
Cheese Intake Exhibits an Alteration of Glycolipid Profile and Impacts on Non-Alcoholic Fatty Liver in Bahraini Older Adults

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Study Design
2.2. Sample Size and Inclusion and Exclusion Criteria
2.3. Data Collection
2.3.1. Dietary Intake Assessment
2.3.2. Ultrasound Examination
2.3.3. Demographic, Anthropometric, and Biochemical Assessment
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Study Population
3.2. Relationship between Food Frequency Consumption and MetS Risk Factors
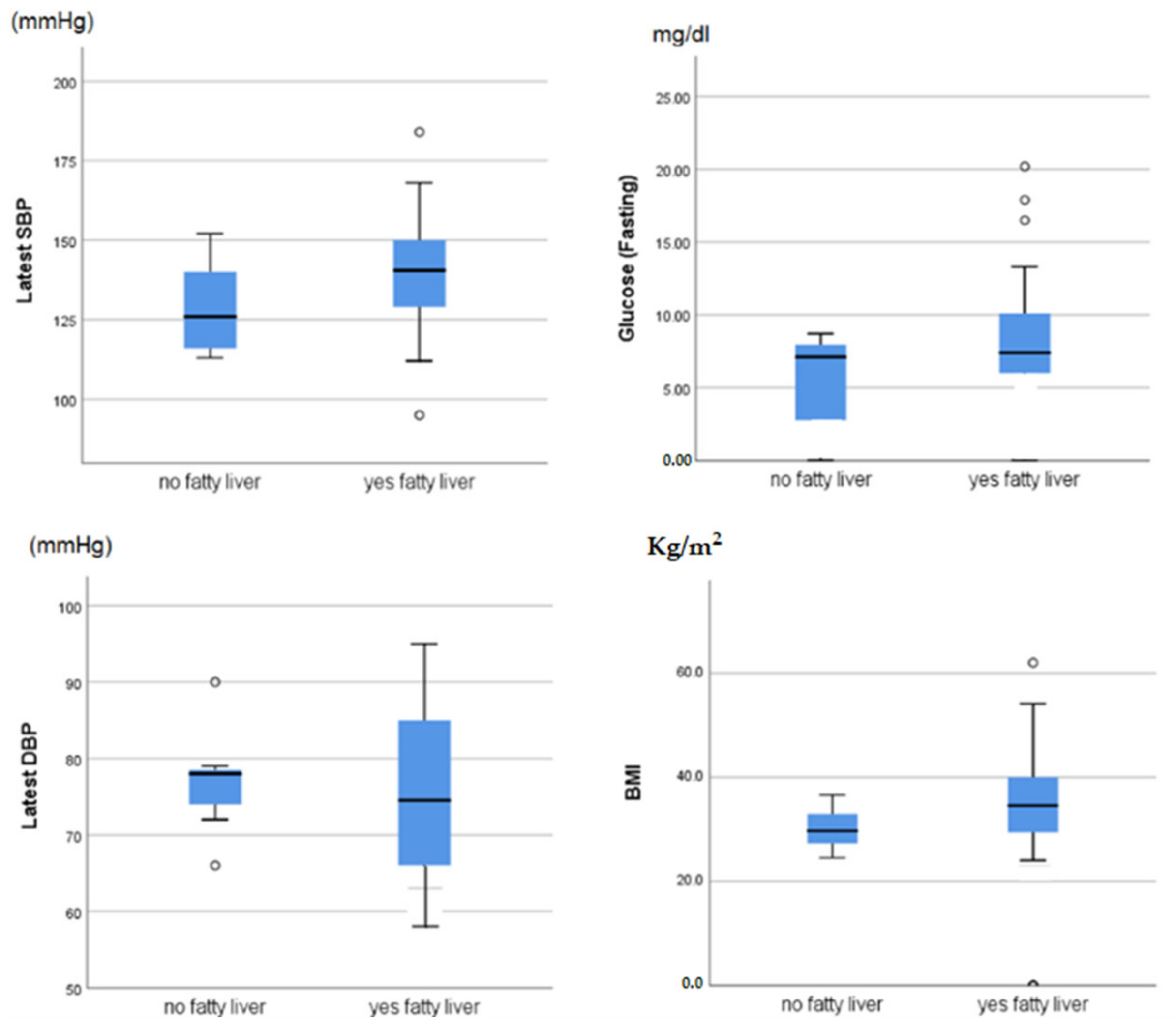
3.3. Relationship between Food Frequency Consumption and Fatty Liver
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaur, J. A comprehensive review on metabolic syndrome. Cardiol. Res. Pract. 2014, 2014, 943162. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M.; Thamer, L.; Jahrami, H. Prevalence of Metabolic Syndrome among Patients with Bipolar Affective Disorder. Bahrain Med. Bull. 2019, 41, 230–233. [Google Scholar]
- VanWormer, J.J.; Boucher, J.L.; Sidebottom, A.C.; Sillah, A.; Knickelbine, T. Lifestyle changes and prevention of metabolic syndrome in the Heart of New Ulm Project. Prev. Med. Rep. 2017, 6, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Sekgala, M.D.; Monyeki, K.D.; Mogale, A.; Mchiza, Z.J.; Parker, W.-A.; Choma, S.; Makgopa, H.M. The risk of metabolic syndrome as a result of lifestyle among Ellisras rural young adults. J. Hum. Hypertens. 2018, 32, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Al-Qawasmeh, R.; Tayyem, R.F. Dietary and lifestyle risk factors and metabolic syndrome: Literature review. Curr. Res. Nutr. Food Sci. 2018, 6, 594–608. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, M.M.; Sánchez, E.; Barrio, F.; Costa, B.; Flores-Mateo, G. Metabolic syndrome and dietary patterns: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2016, 56, 925–947. [Google Scholar] [CrossRef]
