
The Atherosclerotic Profile of a Young Symptomatic Population between 19 and 49 Years: Coronary Computed Tomography Angiography or Coronary Artery Calcium Score?

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
- The coronary stenosis severity was scored qualitatively according to the CAD-RADSTM score (0–5) as minimal (1) <25%, mild (2) 25–49.9%, moderate (3) 50–69.9%, severe (4) ≥70–99% and (5) occluded 100% [15] on a per-coronary segment-base (AHA-modified-17-segment classification)
- High-risk plaque (HRP) analysis: Low attenuation plaque (LAP) was defined as hypoattenuating lesion with <150 Housfield Units (HU). CT-density was screened with the “pixel lens” and the lowest HU recorded [8]. Then, a region-of-interest (ROI) of approximately 2 mm2 size was placed at the region of lowest density and drawn as large as possible, while sparing areas affected by artifacts or adjacent to calcifications and the CT-attenuation (HU) quantified. If a patient had multiple lesions, the one with the lowest HU was selected for a patient-based analysis. Low-attenuation plaque (LAP) was stratified into LAP < 90 HU, <60 HU (fibrofatty) [10], and LAP < 30 HU (lipid-rich necrotic core) [6,9]. The napkin-ring sign was defined as an outer high-density rim with an inner hypodense area [7]. Spotty calcification was defined as a calcification of less than 3 mm size. The remodeling index was calculated as the ratio of the maximal cross-sectional lumen of the plaque diameter and its closed proximal (or distal, e.g., in case of ostial lesions) normal reference vessel lumen diameter. Positive remodeling was defined as remodeling index > 1.1.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Carr, J.J.; Jacobs, D.R.; Terry, J.G.; Shay, C.M.; Sidney, S.; Liu, K.; Schreiner, P.J.; Lewis, C.E.; Shikany, J.M.; Reis, J.P.; et al. Association of Coronary Artery Calcium in Adults Aged 32 to 46 Years With Incident Coronary Heart Disease and Death. JAMA Cardiol. 2017, 2, 391–399. [Google Scholar] [CrossRef]
