3. Results
Descriptive statistics were used by calculating the average for data treatment. The relationship between the independent variable (thickness and infill) and the radiation transmission was further evaluated through simple linear regression.
3.1. Dosimetric Properties
The results of transmitted radiation, in %, are shown in
Table 3. To observe the trend between different parameters such as energy, infill and thickness for each plate, the graphs in
Figure 6,
Figure 7 and
Figure 8 were generated.
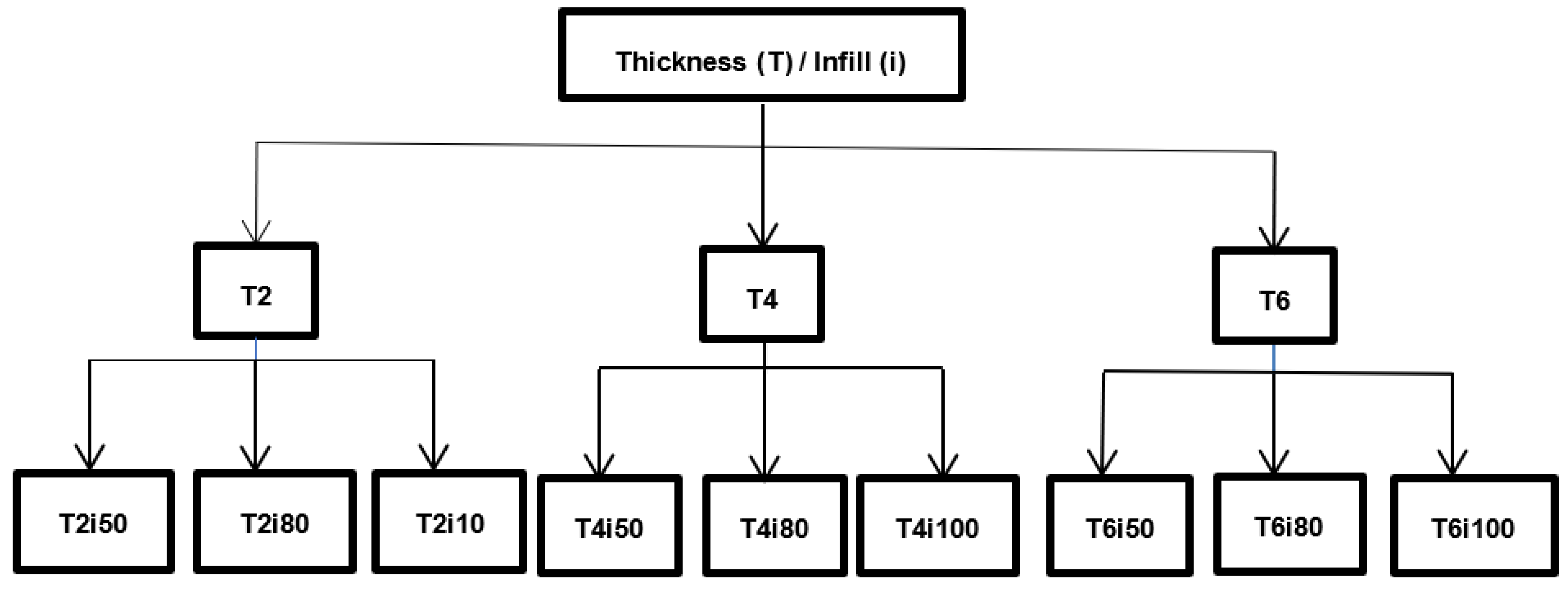
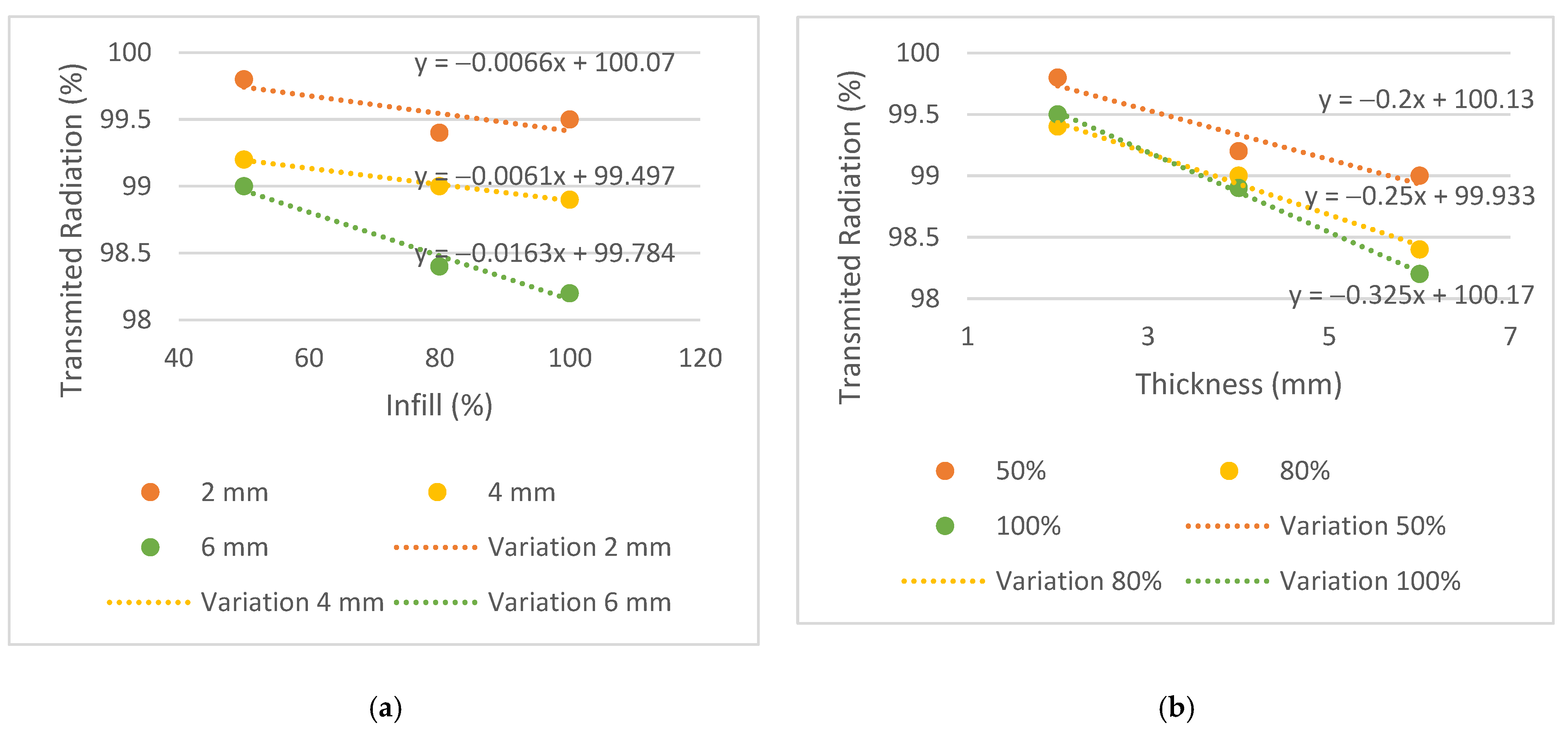
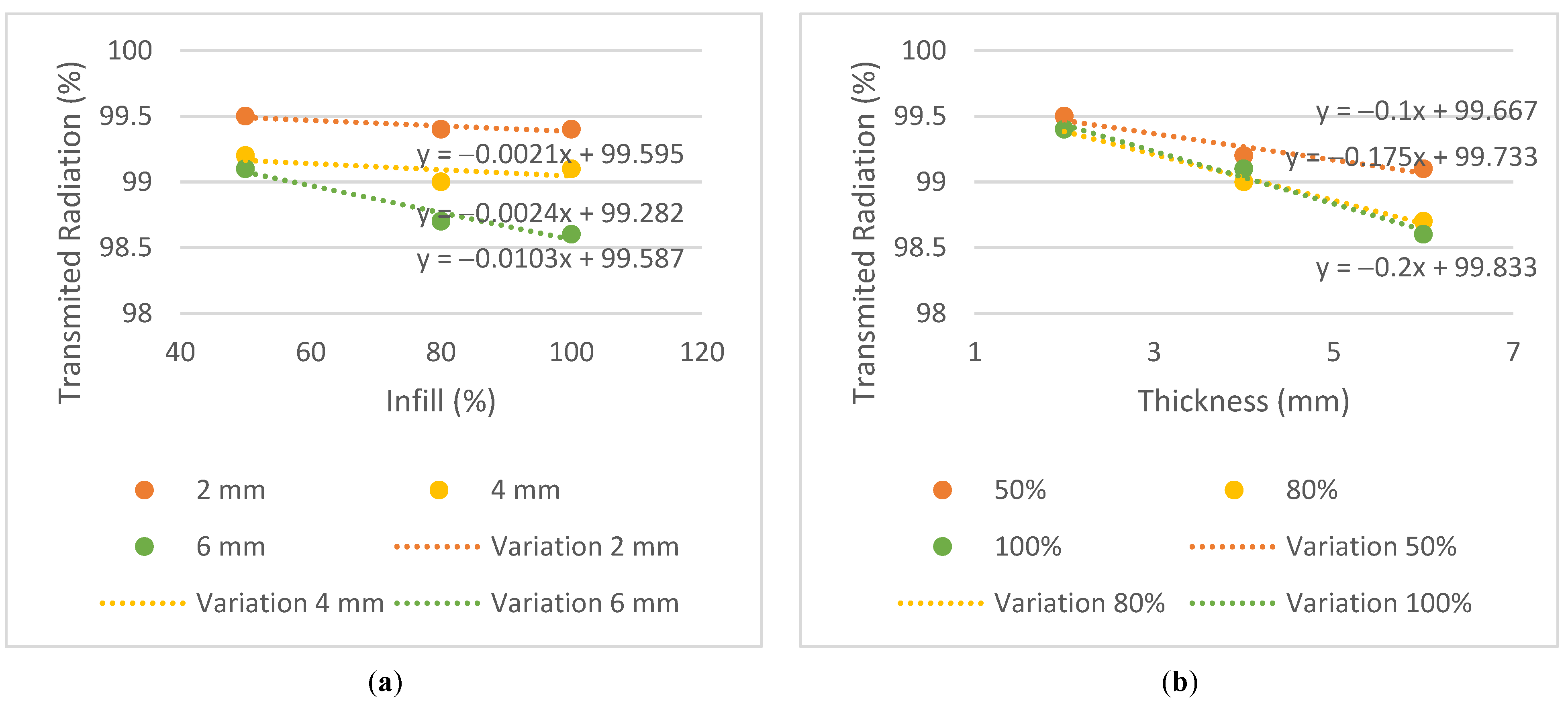
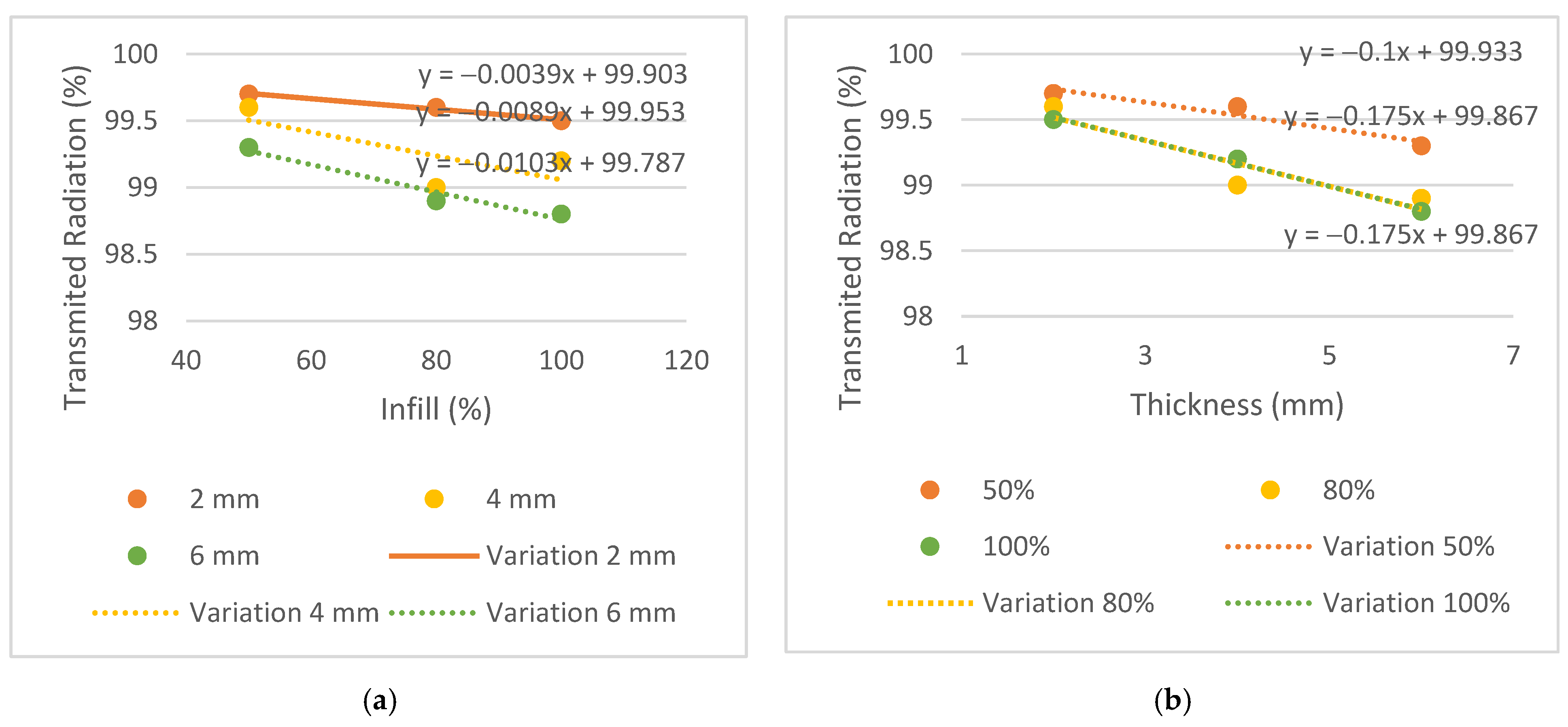
Similar behaviors were considered when the difference between the transmission obtained in the plates and the conventional mask was equal to or less than 0.3%. The 2 mm thick plates and the T4i50 plate showed equivalent dose transmissions to the conventional mask in all