
Association of Circulating IgE and CML Levels with In-Stent Restenosis in Type 2 Diabetic Patients with Stable Coronary Artery Disease

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Cohort
2.2. Coronary Angiography and Quantitative Analysis
2.3. Biochemical Assessments
2.4. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
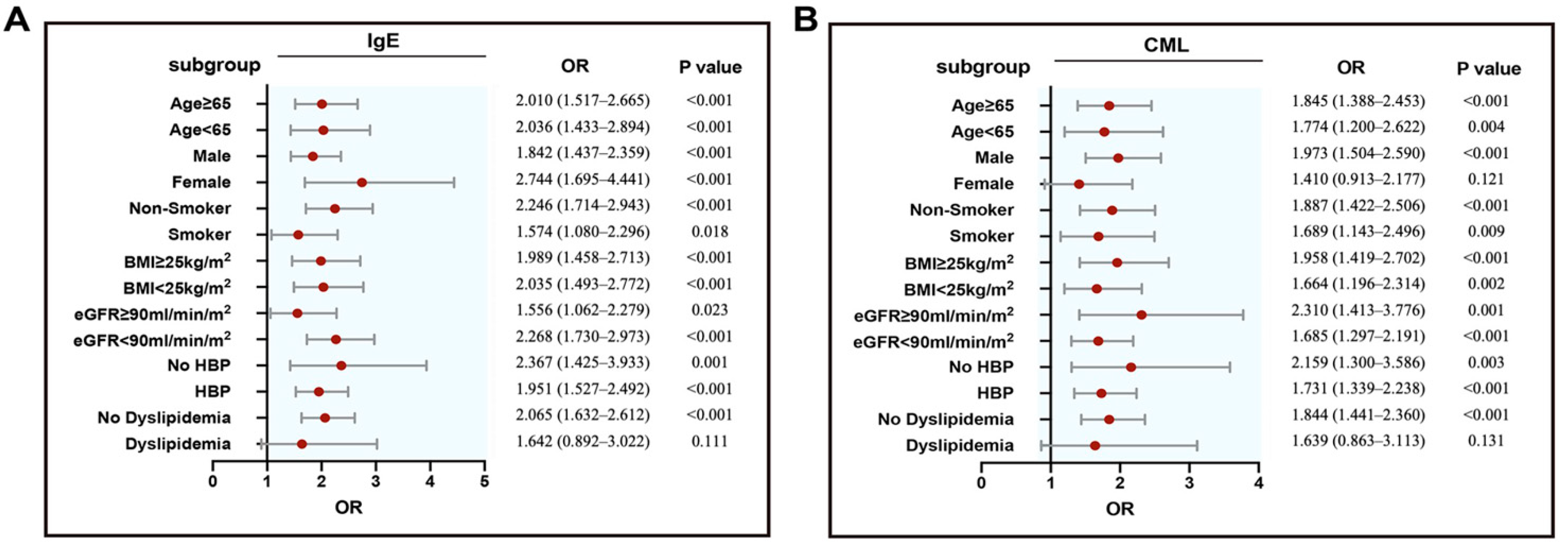
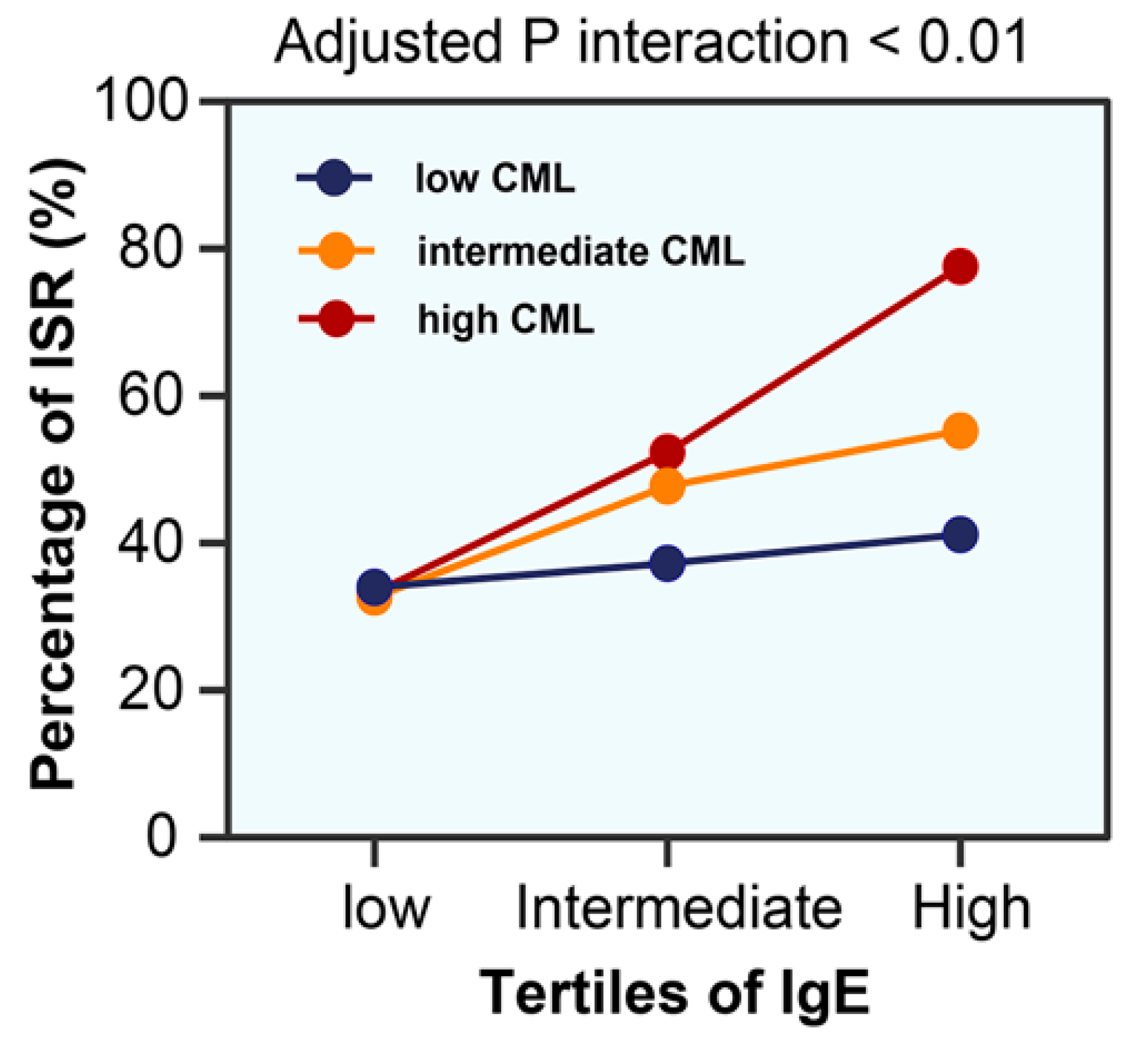
3.2. IgE and CML Levels with ISR
4. Discussion
4.1. Role of Elevated Circulating IgE and CML in ISR
4.2. Potential Clinical Implications
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alfonso, F.; Byrne, R.; Rivero, F.; Kastrati, A. Current treatment of in-stent restenosis. J. Am. Coll. Cardiol. 2014, 63, 2659–2673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dangas, G.D.; Claessen, B.; Caixeta, A.; Sanidas, E.A.; Mintz, G.S.; Mehran, R. In-stent restenosis in the drug-eluting stent era. J. Am. Coll. Cardiol. 2010, 56, 1897–1907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siontis, G.C.M.; Stefanini, G.; Mavridis, D.; Siontis, K.C.; Alfonso, F.; Pérez-Vizcayno, M.J.; Byrne, R.; Kastrati, A.; Meier, B.; Salanti, G.; et al. Percutaneous coronary interventional strategies for treatment of in-stent restenosis: A network meta-analysis. Lancet 2015, 386, 655–664. [Google Scholar] [CrossRef]
- Bednarska, J.; Bednarska-Chabowska, D.; Adamiec-Mroczek, J. Coronary artery disease: New insights into revascularization treatment of diabetic patients. Adv. Clin. Exp. Med. 2017, 26, 1163–1167. [Google Scholar]
- Cassese, S.; Byrne, R.; Tada, T.; Pinieck, S.; Joner, M.; Ibrahim, T.; King, L.A.; Fusaro, M.; Laugwitz, K.-L.; Kastrati, A. Incidence and predictors of restenosis after coronary stenting in 10 004 patients with surveillance angiography. Heart 2013, 100, 153–159. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Iantorno, M.; Waksman, R. Restenosis of drug-eluting stents: A New Classification System Based on Disease Mechanism to Guide Treatment and State-of-the-Art Review. Circ. Cardiovasc. Interv. 2019, 12, e007023. [Google Scholar] [CrossRef]
- Petrie, J.; Guzik, T.J.; Touyz, R.M. Diabetes, hypertension, and cardiovascular disease: Clinical insights and vascular mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef] [Green Version]
- Goldin, A.; Beckman, J.A.; Schmidt, A.M.; Creager, M.A. Advanced glycation end products: Sparking the development of diabetic vascular injury. Circulation 2006, 114, 597–605. [Google Scholar] [CrossRef] [Green Version]