- Miedema, M.D.; Dardari, Z.A.; Nasir, K.; Blankstein, R.; Knickelbine, T.; Oberembt, S.; Shaw, L.; Rumberger, J.; Michos, E.D.; Rozanski, A.; et al. Association of Coronary Artery Calcium With Long-term, Cause-Specific Mortality Among Young Adults. JAMA Netw. Open 2019, 2, e197440. [Google Scholar] [CrossRef] [PubMed]
- Greenland, P.; Alpert, J.S.; Beller, G.A.; Benjamin, E.J.; Budoff, M.J.; Fayad, Z.A.; Foster, E.; Hlatky, M.A.; Hodgson, J.M.; Kushner, F.G.; et al. 2010 ACCF/AHA Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the American Society of Echocardiography, American Society of Nuclear Cardiology, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance. J. Am. Coll. Cardiol. 2010, 56, 2182–2199. [Google Scholar]
- Blaha, M.J.; Cainzos-Achirica, M.; Dardari, Z.; Blankstein, R.; Shaw, L.J.; Rozanski, A.; Rumberger, J.A.; Dzaye, O.; Michos, E.D.; Berman, D.S.; et al. All-cause and cause-specific mortality in individuals with zero and minimal coronary artery calcium: A long-term, competing risk analysis in the Coronary Artery Calcium Consortium. Atherosclerosis 2019, 294, 72–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferencik, M.; Mayrhofer, T.; Bittner, D.O.; Emami, H.; Puchner, S.B.; Lu, M.T.; Meyersohn, N.M.; Ivanov, A.V.; Adami, E.C.; Patel, M.R.; et al. Use of High-Risk Coronary Atherosclerotic Plaque Detection for Risk Stratification of Patients With Stable Chest Pain: A Secondary Analysis of the PROMISE Randomized Clinical Trial. JAMA Cardiol. 2018, 3, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.C.; Kwiecinski, J.; Doris, M.; McElhinney, P.; D’Souza, M.S.; Cadet, S.; Adamson, P.D.; Moss, A.J.; Alam, S.; Hunter, A.; et al. Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results from the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the HEART). Circulation 2020, 141, 1452–1462. [Google Scholar] [CrossRef] [Green Version]
- Maurovich-Horvat, P.; Schlett, C.L.; Alkadhi, H.; Nakano, M.; Otsuka, F.; Stolzmann, P.; Scheffel, H.; Ferencik, M.; Kriegel, M.F.; Seifarth, H.; et al. The napkin-ring sign indicates advanced atherosclerotic lesions in coronary CT angiography. JACC Cardiovasc. Imaging 2012, 5, 1243–1252. [Google Scholar] [CrossRef] [Green Version]