energies. The T2i50 plate showed equal or better results than others, especially for the energy of 6 MV, which had a lower attenuation compared to the conventional mask, in the amount of 0.2% vs. 0.6%. This means that the T2i50 sample presents dosimetric characteristics similar to those of conventional masks. It is possible to observe an increase in dose transmission with the increase in energy since a greater penetration capacity and dose deposition in the material at a greater depth revealed a greater transmission to 6 MV energy, except for the T2i50 plate. In addition, unusual behavior was observed for the T4i80 plate, which revealed 99% radiation transmission in all energies. These exceptions may be essentially due to some statistical fluctuations, since the differences between readings are minimal, with an order of magnitude close to the accuracy of the measuring equipment itself. In fact, for smaller thicknesses, the transmission is very high and almost independent of the energy itself, so the uncertainty of the measurement itself can generate these particularities in the analysis of the results (without real physical significance). By analyzing the slope on the transmission variation graphs, it is possible to observe a greater decrease in the thickness graphs compared to the infill graphs—observing the 6 MV graphs, the slopes of the trend lines for thickness are −0.2, −0.25 and −0.325, compared to −0.0066, −0.0061 and −0.0163 for infill. This may indicate that the increase in thickness has a greater impact on the attenuation of radiation than the increase in the infill. In conclusion, despite the 2 mm thick plates and the T4i50 plate showing radio transparency within the acceptable limit, the T2i50 plate showed better results than the conventional mask. This is because it contains less material than the other plates and hence, fewer attenuating factors for radiation.
