
Developmental Ultrasound Characteristics in Guinea Pigs: Similarities with Human Pregnancy
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Ultrasound Assessment
2.3. Ultrasound Data Processing
2.4. Histology
2.5. Statistics
3. Results
3.1. Fetal Biometry
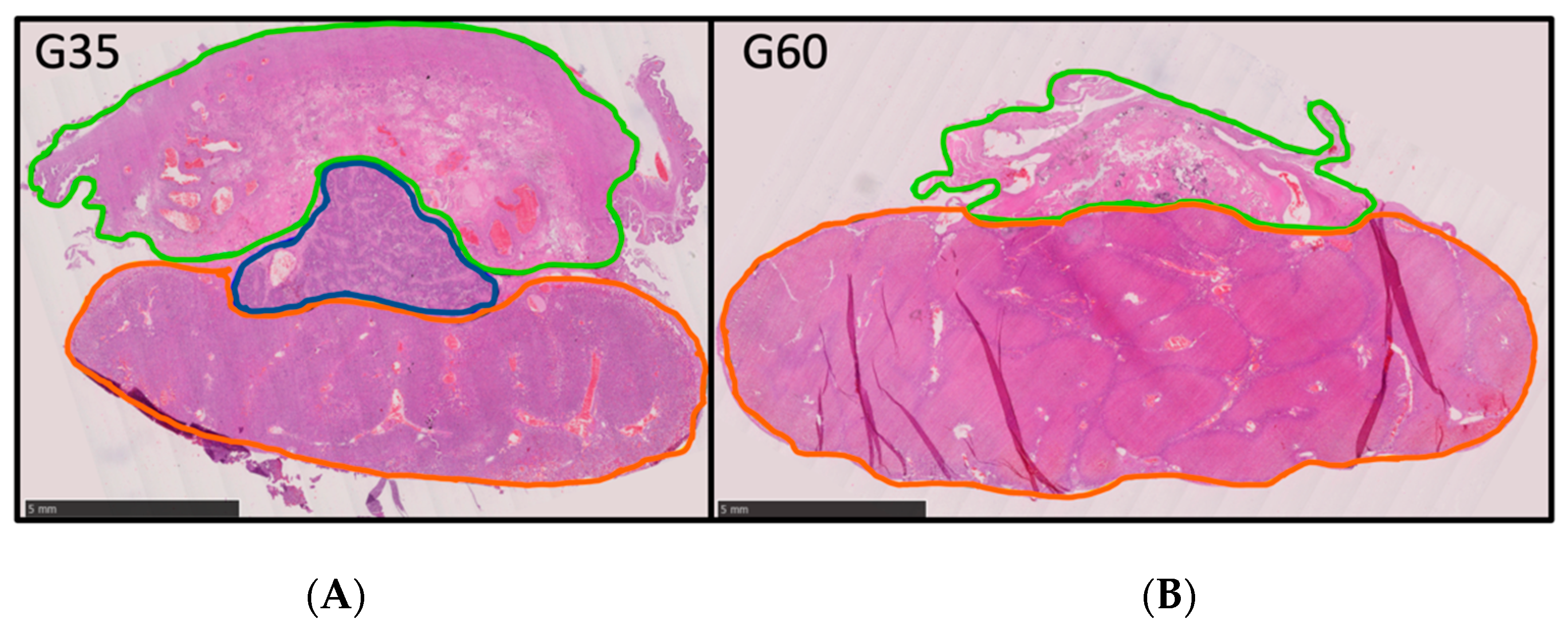
3.2. Placental Biometry
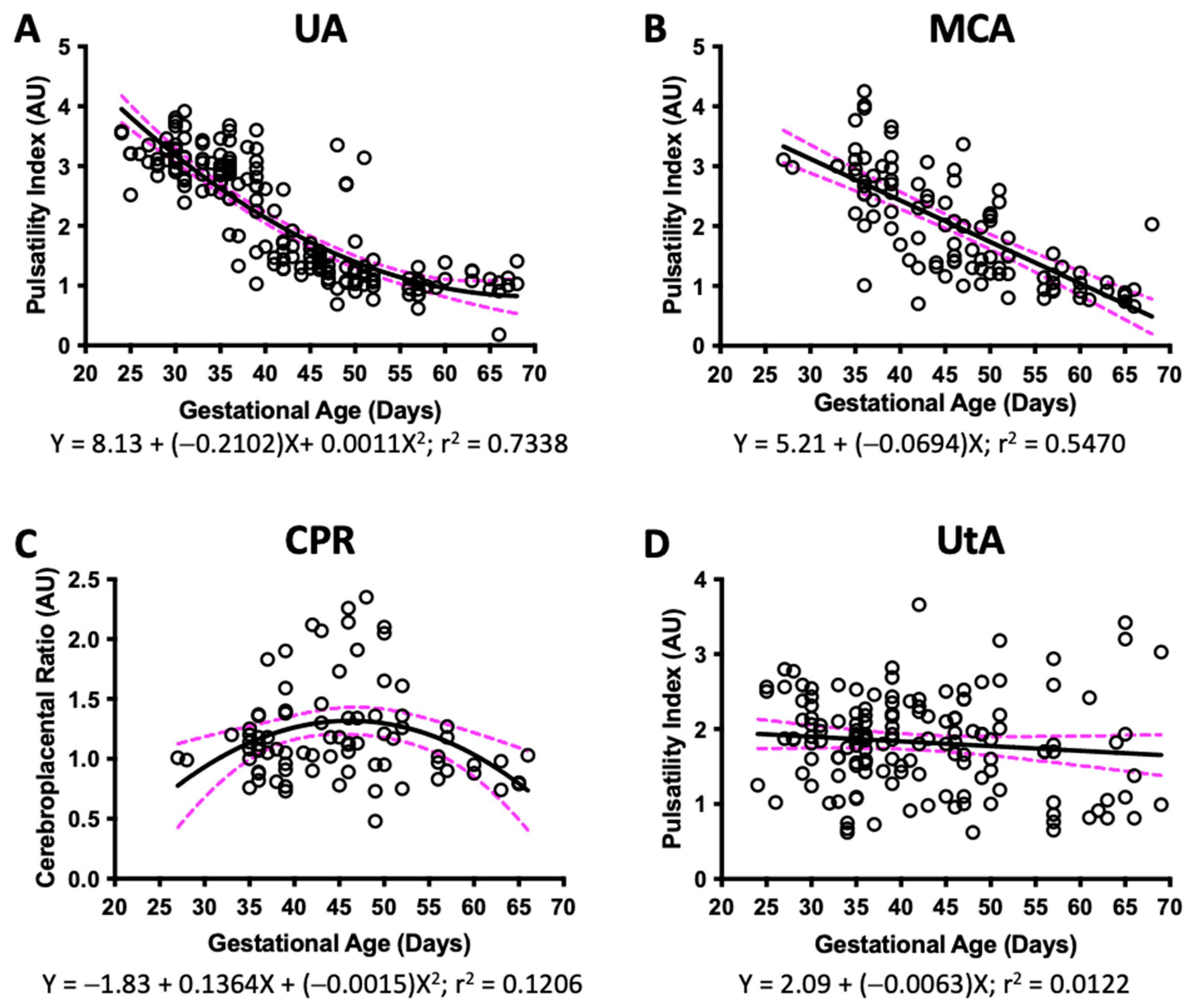
3.3. Doppler Ultrasound
3.4. Fetal and Placental Biometry
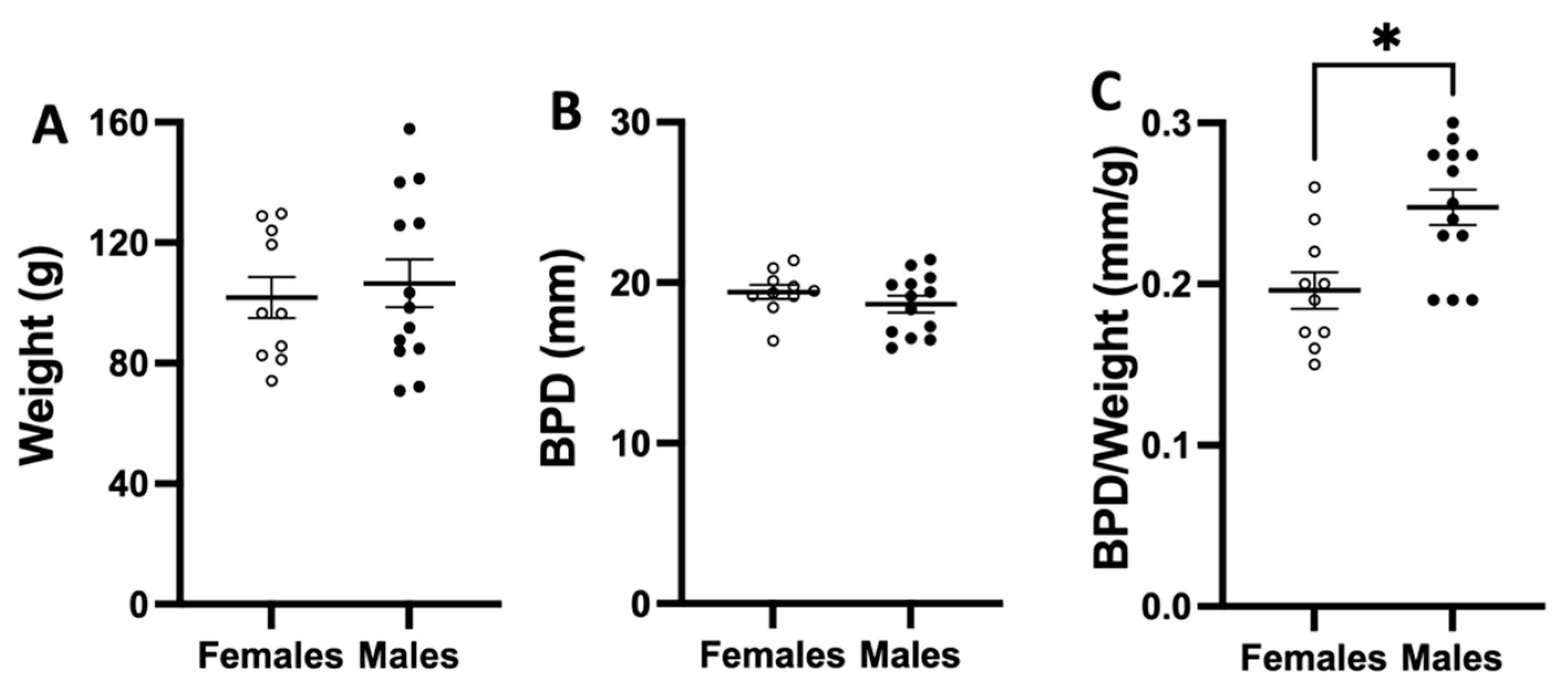
3.5. Fetal Biometry at Birth
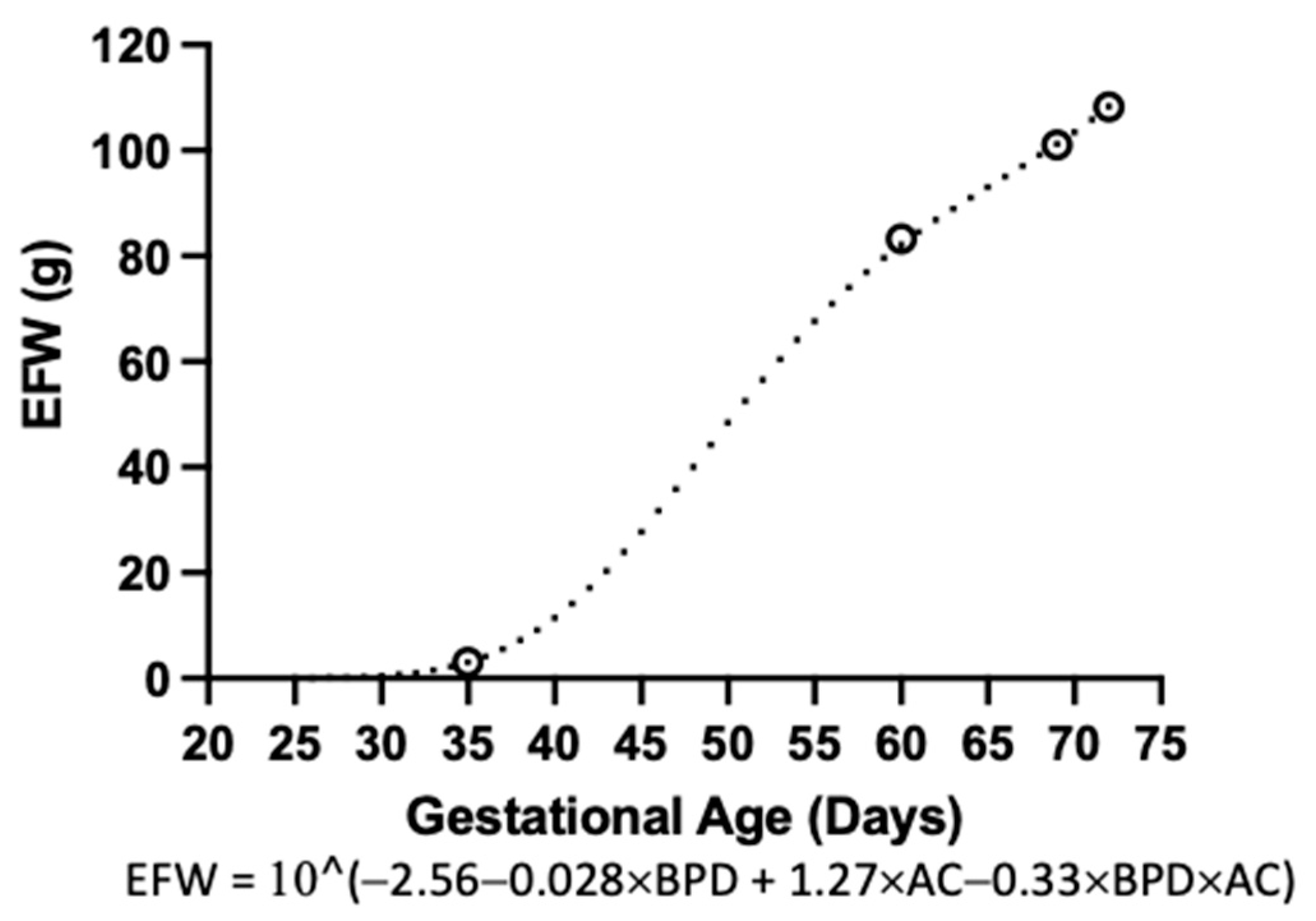
3.6. Estimated Fetal Weight
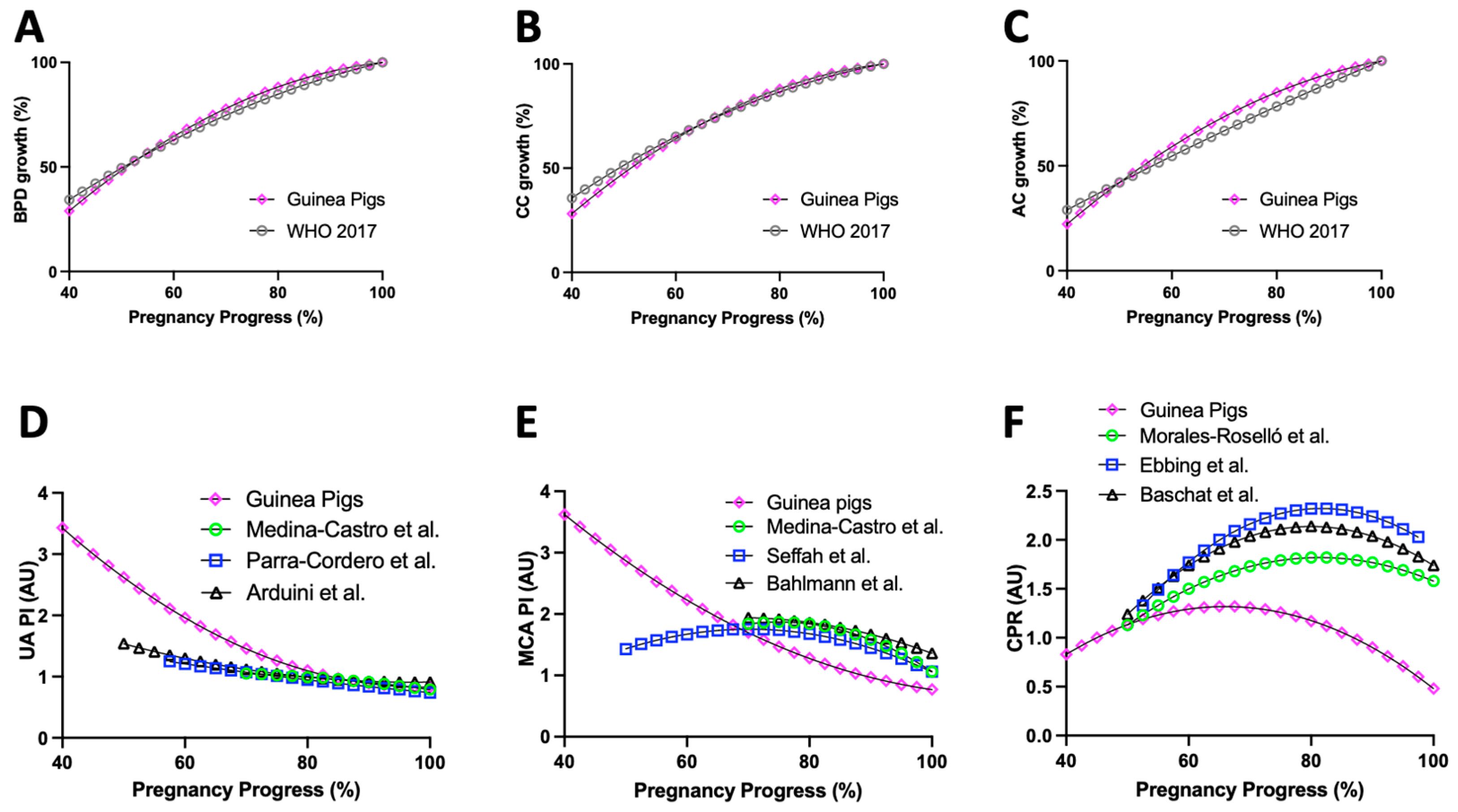
3.7. Comparison of Guinea Pig and Human Fetal Biometry
3.8. Guinea Pig and Human Doppler Ultrasound
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chilumula, K.; Saha, P.K.; Muthyala, T.; Saha, S.C.; Sundaram, V.; Suri, V. Prognostic Role of Uterine Artery Doppler in Early- and Late-Onset Preeclampsia with Severe Features. J. Ultrasound 2021, 24, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Marek, J.; Tomek, V.; Skovranek, J.; Povysilova, V.; Samanek, M. Prenatal Ultrasound Screening of Congenital Heart Disease in an Unselected National Population: A 21-Year Experience. Heart 2011, 97, 124–130. [Google Scholar] [CrossRef]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus Definition of Fetal Growth Restriction: A Delphi Procedure: Consensus Definition of FGR. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef]
- Loardi, C.; Fratelli, N.; Mazzoni, G.; Orabona, R.; Valcamonico, A.; Fichera, A.; Sartori, E.; Prefumo, F. Uterine Artery Doppler for the Prediction of Outcome in Pregnancies Complicated by Hypertensive Disorders of Pregnancy. Pregnancy Hypertens. 2021, 26, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Conde-Agudelo, A.; Villar, J.; Kennedy, S.H.; Papageorghiou, A.T. Predictive Accuracy of Cerebroplacental Ratio for Adverse Perinatal and Neurodevelopmental Outcomes in Suspected Fetal Growth Restriction: Systematic Review and Meta-Analysis: CPR Predicts Perinatal Death in Suspected FGR. Ultrasound Obstet. Gynecol. 2018, 52, 430–441. [Google Scholar] [CrossRef]
