
Impacts of Mobility Dogs on Kinematics during Ambulation: A Quantitative Study

 ,
,
Abstract
:1. Introduction
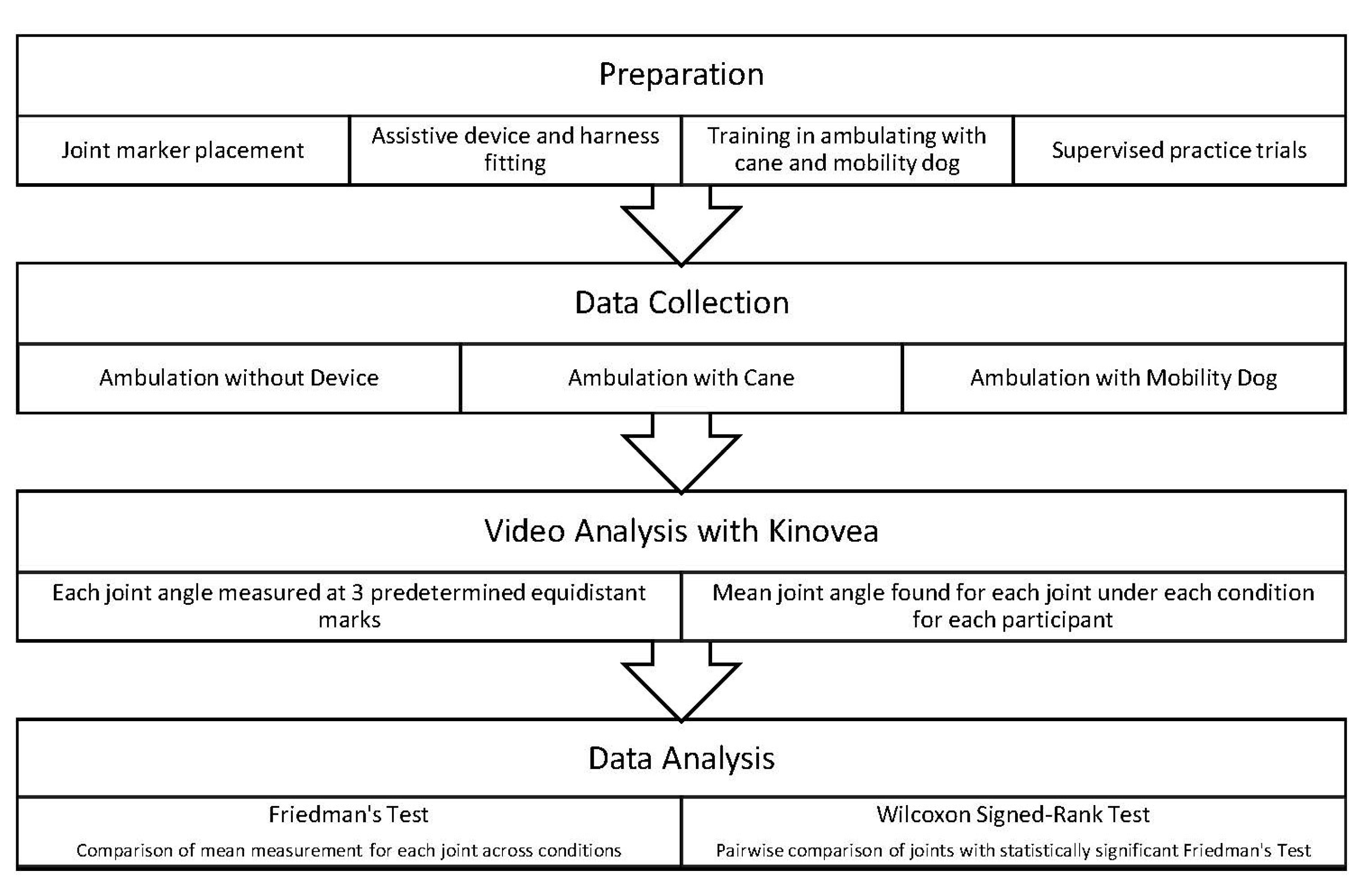
2. Materials and Methods
2.1. Participant Recruitment
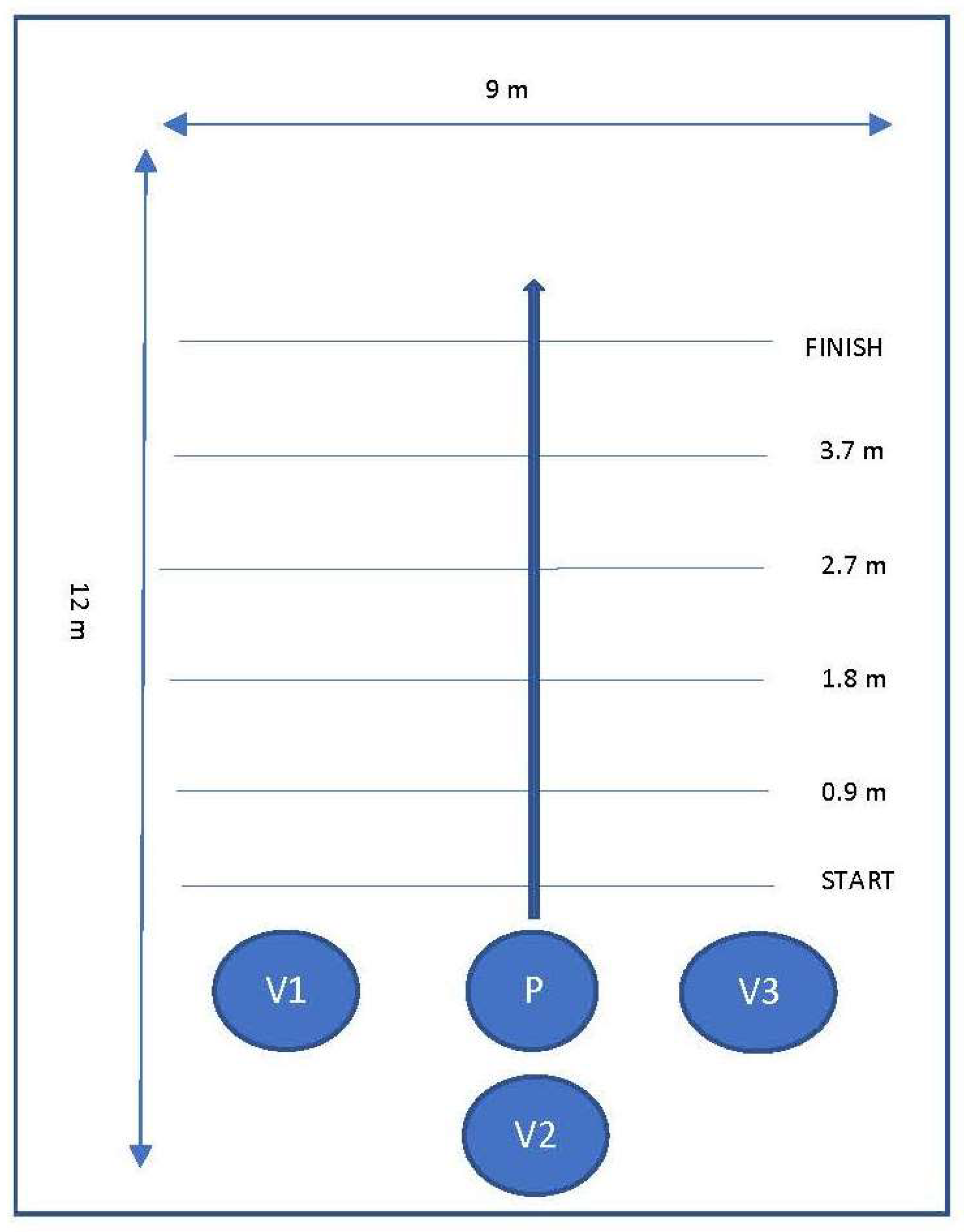
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Significant Differences in Joint Position across Conditions
3.2. Significant Differences in Joint Positions within Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Disability and Health. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/disability-and-health (accessed on 16 January 2018).