- Nakazato, R.; Otake, H.; Konishi, A.; Iwasaki, M.; Koo, B.K.; Fukuya, H.; Shinke, T.; Hirata, K.-i.; Leipsic, J.; Berman, D.S.; et al. Atherosclerotic plaque characterization by CT angiography for identification of high-risk coronary artery lesions: A comparison to optical coherence tomography. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Motoyama, S.; Ito, H.; Sarai, M.; Kondo, T.; Kawai, H.; Nagahara, Y.; Harigaya, H.; Kan, S.; Anno, H.; Takahashi, H.; et al. Plaque Characterization by Coronary Computed Tomography Angiography and the Likelihood of Acute Coronary Events in Mid-Term Follow-Up. J. Am. Coll. Cardiol. 2015, 66, 337–346. [Google Scholar] [CrossRef] [Green Version]
- Feuchtner, G.; Kerber, J.; Burghard, P.; Dichtl, W.; Friedrich, G.; Bonaros, N.; Plank, F. The high-risk criteria low-attenuation plaque <60 HU and the napkin-ring sign are the most powerful predictors of MACE: A long-term follow-up study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 772–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, I.; Chang, H.-J.; Sung, J.M.; Pencina, M.J.; Lin, F.Y.; Dunning, A.M.; Achenbach, S.; Al-Mallah, M.; Berman, D.S.; Budoff, M.J.; et al. CONFIRM Investigators. Coronary computed tomographic angiography and risk of all-cause mortality and nonfatal myocardial infarction in subjects without chest pain syndrome from the CONFIRM Registry (coronary CT angiography evaluation for clinical outcomes: An international multicenter registry). Circulation 2012, 126, 304–313. [Google Scholar]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Jin, K.N.; Chun, E.J.; Lee, C.-H.; Kim, J.A.; Lee, M.S.; Choi, S.I. Subclinical coronary atherosclerosis in young adults: Prevalence, characteristics, predictors with coronary computed tomography angiography. Int J. Cardiovasc. Imaging 2012, 28, 93–100. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Cury, R.C.; Abbara, S.; Achenbach, S.; Agatston, A.; Berman, D.S.; Budoff, M.J.; Dill, K.E.; Jacobs, J.E.; Maroules, C.D.; Rubin, G.D.; et al. CAD-RADS(TM) Coronary Artery Disease-Reporting and Data System. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society of Cardiovascular Imaging (NASCI). J. Cardiovasc. Comput. Tomogr. 2016, 10, 269–281. [Google Scholar] [PubMed] [Green Version]
