
Time Trends of Ventricular Reconstruction and Outcomes among Patients with Left Ventricular Thrombus and Aneurysms
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patient Population
2.2. Baseline, Follow-Up, and Outcomes
2.3. Left Ventricular Thrombus and Aneurysm Evaluation
2.4. Other Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Time Trends of SVR and Anticoagulation Therapy
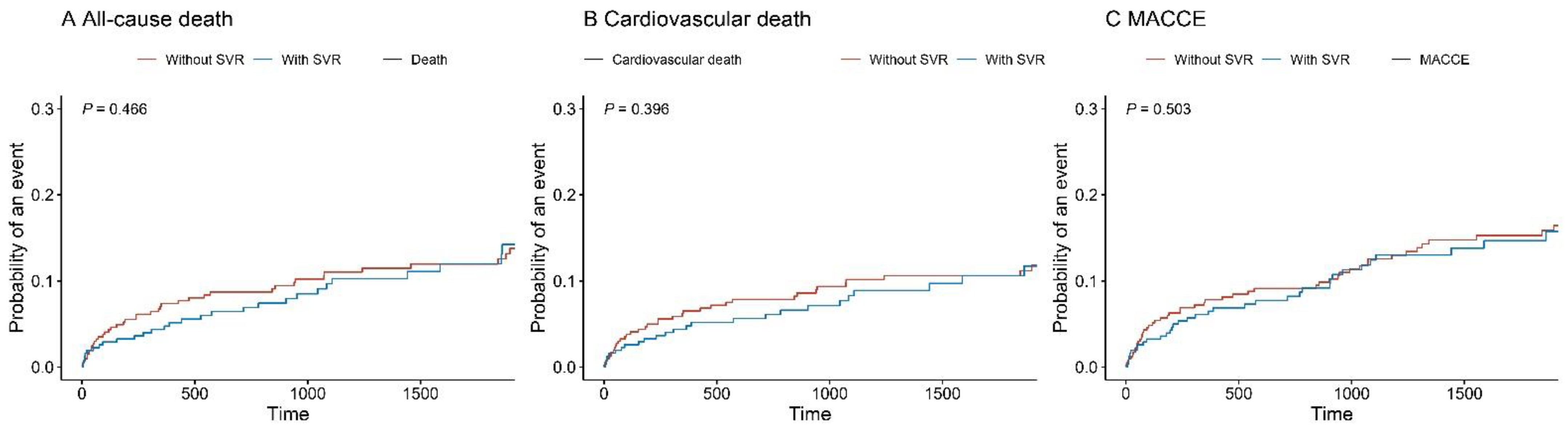
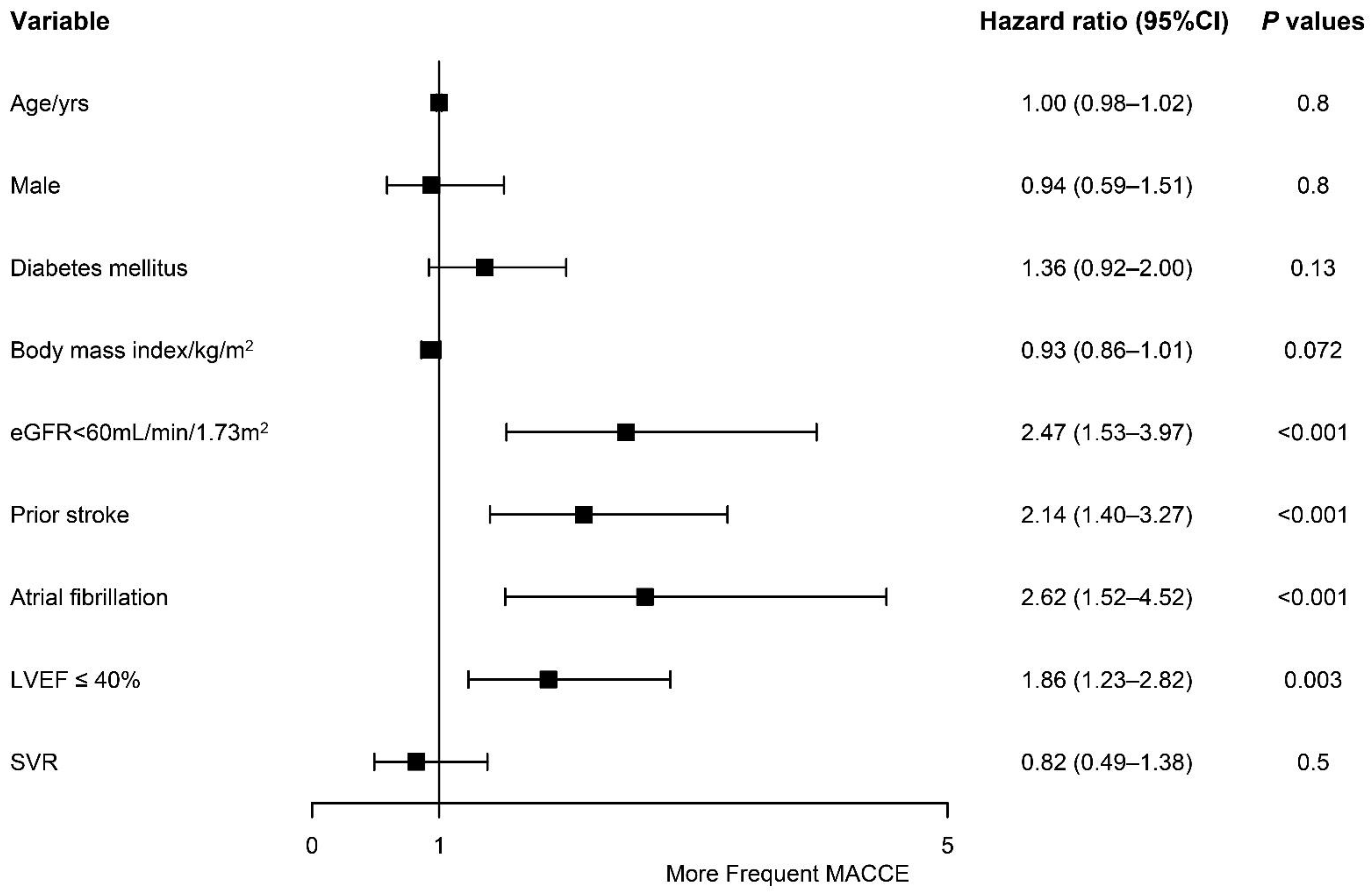
3.3. Competing Risks of Adverse Outcomes
4. Discussion
4.1. Trends in the Incidence of LVT
4.2. Impact of LVT on Prognosis and Treatment
4.3. Comparison of Medical and Surgical Treatment
4.4. Whether Postoperative Anticoagulant Therapy Is Required
4.5. Risk Factors for the Prognosis
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- McCarthy, C.P.; Vaduganathan, M.; McCarthy, K.J.; Januzzi, J.L., Jr.; Bhatt, D.L.; McEvoy, J.W. Left Ventricular Thrombus after Acute Myocardial Infarction: Screening, Prevention, and Treatment. JAMA Cardiol. 2018, 3, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Camaj, A.; Fuster, V.; Giustino, G.; Bienstock, S.W.; Sternheim, D.; Mehran, R.; Dangas, G.D.; Kini, A.; Sharma, S.K.; Halperin, J.; et al. Left Ventricular Thrombus Following Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2022, 79, 1010–1022. [Google Scholar] [CrossRef]
- Habash, F.; Vallurupalli, S. Challenges in management of left ventricular thrombus. Ther. Adv. Cardiovasc. Dis. 2017, 11, 203–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E., Jr.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 61, e78–e140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.; Zhou, J.; Liu, C.; Zhou, P.; Li, J.; Wang, Y.; Zhao, X.; Chen, Y.; Song, L.; Zhao, H.; et al. Direct oral anticoagulants versus vitamin K antagonists for patients with left ventricular thrombus: A systematic review and meta-analysis. Pol. Arch. Intern. Med. 2021, 131, 429–438. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [Green Version]
- Shi, B.; Wang, H.; Song, C.; Yin, D.; Wang, H.; Dou, K.F.; Song, W. Widespread Off-Label Use of Direct Oral Anticoagulants in Patients with Left Ventricular Thrombus. J. Am. Coll. Cardiol. 2022, 79, 1028. [Google Scholar] [CrossRef]