- Winchester, M.-L.; McCarther, N.; Cancino, D.; Fitzgerald, S.; Parrish, M. Second Trimester Cerebroplacental Ratio versus Umbilicocerebral Ratio for the Prediction of Adverse Perinatal Outcomes. J. Matern. Fetal Neonatal Med. 2021, 35, 7929–7935. [Google Scholar] [CrossRef]
- Monteith, C.; Flood, K.; Pinnamaneni, R.; Levine, T.A.; Alderdice, F.A.; Unterscheider, J.; McAuliffe, F.M.; Dicker, P.; Tully, E.C.; Malone, F.D.; et al. An Abnormal Cerebroplacental Ratio (CPR) Is Predictive of Early Childhood Delayed Neurodevelopment in the Setting of Fetal Growth Restriction. Am. J. Obstet. Gynecol. 2019, 221, e1–e273. [Google Scholar] [CrossRef] [PubMed]
- Morrison, J.L.; Botting, K.J.; Darby, J.R.T.; David, A.L.; Dyson, R.M.; Gatford, K.L.; Gray, C.; Herrera, E.A.; Hirst, J.J.; Kim, B.; et al. Guinea Pig Models for Translation of the Developmental Origins of Health and Disease Hypothesis into the Clinic: Guinea Pig as a Developmental Origins of Health and Disease Model. J. Physiol. 2018, 596, 5535–5569. [Google Scholar] [CrossRef]
- Fowden, A.L.; Camm, E.J.; Sferruzzi-Perri, A.N. Effects of Maternal Obesity On Placental Phenotype. Curr. Vasc. Pharmacol. 2020, 19, 113–131. [Google Scholar] [CrossRef]
- Gonzaléz-Candia, A.; Candia, A.A.; Ebensperger, G.; Reyes, R.V.; Llanos, A.J.; Herrera, E.A. The Newborn Sheep Translational Model for Pulmonary Arterial Hypertension of the Neonate at High Altitude. J. Dev. Orig. Health Dis. 2020, 11, 452–463. [Google Scholar] [CrossRef]
- Lopez-Tello, J.; Arias-Alvarez, M.; Gonzalez-Bulnes, A.; Sferuzzi-Perri, A.N. Models of Intrauterine Growth Restriction and Fetal Programming in Rabbits. Mol. Reprod. Dev. 2019, 86, 1781–1809. [Google Scholar] [CrossRef]
