
Asymptomatic Patients with Severe Aortic Stenosis and the Impact of Intervention

Abstract
:1. Introduction
2. Methods
2.1. Patient Population
2.2. Endpoints and Definitions
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
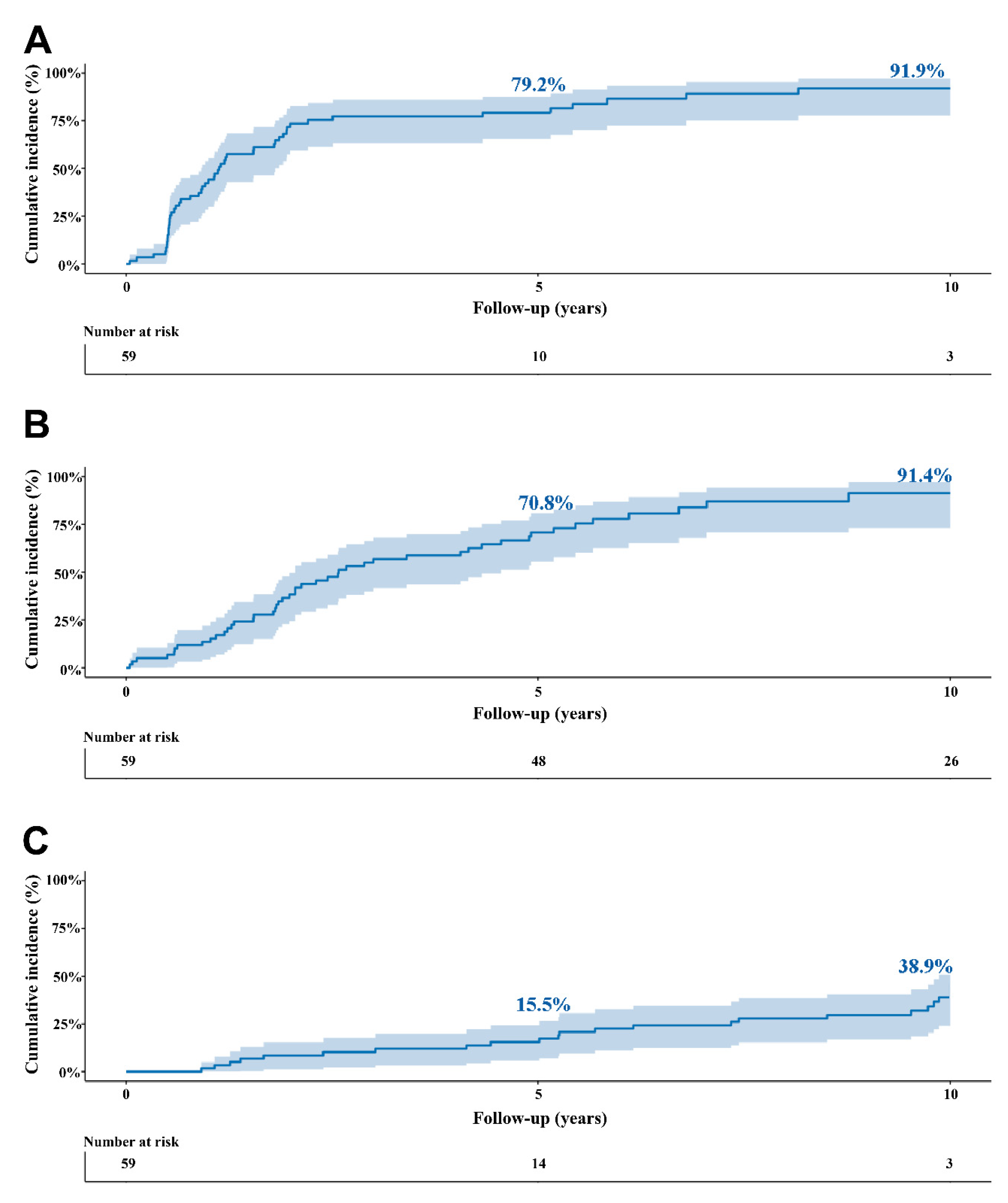
3.2. Natural Course of Asymptomatic Severe Stenosis
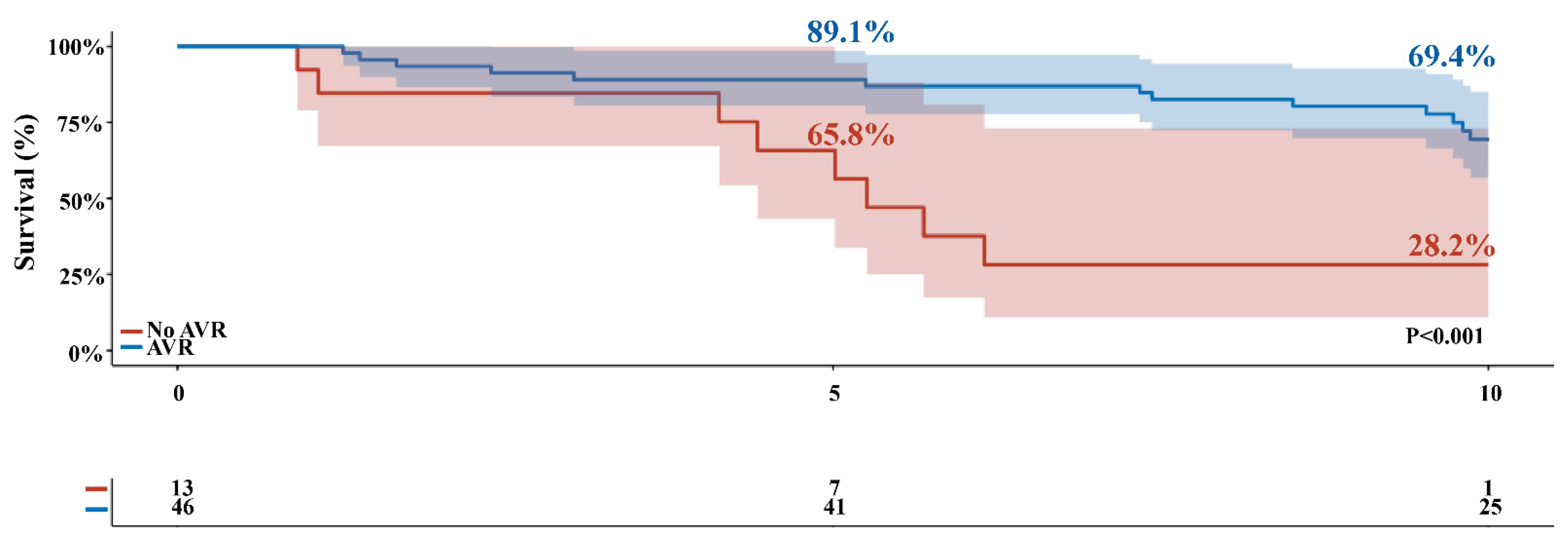
3.3. Survival
3.4. Predictors of Outcome
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| A′ | peak velocity of diastolic mitral annular motion |
| AR | aortic regurgitation |
| AS | aortic stenosis |
| AVA | aortic valve area |
| AVR | aortic valve replacement |
| BMI | body mass index |
| BSA | body surface area |
| CI | confidence interval |
| COPD | chronic obstructive pulmonary disease |
| E′ | peak velocity of early diastolic mitral annular motion |
| E′A′ ratio | ratio of E′ to A |
| EuroSCORE | European system for cardiac operative risk evaluation |
| HR | hazard ratio |
| iAVA | indexed aortic valve area |
| IVCd | inferior vena cava dimension |
| IVSd | interventricular septum dimension |
| LA | left atrium |
| LF/LG AS | low-flow/low-grade AS |
| LVEDD | left ventricular end diastolic diameter |
| LVEF | left ventricular ejection fraction |
| LVET | left ventricular ejection time |
| LVESD | left ventricular end systolic diameter |
| LVFS | left ventricular fractional shortening |
| LVH | left ventricular hypertrophy |
| MAG | mean aortic gradient |
| MR | mitral regurgitation |
| PAD | peripheral arterial disease |
| PAG | peak aortic gradient |
| PWd | posterior wall dimension |
| RCT | randomized controlled trial |
| SAVR | surgical aortic valve replacement |
| STS | society of thoracic surgery |
| TAPSE | tricuspid annular plane systolic excursion |
| TAVI | transcatheter aortic valve implantation |
| Vmax | maximal velocity |
References
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Heart Disease and Stroke Statistics—2014 Update: A Report from the American Heart Association. Circulation 2013, 129, e28–e292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Muñoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef] [PubMed]