- Dai, Y.; Shen, Y.; Li, Q.R.; Ding, F.H.; Wang, X.Q.; Liu, H.J.; Yan, X.X.; Wang, L.J.; Yang, K.; Wang, H.B.; et al. Glycated apolipoprotein A-IV induces atherogenesis in patients with CAD in type 2 diabetes. J. Am. Coll. Cardiol. 2017, 70, 2006–2019. [Google Scholar] [CrossRef]
- Chen, Y.; Niu, W.; Chao, Y.C.; He, Z.; Ding, R.; Wu, F.; Liang, C. Alagebrium targets the miR-27b/TSP-1 signaling pathway to rescue N(epsilon)-carboxymethyl-lysine-induced endothelial dysfunction. Am. J. Transl. Res. 2019, 11, 1569–1580. [Google Scholar]
- Semba, R.D.; Bandinelli, S.; Sun, K.; Guralnik, J.M.; Ferrucci, L. Plasma carboxymethyl-lysine, an advanced glycation end product, and all-cause and cardiovascular disease mortality in older community-dwelling adults. J. Am. Geriatr. Soc. 2009, 57, 1874–1880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartog, J.W.; Voors, A.A.; Schalkwijk, C.G.; Scheijen, J.; Smilde, T.D.; Damman, K.; Bakker, S.J.; Smit, A.J.; Van Veldhuisen, D.J. Clinical and prognostic value of advanced glycation end-products in chronic heart failure. Eur. Heart J. 2007, 28, 2879–2885. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.C.; Zarrin, A.A. The production and regulation of IgE by the immune system. Nat. Rev. Immunol. 2014, 14, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Cepelis, A.; Brumpton, B.M.; Laugsand, L.E.; Dalen, H.; Langhammer, A.; Janszky, I.; Strand, L.B. Asthma, asthma control and risk of acute myocardial infarction: HUNT study. Eur. J. Epidemiol. 2019, 34, 967–977. [Google Scholar] [CrossRef]
- Carter, P.; Lagan, J.; Fortune, C.; Bhatt, D.L.; Vestbo, J.; Niven, R.; Chaudhuri, N.; Schelbert, E.B.; Potluri, R.; Miller, C.A. Association of cardiovascular disease with respiratory disease. J. Am. Coll. Cardiol. 2019, 73, 2166–2177. [Google Scholar] [CrossRef]
- Iribarren, C.; Tolstykh, I.V.; Miller, M.K.; Sobel, E.; Eisner, M.D. Adult asthma and risk of coronary heart disease, cerebrovascular disease, and heart failure: A prospective study of 2 matched cohorts. Am. J. Epidemiol. 2012, 176, 1014–1024. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Fu, Y.; Wang, K. Asthma and risk of coronary heart disease: A meta-analysis of cohort studies. Ann. Allergy Asthma Immunol. 2017, 118, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Kounis, N.G.; Koniari, I.; Tsigkas, G.; Davlouros, P. Humanized monoclonal antibodies against IgE antibodies as therapy for IgE-mediated coronary syndromes: Are we there yet? Can. J. Cardiol. 2020, 36, 816–819. [Google Scholar] [CrossRef]
