of Osteoarthritis Biomarkers in Human Chondrocytes. Antioxidants 2022, 11, 1210. [Google Scholar] [CrossRef]
- AlHowaish, N.A.; AlSudani, D.I.; AlMuraikhi, N.A. Evaluation of a hyaluronic acid hydrogel (Restylane Lyft) as a scaffold for dental pulp regeneration in a regenerative endodontic organotype model. Odontology 2022, 110, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Olszewska-Czyz, I.; Kralik, K.; Tota, M.; Prpic, J. The Influence of Hyaluronic Acid Adjunctive Therapy of Periodontitis on Salivary Markers of Oxidative Stress: Randomized, Controlled Clinical Trial. Antioxidants 2022, 11, 135. [Google Scholar] [CrossRef]
- Eeckhout, C.; Ackerman, J.; Glibert, M.; Cosyn, J. A randomized controlled trial evaluating hyaluronic acid gel as wound healing agent in alveolar ridge preservation. J. Clin. Periodontol. 2022, 49, 280–291. [Google Scholar] [CrossRef]
- Nolan, A.; Badminton, J.; Maguire, J.; Seymour, R.A. The efficacy of topical hyaluronic acid in the management of oral lichen planus. J. Oral Pathol. Med. 2009, 38, 299–303. [Google Scholar] [CrossRef]
- Lee, J.H.; Jung, J.Y.; Bang, D. The efficacy of topical 0.2% hyaluronic acid gel on recurrent oral ulcers: Comparison between recurrent aphthous ulcers and the oral ulcers of Behçet’s disease. J. Eur. Acad. Dermatol Venereol. 2008, 22, 590–595. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Gizdulich, A.; Farronato, M.; Gupta, R.J.; Connelly, S.T. Electroporation technique for joint pain—Pilot feasibility study on TMD patients. Clin. Exp. Dent. Res. 2020, 6, 642–649. [Google Scholar] [CrossRef]
- Farronato, M.; Cossellu, G.; Farronato, G.; Inchingolo, F.; Blasi, S.; Angiero, F. Physico-chemical characterization of a smart thermo-responsive fluoride-releasing poloxamer-based gel. J. Biol. Regul. Homeost. Agents 2019, 33, 1309–1314. [Google Scholar]