3.2. Mechanical Properties
For most thermoplastic masks, deviations between 2 and 5 mm are accepted [
5]. The results of the mechanical simulations performed in the plate models are shown in
Table 4.
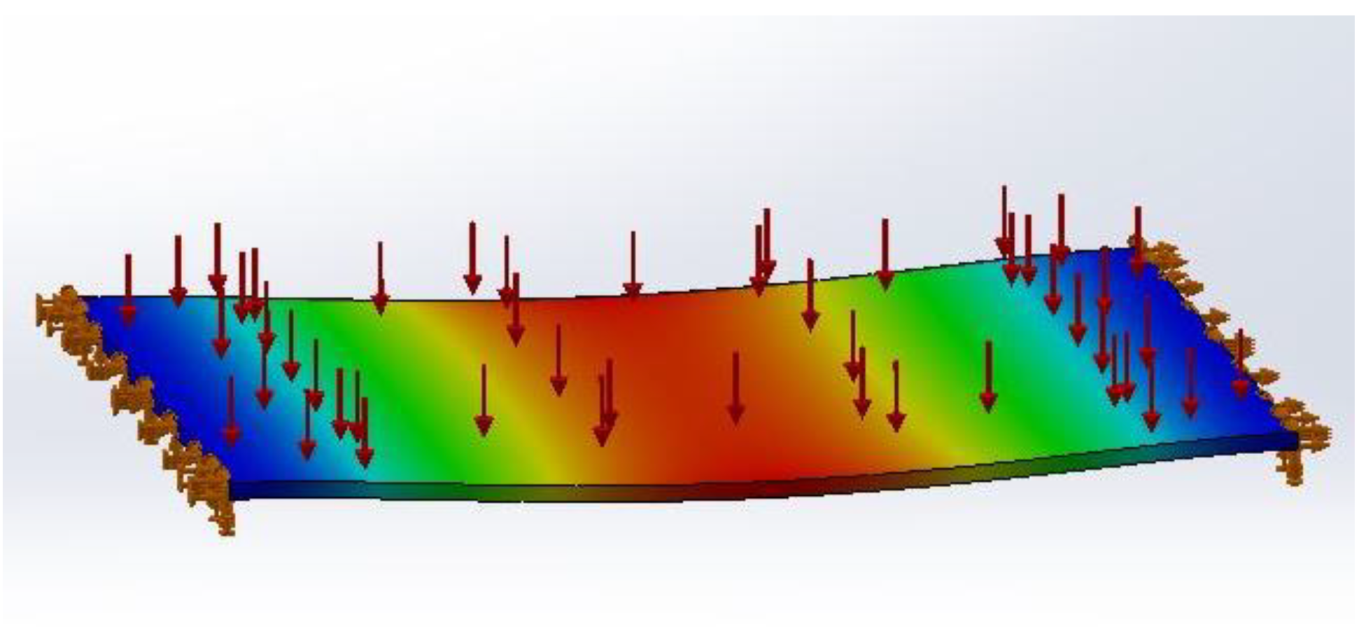
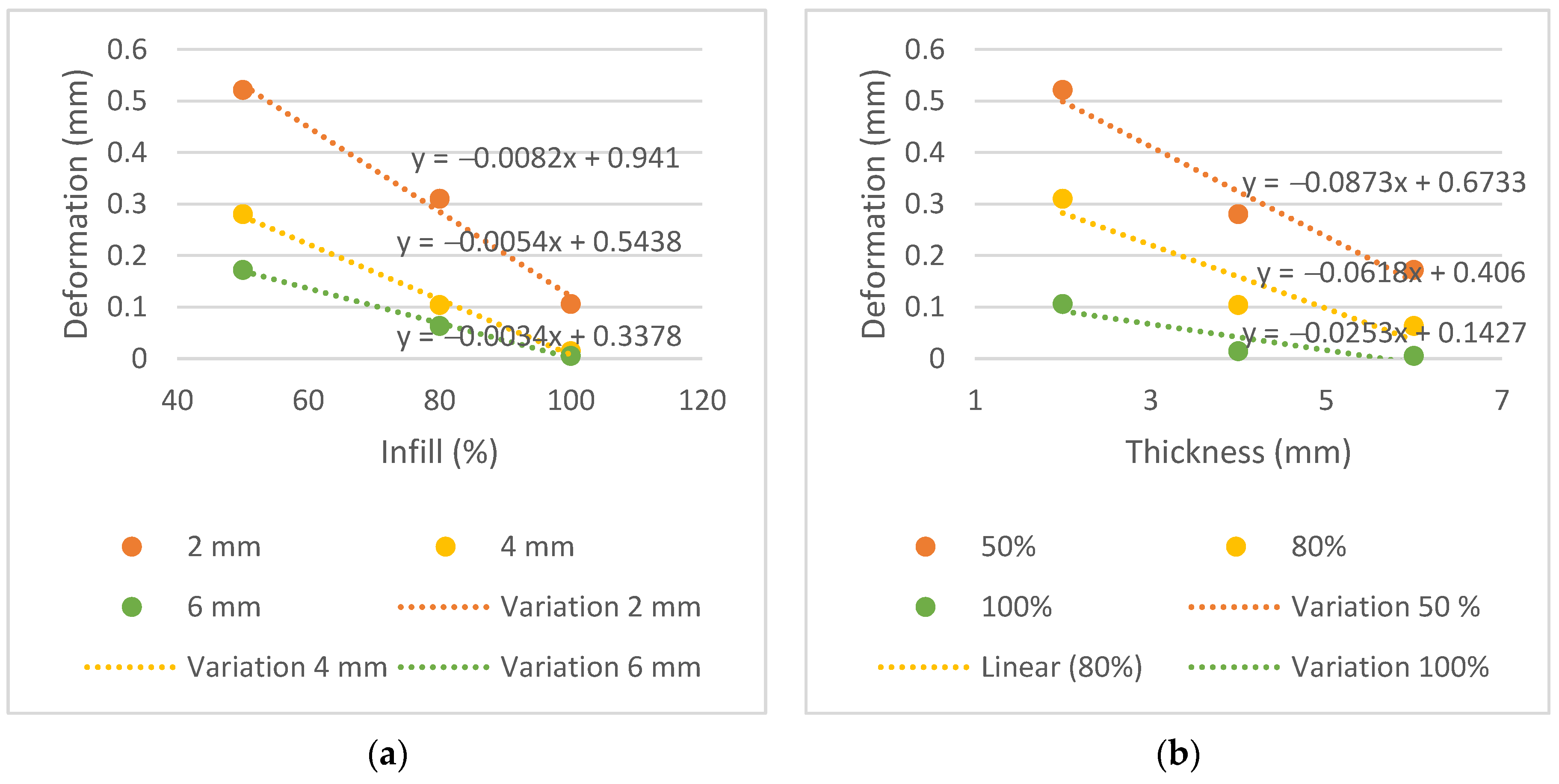
The displacement, in mm, did not exceed 0.521 mm in all samples. This proved to be a very positive result and below the above-mentioned range of 2 mm to 5 mm. The measurements of displacement variation in function of thickness and infill are shown in
Figure 9.
Analyzing the displacement variation graphs and the slope of the trend line, it is possible to observe a greater decrease in the thickness graphs than the infill graphs, similar to the transmission graphs. Steeper slopes are observed in the trend lines for thickness, −0.0873, −0.0618 and −0.0253, compared to −0.0082, −0.0054 and −0.0034 for infill. This indicates that the thickness parameter affects the mechanical performance more than the infill does.
3.3. Financial Properties
Table 5 shows the time results, in hours, and the masses, in grams, for the 3D printing of the mask in four parts.
Table 6 shows the costs and hours spent on printing an immobilization mask vs. molding a conventional mask.
Durations were estimated from average times obtained in typical clinical situations. Labour costs were calculated taking into account the average salary in Portugal in 2019, per hour, of a diagnostic and therapeutic technician [
25]. The typical variation in the cost of a conventional mask reported by the hospital was assumed to be between EUR 40 and 60. A total time of 47 h and 32 min was needed to print the full mask (equivalent to 2.852 min). The PLA coil (BQ, 1.75 mm) used was 1 kg and had a cost of EUR 20.00, but coils can