- Chang, H.-J.; Lin, F.Y.; Lee, S.-E.; Andreini, D.; Bax, J.; Cademartiri, F.; Chinnaiyan, K.; Chow, B.; Conte, E.; Cury, R.C.; et al. Coronary Atherosclerotic Precursors of Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2018, 71, 2511–2522. [Google Scholar] [CrossRef]
- Ferraro, R.A.; Van Rosendael, A.R.; Lu, Y.; Andreini, D.; Al-Mallah, M.H.; Cademartiri, F.; Chinnaiyan, K.; Chow, B.J.W.; Conte, E.; Cury, R.C.; et al. Non-obstructive high-risk plaques increase the risk of future culprit lesions comparable to obstructive plaques without high-risk features: The ICONIC study. Eur. Hear. J. Cardiovasc. Imaging 2020, 21, 973–980. [Google Scholar] [CrossRef]
- Mahmood, T.; Shapiro, M.D. Coronary artery calcium testing in low-intermediate risk symptomatic patients with suspected coronary artery disease: An effective gatekeeper to further testing? PLoS ONE 2020, 15, e0240539. [Google Scholar] [CrossRef] [PubMed]
- Villines, T.C.; Hulten, E.A.; Shaw, L.J.; Goyal, M.; Dunning, A.; Achenbach, S.; Al-Mallah, M.; Berman, D.S.; Budoff, M.J.; Cademartiri, F.; et al. Prevalence and severity of coronary artery disease and adverse events among symptomatic patients with coronary artery calcification scores of zero undergoing coronary computed tomography angiography: Results from the CONFIRM registry. J. Am. Coll. Cardiol. 2011, 58, 2533–2540. [Google Scholar] [CrossRef] [Green Version]
- Naoum, C.; Berman, D.S.; Ahmadi, A.; Blanke, P.; Gransar, H.; Narula, J.; Shaw, L.J.; Kritharides, L.; Achenbach, S.; Al-Mallah, M.H.; et al. Predictive Value of Age- and Sex-Specific Nomograms of Global Plaque Burden on Coronary Computed Tomography Angiography for Major Cardiac Events. Circ. Cardiovasc. Imaging 2017, 10, e004896. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Chun, E.J.; Kim, K.J.; Kim, J.A.; Yoo, J.Y.; Choi, S.I. Asymptomatic subjects with zero coronary calcium score: Coronary CT angiographic features of plaques in event-prone patients. Int. J. Cardiovasc. Imaging 2013, 29, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.