- Touyz LZ, G.; Afrashtehfar, K.I. Implications of bisphosphonate calcium ion depletion interfering with desmosome epithelial seal in osseointegrated implants and pressure ulcers. Med. Hypotheses 2017, 107, 22–25. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Almomani, M.M.; Momani, M. Lack of association between dental implants and oral squamous cell carcinoma. Evid.-Based Dent. 2022, 23, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Höfling, K.; Fimmers, R.; Frentzen, M.; Jervøe-Storm, P.M. Clinical and microbiological effects of topical subgingival application of hyaluronic acid gel adjunctive to scaling and root planing in the treatment of chronic periodontitis. J. Periodontol. 2004, 75, 1114–1118. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, E.; Locarno, S.; Gallo, S.; Orsini, F.; Pini, C.; Farronato, M.; Thomaz, D.V.; Lenardi, C.; Piazzoni, M.; Tartaglia, G. Poloxamer-Based Hydrogel as Drug Delivery System: How Polymeric Excipients Influence the Chemical-Physical Properties. Polymers 2022, 14, 3624. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Baselli, G.; Baldini, B.; Favia, G.; Tartaglia, G.M. 3D Cephalometric Normality Range: Auto Contractive Maps (ACM) Analysis in Selected Caucasian Skeletal Class I Age Groups. Bioengineering 2022, 9, 216. [Google Scholar] [CrossRef]
- Farronato, M.; Maspero, C.; Abate, A.; Grippaudo, C.; Connelly, S.T.; Tartaglia, G.M. 3D cephalometry on reduced FOV CBCT: Skeletal class assessment through AF-BF on Frankfurt plane-validity and reliability through comparison with 2D measurements. Eur. Radiol. 2020, 30, 6295–6302. [Google Scholar] [CrossRef]