- Généreux, P.; Stone, G.W.; O’Gara, P.T.; Marquis-Gravel, G.; Redfors, B.; Giustino, G.; Pibarot, P.; Bax, J.J.; Bonow, R.O.; Leon, M.B. Natural History, Diagnostic Approaches, and Therapeutic Strategies for Patients with Asymptomatic Severe Aortic Stenosis. J. Am. Coll. Cardiol. 2016, 67, 2263–2288. [Google Scholar] [CrossRef]
- Taniguchi, T.; Morimoto, T.; Shiomi, H.; Ando, K.; Kanamori, N.; Murata, K.; Kitai, T.; Kawase, Y.; Izumi, C.; Kato, T.; et al. Sudden Death in Patients with Severe Aortic Stenosis: Observations from the CURRENT AS Registry. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Heuvelman, H.J.; Van Geldorp, M.W.A.; Kappetein, A.P.; Geleijnse, M.L.; Galema, T.W.; Bogers, A.J.J.C.; Takkenberg, J.J.M. Clinical course of patients diagnosed with severe aortic stenosis in the Rotterdam area: Insights from the AVARIJN study. Neth. Heart J. 2012, 20, 487–493. [Google Scholar] [CrossRef] [Green Version]
- Bonow, R.O.; Carabello, B.A.; Kanu, C.; de Leon, A.C.; Faxon, D.P.; Freed, M.D.; Gaasch, W.H.; Lytle, B.W.; Nishimura, R.A.; O’Gara, P.T.; et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): Developed in collaboration with the Society of Cardiovascular Anesthesiologists: Endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation 2006, 114, e84–e231. [Google Scholar]
- Vahanian, A.; Baumgartner, H.; Bax, J.; Butchart, E.; Dion, R.; Filippatos, G.; Flachskampf, F.; Hall, R.; Iung, B.; Kasprzak, J.; et al. Guidelines on the management of valvular heart disease: The Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology. Eur. Heart J. 2006, 28, 230–268. [Google Scholar] [CrossRef] [Green Version]
- Gibbons, R.J. ACC/AHA 2002 Guideline Update for Exercise Testing: Summary Article: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation 2002, 106, 1883–1892. [Google Scholar]