- Naja, F.; Nasreddine, L.; Itani, L.; Adra, N.; Sibai, A.M.; Hwalla, N. Association between dietary patterns and the risk of metabolic syndrome among Lebanese adults. Eur. J. Nutr. 2011, 52, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Al-Daghri, N.M.; Khan, N.; Alkharfy, K.M.; Al-Attas, O.S.; Alokail, M.S.; Alfawaz, H.A.; Alothman, A.; Paul, M.V. Selected Dietary Nutrients and the Prevalence of Metabolic Syndrome in Adult Males and Females in Saudi Arabia: A Pilot Study. Nutrients 2013, 5, 4587–4604. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Lee, K.; Rebholz, C.M.; Kim, J. Association between unhealthy plant-based diets and the metabolic syndrome in adult men and women: A population-based study in South Korea. Br. J. Nutr. 2021, 125, 577–590. [Google Scholar] [CrossRef]
- Wei, Z.-Y.; Liu, J.-J.; Zhan, X.-M.; Feng, H.-M.; Zhang, Y.-Y. Dietary patterns and the risk of metabolic syndrome in Chinese adults: A population-based cross-sectional study. Public Health Nutr. 2018, 21, 2409–2416. [Google Scholar] [CrossRef] [Green Version]
- Neuenschwander, M.; Barbaresko, J.; Pischke, C.R.; Iser, N.; Beckhaus, J.; Schwingshackl, L.; Schlesinger, S. Intake of dietary fats and fatty acids and the incidence of type 2 diabetes: A systematic review and dose-response meta-analysis of prospective observational studies. PLoS Med. 2020, 17, e1003347. [Google Scholar] [CrossRef] [PubMed]
- Zeraatkar, D.; Han, M.A.; Guyatt, G.H.; Vernooij, R.W.; El Dib, R.; Cheung, K.; Milio, K.; Zworth, M.; Bartoszko, J.J.; Valli, C.; et al. Red and processed meat consumption and risk for all-cause mortality and cardiometabolic outcomes: A systematic review and meta-analysis of cohort studies. Ann. Intern. Med. 2019, 171, 703–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzeidan, R.A.; Rabiee, F.; Mandil, A.A.; Hersi, A.S.; Ullah, A.A. Changes in dietary habits, physical activity and status of metabolic syndrome among expatriates in Saudi Arabia. East Mediterr. Health J. 2017, 23, 836–844. [Google Scholar] [CrossRef]
- National Institutes of Health. ATP III Guidelines at-A-Glance Quick Desk Reference; NIH: Bethesda, MD, USA, 2001; pp. 01–3305.