vary between EUR 10 and 30. With this, the manufactured mask had a weight of 139.02 g, which means that, depending on the price of the purchased coil, between EUR 1.39 and 4.17 worth of PLA can be spent printing the mask. Normally, the time spent by the HCP making a conventional mask is about 10 min. In contrast, the time spent by a healthcare professional on the new process was significantly longer—46 min—determined mainly by the processing time and optimization of the mesh (not considering the time the mask was being printed, as it does not require human intervention). Proportionally, the labour cost in the conventional process is EUR 1.17 vs. EUR 5.52 for the proposed 3D printing process, representing an increase of about 472%. However, the reduction in material resources offers a significant reduction in cost—between 93% and 97%—since the price of a conventional mask varies between EUR 40 and 60 (depending on the manufacturer) and the amount of PLA spent on the 3D-printed mask varies between EUR 1.39 and 4.17. Furthermore, three-dimensional printing technology can reduce the time the CT scanner is occupied by the same patient since the patient only needs to be lying down in the first phase of the scanning with the optical sensor for 5 min vs. 10 min in the conventional process. This creates a strong benefit for both the healthcare facility and the patient as it reduces the time needed to lie down in a particularly uncomfortable position by about 50%, increasing the availability of the CT scanner to perform other procedures and thus optimizing its profitability for the health institution.
Table 7 shows the cost analysis associated with 3D printing an immobilization mask with 50% infill and weighing 139.02 g (the total printing time was 47 h and 32 min).