- Pellikka, P.A.; Sarano, M.E.; Nishimura, R.A.; Malouf, J.F.; Bailey, K.R.; Scott, C.G.; Barnes, M.E.; Tajik, A.J. Outcome of 622 Adults with Asymptomatic, Hemodynamically Significant Aortic Stenosis During Prolonged Follow-Up. Circulation 2005, 111, 3290–3295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancellotti, P.; Lebois, F.; Simon, M.; Tombeux, C.; Chauvel, C.; Pierard, L.A. Prognostic importance of quantitative exercise Doppler echocardiography in asymptomatic valvular aortic stenosis. Circulation 2005, 112, I377–I382. [Google Scholar] [PubMed]
- Peidro, R.; Brión, G.; Angelino, A. Exercise Testing in Asymptomatic Aortic Stenosis. Cardiology 2006, 108, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Rafique, A.M.; Biner, S.; Ray, I.; Forrester, J.S.; Tolstrup, K.; Siegel, R.J. Meta-Analysis of Prognostic Value of Stress Testing in Patients with Asymptomatic Severe Aortic Stenosis. Am. J. Cardiol. 2009, 104, 972–977. [Google Scholar] [CrossRef]
- Iung, B.; Baron, G.; Butchart, E.G.; Delahaye, F.; Gohlke-Bärwolf, C.; Levang, O.W.; Tornos, P.; Vanoverschelde, J.-L.; Vermeer, F.; Boersma, E.; et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 2003, 24, 1231–1243. [Google Scholar] [CrossRef] [Green Version]
- Das, P.; Rimington, H.; Chambers, J. Exercise testing to stratify risk in aortic stenosis. Eur. Heart J. 2005, 26, 1309–1313. [Google Scholar] [CrossRef] [Green Version]
- Redfors, B.; Pibarot, P.; Gillam, L.D.; Burkhoff, D.; Bax, J.J.; Lindman, B.R.; Bonow, R.O.; O’Gara, P.T.; Leon, M.B.; Généreux, P. Stress Testing in Asymptomatic Aortic Stenosis. Circulation 2017, 135, 1956–1976. [Google Scholar] [CrossRef]
- Hussain, A.I.; Auensen, A.; Brunborg, C.; Beitnes, J.O.; Gullestad, L.; Pettersen, K.I. Age-dependent morbidity and mortality outcomes after surgical aortic valve replacement. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 650–656. [Google Scholar] [CrossRef] [Green Version]
- Everett, R.J.; Clavel, M.-A.; Pibarot, P.; Dweck, M.R. Timing of intervention in aortic stenosis: A review of current and future strategies. Heart 2018, 104, 2067–2076. [Google Scholar] [CrossRef] [Green Version]