- Jahrami, H.A.; Faris, M.E.; Saif, Z.Q.; Hammad, L.H. Assessing dietary and lifestyle risk factors and their associations with disease comorbidities among patients with schizophrenia: A case-control study from Bahrain. Asian J. Psychiatr. 2017, 28, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; Worsley, A.; Timperio, A.; McNaughton, S.A. Understanding meal patterns: Definitions, methodology and impact on nutrient intake and diet quality. Nutr. Res. Rev. 2015, 28, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Alalwan, T.A.; Perna, S.; Mandeel, Q.A.; Abdulhadi, A.; Alsayyad, A.S.; D’Antona, G.; Negro, M.; Riva, A.; Petrangolini, G.; Allegrini, P.; et al. Effects of daily low-dose date consumption on glycemic control, lipid profile, and quality of life in adults with pre-and type 2 diabetes: A randomized controlled trial. Nutrients 2020, 12, 217. [Google Scholar] [CrossRef] [Green Version]
- De Goede, J.; Geleijnse, J.M.; Ding, E.L.; Soedamah-Muthu, S.S. Effect of cheese consumption on blood lipids: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2015, 73, 259–275. [Google Scholar] [CrossRef]
- Miller, M.; Stone, N.J.; Ballantyne, C.; Bittner, V.; Criqui, M.H.; Ginsberg, H.N.; Goldberg, A.C.; Howard, W.J.; Jacobson, M.S.; Kris-Etherton, P.M.; et al. Triglycerides and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2011, 123, 2292–2333. [Google Scholar] [CrossRef] [Green Version]
- Williamson, D.A.; Geiselman, P.J.; Lovejoy, J.; Greenway, F.; Volaufova, J.; Martin, C.K.; Arnett, C.; Ortego, L. Effects of consuming mycoprotein, tofu or chicken upon subsequent eating behaviour, hunger and safety. Appetite 2006, 46, 41–48. [Google Scholar] [CrossRef]
- Seidelmann, S.B.; Claggett, B.; Cheng, S.; Henglin, M.; Shah, A.; Steffen, L.M.; Folsom, A.R.; Rimm, E.B.; Willett, W.C.; Solomon, S.D. Dietary carbohydrate intake and mortality: A prospective cohort study and meta-analysis. Lancet Public Health 2018, 3, e419–e428. [Google Scholar] [CrossRef] [Green Version]
- Hu, E.A.; Pan, A.; Malik, V.; Sun, Q. White rice consumption and risk of type 2 diabetes: Meta-analysis and systematic review. BMJ 2012, 344, e1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boers, H.M.; Jack, S.T.H.; David, J.M. A systematic review of the influence of rice characteristics and processing methods on postprandial glycaemic and insulinaemic responses. Br. J. Nutr. 2015, 114, 1035–1045. [Google Scholar] [CrossRef] [PubMed]
- Diehl, A.M. Obesity and alcoholic liver disease. Alcohol 2004, 34, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Perna, S.; Spadaccini, D.; Nichetti, M.; Avanzato, I.; Faliva, M.A.; Rondanelli, M. Osteosarcopenic visceral obesity and osteosarcopenic subcutaneous obesity, two new phenotypes of sarcopenia: Prevalence, metabolic profile, and risk factors. J. Aging Res. 2018, 2018, 6147426. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | (Median IQR) | |