- Centers for Disease Control and Prevention. Disability Impacts All of Us. Available online: https://www.cdc.gov/ncbddd/disabilityandhealth/infographic-disability-impacts-all.html (accessed on 9 September 2019).
- Gell, N.M.; Wallace, R.B.; Lacroix, A.Z.; Mroz, T.M.; Patel, K.V. Mobility Device Use in Older Adults and Incidence of Falls and Worry About Falling: Findings from the 2011–2012 National Health and Aging Trends Study. J. Am. Geriatr. Soc. 2015, 63, 853–859. [Google Scholar] [CrossRef]
- Bateni, H.; Maki, B.E. Assistive devices for balance and mobility: Benefits, demands, and adverse consequences. Arch. Phys. Med. Rehabil. 2005, 86, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Bradley, S.M.; Hernandez, C.R. Geriatric assistive devices. Am. Fam. Physician 2011, 84, 405–411. [Google Scholar] [PubMed]
- Bachschmidt, R.; Harris, G.; Simoneau, G. Walker-assisted gait in rehabilitation: A study of biomechanics and instrumentation. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 96–105. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, G. Good posture supports the use of assistive technology. Technol. Spec. Interest Sect. Q./Am. Occup. Ther. Assoc. 2013, 23, 1–4. [Google Scholar]
- Stevens, J.A.; Thomas, K.; Teh, L.; Greenspan, A.I. Unintentional Fall Injuries Associated with Walkers and Canes in Older Adults Treated in U.S. Emergency Departments. J. Am. Geriatr. Soc. 2009, 57, 1464–1469. [Google Scholar] [CrossRef]
- Krautwurst, B.K.; Dreher, T.; Wolf, S.I. The impact of walking devices on kinematics in patients with spastic bilateral cerebral palsy. Gait Posture 2016, 46, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Grace, K. Brace and Mobility Support Dogs: Everything You Need to Know. Available online: https://www.anythingpawsable.com/brace-mobility-support-dogs-complete-guide/ (accessed on 14 September 2020).
- Martin-Lemoyne, V.; Gagnon, D.H.; Routhier, F.; Poissant, L.; Tousignant, M.; Corriveau, H.; Vincent, C.; Tousignan, M. To What Extent Can the Use of a Mobility Assistance Dog Reduce Upper Limb Efforts When Manual Wheelchair Users Ascend a Ramp? J. Appl. Biomech. 2016, 32, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, D.; Blanchet, M.; Martin-Lemoyne, V.; Vincent, C.; Routhier, F.; Corriveau, H. Using a mobility assistance dog reduces upper limb effort during manual wheelchair ramp ascent in an individual with spinal cord injury. J. Spinal Cord Med. 2013, 36, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Blanchet, M.; Pt, D.H.G.; Ot, C.V.; Boucher, P.; Routhier, F.; Martin-Lemoyne, V. Effects of a Mobility Assistance Dog on the Performance of Functional Mobility Tests Among Ambulatory Individuals with Physical Impairments and Functional Disabilities. Assist. Technol. 2013, 25, 247–252. [Google Scholar] [CrossRef]
- Abbud, G.; Janelle, C.; Vocos, M. The Use of a Trained Dog as a Gait Aid for Clients with Ataxia: A Case Report. Physiother. Can. 2014, 66, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Rondeau, L.; Corriveau, H.; Bier, N.; Camden, C.; Champagne, N.; Dion, C. Effectiveness of a rehabilitation dog in fostering gait retraining for adults with a recent stroke: A multiple single-case study. NeuroRehabilitation 2010, 27, 155–163. [Google Scholar] [CrossRef]
- Noguchi, H.; Hoshiyama, M.; Tagawa, Y. Kinematic analysis of sit to stand by persons with rheumatoid arthritis supported by a service dog. Disabil. Rehabil. Assist. Technol. 2010, 7, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Coppinger, R.; Coppinger, L.; Skillings, E. Observations on Assistance Dog Training and Use. J. Appl. Anim. Welf. Sci. 1998, 1, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Orthopaedic Section Poster Presentations (Abstracts OPO1–OPO300). J. Orthop. Sports Phys. Ther. 2018, 48, A67–A202. [CrossRef]
- Davis, M. Guide Dog User Research Takes a Holistic Approach to Reduce Joint Pain. Available online: https://workinglikedogs.com/guide-dog-user-research-takes-a-holistic-approach-to-reduce-joint-pain/ (accessed on 14 September 2020).