-T.; Hou, Z.-H.; Lu, B.; An, Y.-Q.; Gao, Y.; Yin, W.-H.; Ren, X.-S. Prevalence of coronary artery disease in symptomatic patients with zero coronary artery calcium score in different age population. Int. J. Cardiovasc. Imaging 2020, 37, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Hartaigh, B.; Gransar, H.; Lee, J.H.; Rizvi, A.; Baskaran, L.; Schulman-Marcus, J.; Dunning, A.; Achenbach, S.; Al-Mallah, M.H.; et al. Incremental prognostic value of coronary computed tomography angiography over coronary calcium scoring for major adverse cardiac events in elderly asymptomatic individuals. Eur. Hear. J. Cardiovasc. Imaging 2017, 19, 675–683. [Google Scholar]
- Cho, I.; Chang, H.J.; Ó Hartaigh, B.; Shin, S.; Sung, J.M.; Lin, F.Y.; Achenbach, S.; Heo, R.; Berman, D.S.; Budoff, M.J.; et al. Incremental prognostic utility of coronary CT angiography for asymptomatic patients based upon extent and severity of coronary artery calcium: Results from the COronary CT Angiography EvaluatioN For Clinical Outcomes InteRnational Multicenter (CONFIRM) study. Eur. Heart J. 2015, 36, 501–508. [Google Scholar]
- Osei, A.D.; Uddin, S.M.I.; Dzaye, O.; Achirica, M.C.; Dardari, Z.A.; Obisesan, O.H.; Kianoush, S.; Mirbolouk, M.; Orimoloye, O.A.; Shaw, L.; et al. Predictors of coronary artery calcium among 20–30-year-olds: The Coronary Artery Calcium Consortium. Atherosclerosis 2020, 301, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Henzel, J.; Kępka, C.; Kruk, M.; Makarewicz-Wujec, M.; Wardziak, Ł.; Trochimiuk, P.; Dzielińska, Z.; Demkow, M. High-Risk Coronary Plaque Regression after Intensive Lifestyle Intervention in Nonbstructive Coronary Disease: A Randomized Study. JACC Cardiovasc. Imaging 2020, 14, 1192–1202. [Google Scholar] [CrossRef] [PubMed]
- Faletra, F.F.; Klersy, C.; D’Angeli, I.; Penco, M.; Procaccini, V.; Pasotti, E.; Marcolongo, A.; Pedrazzini, G.B.; De Castro, S.; Scappaticci, M.; et al. Relation between coronary atherosclerotic plaques and traditional risk factors in people with no history of cardiovascular disease undergoing multi-detector computed coronary angiography. Heart 2009, 95, 1265–1272. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (y) | 42.4 ± 6.3 (19–49) | |