- Mitchell, B.F.; Taggart, M.J. Are Animal Models Relevant to Key Aspects of Human Parturition? Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2009, 297, R525–R545. [Google Scholar] [CrossRef]
- Kaufmann, P.; Black, S.; Huppertz, B. Endovascular Trophoblast Invasion: Implications for the Pathogenesis of Intrauterine Growth Retardation and Preeclampsia. Biol. Reprod. 2003, 69, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Tello, J.; Jimenez-Martinez, M.A.; Herrera, E.A.; Krause, B.J.; Sferruzzi-Perri, A.N. Progressive Uterine Artery Occlusion in the Guinea Pig Leads to Defects in Placental Structure That Relate to Fetal Growth. Placenta 2018, 72–73, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Herrera, E.A.; Alegría, R.; Farias, M.; Díaz-López, F.; Hernández, C.; Uauy, R.; Regnault, T.R.H.; Casanello, P.; Krause, B.J. Assessment of in vivo Fetal Growth and Placental Vascular Function in a Novel Intrauterine Growth Restriction Model of Progressive Uterine Artery Occlusion in Guinea Pigs: Intrauterine Growth Restriction Model in Guinea Pigs. J. Physiol. 2016, 594, 1553–1561. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.J.; Trudinger, B.J. A Modification of the Uterine Artery Restriction Technique in the Guinea Pig Fetus Produces Asymmetrical Ultrasound Growth. Placenta 2009, 30, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.; Fonseca, E.; van Melis, J.; Miglino, M.A. Morphometric Analysis of Fetal Development of Cavia Porcellus (Linnaeus, 1758) by Ultrasonography—Pilot Study. Theriogenology 2014, 81, 896–900. [Google Scholar] [CrossRef]
- Swanson, A.M.; Mehta, V.; Ofir, K.; Rowe, M.; Rossi, C.; Ginsberg, Y.; Griffin, H.; Barker, H.; White, T.; Boyd, M.; et al. The Use of Ultrasound to Assess Fetal Growth in a Guinea Pig Model of Fetal Growth Restriction. Lab. Anim. 2017, 51, 181–190. [Google Scholar] [CrossRef]