- Opheim, A.; McGinley, J.; Olsson, E.; Stanghelle, J.; Jahnsen, R. Walking deterioration and gait analysis in adults with spastic bilateral cerebral palsy. Gait Posture 2013, 37, 165–171. [Google Scholar] [CrossRef]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait Analysis Using Wearable Sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef] [PubMed]
- Zügner, R.; Tranberg, R.; Lisovskaja, V.; Kärrholm, J. Different reliability of instrumented gait analysis between patients with unilateral hip osteoarthritis, unilateral hip prosthesis and healthy controls. BMC Musculoskelet. Disord. 2018, 19, 1–9. [Google Scholar] [CrossRef]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly: A clinical guide. Wien. Klin. Wochenschr. 2016, 129, 81–95. [Google Scholar] [CrossRef] [Green Version]
- Assessment: Timed Up & Go (TUG). Available online: https://www.cdc.gov/steadi/pdf/TUG_test-print.pdf (accessed on 30 September 2021).
- Stroke Engine: Functional Ambulation Categories (FAC). Available online: https://strokengine.ca/en/assessments/fac/ (accessed on 30 September 2021).
- Tinetti Test. Available online: https://www.physio-pedia.com/Tinetti_Test (accessed on 30 September 2021).
- Core Measure: Functional Gait Assessment (FGA). Available online: https://www.neuropt.org/docs/default-source/cpgs/core-outcome-measures/core-measure-functional-gait-assessment_final.pdf?sfvrsn=d4585243_2&sfvrsn=d4585243_2 (accessed on 30 September 2021).
- Mayo Clinic Cane Tips. Available online: https://www.mayoclinic.org/healthy-lifestyle/healthy-aging/multimedia/canes/sls-20077060?s=3 (accessed on 21 August 2019).
- Bold Lead Designs. Balance Assistance Harness (BAH) & Mobility Support Harness (MSH) by Bold Lead Designs: Detailed Information Booklet. Aurora (CO). Available online: https://1nz5jq3h8hsp3sh32y152o7c-wpengine.netdna-ssl.com/wp-content/uploads/2020/08/BAH-MSH-Info-Booklet-2020-r1.pdf (accessed on 9 June 2021).
- Kinovea. (n.d.). Kinovea Overview. Available online: http://www.kinovea.org/help/en/004.html (accessed on 29 September 2021).
- Elrahim, R.M.A.; Embaby, E.A.; Ali, M.F.; Kamel, R.M. Inter-rater and intra-rater reliability of Kinovea software for measurement of shoulder range of motion. Bull. Fac. Phys. Ther. 2016, 21, 80–87. [Google Scholar] [CrossRef]
- El-Raheem, R.M.A.; Kamel, R.M.; Ali, M.F. Reliability of Using Kinovea Program in Measuring Dominant Wrist Joint Range of Motion. Trends Appl. Sci. Res. 2015, 10, 224–230. [Google Scholar] [CrossRef] [Green Version]
- Elwardany, S.H.; El-Sayed, W.H.; Ali, M.F. Reliability of Kinovea Computer Program in Measuring Cervical Range of Motion in Sagittal Plane. Open Access Libr. J. 2015, 2. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical notes for clinical researchers: Nonparametric statistical methods: 2. Nonparametric methods for comparing three or more groups and repeated measures. Restor. Dent. Endod. 2014, 39, 329–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parris, A. Ruffwear Rethinks Guide Dog Harnesses. Available online: https://www.rei.com/blog/run/ruffwear-unifly-harness (accessed on 14 September 2020).