- Savadori, P.; Rai, P.M.; Tadakamadla, S.; Khijmatgar, S.; Inchingolo, F.; Greco, C.; Occhipinti, C.; Fahim, M.S.; Del Fabbro, M.; Tartaglia, G.M. Minor Recurrent Aphthous Ulcer Management with Hyaluronic Acid Gel in an Italian Cohort: A Double-Blind Randomized Clinical Trial. BioMed Res. Int. 2022, 2022, 7202831. [Google Scholar] [CrossRef]
- Ferrillo, M.; Nucci, L.; Giudice, A.; Calafiore, D.; Marotta, N.; Minervini, G.; d’Apuzzo, F.; Ammendolia, A.; Perillo, L.; de Sire, A. Efficacy of conservative approaches on pain relief in patients with temporomandibular joint disorders: A systematic review with network meta-analysis. Cranio J. Craniomandib. Pract. 2022, 1–17, advance online publication. [Google Scholar] [CrossRef]
- Ariel, H.; Kahn, A.; Hila, Z.O.; Anton, S.; Natan, G.; Kolerman, R. A thermosensitive gel with an active hyaluronic acid ingredient that contains an octenidine preservation system as an adjunct to scaling and root planning: A randomized prospective clinical study. Clin. Oral Investig. 2022, 26, 3721–3733. [Google Scholar] [CrossRef]
- DIPierro, F.; Bertuccioli, A.; Donato, G.; Spada, C. Retrospective analysis of the effects of a hyaluronic-based gum gel to counteract signs and symptoms of teething in infants. Minerva Pediatr. 2022, 74, 101–106. [Google Scholar] [CrossRef]
- Hassan, A.; Ahmed, E.; Ghalwash, D.; Elarab, A.E. Clinical Comparison of MEBO and Hyaluronic Acid Gel in the Management of Pain after Free Gingival Graft Harvesting: A Randomized Clinical Trial. Int. J. Dent. 2021, 2021, 2548665. [Google Scholar] [CrossRef] [PubMed]
- Canciani, E.; Sirello, R.; Pellegrini, G.; Henin, D.; Perrotta, M.; Toma, M.; Khomchyna, N.; Dellavia, C. Effects of Vitamin and Amino Acid-Enriched Hyaluronic Acid Gel on the Healing of Oral Mucosa: In Vivo and In Vitro Study. Medicina 2021, 57, 285. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Group | Control Group | ||
|---|---|---|---|