- Wang, J.; Lindholt, J.S.; Sukhova, G.K.; Shi, M.A.; Xia, M.; Chen, H.; Xiang, M.; He, A.; Wang, Y.; Xiong, N.; et al. IgE actions on CD 4 + T cells, mast cells, and macrophages participate in the pathogenesis of experimental abdominal aortic aneurysms. EMBO Mol. Med. 2014, 6, 952–969. [Google Scholar] [CrossRef]
- Kounis, N.G. Kounis syndrome (allergic angina and allergic myocardial infarction): A natural paradigm? Int. J. Cardiol. 2006, 110, 7–14. [Google Scholar] [CrossRef]
- Guo, X.; Yuan, S.; Liu, Y.; Zeng, Y.; Xie, H.; Liu, Z.; Zhang, S.; Fang, Q.; Wang, J.; Shen, Z. Serum IgE levels are associated with coronary artery disease severity. Atherosclerosis 2016, 251, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Tochino, Y.; Kanazawa, H.; Ichimaru, Y.; Asai, K.; Kyoh, S.; Hirata, K. Nε-(Carboxymethyl)Lysine, a major advanced glycation end product in exhaled breath condensate as a biomarker of small airway involvement in asthma. J. Asthma 2007, 44, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Niccoli, G.; Montone, R.A.; Sabato, V.; Crea, F. Role of allergic inflammatory cells in coronary artery disease. Circulation 2018, 138, 1736–1748. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2020. Diabetes Care 2020, 43 (Suppl. S1), S14–S31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Pu, L.J.; Chen, Q.J.; Wang, L.; Peng, W.; Yan, X.; Zhang, Q.; Zhang, R.Y.; Gong, P.H.; Qiu, J.P.; et al. Increased glycated albumin and decreased esRAGE concentrations are associated with in-stent restenosis in Chinese diabetic patients. Clin. Chim. Acta 2008, 396, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Farb, A.; Sangiorgi, G.; Carter, A.J.; Walley, V.M.; Edwards, W.D.; Schwartz, R.S.; Virmani, R. Pathology of acute and chronic coronary stenting in humans. Circulation 1999, 99, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Kounis, N.G.; Koniari, I.; Roumeliotis, A.; Tsigas, G.; Soufras, G.; Grapsas, N.; Davlouros, P.; Hahalis, G. Thrombotic responses to coronary stents, bioresorbable scaffolds and the Kounis hypersensitivity-associated acute thrombotic syndrome. J. Thorac. Dis. 2017, 9, 1155–1164. [Google Scholar] [CrossRef] [Green Version]
- Barros, V.; Pereira, M.; Araújo, C.; Braga, P.; Azevedo, A. Use of drug-eluting versus bare-metal stents after an acute coronary syndrome in Portugal: The EURHOBOP study. Rev. Port. Cardiol. 2015, 34, 449–456. [Google Scholar] [CrossRef]
