
Comparative Outcomes and Surgical Timing for Operative Fragility Hip Fracture Patients during the COVID-19 Pandemic: A Retrospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
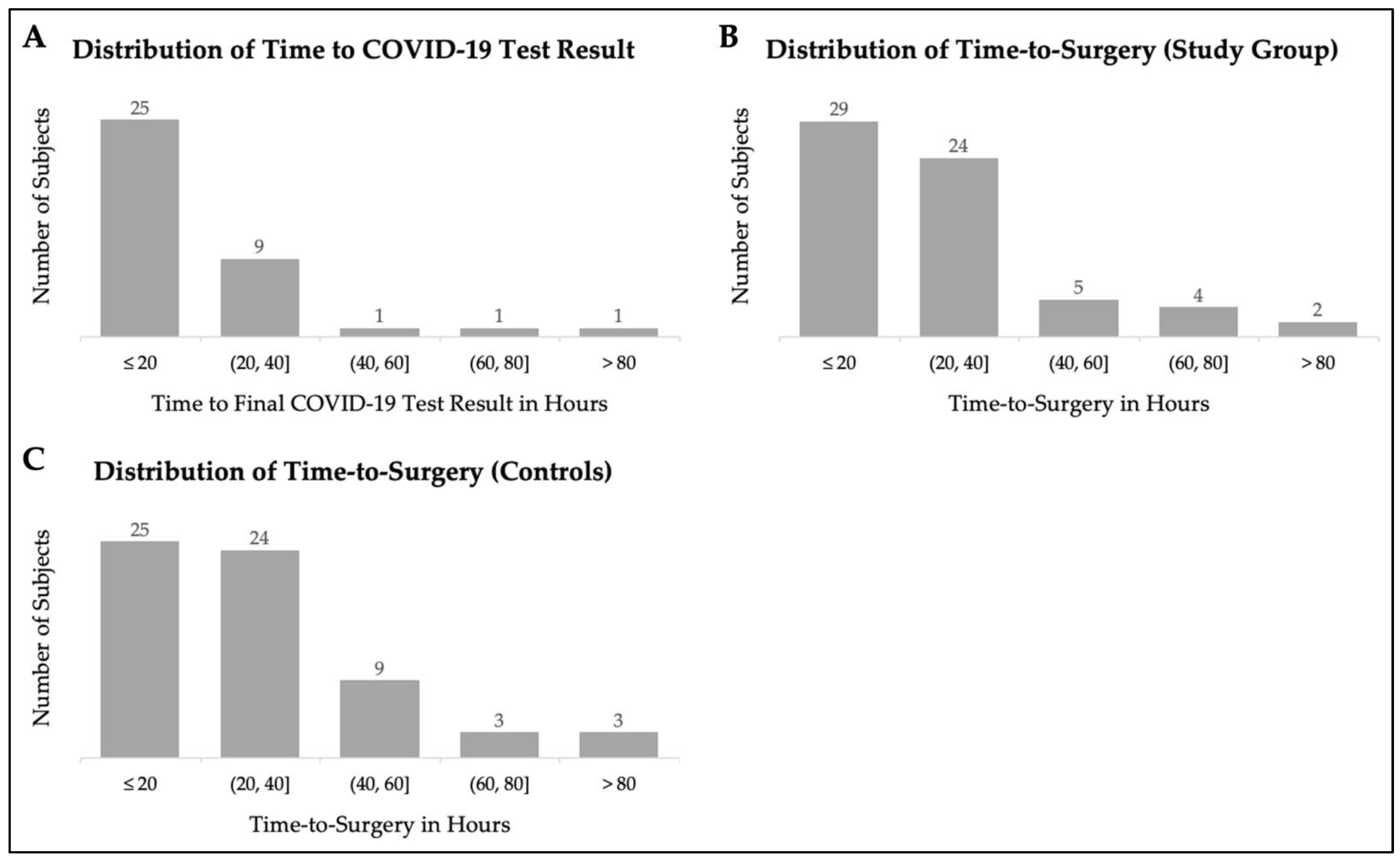
3.2. COVID-19 Testing and Time-to-Surgery
3.3. Surgical and Anesthesia Characteristics
3.4. Outcomes, Length-of-Stay, and Discharge Disposition
3.5. Subgroup Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ogliari, G.; Lunt, E.; Ong, T.; Marshall, L.; Sahota, O. The Impact of Lockdown during the COVID-19 Pandemic on Osteoporotic Fragility Fractures: An Observational Study. Arch. Osteoporos. 2020, 15, 156. [Google Scholar] [CrossRef] [PubMed]
- Cheruvu, M.S.; Bhachu, D.S.; Mulrain, J.; Resool, S.; Cool, P.; Ford, D.J.; Singh, R.A. Effect of COVID-19 on a Rural Orthopaedic Hip Fracture Service. Bone Jt. Open 2020, 1, 500–507. [Google Scholar] [CrossRef]
- Craig, J.; Maguire, M.; Shevlin, S.P.; Black, N.D. The Effects of COVID-19 on Hip Fracture Management and Mortality in a Regional Trauma Centre. Anaesthesia 2020, 76, 710–711. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, M.; Dupley, L.; Unsworth, R.; Boden, R. Where Did All the Trauma Go? A Rapid Review of the Demands on Orthopaedic Services at a UK Major Trauma Centre during the COVID-19 Pandemic. Int. J. Clin. Pract. 2020, 75, e13690. [Google Scholar] [CrossRef] [PubMed]
- Haskel, J.D.; Lin, C.C.; Kaplan, D.J.; Dankert, J.F.; Merkow, D.; Crespo, A.; Behery, O.; Ganta, A.; Konda, S.R. Hip Fracture Volume Does Not Change at a New York City Level 1 Trauma Center During a Period of Social Distancing. Geriatr. Orthop. Surg. Rehabil. 2020, 11, 2151459320972674. [Google Scholar] [CrossRef]
- Ishii, K.; Kurozumi, T.; Suzuki, T.; Matsui, K.; Inui, T.; Nakayama, Y.; Yamashita, S.; Takahashi, S.; Nakagawa, T.; Suzuki, J.; et al. Impact of the COVID-19 Pandemic on a Trauma Center of a University Hospital in Japan. J. Orthop. Sci. 2021, 27, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Karia, M.; Gupta, V.; Zahra, W.; Dixon, J.; Tayton, E. The Effect of COVID-19 on the Trauma Burden, Theatre Efficiency and Training Opportunities in a District General Hospital. Bone Jt. Open 2020, 1, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Nuñez, J.H.; Sallent, A.; Lakhani, K.; Guerra-Farfan, E.; Vidal, N.; Ekhtiari, S.; Minguell, J. Impact of the COVID-19 Pandemic on an Emergency Traumatology Service: Experience at a Tertiary Trauma Centre in Spain. Injury 2020, 51, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Biarnés-Suñé, A.; Solà-Enríquez, B.; González Posada, M.; Teixidor-Serra, J.; García-Sánchez, Y.; Manrique Muñóz, S. Impact of the COVID-19 Pandemic on the Mortality of the Elderly Patient with a Hip Fracture. Rev. Esp. Anestesiol. Reanim. 2021, 68, 65–72. [Google Scholar] [CrossRef] [PubMed]