- Bhardwaj, B.; Kumar, V.; Patel, N.; Abdullah, O.; Balla, S.; Alpert, M.; Chan, A.; Kumar, A. Implications of Left Ventricular Aneurysm in Patients with Acute Myocardial Infarction: An Analysis from National Inpatient Sample Database. J. Am. Coll. Cardiol. 2018, 71, A146. [Google Scholar] [CrossRef]
- Song, Y.; Hu, S.; Sun, H.; Song, Y.; Wang, L.; Wang, W.; Pan, S.; Wang, S.; Feng, W.; Zheng, Z. Results of Left Ventricular Reconstruction with and without Mitral Valve Surgery. Ann. Thorac. Surg. 2020, 109, 753–761. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. Professional Practice Committee: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S3. [Google Scholar] [CrossRef]
- Küpper, A.J.F.; Verheugt, F.W.; Peels, C.H.; Galema, T.W.; Roos, J.P. Left ventricular thrombus incidence and behavior studied by serial two-dimensional echocardiography in acute anterior myocardial infarction: Left ventricular wall motion, systemic embolism and oral anticoagulation. J. Am. Coll. Cardiol. 1989, 13, 1514–1520. [Google Scholar] [CrossRef] [Green Version]
- Pizzeti, G.; Belotti, G.; Margonato, A.; Carlino, M.; Gerosa, S.; Carandente, O.; Chierchia, S.L. Thrombolytic therapy reduces the incidence of left ventricular thrombus after anterior myocardial infarction. Relationship to vessel patency and infarct size. Eur. Heart J. 1996, 17, 421–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osherov, A.B.; Borovik-Raz, M.; Aronson, D.; Agmon, Y.; Kapeliovich, M.; Kerner, A.; Grenadier, E.; Hammerman, H.; Nikolsky, E.; Roguin, A. Incidence of early left ventricular thrombus after acute anterior wall myocardial infarction in the primary coronary intervention era. Am. Heart J. 2009, 157, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Meurin, P.; Brandao Carreira, V.; Dumaine, R.; Shqueir, A.; Milleron, O.; Safar, B.; Perna, S.; Smadja, C.; Genest, M.; Garot, J.; et al. Incidence, diagnostic methods, and evolution of left ventricular thrombus in patients with anterior myocardial infarction and low left ventricular ejection fraction: A prospective multicenter study. Am. Heart J. 2015, 170, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Cambronero-Cortinas, E.; Bonanad, C.; Monmeneu, J.V.; Lopez-Lereu, M.P.; Gavara, J.; de Dios, E.; Rios, C.; Perez, N.; Racugno, P.; Paya, A.; et al. Incidence, Outcomes, and Predictors of Ventricular Thrombus after Reperfused ST-Segment-Elevation Myocardial Infarction by Using Sequential Cardiac MR Imaging. Radiology 2017, 284, 372–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulluck, H.; Chan, M.H.H.; Paradies, V.; Yellon, R.L.; Ho, H.H.; Chan, M.Y.; Chin, C.W.L.; Tan, J.W.; Hausenloy, D.J. Incidence and predictors of left ventricular thrombus by cardiovascular magnetic resonance in acute ST-segment elevation myocardial infarction treated by primary percutaneous coronary intervention: A meta-analysis. J. Cardiovasc. Magn. Reson. 2018, 20, 72. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Ye, X.; Yan, D.; Peng, Y.; Zhang, Z. Incidence and risk factors of left ventricular thrombus in acute ST-segment elevation myocardial infraction treated by primary percutaneous coronary intervention: A meta-analysis. Med. Princ. Pract. 2022, 31, 415–423. [Google Scholar] [CrossRef]
- Yang, Q.; Lang, X.; Quan, X.; Gong, Z.; Liang, Y. Different Oral Antithrombotic Therapy for the Treatment of Ventricular Thrombus: An Observational Study from 2010 to 2019. Int. J. Clin. Pract. 2022, 2022, 7400860. [Google Scholar] [CrossRef]
- Delewi, R.; Zijlstra, F.; Piek, J.J. Left ventricular thrombus formation after acute myocardial infarction. Heart 2012, 98, 1743–1749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaitkus, P.T.; Barnathan, E.S. Embolic potential, prevention and management of mural thrombus complicating anterior myocardial infarction: A meta-analysis. J. Am. Coll. Cardiol. 1993, 22, 1004–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maniwa, N.; Fujino, M.; Nakai, M.; Nishimura, K.; Miyamoto, Y.; Kataoka, Y.; Asaumi, Y.; Tahara, Y.; Nakanishi, M.; Anzai, T.; et al. Anticoagulation combined with antiplatelet therapy in patients with left ventricular thrombus after first acute myocardial infarction. Eur. Heart J. 2018, 39, 201–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, G.N.; McEvoy, J.W.; Fang, J.C.; Ibeh, C.; McCarthy, C.P.; Misra, A.; Shah, Z.I.; Shenoy, C.; Spinler, S.A.; Vallurupalli, S.; et al. Management of Patients at Risk for and With Left Ventricular Thrombus: A Scientific Statement From the American Heart Association. Circulation 2022, 146, e205–e223. [Google Scholar] [CrossRef]