The analysis was performed considering the parameters of a hospital in the Lisbon region, in terms of material costs. All information was provided by the RT department. In this case, an average of 800 patients are treated per year, and it is estimated that 40% need immobilization masks for the treatment. This translates to about 320 masks per year. As the cost of a mask can vary between EUR 40 and 60, between EUR 12,800 and 19,200 are spent per year on masks alone (not including labour costs or expenses with the hot water tank).
As previously mentioned, the costs were extrapolated in a case where the mask could be printed on a larger-scale printer and therefore printed in one run. The initial investment required to implement this technology is around EUR 1000 for the scanner and EUR 1000–3000 for the printer. However, different materials than those used in this study can be used to obtain the same workflow, particularly, less expensive scanners, from EUR 200 to 1000. The PLA coil (BQ, 1.75 mm) used weighed 1 kg and had a cost of EUR 20.00. This implies that the manufactured mask weighed 139.02 g, meaning that EUR 2.78 worth of PLA was spent 3D printing it. Similarly, it is possible to verify that a 1 kg coil can essentially generate 7.18 masks—this may vary with the volume of each patient. Maintenance costs were calculated assuming they would be around 10% of the total cost of the printer per year. Regarding electricity, consumption in kWh and average power were estimated from average data obtained in the national population in 2019. Hence, the cost of printing an immobilization mask using 3D printing technology can cost between EUR 8.41 and 15.54. Considering a workflow of 320 patients per year who require such masks, it is possible to estimate the cost of the service at around EUR 2691–4973 per year compared to the EUR 12,800–19,200 currently spent on the service (disregarding the costs with labour and with the hot water tank), providing cost savings in material resources at around 75–80%.
A comparison of the final costs—material costs plus labour costs—between the conventional method and the proposed automated process is shown in
Table 8.
The calculated labour costs are regarding the sum of the costs in the different phases of the healthcare professional’s intervention, shown in
Table 6, multiplied by the number of masks that would have to be made per year—in this case, 320 masks. It is possible to observe a sharp decrease in the final costs—from EUR 13,174–19,574 to EUR 4457–6739, about 66% less.
4. Discussion
The most appropriate immobilization method is one that ensures a comfortable positioning of the patient while ensuring effective immobilization without affecting radiation beam quality [
5]. Radiotherapy continues to introduce new technologies into the workflow, namely devices from other fields of science, such as surface scanners and 3D printers [
26]. Recent advances in the field of 3D technology have been introducing new processes that make it possible to use a variety of materials [
11]. The present work intended to emphasize the importance of thermoplastic masks’ automation manufacturing process using 3D printing, providing a global view of the suggested technology.
To achieve the first specific purpose—to evaluate whether the PLA has a dosimetric behavior comparable to conventional immobilization masks—the dose measured by the ionization chamber was compared with the doses measured in a conventional mask. The expected results for radiation transmission consisted of increasing radiation with increasing energy since higher energy has a higher radiation penetration capacity, and reducing transmission with increasing thickness and infill, thus increasing the difficulty for the beam to pass through each sample.
The conventional mask had a thickness of 2 mm and showed results comparable to plates T2i50, T2i80 and T2i100, and similar radiological behavior was found in the PLA. Moreover, the T4i50 plate showed a similar behavior due to its 50% infill, supporting the conclusion that despite the doubling the thickness, dose transmission remained within acceptable parameters for all three energies.
Dancewicz et al. [
13] determined that a 3 mm, 50% infill PLA sample, when irradiated with megavoltage photons, reveals a radiological density (determined by the Hounsfield scale) of −388 HU. This result shows that PLA with 50% infill has a very low radiological density—close to lung density—allowing us to infer its high radiolucency capacity.
Immobilization device influence on dosimetry must be taken into account. Considering that beam attenuation is automatically neglected in CT-based treatment planning, the potential bolus effect of the mask material by increasing the skin surface or dose has additional implications. With the use of thermoluminescence dosimeters (TLD), Haefner et al. [
5] revealed an increase in the surface dose of up to 18% for thermoplastic material of 3 mm thickness. As a result, the mask system presented in this study can limit skin toxicity due to a thickness of only 2 mm and its potential to create additional personalized cuts. Since conventional masks are stretched at certain points, it is expected that by reducing thickness, the transmission will be slightly higher in some regions of the masks. Although smaller thickness samples are possible to print to obtain this comparison, it is only possible to extract concrete results with the fully printed mask irradiation vs. with a conventional stretched mask.
From the analysis of
Table 4 and
Figure 9, with a maximum displacement of 0.521 mm, it is possible to conclude that PLA provides sufficient stiffness to minimize material deformation when a reference pressure is applied; this relates to the second specific purpose of this study. It is expected that deformation will decrease with increasing thickness and infill of the samples due to the increase in the material in each plate. The plate with the greatest mechanical strength is the T6i100 plate, with a maximum displacement of 0.005 mm. Since the limit stipulated for the difference in the radiation transmission in the plates and the conventional mask is equal to or less than 0.3%, this plate could not be considered for printing due to the higher difference in the transmission (−1.2%, −0.9%, −0.9% for the energies of 6, 10 and 15 MV, respectively).