- Finn, A.V.; Nakazawa, G.; Joner, M.; Kolodgie, F.D.; Mont, E.K.; Gold, H.K.; Virmani, R. Vascular responses to drug eluting stents: Importance of delayed healing. Arter. Thromb. Vasc. Biol. 2007, 27, 1500–1510. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Jeong, J.S.; Han, K.; Baek, K.H.; Song, K.-H.; Kwon, H.-S. House dust mite and cockroach specific immunoglobulin E sensitization is associated with diabetes mellitus in the adult Korean population. Sci. Rep. 2018, 8, 2614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Zhang, H.; Shen, X.-H.; Jin, K.-L.; Ye, G.-F.; Qiu, W.; Qian, L.; Li, B.; Zhang, Y.-H.; Shi, G.-P. Immunoglobulin E and mast cell proteases are potential risk factors of impaired fasting glucose and impaired glucose tolerance in humans. Ann. Med. 2012, 45, 220–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gresele, P.; Todisco, T.; Merante, F.; Nenci, G.G. Platelet activation and allergic asthma. N. Engl. J. Med. 1982, 306, 549. [Google Scholar]
- Morley, J.; Sanjar, S.; Page, C. The platelet in asthma. Lancet 1984, 324, 1142–1144. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, C.; Fang, H. Blood cell parameters and predicting coronary in-stent restenosis. Angiology 2019, 70, 711–718. [Google Scholar] [CrossRef]
- Kanagaratham, C.; El Ansari, Y.S.; Lewis, O.L.; Oettgen, H.C. IgE and IgG antibodies as regulators of mast cell and basophil functions in food allergy. Front. Immunol. 2020, 11, 603050. [Google Scholar] [CrossRef]
- Rivera, J.; Gilfillan, A.M. Molecular regulation of mast cell activation. J. Allergy Clin. Immunol. 2006, 117, 1214–1225. [Google Scholar] [CrossRef]
- Moldogazieva, N.T.; Mokhosoev, I.M.; Mel’Nikova, T.I.; Porozov, Y.B.; Terentiev, A.A. Oxidative stress and advanced lipoxidation and glycation end products (ALEs and AGEs) in aging and age-related diseases. Oxidative Med. Cell. Longev. 2019, 2019, 3085756. [Google Scholar] [CrossRef] [Green Version]
- Han, K.; Suzukawa, M.; Yamaguchi, M.; Sugimoto, N.; Nakase, Y.; Toda, T.; Nagase, H.; Ohta, K. The in vitro effects of advanced glycation end products on basophil functions. Int. Arch. Allergy Immunol. 2011, 155 (Suppl. S1), 64–70. [Google Scholar] [CrossRef]