- De, C.; Wignall, A.; Giannoudis, V.; Jimenez, A.; Sturdee, S.; Aderinto, J.; Pandit, H.; Palan, J.; Gulati, A. Peri-Operative Outcomes and Predictors of Mortality in COVID-19 Positive Patients with Hip Fractures: A Multicentre Study in the UK. Indian J. Orthop. 2020, 54, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.J.; Clement, N.D.; MacLullich, A.M.J.; White, T.O.; Duckworth, A.D. IMPACT-Scot 2 Report on COVID-19 in Hip Fracture Patients. Bone Jt. J. 2021, 103, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Kayani, B.; Onochie, E.; Patil, V.; Begum, F.; Cuthbert, R.; Ferguson, D.; Bhamra, J.S.; Sharma, A.; Bates, P.; Haddad, F.S. The Effects of COVID-19 on Perioperative Morbidity and Mortality in Patients with Hip Fractures. Bone Jt. J. 2020, 102, 1136–1145. [Google Scholar] [CrossRef] [PubMed]
- LeBrun, D.G.; Konnaris, M.A.; Ghahramani, G.C.; Premkumar, A.; Defrancesco, C.J.; Gruskay, J.A.; Dvorzhinskiy, A.; Sandhu, M.S.; Goldwyn, E.M.; Mendias, C.L.; et al. Hip Fracture Outcomes during the COVID-19 Pandemic: Early Results from New York. J. Orthop. Trauma 2020, 34, 403–410. [Google Scholar] [CrossRef]
- Mamarelis, G.; Oduoza, U.; Chekuri, R.; Estfan, R.; Greer, T. Mortality in Patients with Proximal Femoral Fracture During the COVID-19 Pandemic. JBJS Open Access 2020, 5, e20.00086. [Google Scholar] [CrossRef] [PubMed]
- Muñoz Vives, J.M.; Jornet-Gibert, M.; Cámara-Cabrera, J.; Esteban, P.L.; Brunet, L.; Delgado-Flores, L.; Camacho-Carrasco, P.; Torner, P.; Marcano-Fernández, F. Mortality Rates of Patients with Proximal Femoral Fracture in a Worldwide Pandemic: Preliminary Results of the Spanish HIP-COVID Observational Study. J. Bone Jt. Surg. Am. 2020, 102, e69. [Google Scholar] [CrossRef]
- Rasidovic, D.; Ahmed, I.; Thomas, C.; Kimani, P.K.-U.; Wall, P.; Mangat, K. Impact of COVID-19 on Clinical Outcomes for Patients with Fractured Hip: A Multicentre Observational Cohort Study. Bone Jt. Open 2020, 1, 697–705. [Google Scholar] [CrossRef]
- Ward, A.E.; Tadross, D.; Wells, F.; Majkowski, L.; Naveed, U.; Jeyapalan, R.; Partridge, D.G.; Madan, S.; Blundell, C.M. The Impact of COVID-19 on Morbidity and Mortality in Neck of Femur Fracture Patients. Bone Jt. Open 2020, 1, 669–675. [Google Scholar] [CrossRef]
- Clement, N.D.; Ng, N.; Simpson, C.J.; Patton, R.F.L.; Hall, A.J.; Simpson, A.H.R.W.; Duckworth, A.D. The Prevalence, Mortality, and Associated Risk Factors for Developing COVID-19 in Hip Fracture Patients: A Systematic Review and Meta-Analysis. Bone Jt. Res. 2020, 9, 873–883. [Google Scholar] [CrossRef]