| Total number | n (%) | n (%) | |
| 35 | 35 | ||
| Gender | |||
| Female | 17 (48.6) | 16 (45.7) | |
| Male | 17 (48.6) | 19 (54.3) | |
| Not reported | 1 (2.9) | 0 (0.0) | |
| Site location | |||
| right hemipalate | 7 (20.0) | 2 (5.7) | |
| left hemipalate | 2 (5.7) | 5 (14.3) | |
| Right tongue | 0 (0.0) | 1 (2.9) | |
| Left tongue | 2 (5.7) | 0 (0.0) | |
| Right inner cheek mucosa | 9 (25.7) | 9 (25.7) | |
| Left inner cheek mucosa | 7 (20.0) | 8 (22.9) | |
| Right labial mucosa | 4 (11.4) | 5 (14.3) | |
| Left labial mucosa | 4 (11.4) | 5 (14.3) | |
| Color | |||
| White | 18 (51.4) | 16 (45.7) | |
| White-red | 3 (8.6) | 5(14.3) | |
| Red | 14 (40.0) | 14 (40.0) | |
| Surface | |||
| Endophyic | 17 (48.6) | 18 (51.4) | |
| Exo-endophytic | 6 (17.1) | 9 (25.7) | |
| Exophytic | 12 (34.3) | 8 (22.9) |
| Test Group | Control Group | |
|---|---|---|
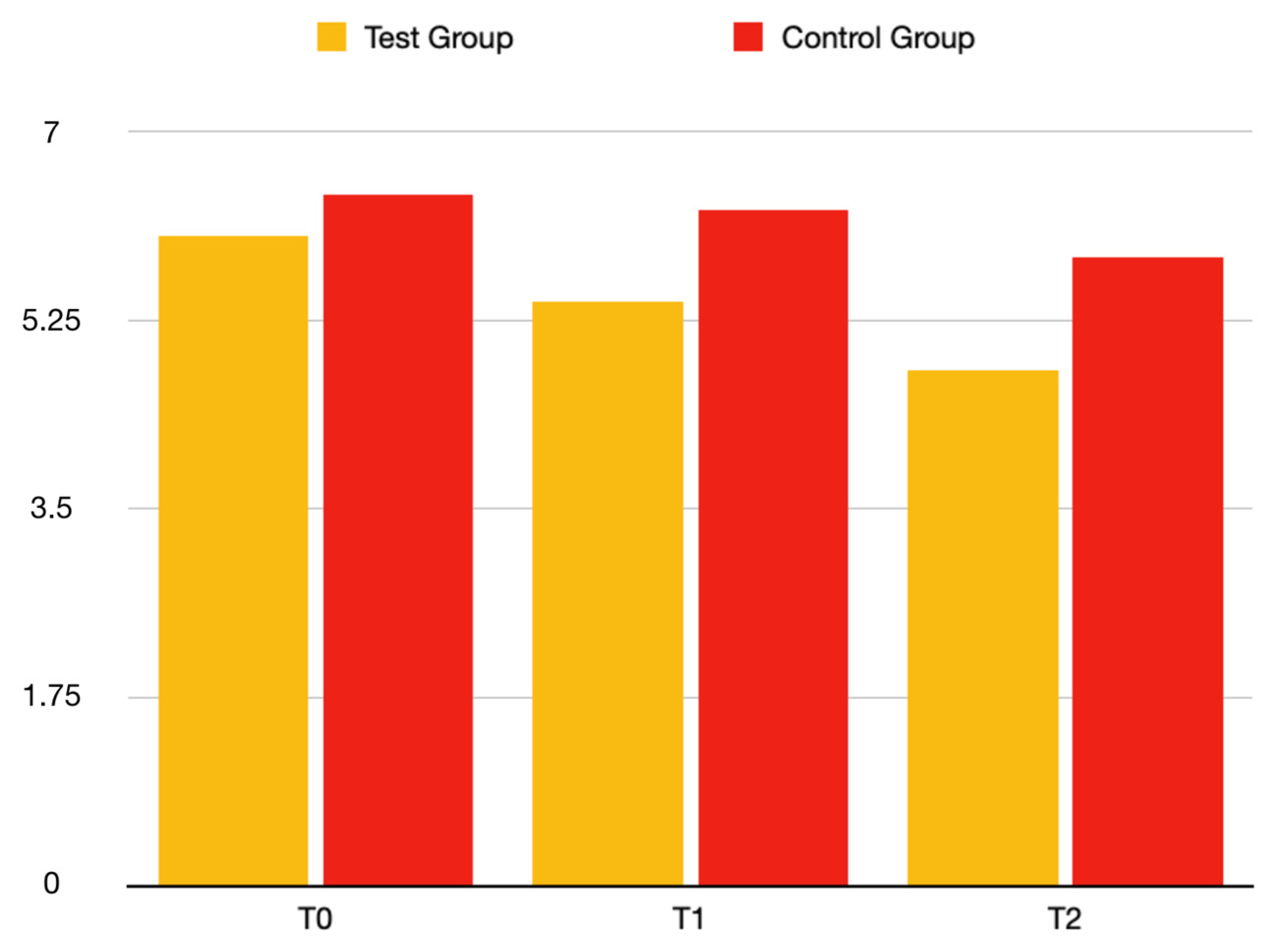
| VAS (T0) | ||
| Median (IQR) | 4.00 (4.00, 6.00) | 6.00 (4.00, 6.00) |
| Mean (SD) | 5.19 (1.39) | 5.40 (1.40) |
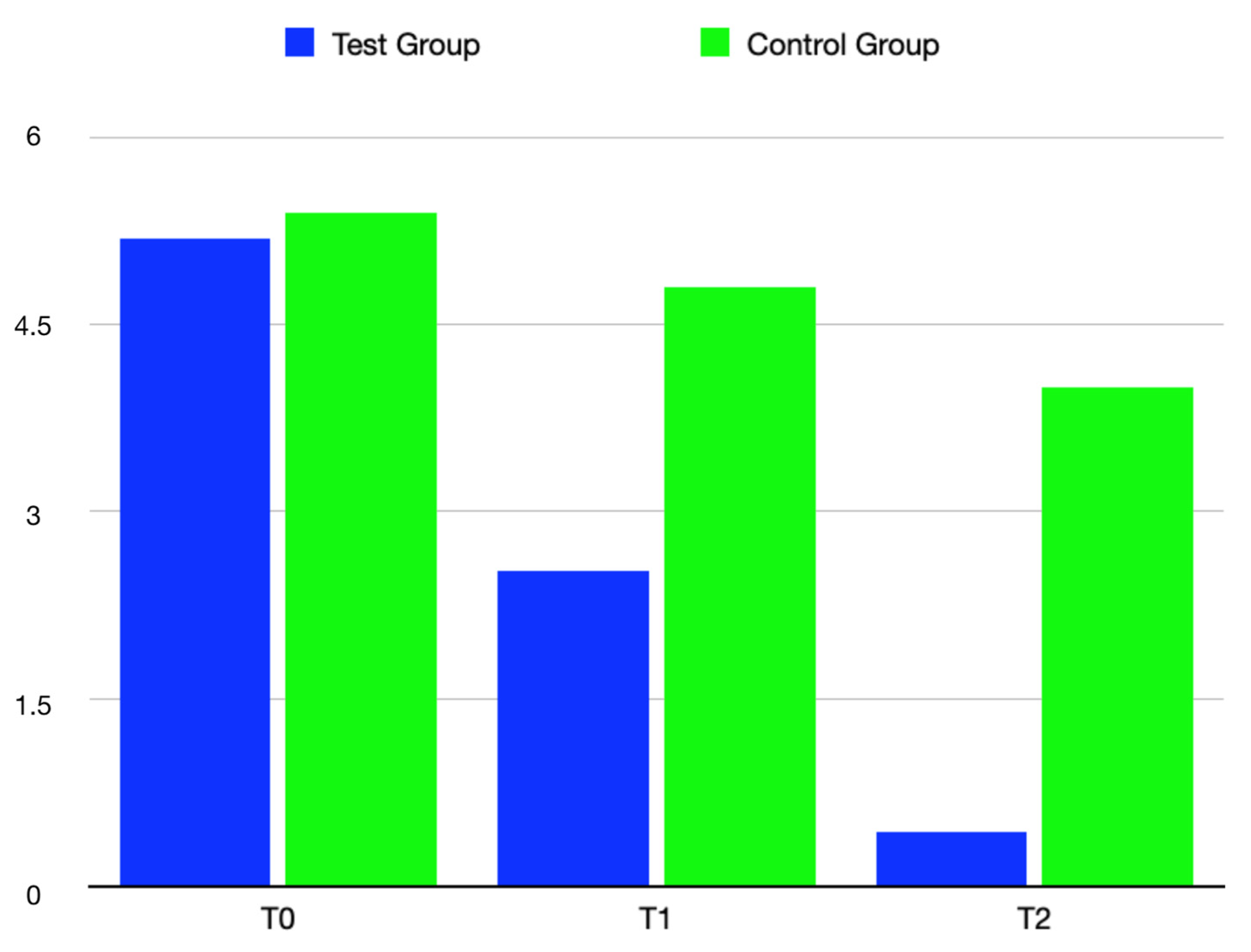
| Dimension (T0) | ||
| Median (IQR) | 6.00 (5.00, 7.00) | 6.00 (5.00, 8.00) |
| Mean (SD) | 6.03 (2.11) | 6.41 (2.17) |
| Test Group | Control Group | p Value | |
|---|---|---|---|
| VAS (T1) | >0.001 | ||
| Median (IQR) | 2.00 (2.00, 3.00) | 4.00 (4.00, 6.00) | |
| Mean (95% CI) | 2.52 (2.16–2.87) | 4.80 (4.33–5.26) | |
| VAS (T2) | >0.001 | ||
| Median (IQR) | 0.00 (0.00, 0.00) | 4.00 (2.00, 6.00) | |
| Mean (95% CI) | 0.44 (0.11–0.78) | 4.00 (3.35–4.65) | |
| Dimension (T1) | 0.1223 | ||
| Median (IQR) | 5.00 (4.25, 6.00) | 6.00 (4.50, 8.00) | |
| Mean (95% CI) | 5.43 (4.69–6.16) | 6.27 (5.49–7.05) | |
| Dimension (T2) | 0.03199 | ||
| Median (IQR) | 4.50 (3.50, 5.50) | 6.00 (4.50, 8.00) | |
| Mean (95% CI) | 4.78 (4.09–5.46) | 5.83 (5.08–6.59) |