| Females | 346 (30.4%) | |
| BMI (kg/m2) | 26.1 ± 5.02 | |
| Smoking | 339 (41.5%) | |
| Arterial Hypertension | 303 (37.2%) | |
| Positive Family History | 357 (44.2%) | |
| Dyslipidemia | 358 (45.1%) | |
| Diabetes | 40 (5.2%) | |
| CACS (AU) | 17.5 ± 80.3 (Range, 0–1203.5) | |
| CACS | ||
| 0 | 70.5% | |
| >1.0 AU | 29.5% | |
| CTA-Stenosis Severity (CADRADS) | ||
| 0 | 615 (54.4%) | |
| 1 | 158 (14%) | |
| 2 | 201 (17.8%) | |
| 3 | 71 (6.3%) | |
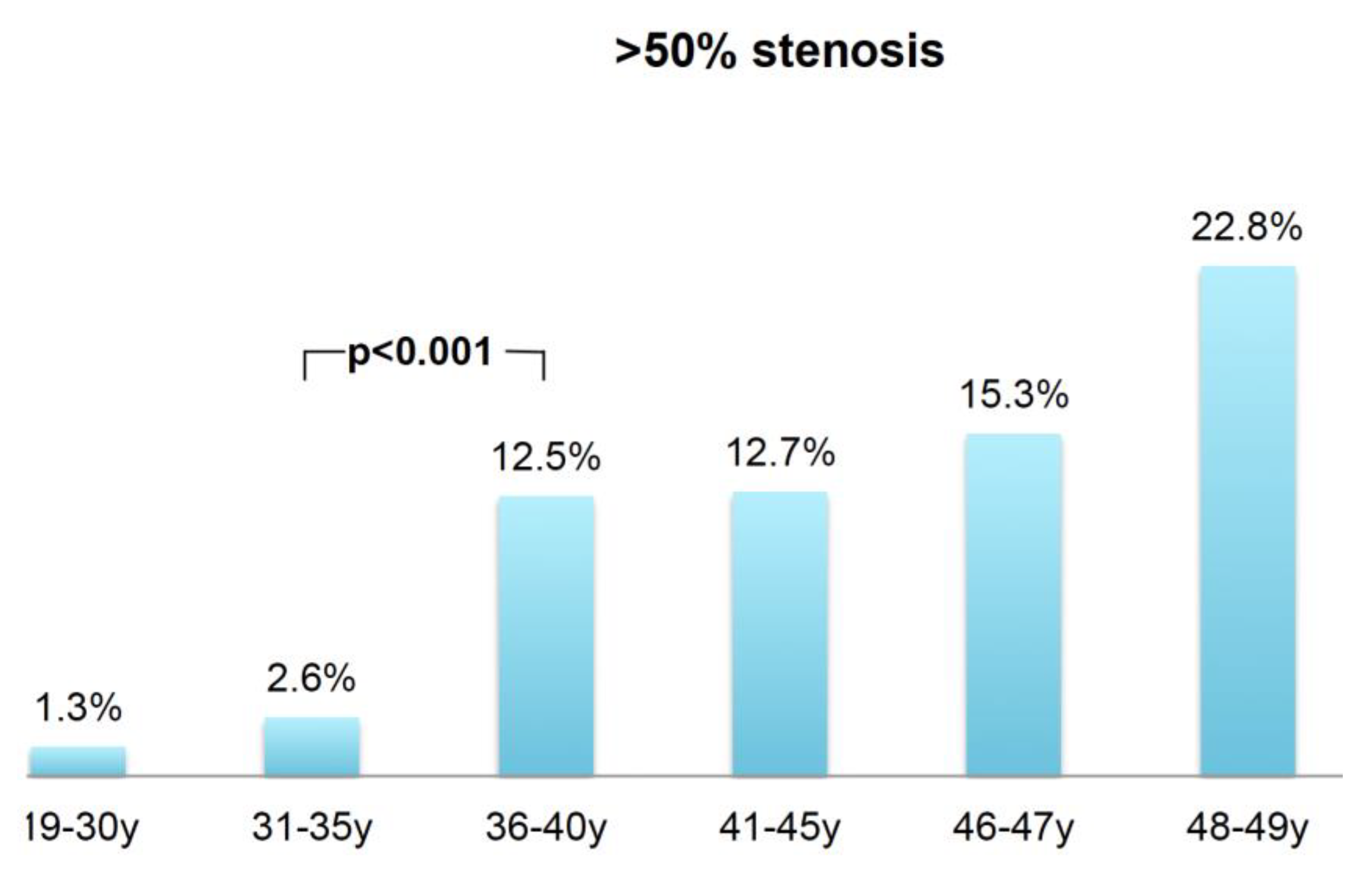
| 4 + 5 | 82 (7.3%) | >50% Stenosis |
| 6/N * | 4 (0.4%) | 13.6% |
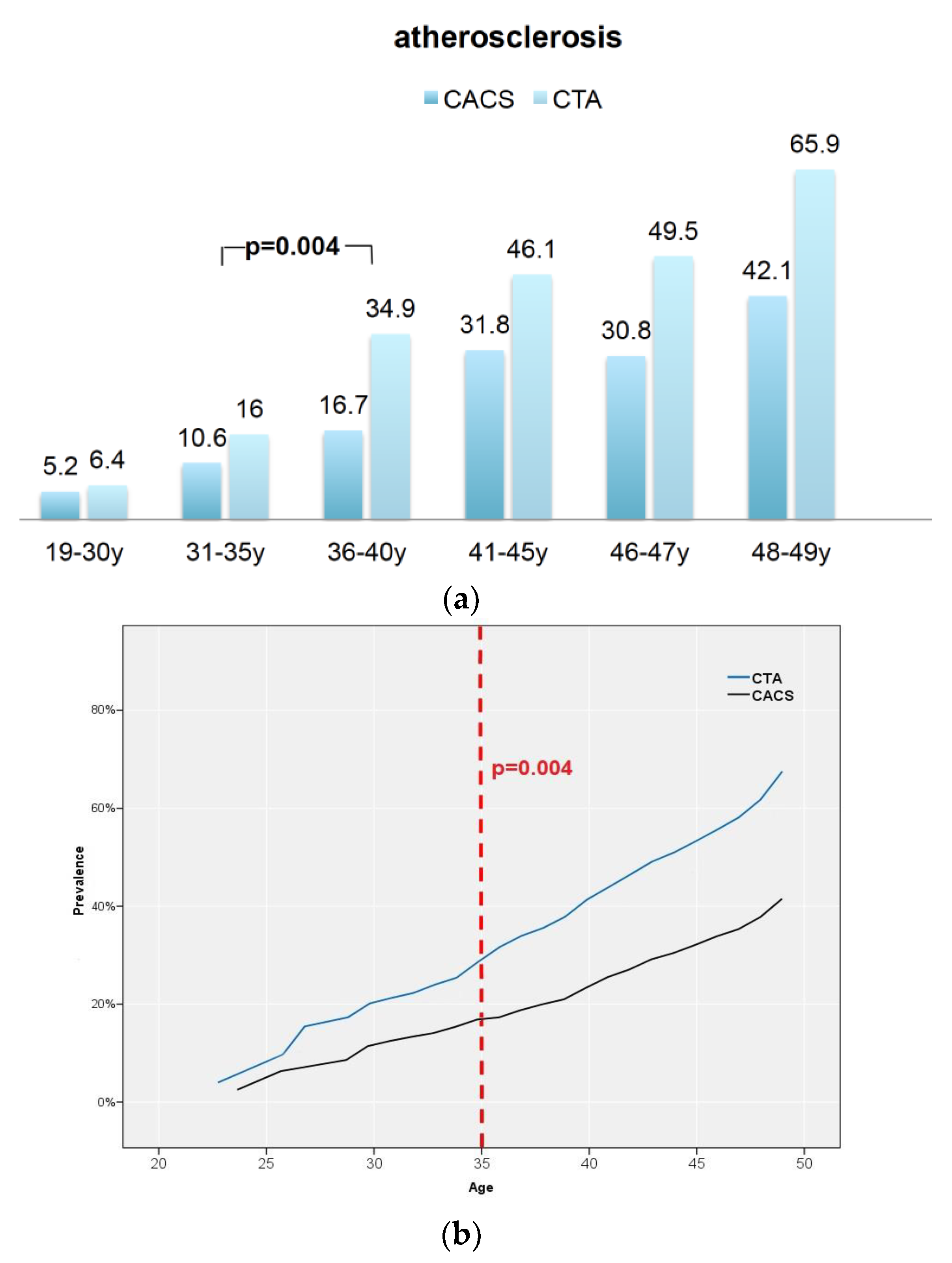
| Atherosclerosis | ||
| CACS | 298 (27.0%) | p < 0.0001 |
| CTA | 512 (45.0%) | OR: 0.44 (95%CI: 0.37–0.53) |
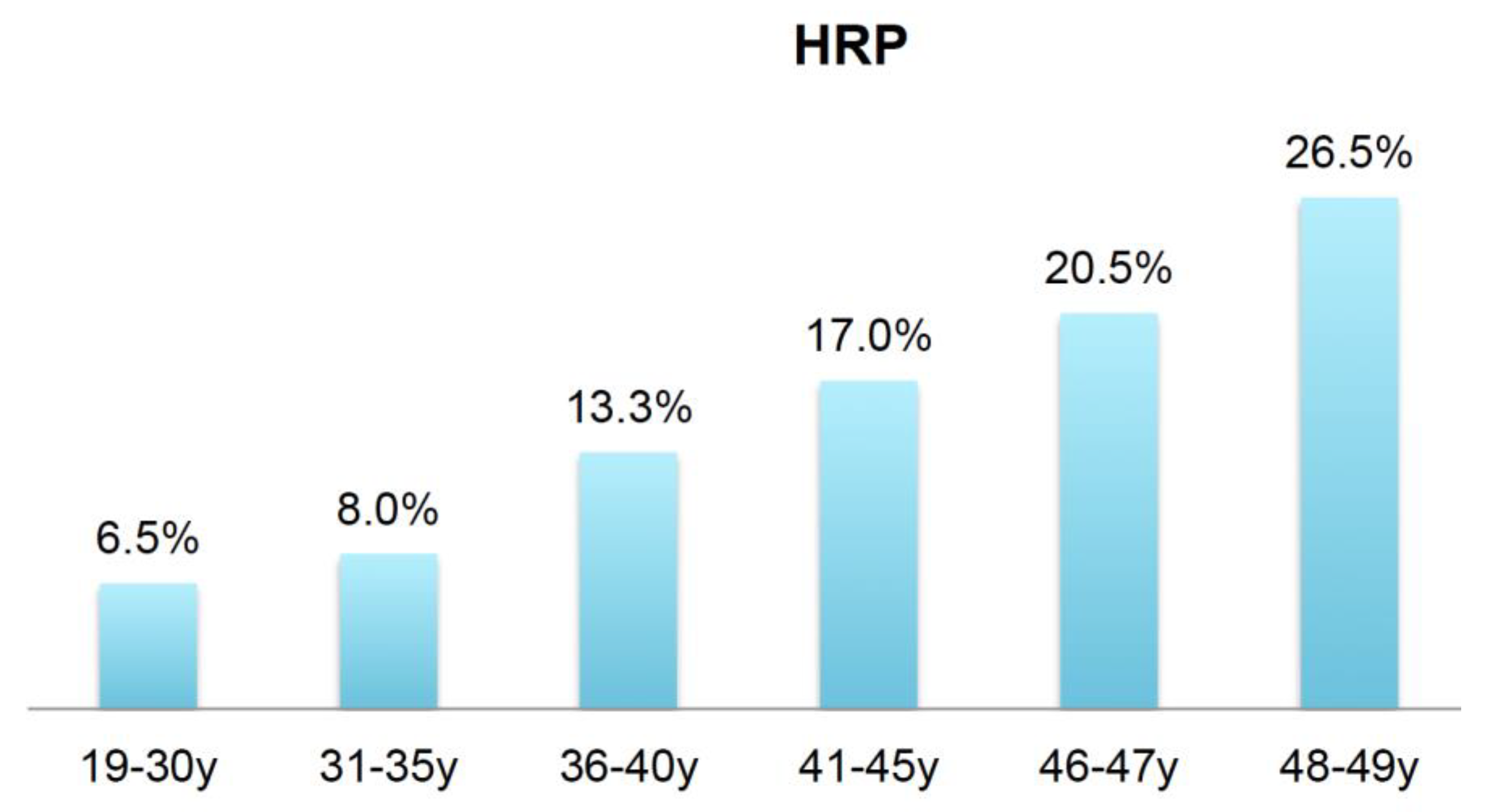
| CTA-HRP | 202/1137 (17.7%) | |
| CACS 0 | 91 (45.1%) | |
| CACS 0.1–0.9 | 31 (15.3%) | |
| CACS > 1.0 | 80 (39.6%) | |
| CACS 0 N = 802 | ||
| CAD by CTA | ||
| CADRADS 0 | 200 (24.9%) | |
| 1 | 600 (74.8%) | |
| 2 | 87 | |
| 3 | 78 | |
| 4 + 5 | 17 | |
| 6/N * | 18 | >50% Stenosis |
| HRP | 2 (0.3%) | 35/802 |
| 92 (11.5%) | (4.4%) | |
| 19–30 y Group 1 n = 77 | 31–35 y Group 2 n = 75 | 36–40 y Group 3 n = 173 | 41–45 y Group 4 n = 358 | 46–47 y Group 5 n = 220 | 47–48 y Group 6 n = 234 | |
|---|---|---|---|---|---|---|
| CACS | ||||||
| 0 | 92.2% | 88.2% | 86.2% | 68.2% | 69.2% | 57.9% |
| >=0.1 AU | 5.2% | 10.6% | 13.8% | 31.8% | 30.8% | 42.1% |
| Cat 1 0.1–10 | 4 (5.2%) | 7 (9.3%) | 17 (9.8%) | 53 (14.8%) | 34 (15.5%) | 37 (15.8%) |
| 2 10–100 | 0 (0%) | 0 (0%) | 3 (1.7%) | 29 (8.1%) | 22 (10%) | 31 (13.2%) |
| 3 100–300 | 0 (0%) | 1 (1.4%) | 3 (1.7%) | 15 (4.2%) | 6 (2.7%) | 21 (9.1%) |
| 4 >300 | 0 (0%) | 0 (0%) | 1 (0.58%) | 3 (8.4%) | 3 (1.4%) | 7 (2.9%) |
| CACS (AU) (range) | 0.03 ± 0.02 (0–1.5) | 1.42 ± 11.8 (0–102) | 11.5 ± 89.1 (0–1101.4) | 15.4 ± 54.1 (0–420) | 18.1 ± 82.0 (0–758.1) | 35.7 ± 11.9 (0–1203.5) |
| CAD-RADS | ||||||