- Lim, M.A.; Pranata, R. Coronavirus Disease 2019 (COVID-19) Markedly Increased Mortality in Patients with Hip Fracture—A Systematic Review and Meta-Analysis. J. Clin. Orthop. Trauma 2020, 12, 187–193. [Google Scholar] [CrossRef]
- Wang, K.C.; Xiao, R.; Cheung, Z.B.; Barbera, J.P.; Forsh, D.A. Early Mortality after Hip Fracture Surgery in COVID-19 Patients: A Systematic Review and Meta-Analysis. J. Orthop. 2020, 22, 584–591. [Google Scholar] [CrossRef]
- Raheman, F.J.; Rojoa, D.M.; Nayan Parekh, J.; Berber, R.; Ashford, R. Meta-Analysis and Metaregression of Risk Factors Associated with Mortality in Hip Fracture Patients during the COVID-19 Pandemic. Sci. Rep. 2021, 11, 10157. [Google Scholar] [CrossRef] [PubMed]
- Alcock, H.; Moppett, E.A.; Moppett, I.K. Early Mortality Outcomes of Patients with Fragility Hip Fracture and Concurrent SARS-CoV-2 Infection. Bone Jt. Open 2021, 2, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Klestil, T.; Röder, C.; Stotter, C.; Winkler, B.; Nehrer, S.; Lutz, M.; Klerings, I.; Wagner, G.; Gartlehner, G.; Nussbaumer-Streit, B. Impact of Timing of Surgery in Elderly Hip Fracture Patients: A Systematic Review and Meta-Analysis. Sci. Rep. 2018, 8, 13933. [Google Scholar] [CrossRef]
- Tarantino, U.; Cariati, I.; Tancredi, V.; Casamassima, D.; Piccirilli, E.; Iundusi, R.; Gasbarra, E. State of Fragility Fractures Management during the Covid-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7732. [Google Scholar] [CrossRef] [PubMed]
- Upadhyaya, G.K.; Iyengar, K.; Jain, V.K.; Vaishya, R. Challenges and Strategies in Management of Osteoporosis and Fragility Fracture Care during COVID-19 Pandemic. J. Orthop. 2020, 21, 287–290. [Google Scholar] [CrossRef]
- Napoli, N.; Elderkin, A.L.; Kiel, D.P.; Khosla, S. Managing Fragility Fractures during the COVID-19 Pandemic. Nat. Rev. Endocrinol. 2020, 16, 467–468. [Google Scholar] [CrossRef]
- Slullitel, P.A.; Lucero, C.M.; Soruco, M.L.; Barla, J.D.; Benchimol, J.A.; Boietti, B.R.; Zanotti, G.; Comba, F.; Taype-Zamboni, D.R.; Carabelli, G.S.; et al. Prolonged Social Lockdown during COVID-19 Pandemic and Hip Fracture Epidemiology. Int. Orthop. 2020, 44, 1887–1895. [Google Scholar] [CrossRef]
- Segarra, B.; Ballesteros Heras, N.; Viadel Ortiz, M.; Ribes-Iborra, J.; Martinez-Macias, O.; Cuesta-Peredo, D. Are Hospitals Safe? A Prospective Study on SARS-CoV-2 Prevalence and Outcome on Surgical Fracture Patients: A Closer Look at Hip Fracture Patients. J. Orthop. Trauma 2020, 34, e371–e376. [Google Scholar] [CrossRef]
- Tripathy, S.K.; Varghese, P.; Panigrahi, S.; Panda, B.B.; Velagada, S.; Sahoo, S.S.; Naik, M.A.; Rao, S.K. Thirty-Day Mortality of Patients with Hip Fracture during COVID-19 Pandemic and Pre-Pandemic Periods: A Systematic Review and Metaanalysis. World J. Orthop. 2021, 12, 35–50. [Google Scholar] [CrossRef]