- Kiserud, T.; Piaggio, G.; Carroli, G.; Widmer, M.; Carvalho, J.; Neerup Jensen, L.; Giordano, D.; Cecatti, J.G.; Abdel Aleem, H.; Talegawkar, S.A.; et al. The World Health Organization Fetal Growth Charts: A Multinational Longitudinal Study of Ultrasound Biometric Measurements and Estimated Fetal Weight. PLoS Med. 2017, 14, e1002220. [Google Scholar] [CrossRef]
- Oros, D.; Ruiz-Martinez, S.; Staines-Urias, E.; Conde-Agudelo, A.; Villar, J.; Fabre, E.; Papageorghiou, A.T. Reference Ranges for Doppler Indices of Umbilical and Fetal Middle Cerebral Arteries and Cerebroplacental Ratio: Systematic Review. Ultrasound Obstet. Gynecol. 2019, 53, 454–464. [Google Scholar] [CrossRef] [Green Version]
- Burd, I.; Srinivas, S.; Paré, E.; Dharan, V.; Wang, E. Is Sonographic Assessment of Fetal Weight Influenced by Formula Selection? J. Ultrasound Med. 2009, 28, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Stirnemann, J.; Salomon, L.J.; Papageorghiou, A.T. INTERGROWTH-21st Standards for Hadlock’s Estimation of Fetal Weight. Ultrasound Obstet. Gynecol. 2020, 56, 946–948. [Google Scholar] [CrossRef]
- Cardiff, R.D.; Miller, C.H.; Munn, R.J. Manual Hematoxylin and Eosin Staining of Mouse Tissue Sections. Cold Spring Harb. Protoc. 2014, 2014, pdb-prot073411. [Google Scholar] [CrossRef] [PubMed]
- Medina Castro, N.; Figueroa Diesel, H.; Guzmán Huerta, M.; Hernández Andrade, E. Normal reference values of the pulsatility index from the uterine and umbilical arteries during pregnancy. Ginecol. Obstet. Mex. 2006, 74, 509–515. [Google Scholar]
- Medina Castro, N.; Figueroa Diesel, H.; Hernández Andrade, E. Normal reference values of the pulsatility index and peak systolic velocity in the fetal middle cerebral artery during normal pregnancy. Ginecol. Obstet. Mex. 2006, 74, 376–382. [Google Scholar] [PubMed]
- Parra-Cordero, M.; Lees, C.; Missfelder-Lobos, H.; Seed, P.; Harris, C. Fetal Arterial and Venous Doppler Pulsatility Index and Time Averaged Velocity Ranges: Reference Ranges for Fetal Arterial and Venous Doppler. Prenat. Diagn. 2007, 27, 1251–1257. [Google Scholar] [CrossRef]