- Cruz Rodriguez, J.B.; Okajima, K.; Greenberg, B.H. Management of left ventricular thrombus: A narrative review. Ann. Transl. Med. 2021, 9, 520. [Google Scholar] [CrossRef]
- Massussi, M.; Scotti, A.; Lip, G.Y.H.; Proietti, R. Left ventricular thrombosis: New perspectives on an old problem. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, 158–167. [Google Scholar] [CrossRef]
- Lee, J.M.; Park, J.J.; Jung, H.W.; Cho, Y.S.; Oh, I.Y.; Yoon, C.H.; Suh, J.W.; Chun, E.J.; Choi, S.I.; Youn, T.J.; et al. Left ventricular thrombus and subsequent thromboembolism, comparison of anticoagulation, surgical removal, and antiplatelet agents. J. Atheroscler. Thromb. 2013, 20, 73–93. [Google Scholar] [CrossRef] [Green Version]
- Robinson, A.A.; Trankle, C.R.; Eubanks, G.; Schumann, C.; Thompson, P.; Wallace, R.L.; Gottiparthi, S.; Ruth, B.; Kramer, C.M.; Salerno, M.; et al. Off-label Use of Direct Oral Anticoagulants Compared With Warfarin for Left Ventricular Thrombi. JAMA Cardiol. 2020, 5, 685–692. [Google Scholar] [CrossRef]
- Lattuca, B.; Bouziri, N.; Kerneis, M.; Portal, J.J.; Zhou, J.; Hauguel-Moreau, M.; Mameri, A.; Zeitouni, M.; Guedeney, P.; Hammoudi, N.; et al. Antithrombotic Therapy for Patients With Left Ventricular Mural Thrombus. J. Am. Coll. Cardiol. 2020, 75, 1676–1685. [Google Scholar] [CrossRef]
- Zhou, X.; Shi, R.; Wu, G.; Zhu, Q.; Zhou, C.; Wang, L.; Xue, C.; Jiang, Y.; Cai, X.; Huang, W.; et al. The prevalence, predictors, and outcomes of spontaneous echocardiographic contrast or left ventricular thrombus in patients with HFrEF. ESC Heart Fail. 2021, 8, 1284–1294. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | Non-SVR Group | SVR Group | p-Value | SMD | |
|---|---|---|---|---|---|
| n | 723 | 518 | 205 | ||
| Demographics | |||||
| Age (years), median [Q1, Q3] | 58.0 [51.0, 66.0] | 59.0 [51.0, 67.0] | 58.0 [50.0, 63.0] | 0.049 | 0.156 |
| Male, n (%) | 636 (88.0) | 451 (87.1) | 185 (90.2) | 0.29 | 0.1 |