|---|---|---|
| Age (Years) | 65 ± 10 | |
| BMI (kg/m) | 33.49 ± 6.11 | |
| (n; %) | ||
| Gender | Male | 62 (41.1) |
| Female | 89 (58.9) | |
| Education | Below Secondary School Certificate | 26 (17.2) |
| Secondary School Certificate | 29 (19.2) | |
| Diploma Degree | 10 (6.6) | |
| Bachelor’s Degree (BSc) | 7 (4.6) | |
| Master’s Degree (MSc) | 1 (0.7) | |
| Doctorate (PhD) | 1 (0.7) | |
| Non-respondent | 77 (51) | |
| Metabolic Syndrome Family History | Yes | 12 (7.9) |
| No | 37 (24.5) | |
| Do not know | 25 (16.6) | |
| Non-respondent | 77 (51) | |
| Fatty liver | Yes | 54 (89) |
| No | 7 (11) |
| Latest SBP | Latest DBP | BMI | HDL | Triglycerides | Glucose | |
|---|---|---|---|---|---|---|
| Fish | 0.071 | −0.056 | −0.135 | 0.052 | 0.014 | 0.126 |
| Chicken | 0.031 | 0.087 | −0.273 ** | −0.120 | 0.043 | −0.059 |
| Processed Meat | 0.075 | 0.064 | −0.124 | −0.140 | −0.007 | 0.006 |
| Beef | −0.036 | −0.195 | −0.072 | 0.122 | −0.013 | 0.069 |
| Lamb | 0.097 | −0.061 | −0.016 | 0.087 | 0.092 | 0.052 |
| Legumes | 0.023 | 0.019 | −0.154 | −0.066 | 0.039 | −0.071 |
| Eggs | −0.018 | 0.074 | −0.130 | −0.182 | 0.121 | 0.041 |
| Rice | −0.035 | −0.112 | −0.078 | 0.000 | −0.037 | −0.199 * |
| Dairy products (Full fat) | −0.013 | 0.112 | −0.012 | −0.016 | 0.050 | −0.053 |
| Dairy products (Low fat) | 0.182 * | 0.060 | −0.195 * | 0.024 | 0.110 | 0.045 |
| Ricotta or goat cheese | −0.171 | −0.060 | 0.140 | −0.021 | 0.206 * | 0.058 |
| Cheddar cheese | 0.009 | −0.024 | −0.097 | −0.175 | 0.195 * | 0.099 |
| Cream cheese | 0.022 | −0.135 | −0.109 | 0.007 | −0.032 | −0.051 |
| Butter/Mayonnaise | 0.026 | −0.043 | 0.076 | −0.109 | 0.032 | 0.132 |
| Vegetable oil | −0.072 | −0.046 | −0.038 | −0.025 | −0.037 | 0.042 |
| Olives | 0.055 | −0.046 | −0.130 | −0.014 | 0.019 | 0.016 |
| Fruits | 0.098 | −0.003 | −0.102 | −0.026 | 0.011 | 0.064 |
| Vegetables | 0.189 | −0.008 | −0.054 | 0.090 | −0.061 | −0.020 |
| Nuts and dried fruits | 0.005 | −0.066 | −0.027 | −0.063 | −0.047 | 0.063 |
| Dates | 0.149 | 0.086 | −0.098 | 0.105 | 0.059 | −0.123 |
| Desserts | 0.025 | 0.008 | −0.100 | −0.090 | 0.155 | 0.040 |
| Traditional sweets: | 0.135 | 0.029 | 0.006 | 0.064 | 0.029 | 0.052 |
| Chips | 0.043 | −0.060 | 0.025 | 0.026 | −0.059 | 0.058 |
| Hamburgers | −0.017 | 0.039 | −0.084 | −0.052 | −0.003 | 0.071 |
| Shawarma | −0.025 | 0.036 | −0.169 | −0.170 | −0.003 | 0.053 |
| Pizzas and pies | 0.073 | 0.085 | −0.006 | −0.009 | 0.145 | 0.108 |
| Falafel sandwiches | 0.129 | 0.089 | −0.103 | −0.099 | 0.126 | 0.010 |
| French fries | 0.004 | 0.136 | 0.020 | −0.014 | 0.022 | 0.127 |
| Sambosa | 0.098 | 0.184 | −0.122 | −0.002 | 0.017 | 0.051 |