| 0 | 70 (90.9%) | 63 (84%) | 112 (65.1%) | 181 (50.7%) | 110 (50%) | 80 (34.1%) |
| 1 | 3 (3.9%) | 5 (6.7%) | 20 (11.6%) | 58 (16.2%) | 29 (13.2%) | 42 (17.9%) |
| 2 | 1 (1.3%) | 5 (6.7%) | 18 (10.5%) | 70 (19.6%) | 49 (22.3%) | 61 (26%) |
| 3 | 0% | 1 (1.3%) | 11 (6.4%) | 17 (4.8%) | 14 (6.4%) | 29 (12.4%) |
| 4 + 5 | 1 (1.3%) | 1 (1.3%) | 10 (5.8%) | 31 (8.7%) | 18 (8.3%) | 22 (9.4%) |
| 6/N | 2 (2.6%) | 63 (84%) | 1 (0.6%) | 181 (50.7%) | 110 (50%) | 80 (34.1%) |
| Atherosclerosis-CTA | 6.4% | 16.0% | 34.9% | 46.1% | 49.5% | 65.9% |
| HRP | 5 (6.5%) | 6 (8%) | 23 (13.3%) | 61 (17.0%) | 45 (20.5%) | 62 (26.5%) |
| CACS 0 | 2 | 5 | 13 | 30 | 21 | 20 |
| CACS 0.1–0.9 AU | 3 | 1 | 3 | 12 | 4 | 8 |
| CACS > 1.0 AU | 0 | 0 | 7 | 19 | 20 | 34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feuchtner, G.M.; Beyer, C.; Langer, C.; Bleckwenn, S.; Senoner, T.; Barbieri, F.; Luger, A.; Spitaler, P.; Widmann, G.; Adukauskaite, A.; et al. The Atherosclerotic Profile of a Young Symptomatic Population between 19 and 49 Years: Coronary Computed Tomography Angiography or Coronary Artery Calcium Score? J. Cardiovasc. Dev. Dis. 2021, 8, 157. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8110157
Feuchtner GM, Beyer C, Langer C, Bleckwenn S, Senoner T, Barbieri F, Luger A, Spitaler P, Widmann G, Adukauskaite A, et al. The Atherosclerotic Profile of a Young Symptomatic Population between 19 and 49 Years: Coronary Computed Tomography Angiography or Coronary Artery Calcium Score? Journal of Cardiovascular Development and Disease. 2021; 8(11):157. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8110157
Chicago/Turabian StyleFeuchtner, Gudrun Maria, Christoph Beyer, Christian Langer, Sven Bleckwenn, Thomas Senoner, Fabian Barbieri, Anna Luger, Philipp Spitaler, Gerlig Widmann, Agne Adukauskaite, and et al. 2021. "The Atherosclerotic Profile of a Young Symptomatic Population between 19 and 49 Years: Coronary Computed Tomography Angiography or Coronary Artery Calcium Score?" Journal of Cardiovascular Development and Disease 8, no. 11: 157. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8110157