- Arduini, D.; Rizzo, G. Normal Values of Pulsatility Index Front Fetal Vessels: A Cross-Sectional Study on 1556 Healthy Fetuses. J. Perinat. Med. 1990, 18, 165–172. [Google Scholar] [CrossRef]
- Seffah, J.D.; Swarray-Deen, A. Fetal Middle Cerebral Artery Doppler Indices and Clinical Application at Korle Bu Teaching Hospital, Accra, Ghana. Int. J. Gynecol. Obstet. 2016, 134, 135–139. [Google Scholar] [CrossRef]
- Bahlmann, F.; Fittschen, M.; Reinhard, I.; Wellek, S.; Puhl, A. Blood Flow Velocity Waveforms of the Umbilical Artery in a Normal Population: Reference Values from 18 Weeks to 42 Weeks of Gestation. Ultraschall Med. Eur. J. Ultrasound 2012, 33, E80–E87. [Google Scholar] [CrossRef]
- Morales-Roselló, J.; Khalil, A.; Morlando, M.; Hervás-Marín, D.; Perales-Marín, A. Doppler Reference Values of the Fetal Vertebral and Middle Cerebral Arteries, at 19–41 Weeks Gestation. J. Matern. Fetal Neonatal Med. 2015, 28, 338–343. [Google Scholar] [CrossRef]
- Ebbing, C.; Rasmussen, S.; Kiserud, T. Middle Cerebral Artery Blood Flow Velocities and Pulsatility Index and the Cerebroplacental Pulsatility Ratio: Longitudinal Reference Ranges and Terms for Serial Measurements. Ultrasound Obstet. Gynecol. 2007, 30, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Baschat, A.A.; Gembruch, U. The Cerebroplacental Doppler Ratio Revisited: Cerebroplacental Doppler Ratio. Ultrasound Obstet. Gynecol. 2003, 21, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Chavatte-Palmer, P.; Laigre, P.; Simonoff, E.; Chesné, P.; Challah-Jacques, M.; Renard, J.-P. In Utero Characterisation of Fetal Growth by Ultrasound Scanning in the Rabbit. Theriogenology 2008, 69, 859–869. [Google Scholar] [CrossRef]