In summary, PLA proved to be an appropriate material to integrate an immobilization mask. However, Fernandes [
27] states that several factors may influence analysis of the mechanical characteristics of PLA: infill density, extrusion temperature, infill orientation, layer thickness and even filament color. Therefore, the printed mask itself must be subjected to mechanical tests for a more reliable property test and to obtain the actual displacement. For this reason, T2i50 plate characteristics were chosen to compose the mask, as it demonstrated positive results in terms of radiation transmission and within the resistance limit of an immobilization mask, with a displacement of 0.521 mm.
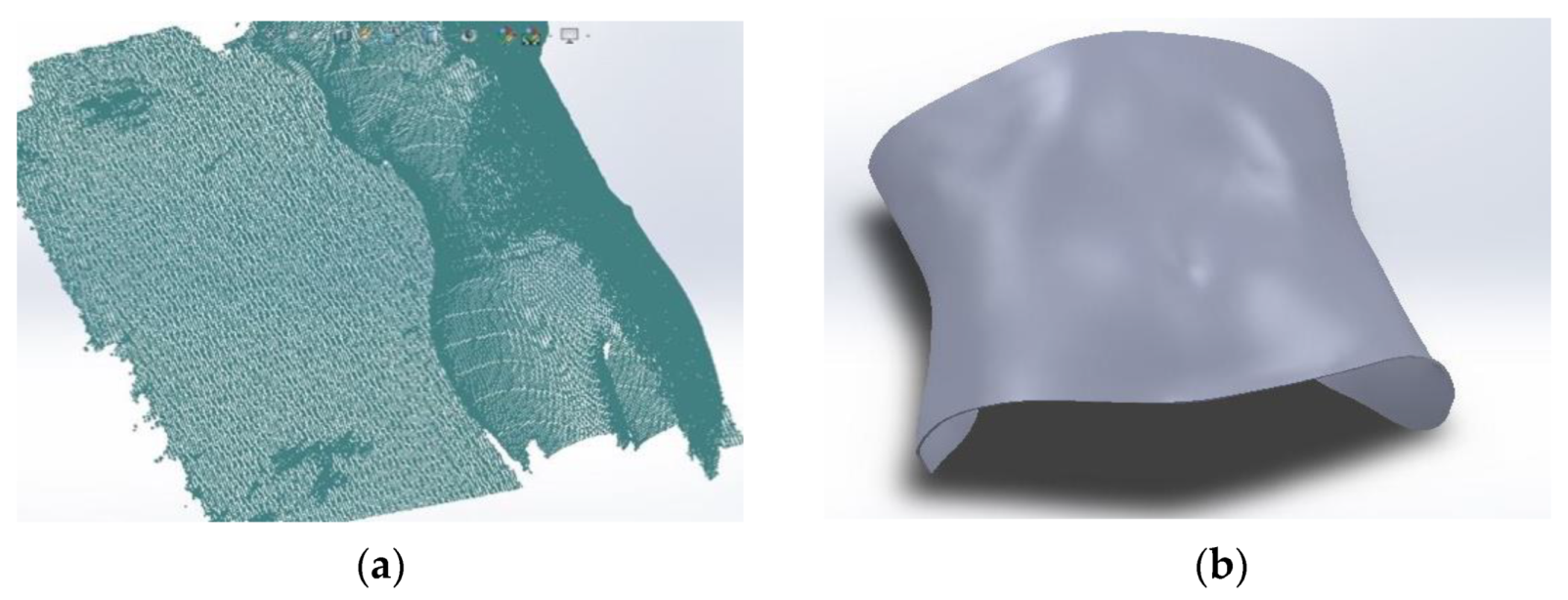
Regarding the third specific purpose of this study, we found that the total time to complete the operations before printing was approximately 45 min, subdivided as follows: 5 min for abdominal surface acquisition and about 40 min for modelling, creating and optimizing the mesh. The total printing time was 47 h and 32 min. Adding the acquisition time, modelling and printing, a total time equivalent to two full days, or 6 working days (mainly dominated by the printing time, using the FDM technique), was obtained. If the RT department produces about 320 masks per year, this translates into about 6 masks per week considering that 2019 had 53 weeks. This scenario can be considered problematic and incompatible with the clinical practice and needs of patients. However, printing times may vary depending on several factors. It is possible to greatly reduce the printing time of the mask (to 14 h) by opting for larger print layers and consequently reducing the quality and resolution of the printed mask. With this, it is necessary to verify the robustness of the mask, PLA overlap and general appearance of the mask. Patients’ individual volumes can influence time, as well, as larger patients result in longer acquisitions and printing times.
Another aspect is the experience of the staff. It is essential to introduce training programs for healthcare professionals in different 3D printing stages, creating a larger group of people involved in the process, improving the quality of the models created and helping with the continuity and sustainability of this technology in clinical departments. Additionally, modelling software plays an important role in 3D printing; however, it is often limited, given the technology that departments currently use in clinical settings. A reduction may also occur in printing time on double extruder printers. Costs can vary as well, depending on the different printer manufacturers, PLA coils and conventional masks.