- Egol, K.A.; Konda, S.R.; Bird, M.L.; Dedhia, N.; Landes, E.K.; Ranson, R.A.; Solasz, S.J.; Aggarwal, V.K.; Bosco, J.A.; Furgiuele, D.L.; et al. Increased Mortality and Major Complications in Hip Fracture Care during the COVID-19 Pandemic: A New York City Perspective. J. Orthop. Trauma 2020, 34, 395–402. [Google Scholar] [CrossRef]
- Jarvis, S.; Salottolo, K.; Madayag, R.; Pekarek, J.; Nwafo, N.; Wessel, A.; Duane, T.; Roberts, Z.; Lieser, M.; Corrigan, C.; et al. Delayed Hospital Admission for Traumatic Hip Fractures during the COVID-19 Pandemic. J. Orthop. Surg. Res. 2021, 16, 237. [Google Scholar] [CrossRef] [PubMed]
- Zhong, H.; Poeran, J.; Liu, J.; Wilson, L.A.; Memtsoudis, S.G. Hip Fracture Characteristics and Outcomes during COVID-19: A Large Retrospective National Database Review. Br. J. Anaesth. 2021, 127, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Crozier-Shaw, G.; Hughes, A.J.; Conlon, B.; Sheehan, E.; Merghani, K. Hip Fracture Care during Covid-19: A Regional Trauma Centre’s Experience. Ir. J. Med. Sci. 2021, 190, 1275–1280. [Google Scholar] [CrossRef] [PubMed]
- Narang, A.; Chan, G.; Aframian, A.; Ali, Z.; Carr, A.; Goodier, H.; Morgan, C.; Park, C.; Sugand, K.; Walton, T.; et al. Thirty-Day Mortality Following Surgical Management of Hip Fractures during the COVID-19 Pandemic: Findings from a Prospective Multi-Centre UK Study. Int. Orthop. 2021, 45, 23–31. [Google Scholar] [CrossRef]
- Dupley, L.; Oputa, T.J.; Bourne, J.T.; Lum, J.; Hodhody, G.; Rogers, S.; Mcloughlin, K.; Murphy, L.; Konarski, A.; Almari, F.; et al. 30-Day Mortality for Fractured Neck of Femur Patients with Concurrent COVID-19 Infection. Eur. J. Orthop. Surg. Traumatol. 2020, 31, 341–347. [Google Scholar] [CrossRef]
- Macey, A.R.M.; Butler, J.; Martin, S.C.; Tan, T.Y.; Leach, W.J.; Jamal, B. 30-Day Outcomes in Hip Fracture Patients during the COVID-19 Pandemic Compared to the Preceding Year. Bone Jt. Open 2020, 1, 415–419. [Google Scholar] [CrossRef]
- Malik-Tabassum, K.; Crooks, M.; Robertson, A.; To, C.; Maling, L.; Selmon, G. Management of Hip Fractures during the COVID-19 Pandemic at a High-Volume Hip Fracture Unit in the United Kingdom. J. Orthop. 2020, 20, 332–337. [Google Scholar] [CrossRef]
- Arafa, M.; Nesar, S.; Abu-Jabeh, H.; Jayme, M.O.R.; Kalairajah, Y. COVID-19 Pandemic and Hip Fractures: Impact and Lessons Learned. Bone Jt. Open 2020, 1, 530–540. [Google Scholar] [CrossRef]