- Pallares, P.; Gonzalez-Bulnes, A. Use of Ultrasound Imaging for Early Diagnosis of Pregnancy and Determination of Litter Size in the Mouse. Lab. Anim. 2009, 43, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.J.; Trudinger, B.J. Ultrasound Measurement of Biparietal Diameter and Umbilical Artery Blood Flow in the Normal Fetal Guinea Pig. Comp. Med. 2000, 50, 6. [Google Scholar]
- Czarnecki, R.; Adamski, M. Factors Influencing Litter Size and Birthweight in the Newborn Long-Haired Guinea Pigs ( Cavia Aperea f. Porcellus). J. Appl. Anim. Res. 2016, 44, 71–76. [Google Scholar] [CrossRef]
- Draper, R.L. The Prenatal Growth of the Guinea-Pig. Anat. Rec. 1920, 18, 369–392. [Google Scholar] [CrossRef]
- Ibsen, H.L. Prenatal Growth in Guinea-Pigs with Special Reference to Environmental Factors Affecting Weight at Birth. J. Exp. Zool. 1928, 51, 51–93. [Google Scholar] [CrossRef]
- Ahn, K.H.; Lee, J.H.; Cho, G.J.; Hong, S.-C.; Oh, M.-J.; Kim, H.-J. Placental Thickness-to-Estimated Foetal Weight Ratios and Small-for-Gestational-Age Infants at Delivery. J. Obstet. Gynaecol. 2017, 37, 883–887. [Google Scholar] [CrossRef]
- Burton, G.J.; Fowden, A.L.; Thornburg, K.L. Placental Origins of Chronic Disease. Physiol. Rev. 2016, 96, 1509–1565. [Google Scholar] [CrossRef]
- Davies, J.; Dempsey, E.W.; Amoroso, E.C. The Subplacenta of the Guinea-Pig: Development, Histology and Histochemistry. J. Anat. 1961, 95, 457–473. [Google Scholar] [PubMed]
- De Clercq, K.; Persoons, E.; Napso, T.; Luyten, C.; Parac-Vogt, T.N.; Sferruzzi-Perri, A.N.; Kerckhofs, G.; Vriens, J. High-Resolution Contrast-Enhanced MicroCT Reveals the True Three-Dimensional Morphology of the Murine Placenta. Proc. Natl. Acad. Sci. USA 2019, 116, 13927–13936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikkelsen, E.; Lauridsen, H.; Nielsen, P.M.; Qi, H.; Nørlinger, T.; Andersen, M.D.; Uldbjerg, N.; Laustsen, C.; Sandager, P.; Pedersen, M. The Chinchilla as a Novel Animal Model of Pregnancy. R. Soc. Open Sci. 2017, 4, 161098. [Google Scholar] [CrossRef]