| Carbonated beverages | 0.125 | 0.020 | 0.017 | −0.048 | −0.030 | 0.011 |
| Alcoholic drinks | 0.030 | −0.101 | 0.151 | 0.111 | 0.005 | −0.091 |
| Hot drinks: tea, coffee | −0.055 | 0.116 | 0.035 | −0.129 | −0.079 | −0.054 |
| Variable | βeta | Bias | p Value |
|---|---|---|---|
| Fish | 0.84 | 7.648 b | 0.298 |
| Chicken | −53.68 | 42.085 b | 0.484 |
| Processed Meat | −154.07 | 163.977 b | 0.405 |
| Beef | 203.89 | −233.279 b | 0.915 |
| Lamb | −167.08 | 156.712 b | 0.956 |
| Legumes lentil peas beans | 207.25 | −210.479 b | 0.304 |
| Eggs | −74.03 | 69.987 b | 0.147 |
| Rice | −28.87 | 36.894 b | 0.460 |
| Dairy products Full fat | −35.00 | 25.043 b | 0.179 |
| Dairy products Low fat | −43.46 | 57.801 b | 0.247 |
| Ricotta or goat cheese | −70.95 | 72.593 b | 0.270 |
| Cheddar cheese | 98.19 | −97.082 b | 0.617 |
| Cream cheese | 41.53 | −19.240 b | 0.034 ** |
| Butter Mayonnaise | −42.76 | 45.696 b | 0.241 |
| Vegetable oil | 70.56 | −73.003 b | 0.753 |
| Olives | −33.16 | 36.963 b | 0.747 |
| Fruits | −59.59 | 49.281 b | 0.549 |
| Vegetables | 100.52 | −118.915 b | 0.956 |
| Nuts | 83.13 | −60.547 b | 0.898 |
| Dates | −92.48 | 91.305 b | 0.102 |
| Dessert | −7.73 | 4.916 b | 0.553 |
| Traditional sweets | −247.35 | 247.516 b | 0.935 |
| Chips | −79.85 | 78.675 b | 0.651 |
| Hamburgers | 10.69 | −11.075 b | 0.175 |
| Shawarma | 82.29 | −82.093 b | 0.132 |
| Pizzas and pies | 192.56 | −192.560 b | 0.701 |
| Falafels | 1.82 | −1.820 b | 0.753 |
| French fries | −3.74 | 3.741 b | 0.343 |
| Sambosa | 42.10 | −42.099 b | 1.000 |
| Carbonated beverages and juices | 3.80 | −3.802 b | 0.678 |
| Alcoholic drinks | −46.00 | 46.002 b | 0.701 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perna, S.; Hammad, L.H.; Mohamed, M.W.; Alromaihi, D.; Alhammadi, M.; Al-Khater, N.; Alchuban, A.R.; Aledrisy, M.A.; Ilyas, Z.; Alalwan, T.A.; et al. Cheese Intake Exhibits an Alteration of Glycolipid Profile and Impacts on Non-Alcoholic Fatty Liver in Bahraini Older Adults. Geriatrics 2022, 7, 75. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040075
Perna S, Hammad LH, Mohamed MW, Alromaihi D, Alhammadi M, Al-Khater N, Alchuban AR, Aledrisy MA, Ilyas Z, Alalwan TA, et al. Cheese Intake Exhibits an Alteration of Glycolipid Profile and Impacts on Non-Alcoholic Fatty Liver in Bahraini Older Adults. Geriatrics. 2022; 7(4):75. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040075
Chicago/Turabian StylePerna, Simone, Layla H. Hammad, Mohamed Wael Mohamed, Dalal Alromaihi, Mariam Alhammadi, Noora Al-Khater, Anas Rashed Alchuban, Mawadh Ali Aledrisy, Zahra Ilyas, Tariq A. Alalwan, and et al. 2022. "Cheese Intake Exhibits an Alteration of Glycolipid Profile and Impacts on Non-Alcoholic Fatty Liver in Bahraini Older Adults" Geriatrics 7, no. 4: 75. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040075