- Meinberg, E.G.; Agel, J.; Roberts, C.S.; Karam, M.D.; Kellam, J.F. Fracture and Dislocation Classification Compendium-2018. J. Orthop. Trauma 2018, 32, S1–S10. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Thakrar, A.; Chui, K.; Kapoor, A.; Hambidge, J. Thirty-Day Mortality Rate of Patients with Hip Fractures during the COVID-19 Pandemic: A Single Centre Prospective Study in the United Kingdom. J. Orthop. Trauma 2020, 34, e325–e329. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.J.; Clement, N.D.; MacLullich, A.M.J.; Ojeda-Thies, C.; Hoefer, C.; Brent, L.; White, T.O.; Duckworth, A.D. IMPACT of COVID-19 on Hip Fracture Services: A Global Survey by the International Multicentre Project Auditing COVID-19 in Trauma & Orthopaedics. Surgeon 2021, 20, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.V.; Musbahi, O.; Singh, A.; Somashekar, N.; Huber, C.P.; Wiik, A.V. Increased Perioperative Mortality for Femoral Neck Fractures in Patients with Coronavirus Disease 2019 (COVID-19): Experience from the United Kingdom during the First Wave of the Pandemic. Patient Saf. Surg. 2021, 15, 8. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Sugand, K.; Aframian, A.; Morgan, C.; Pakroo, N.; Gibbons, C.; Fertleman, M.; Nathwani, D.; Bhattacharya, R.; Sarraf, K.M. Impact of COVID-19 Pandemic on Hip Fractures: The Central London Experience COVID-Related Urgent Geriatric Hip Trauma (COUGH) Study COVERT (COVid Emergency-Related Trauma and Orthopaedics) Collaborative. Ir. J. Med. Sci. 2021, 191, 1005–1012. [Google Scholar] [CrossRef]
- Amzallag, N.; Factor, S.; Shichman, I.; Ben-Tov, T.; Khoury, A. Hip Fractures during the COVID-19 Pandemic: Demographics, Treatment Pathway, and Outcomes. Isr. Med. Assoc. J. 2021, 23, 484–489. [Google Scholar]
- Bub, C.D.; Larsen, C.G.; Heimroth, J.; Aziz, H.; Pinpin, C.; Intravia, J.M.; Goldman, A. Hip Fracture Trends and Outcomes during the COVID-19 Pandemic. Orthopedics 2021, 44, 293–298. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Study Group (n = 64) | Controls (n = 64) | p-Value |
|---|---|---|---|
| Female sex | 72% (46) | 72% (46) | 1.00 |
| Age (years (SD) | 81.1 ±10.9 | 80.9 ± 10.1 | 0.95 |
| Body mass index (BMI) (kg/m2 ± SD) * | 23.8 ±4.4 | 26.0 ± 4.5 | 0.14 |
| White race/ethnicity ^ | 92% (56) | 92% (58) | 0.96 |
| DNR/DNI orders | 22% (14) | 33% (21) | 0.17 |
| Intertrochanteric fracture | 50% (32) | 52% (33) | 0.66 |
| Intracapsular fracture | 44% (28) | 41% (26) | |
| Subtrochanteric fracture | 5% (3) | 8% (5) | |
| Other fracture | 2% (1) | 0% (0) | |
| Intramedullary nailing | 50% (32) | 50% (32) | 1.00 |
| Open reduction and internal fixation | 8% (5) | 8% (5) | |
| Total hip arthroplasty | 11% (7) | 11% (7) | |
| Hemiarthroplasty | 25% (16) | 25% (16) | |
| Percutaneous pinning | 6% (4) | 6% (4) |
| Comorbidity | Study Group (n = 64) | Controls (n = 64) | p-Value |
|---|---|---|---|
| ASA Score | 3 | 3 | 1.00 |
| CCI (mean ± standard deviation) | 6.78 ± 2.84 | 6.56 ± 2.52 | 0.65 |