- Wolf, H.; Stampalija, T.; Lees, C.C.; TRUFFLE Study Group; Arabin, B.; Berger, A.; Bergman, E.; Bhide, A.; Bilardo, C.M.; Breeze, A.C.; et al. Fetal Cerebral Blood-flow Redistribution: Analysis of Doppler Reference Charts and Association of Different Thresholds with Adverse Perinatal Outcome. Ultrasound Obstet. Gynecol. 2021, 58, 705–715. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Definition | Units | Representative Image |
|---|---|---|---|
| Biparietal diameter (BPD) | From a transversal visualization of the cranium: Distance from the external side of the parietal bone to the internal side of the opposite parietal bone | mm |  |
| Cranial circumference (CC) | Elipse around DBP as transversal diameter and a longitudinal diameter touching the occipital bone | mm (perimeter), mm2 (area) |  |
| Abdominal circumference (AC) | Circumference around the edges of a transversal abdominal visualization at stomach/liver level | mm (perimeter), mm2 (area) |  |
| Transversal area of placenta (PA) | Region observed in a transversal visualization of placenta excluding decidua | mm (perimeter), mm2 (area) |  |
| Placental length (PL) | Longitudinal segment in a transversal visualization of placenta | mm |  |
| Placental thickness (PT) | Transversal segment in a transversal visualization of placenta | mm |  |
| Discoid area of placenta | Region observed in a posterior visualization of placenta | mm (perimeter), mm2 (area) |  |
| Umbilical artery (UA) | From a longitudinal view of the placenta: Blood flow detected by Doppler ultrasound between the fetus abdomen and the placenta | Pulsatility index ((systolic velocity-diastolic velocity)/mean velocity) |  |
| Middle cerebral artery (MCA) | From a transversal visualization of the cranium: Blood flow detected by Doppler ultrasound above the circle of Willis in a transverse direction | Pulsatility index ((systolic velocity-diastolic velocity)/mean velocity) |  |