| Test Group | Control Group | p Value | |
|---|---|---|---|
| VAS (T1) | >0.001 | ||
| Median (IQR) | 2.00 (2.00, 3.00) | 4.00 (4.00, 6.00) | |
| Mean (95% CI) | 2.52 (2.16–2.87) | 4.80 (4.33–5.26) | |
| VAS (T2) | >0.001 | ||
| Median (IQR) | 0.00 (0.00, 0.00) | 4.00 (2.00, 6.00) | |
| Mean (95% CI) | 0.44 (0.11–0.78) | 4.00 (3.35–4.65) | |
| Dimension (T1) | 0.1223 | ||
| Median (Iqr) | 5.00 (4.25, 6.00) | 6.00 (4.50, 8.00) | |
| Mean (95% Ci) | 5.43 (4.69–6.16) | 6.27 (5.49–7.05) | |
| Dimension (T2) | 0.03199 | ||
| Median (Iqr) | 4.50 (3.50, 5.50) | 6.00 (4.50, 8.00) | |
| Mean (95% Ci) | 4.78 (4.09–5.46) | 5.83 (5.08–6.59) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tremolati, M.; Farronato, M.; Ferrantino, L.; Rusconi, F.; Lodi, G.; Maspero, C. Clinical Performance Evaluation of a Hyaluronic Acid Dental Gel for the Treatment of Traumatic Ulcers in Patients with Fixed Orthodontic Appliances: A Randomized Controlled Trial. Bioengineering 2022, 9, 761. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9120761
Tremolati M, Farronato M, Ferrantino L, Rusconi F, Lodi G, Maspero C. Clinical Performance Evaluation of a Hyaluronic Acid Dental Gel for the Treatment of Traumatic Ulcers in Patients with Fixed Orthodontic Appliances: A Randomized Controlled Trial. Bioengineering. 2022; 9(12):761. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9120761
Chicago/Turabian StyleTremolati, Marco, Marco Farronato, Luca Ferrantino, Francesca Rusconi, Giovanni Lodi, and Cinzia Maspero. 2022. "Clinical Performance Evaluation of a Hyaluronic Acid Dental Gel for the Treatment of Traumatic Ulcers in Patients with Fixed Orthodontic Appliances: A Randomized Controlled Trial" Bioengineering 9, no. 12: 761. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9120761