- Patten, M.L.; Newhart, M. Confounding in Experiments. In Understanding Research Methods; Routledge: Oxfordshire, UK, 2017; pp. 198–200. [Google Scholar]



{kind=link}
{kind=link}
| Joint Angle | No Device | Cane | Dog | p-Value |
|---|---|---|---|---|
| Elbow Flexion, Right | 12.80 (3.85) | 13.75 (6.71) | 12.11 (4.75) | 0.38 |
| Shoulder Abduction, Right | -- 1 | -- 1 | -- 1 | |
| Thoracic Spinal Curvature, Right | 1.29 (0.86) 2 | 1.29 (0.97) 2 | 1.56 (1.04) 2 | 0.34 |
| Hip Flexion, Right | 16.40 (3.55) | 15.40 (5.68) | 16.88 (4.69) | 0.74 |
| Hip Extension, Right | -- 3 | -- 3 | -- 3 | |
| Knee Flexion, Right | 10 (3.28) | 9.29 (3.19) | 10.58 (4.84) | 0.83 |
| Ankle Plantarflexion, Right | 15.4 (6.11) | 16.10 (6.75) | 14.40 (7.67) | 0.21 |
| Joint Angle | No Device | Cane | Dog | p-Value |
|---|---|---|---|---|
| Elbow Flexion, Left | 18.79 (11.54) | 36.77 (12.88) | 28.73(12.38) | 0.00 3 |
| Shoulder Abduction, Left | 9.58 (3.60) | 12.88 (3.81) | 20.54 (4.75) | 0.00 3 |
| Thoracic Spinal Curvature, Left | -- 1 | -- 1 | --1 | |
| Hip Flexion, Left | -- 2 | -- 2 | -- 2 | |
| Hip Extension, Left | 14.54 (5.66) | 15.42 (5.60) | 10.42 (4.30) | 0.03 3 |
| Knee Flexion, Left | 19.31 (9.01) | 15.71 (7.53) | 20.10 (6.36) | 0.44 |
| Ankle Plantarflexion, Left | 12.09 (7.22) | 9.44 (5.64) | 13.10 (5.54) | 0.17 |
| Condition | Elbow Flexion (L) | Shoulder Abduction (L) | Hip Extension (L) |
|---|---|---|---|
| Dog-Cane | 0.023 | 0.001 1 | 0.016 1 |
| Dog-No Device | 0.044 | 0.000 1 | 0.006 1 |
| Cane-No Device | 0.001 1 | 0.002 1 | 0.586 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altman, K.; Glumm, S.; Stainton, K.; Herlache-Pretzer, E.; Webster, S.; Winkle, M.Y. Impacts of Mobility Dogs on Kinematics during Ambulation: A Quantitative Study. Vet. Sci. 2021, 8, 250. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8110250
Altman K, Glumm S, Stainton K, Herlache-Pretzer E, Webster S, Winkle MY. Impacts of Mobility Dogs on Kinematics during Ambulation: A Quantitative Study. Veterinary Sciences. 2021; 8(11):250. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8110250
Chicago/Turabian StyleAltman, Kayla, Samantha Glumm, Kendall Stainton, Ellen Herlache-Pretzer, Stacey Webster, and Melissa Y. Winkle. 2021. "Impacts of Mobility Dogs on Kinematics during Ambulation: A Quantitative Study" Veterinary Sciences 8, no. 11: 250. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8110250