| Uterine Artery (UtA) | From a sagittal view of the maternal urinary bladder: Blood flow detected by Doppler ultrasound surrounding the bladder in an ~45° angle | Pulsatility index ((systolic velocity-diastolic velocity)/mean velocity) |  |
| Cerebro-placental ratio (CPR) | Ratio between MCA and UA pulsatility indexes | AU |
| G35 | G60 | |
|---|---|---|
| Fetal Weight (g) | 3.06 ± 0.28 | 83.30 ± 3.47 |
| BPD (mm) 1 | 9.21 ± 0.35 | 10.09 ± 0.35 |
| Volume (mm3) | 3.23 ± 0.16 | 79.00 ± 2.99 |
| Placental weight (g) | 2.51 ± 0.21 | 5.60 ± 0.23 |
| Placental Thickness (mm) | 6.12 ± 0.42 | 8.90 ± 0.71 |
| Placental Length (mm) | 19.43 ± 0.42 | 29.35 ± 0.74 |
| Placental Width (mm) | 14.43 ± 0.45 | 25.70 ± 0.57 |
| Placental Volume (mm3) | 2.74 ± 0.12 | 6.75 ± 0.39 |
| Placental Efficiency (AU) | 1.24 ± 0.08 | 15.06 ± 0.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Candia, A.A.; Jiménez, T.; Navarrete, Á.; Beñaldo, F.; Silva, P.; García-Herrera, C.; Sferruzzi-Perri, A.N.; Krause, B.J.; González-Candia, A.; Herrera, E.A. Developmental Ultrasound Characteristics in Guinea Pigs: Similarities with Human Pregnancy. Vet. Sci. 2023, 10, 144. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci10020144
Candia AA, Jiménez T, Navarrete Á, Beñaldo F, Silva P, García-Herrera C, Sferruzzi-Perri AN, Krause BJ, González-Candia A, Herrera EA. Developmental Ultrasound Characteristics in Guinea Pigs: Similarities with Human Pregnancy. Veterinary Sciences. 2023; 10(2):144. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci10020144
Chicago/Turabian StyleCandia, Alejandro A., Tamara Jiménez, Álvaro Navarrete, Felipe Beñaldo, Pablo Silva, Claudio García-Herrera, Amanda N. Sferruzzi-Perri, Bernardo J. Krause, Alejandro González-Candia, and Emilio A. Herrera. 2023. "Developmental Ultrasound Characteristics in Guinea Pigs: Similarities with Human Pregnancy" Veterinary Sciences 10, no. 2: 144. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci10020144