- Taniguchi, T.; Morimoto, T.; Shiomi, H.; Ando, K.; Kanamori, N.; Murata, K.; Kitai, T.; Kawase, Y.; Izumi, C.; Miyake, M.; et al. Initial Surgical Versus Conservative Strategies in Patients with Asymptomatic Severe Aortic Stenosis. J. Am. Coll. Cardiol. 2015, 66, 2827–2838. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.-H.; Park, S.-J.; Lee, S.-A.; Lee, S.; Kim, D.-H.; Kim, H.-K.; Yun, S.-C.; Hong, G.-R.; Song, J.-M.; Chung, C.-H.; et al. Early Surgery or Conservative Care for Asymptomatic Aortic Stenosis. N. Engl. J. Med. 2020, 382, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-J.; Dweck, M.R. Multimodality Imaging for the Assessment of Severe Aortic Stenosis. J. Cardiovasc. Imaging 2019, 27, 235–246. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (n = 59) | Conservative Treatment (n = 13) | AVR (n = 46) | p-Value | |
|---|---|---|---|---|
| Age (years) | 68.8 ± 10.6 | 74.1 ± 8.9 | 66.5 ± 10.6 | 0.022 |
| Female | 15 (25.4) | 1 (7.7) | 14 (30.4) | 0.096 |
| BMI | 27.1 ± 3.7 | 27.5 ± 3.9 | 26.9 ± 3.7 | 0.661 |
| BSA | 1.93 ± 0.20 | 2.00 ± 0.12 | 1.91 ± 0.21 | 0.226 |
| Previous CABG | 2 (3.4) | 0 | 2 (4.3) | 0.444 |
| Smoking | 42 (71.2) | 10 (76.9) | 32 (69.6) | 0.605 |
| Atrial fibrillation | 4 (7.0) | 2 (15.4) | 2 (4.5) | 0.179 |
| Carotid disease | 1 (1.7) | 1 (7.7) | 0 | 0.058 |
| Coronary artery disease | 4 (6.8) | 0 | 4 (8.7) | 0.271 |
| COPD | 6 (10.2) | 2 (15.4) | 4 (8.7) | 0.481 |
| Diabetes | 12 (20.3) | 6 (46.2) | 6 (13.0) | 0.009 |
| Hyperlipidemia | 29 (49.2) | 8 (61.5) | 21 (45.7) | 0.312 |
| Hypertension | 29 (49.2) | 5 (38.5) | 24 (52.2) | 0.383 |
| Myocardial infarction | 4 (6.8) | 0 | 4 (8.7) | 0.271 |
| Peripheral arterial disease | 5 (8.5) | 0 | 5 (10.9) | 0.214 |
| Stroke | 12 (20.3) | 3 (23.1) | 9 (19.6) | 0.781 |
| NT-proBNP (pmol/l) | 32.0 (18.0–97.0) | 33.0 (12.8–149.3) | 32.0 (18.0–89.0) | 0.976 |
| Baseline positive stress test | 15 (25.4) | 4 (30.8) | 11 (24.4) | 0.646 |
| Logistic EuroSCORE | 4.0 (2.1–6.9) | 4.7 (3.2–8.1) | 3.9 (2.1–5.5) | 0.485 |
| STS score | 3.8 (2.0–6.0) | 5.2 (2.2–8.6) | 3.6 (2.0–5.0) | 0.403 |
| No medication | 13 (22.0) | 2 (15.4) | 11 (23.9) | 0.512 |
| Diuretics | 11 (18.6) | 3 (23.1) | 8 (17.4) | 0.642 |
| Ace Inhibitor | 14 (23.7) | 4 (30.8) | 10 (21.7) | 0.499 |