Although an effective reduction in material costs is achievable, some parameters have not been accounted for, including storage costs. However, it is considered that storing a PLA coil—with approximate dimensions of 200 × 200 × 90 mm, which can originate essentially 7.18 masks—becomes more profitable and practical than storing the same seven conventional masks. Since conventional masks are mainly distributed in boxes of 10 (depending on the manufacturer) and can have dimensions of 460 × 480 × 0.20 mm each, one box will be approximately 480 × 500 × 20 mm. Additionally, a cost reduction is expected in larger centers since they can treat a higher number of patients.
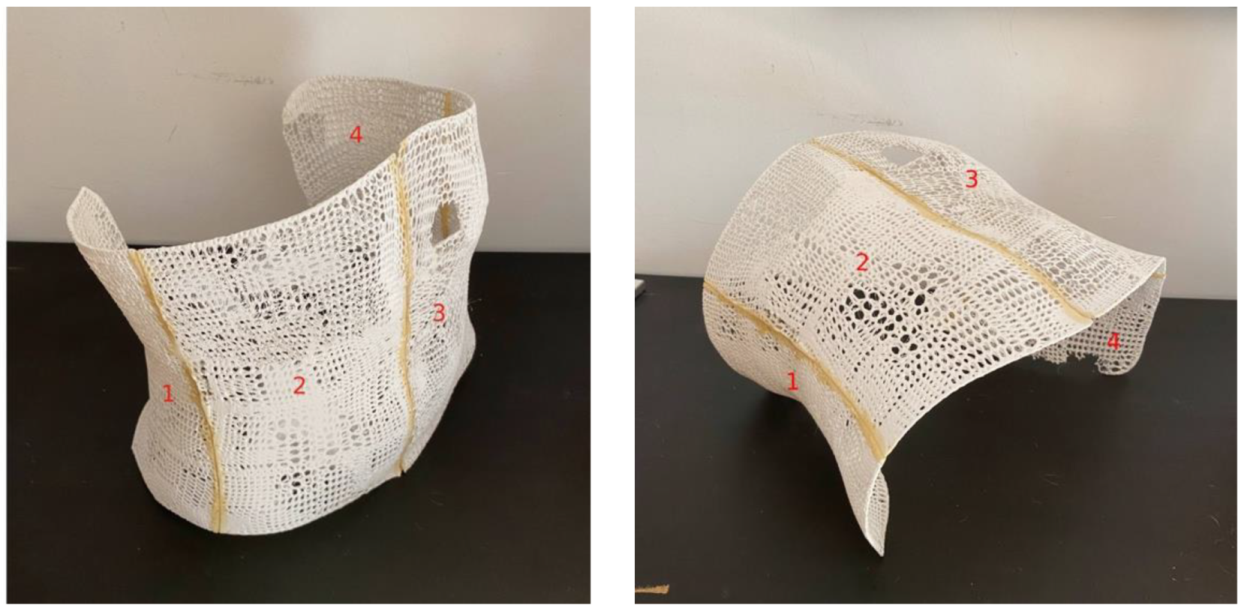
Visual inspection of the mask revealed that although the infill characteristic approached 50% in some areas of the mask, it did not remain uniform throughout the entire mask. This is due to the impossibility of the printer to recreate an infill along the curvature of the mask but in height. The immobilization model presented has several advantages. First, the high degree of automation provides the foundation for scaling the technology to a greater number of patients and the adaptability of the system offers multiple options for customization, such as the development of immobilization devices for other body parts. As an alternative to standard masks, the mask produced can be customized to reduce anxiety and improve comfort in claustrophobic patients, such as with openings in specific areas. For example, for head and neck masks, a lower infill—and hence, more open area—could be used to minimize the feeling of patient claustrophobia, and for abdominal or pelvic masks, the infill could be higher since this effect may not be triggered. Loja et al. [
28] proposed an alternative head immobilization mask prototype. Second, the patient does not have to undergo the uncomfortable and time-consuming process of mask molding, since the proposed process is contact-free. Third, PLA has shown results comparable to conventional masks in terms of radiolucency and can be used for this purpose. Moreover, the mechanical simulation developed was favorable, demonstrating that this material has enough stiffness to resist a pressure equal to the respiratory pressure of the abdomen in the mask.
Finally, taking out the capital investment required to implement the technology, mask printing singularly is less expensive in terms of material costs than purchasing conventional masks. Thus, the cost/benefit ratio of abdominal mask use increases, since if it is necessary to repeat the mask when it gains air gaps between the patient’s skin and the mask, more masks can be fabricated at a lower cost.
The present technology could also be implemented in nuclear medicine and imaging departments. For example, some PET head or abdomen acquisitions can take up to 30 min [
7,
28,
29,
30]. According to Mantlik et al. [
7], PET/MR imaging requires the use of devices to assist patient immobilization and positioning for the entire duration. In the PET/CT case, positioning throughout the combination of exams is essential to ensure maximum precision in the spatial alignment of PET information with CT, ensuring an accurate diagnosis [
7]. As for applications in diagnostic exams, it is proposed to extract the patient’s external surface immediately after the first consultation with the prescribing doctor, where the patient’s anatomy is acquired using the optical scanner so that when the patient returns on the day of the exam itself, the mask is already manufactured and ready for use. Moreover, this reduces the workload for healthcare professionals and the time the patient must be lying down, thereby increasing the availability of the CT scanner and, as a result, the profitability of the health institution with that exam.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}