| Body mass index (kg/m2), median [Q1, Q3] | 25.1 [23.2, 27.3] | 25.2 [23.2, 27.4] | 24.9 [23.4, 27.3] | 0.687 | 0.046 |
| Past medical history | |||||
| Hypertension, n (%) | 399 (55.2) | 303 (58.5) | 96 (46.8) | 0.006 | 0.235 |
| Diabetes mellitus, n (%) | 282 (39.0) | 214 (41.3) | 68 (33.2) | 0.053 | 0.169 |
| eGFR < 60 mL/min/1.73 m2, n (%) | 113 (15.6) | 83 (16.0) | 30 (14.6) | 0.726 | 0.039 |
| Stroke, n (%) | 118 (16.3) | 90 (17.4) | 28 (13.7) | 0.268 | 0.103 |
| CABG, n (%) | 17 (2.4) | 17 (3.3) | 0 | 0.019 | 0.261 |
| PCI, n (%) | 160 (22.1) | 120 (23.2) | 40 (19.5) | 0.333 | 0.089 |
| Atrial fibrillation, n (%) | 52 (7.2) | 48 (9.3) | 4 (2.0) | 0.001 | 0.322 |
| Antithrombotic medications | |||||
| Aspirin, n (%) | 586 (81.1) | 394 (76.1) | 192 (93.7) | <0.001 | 0.506 |
| Clopidogrel, n (%) | 404 (55.9) | 341 (65.8) | 63 (30.7) | <0.001 | 0.75 |
| Ticagrelor, n (%) | 35 (4.8) | 27 (5.2) | 8 (3.9) | 0.584 | 0.063 |
| P2Y12 inhibitor, n (%) | 439 (60.7) | 368 (71.0) | 71 (34.6) | <0.001 | 0.783 |
| DAPT, n (%) | 366 (50.6) | 296 (57.1) | 70 (34.1) | <0.001 | 0.475 |
| VKA, n (%) | 213 (29.5) | 150 (29.0) | 63 (30.7) | 0.703 | 0.039 |
| DOAC, n (%) | 103 (14.2) | 102 (19.7) | 1 (0.5) | <0.001 | 0.673 |
| Antiplatelet therapy only, n (%) | 391 (54.1) | 259 (50.0) | 132 (64.4) | 0.001 | 0.294 |
| Anticoagulation therapy only, n (%) | 48 (6.6) | 45 (8.7) | 3 (1.5) | 0.001 | 0.334 |
| Aspirin with anticoagulants, n (%) | 107 (14.8) | 56 (10.8) | 51 (24.9) | <0.001 | 0.374 |
| Clopidogrel with anticoagulants, n (%) | 66 (9.1) | 66 (12.7) | 0 | <0.001 | 0.54 |
| DAPT with anticoagulants | 93 (12.9) | 84 (16.2) | 9 (4.4) | <0.001 | 0.397 |
| Echocardiographic evaluation | |||||
| LVEDD (mm), median [Q1, Q3] | 56.0 [51.0, 60.9] | 56.0 [52.0, 60.6] | 55.1 [51.0, 61.0] | 0.231 | 0.131 |
| LVEF (%), median [Q1, Q3] | 42.0 [36.0, 48.0] | 40.7 [35.0, 48.0] | 42.0 [38.0, 50.0] | 0.026 | 0.186 |
| LVEF ≤ 40%, n (%) | 344 (47.6) | 258 (49.8) | 86 (42.0) | 0.068 | 0.158 |
| Apical LVT, n (%) | 677 (93.6) | 490 (94.6) | 187 (91.2) | 0.132 | 0.132 |
| Round LVT, n (%) | 400 (55.3) | 299 (57.7) | 101 (49.3) | 0.048 | 0.17 |
| Mobile LVT, n (%) | 28 (3.9) | 21 (4.1) | 7 (3.4) | 0.851 | 0.034 |