| A2 antagonist | 11 (18.6) | 5 (38.5) | 6 (13.0) | 0.038 |
| B blocker | 15 (25.4) | 1 (7.7) | 14 (30.4) | 0.096 |
| Calcium antagonist | 8 (13.6) | 2 (15.4) | 6 (13.0) | 0.828 |
| Digoxine | 4 (6.8) | 0 | 4 (8.7) | 0.271 |
| Echocardiographic Parameters | ||||
| Vmax (m/s) | 4.24 ± 0.68 | 4.28 ± 0.70 | 4.23 ± 0.68 | 0.823 |
| AVA (cm2) | 0.85 ± 0.28 | 0.80 ± 0.30 | 0.85 ± 0.27 | 0.536 |
| iAVA (cm2/m2) | 0.44 ± 0.15 | 0.41 ± 0.16 | 0.44 ± 0.14 | 0.423 |
| MAG (mmHg) | 42.8 ± 15.0 | 44.3 ± 17.4 | 42.3 ± 14.4 | 0.684 |
| PAG (mmHg) | 73.2 ± 23.6 | 75.3 ± 24.1 | 72.6 ± 23.7 | 0.720 |
| AR grade I/II | 29 (50.0) | 6 (46.2) | 23 (51.1) | 0.753 |
| MR grade I/II | 12 (20.7) | 4 (30.8) | 8 (17.8) | 0.308 |
| LVEF | 62.5 ± 5.9 | 61.1 ± 5.9 | 62.7 ± 5.7 | 0.374 |
| LF/LG AS (%) | 5 (8.5) | 0 | 5 (10.9) | 0.214 |
| LVH (%) | 14 (25.5) | 2 (16.7) | 12 (27.9) | 0.429 |
| TAPSE (mm) | 25.1 ± 3.7 | 23.6 ± 2.8 | 25.5 ± 3.9 | 0.104 |
| LVEDD (mm) | 49.0 ± 6.0 | 49.6 ± 5.1 | 25.5 ± 3.9 | 0.687 |
| LVESD (mm) | 31.4 ± 6.2 | 30.3 ± 5.7 | 31.7 ± 6.4 | 0.466 |
| LVFS (%) | 36.1 ± 8.8 | 38.6 ± 11.0 | 35.4 ± 8.1 | 0.248 |
| LA (mm) | 41.3 ± 6.4 | 42.2 ± 6.8 | 41.0 ± 6.3 | 0.563 |
| IVSd (mm) | 12.6 ± 2.7 | 12.5 ± 2.0 | 12.6 ± 2.9 | 0.834 |
| IVCd (mm) | 17.4 ± 3.6 | 16.4 ± 2.7 | 17.7 ± 3.8 | 0.252 |
| PWd (mm) | 10.8 ± 2.0 | 11.5 ± 1.7 | 10.7 ± 2.1 | 0.161 |
| E′ (cm/s) | 79.5 ± 23.6 | 69.1 ± 29.9 | 82.0 ± 21.4 | 0.103 |
| A′ (cm/s) | 89.9 ± 37.2 | 104.2 ± 59.9 | 86.0 ± 27.9 | 0.134 |
| E′A′ ratio | 1.0 ± 0.57 | 0.8 ± 0.5 | 1.1 ± 0.6 | 0.120 |
| LVET (ms) | 322.1 ± 32.2 | 312.6 ± 43.9 | 324.8 ± 28.4 | 0.296 |
| DT (ms) | 239.4 ± 63.3 | 217.5 ± 52.6 | 245.3 ± 65.2 | 0.198 |
| Overall Cohort | |||
|---|---|---|---|
| Restricted Mean Survival Time at 10 Years | 95% CI | p-Value | |
| Difference—months | 31.85 | 13.27–58.44 | 0.002 |
| Ratio | 1.51 | 1.11–2.05 | 0.008 |
| Ratio of restricted mean time lost | 0.28 | 0.13–0.60 | 0.001 |
| Univariable HR (95% CI), p-Value | Multivariable HR (95% CI), p-Value | |
|---|---|---|
| Age | 1.11 (1.06–1.17), p < 0.001 | 1.08 (1.01–1.16), p = 0.026 |