| Congestive heart failure * | 30% (19) | 25% (16) | 0.55 |
| Prior myocardial infarction | 16% (10) | 23% (15) | 0.26 |
| Hypertension | 81% (52) | 89% (57) | 0.21 |
| Prior stroke or transient ischemic attack | 27% (17) | 28% (18) | 0.84 |
| Peripheral vascular disease | 17% (11) | 11% (7) | 0.31 |
| Obesity | 19% (12) | 22% (14) | 0.66 |
| Diabetes mellitus | 30% (18) | 36% (23) | 0.34 |
| Asthma | 19% (12) | 11% (7) | 0.21 |
| Chronic obstructive pulmonary disease | 20% (13) | 16% (10) | 0.49 |
| Liver disease | 2% (1) | 6% (4) | 0.17 |
| Severe chronic kidney disease | 8% (5) | 3% (2) | 0.24 |
| Leukemia | 0% (0) | 2% (1) | 0.32 |
| Lymphoma | 6% (4) | 2% (1) | 0.17 |
| Solid tumor | 38% (24) | 31% (20) | 0.46 |
| Dementia | 30% (19) | 33% (21) | 0.70 |
| Osteoporosis | 42% (27) | 48% (31) | 0.48 |
| Connective tissue disease | 11% (7) | 11% (7) | 1.00 |
| Complication | Study Group (n = 64) | Controls (n = 64) | p-Value |
|---|---|---|---|
| Emergency department visits | 19% (12) | 30% (19) | 0.15 |
| Readmissions | 16% (10) | 17% (11) | 0.81 |
| Reoperation | 2% (1) | 2% (1) | 1.00 |
| Any complication | 38% (24) | 45% (29) | 0.37 |
| Surgical site infection | 2% (1) | 2% (1) | 1.00 |
| Gastrointestinal complications (vomiting) | 8% (5) | 5% (3) | 0.47 |
| Pneumonia | 11% (7) | 9% (6) | 0.77 |
| Myocardial infarction | 5% (3) | 3% (2) | 0.65 |
| Stroke | 2% (1) | 2% (1) | 1.00 |
| Sepsis | 5% (3) | 5% (3) | 1.00 |
| Severe bleeding | 9% (6) | 5% (3) | 0.30 |
| Congestive heart failure | 6% (4) | 6% (4) | 1.00 |
| Venous thromboembolism | 3% (2) | 5% (3) | 0.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rowe, K.A.; Kim, K.; Varady, N.H.; Heng, M.; von Keudell, A.G.; Weaver, M.J.; Abdeen, A.; Rodriguez, E.K.; Chen, A.F. Comparative Outcomes and Surgical Timing for Operative Fragility Hip Fracture Patients during the COVID-19 Pandemic: A Retrospective Cohort Study. Geriatrics 2022, 7, 84. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040084
Rowe KA, Kim K, Varady NH, Heng M, von Keudell AG, Weaver MJ, Abdeen A, Rodriguez EK, Chen AF. Comparative Outcomes and Surgical Timing for Operative Fragility Hip Fracture Patients during the COVID-19 Pandemic: A Retrospective Cohort Study. Geriatrics. 2022; 7(4):84. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040084
Chicago/Turabian StyleRowe, Katherine A., Kiryung Kim, Nathan H. Varady, Marilyn Heng, Arvind G. von Keudell, Michael J. Weaver, Ayesha Abdeen, Edward K. Rodriguez, and Antonia F. Chen. 2022. "Comparative Outcomes and Surgical Timing for Operative Fragility Hip Fracture Patients during the COVID-19 Pandemic: A Retrospective Cohort Study" Geriatrics 7, no. 4: 84. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040084