| Multiple LVT, n (%) | 32 (4.4) | 27 (5.2) | 5 (2.4) | 0.152 | 0.145 |
| Calcified LVT, n (%) | 88 (12.2) | 68 (13.1) | 20 (9.8) | 0.261 | 0.106 |
| LVT largest diameter (mm), median [Q1, Q3] | 25.9 [18.0, 34.0] | 24.0 [17.3, 33.0] | 26.53 [19.0, 35.0] | 0.012 | 0.128 |
| LVA largest diameter (mm), median [Q1, Q3] | 40.0 [32.0, 46.0] | 39.0 [32.0, 45.0] | 41.0 [34.0, 49.0] | 0.002 | 0.254 |
| Univariable Analysis | Multivariable Analysis | PSM Analysis | IPTW Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Without SVR (n = 518) | With SVR (n = 205) | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| All-cause death | 78 (15.1%) | 15 (7.3%) | 0.55 (0.32–0.97) | 0.038 | 0.60 (0.32–1.13) | 0.110 | 0.77 (0.40–1.50) | 0.500 | 0.71 (0.37–1.35) | 0.292 |
| Cardiovascular death | 62 (12.0%) | 14 (6.8%) | 0.69 (0.38–1.23) | 0.200 | 0.79 (0.41–1.50) | 0.500 | 0.93 (0.46–1.88) | 0.800 | 0.88 (0.45–1.71) | 0.702 |
| MACCEs | 85 (16.4%) | 21 (10.2%) | 0.75 (0.46–1.20) | 0.200 | 0.82 (0.49–1.38) | 0.500 | 1.06 (0.59–1.92) | 0.800 | 0.92 (0.54–1.57) | 0.751 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, B.; Tiemuerniyazi, X.; Zhang, R.; Song, C.; Cui, K.; Zhang, D.; Jia, L.; Yin, D.; Wang, H.; Song, W.; et al. Time Trends of Ventricular Reconstruction and Outcomes among Patients with Left Ventricular Thrombus and Aneurysms. J. Cardiovasc. Dev. Dis. 2022, 9, 464. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9120464
Shi B, Tiemuerniyazi X, Zhang R, Song C, Cui K, Zhang D, Jia L, Yin D, Wang H, Song W, et al. Time Trends of Ventricular Reconstruction and Outcomes among Patients with Left Ventricular Thrombus and Aneurysms. Journal of Cardiovascular Development and Disease. 2022; 9(12):464. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9120464
Chicago/Turabian StyleShi, Boqun, Xieraili Tiemuerniyazi, Rui Zhang, Chenxi Song, Kongyong Cui, Dong Zhang, Lei Jia, Dong Yin, Hongjian Wang, Weihua Song, and et al. 2022. "Time Trends of Ventricular Reconstruction and Outcomes among Patients with Left Ventricular Thrombus and Aneurysms" Journal of Cardiovascular Development and Disease 9, no. 12: 464. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9120464