| Gender (female) | 0.43 (0.16–1.37), p = 0.125 | |
| Atrial fibrillation | 4.98 (1.40–17.72), p = 0.013 | 3.10 (0.68–14.26), p = 0.146 |
| Coronary artery disease | 0.62 (0.08–4.59), p = 0.639 | |
| COPD | 1.60 (0.48–5.39), p = 0.446 | |
| Diabetes mellitus | 4.57 (1.91–10.96), p < 0.001 | 2.36 (0.87–6.44), p = 0.094 |
| Hyperlipidemia | 1.65 (0.72–3.78), p = 0.234 | |
| Hypertension | 1.50 (0.66–3.37), p = 0.332 | |
| Myocardial infarction | 1.14 (0.27–4.86), p = 0.862 | |
| Peripheral arterial disease | 1.58 (0.46–5.34), p = 0.466 | |
| Stroke | 2.11 (0.90–4.92), p = 0.086 | |
| Exercise test (positive) | 0.74 (0.27–1.98) p = 0.543 | |
| NT-proBNP | 1.002 (1.001–1.004) p < 0.001 | 1.002 (1.00–1.003), p = 0.053 |
| STS score | 1.06 (0.99–1.14), p = 0.098 | |
| Logistic EuroSCORE | 1.22 (1.09–1.35), p < 0.001 | 0.98 (0.81–1.18), p = 0.830 |
| AVR | 0.24 (0.10–0.58) p = 0.002 | 1.17 (0.31–4.36), p = 0.820 |
| LVEF | 0.96 (0.90–1.04), p = 0.315 | |
| Vmax | 0.95 (0.53–1.70), p = 0.851 | |
| AVA | 0.19 (0.03–1.11), p = 0.065 | |
| iAVA | 0.05 (0.00–1.141), p = 0.078 | |
| MAG | 1.01 (0.99–1.03), p = 0.460 | |
| PAG | 1.00 (0.98–1.10), p = 0.817 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Çelik, M.; Milojevic, M.; Durko, A.P.; Oei, F.B.S.; Mahtab, E.A.F.; Bogers, A.J.J.C. Asymptomatic Patients with Severe Aortic Stenosis and the Impact of Intervention. J. Cardiovasc. Dev. Dis. 2021, 8, 35. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8040035
Çelik M, Milojevic M, Durko AP, Oei FBS, Mahtab EAF, Bogers AJJC. Asymptomatic Patients with Severe Aortic Stenosis and the Impact of Intervention. Journal of Cardiovascular Development and Disease. 2021; 8(4):35. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8040035
Chicago/Turabian StyleÇelik, Mevlüt, Milan Milojevic, Andras P. Durko, Frans B. S. Oei, Edris A. F. Mahtab, and Ad J. J. C. Bogers. 2021. "Asymptomatic Patients with Severe Aortic Stenosis and the Impact of Intervention" Journal of Cardiovascular Development and Disease 8, no. 4: 35. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8040035