- Sohouli, M.H.; Fatahi, S.; Sharifi-Zahabi, E.; Santos, H.O.; Tripathi, N.; Lari, A.; Pourrajab, B.; Kord-Varkaneh, H.; Găman, M.-A.; Shidfar, F. The impact of low advanced glycation end products diet on metabolic risk factors: A systematic review and meta-analysis of randomized controlled trials. Adv. Nutr. 2021, 12, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Toda, M.; Hellwig, M.; Henle, T.; Vieths, S. Influence of the maillard reaction on the allergenicity of food proteins and the development of allergic inflammation. Curr. Allergy Asthma Rep. 2019, 19, 4. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Gupta, K.; Sharma, A.; Das, M.; Ansari, I.A.; Dwivedi, P.D. Maillard reaction in food allergy: Pros and cons. Crit. Rev. Food Sci. Nutr. 2017, 58, 208–226. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non–ISR (n = 220) | ISR (n = 196) | p Value | |
|---|---|---|---|
| Male, n (%) | 168 (76.4) | 143 (73.0) | 0.425 |
| Age, y | 66.53 ± 9.43 | 67.59 ± 8.82 | 0.241 |
| Body mass index, kg/m2 | 25.50 ± 3.42 | 25.10 ± 3.46 | 0.235 |
| Smoking, n (%) | 63 (28.6) | 59 (30.1) | 0.743 |
| Hypertension, n (%) | 169 (76.8) | 160 (81.6) | 0.228 |
| Systolic blood pressure, mm Hg | 137.85 ± 20.40 | 140.26 ± 22.04 | 0.248 |
| Diastolic blood pressure, mm Hg | 74.41 ± 12.58 | 75.43 ± 14.69 | 0.448 |
| Dyslipidemia, n (%) | 25 (11.4) | 20 (10.2) | 0.704 |
| Serum creatinine, µmol/L | 80.00 (70.25–93.00) | 82.50 (68.00–99.75) | 0.518 |
| eGFR, mL/min per 1.73 m2 | 80.00 ± 17.26 | 78.77 ± 33.05 | 0.640 |
| HbA1c, % | 7.33 ± 1.35 | 7.64 ± 1.35 | 0.020 |
| Fasting blood glucose, mmol/L | 7.15 ± 2.28 | 7.66 ± 2.94 | 0.050 |
| Triglyceride, mmol/L | 1.75 ± 1.72 | 1.64 ± 1.16 | 0.442 |
| Total cholesterol, mmol/L | 3.62 ± 1.01 | 3.59 ± 1.03 | 0.823 |
| HDL cholesterol, mmol/L | 1.09 ± 0.27 | 1.04 ± 0.26 | 0.054 |
| LDL cholesterol, mmol/L | 2.04 ± 0.80 | 2.02 ± 0.85 | 0.877 |
| hsCRP, mg/L | 0.94 (0.41–2.24) | 1.15 (0.52–4.59) | 0.021 |
| IgE, ng/mL | 80.25 (30.65–202.50) | 187.10 (63.75–489.65) | <0.001 |
| CML, ng/mL | 174.26 (130.85–215.56) | 203.26 (164.50–266.84) | <0.001 |
| Ejection fraction, % | 62.46 ± 8.89 | 60.34 ± 10.54 | 0.028 |
| Medication, n (%) | |||
| Dual antiplatelet therapy | 209 (95.0) | 185 (94.4) | 0.781 |
| ACEI/ARB | 146 (66.4) | 132 (67.3) | 0.832 |
| β-Blockers | 183 (83.2) | 159 (81.1) | 0.584 |
| Statins | 217 (98.6) | 184 (93.9) | 0.009 |
| Diseased vessel, n (%) | |||
| Left main | 11 (5.0) | 19 (9.7) | 0.065 |
| Left anterior descending | 157 (71.4) | 153 (78.1) | 0.118 |
| Left circumflex | 98 (44.5) | 115 (58.7) | 0.004 |
| Right coronary artery | 108 (49.1) | 138 (70.4) | <0.001 |
| Severity of CAD, n (%) | |||
| 1-vessel | 114 (51.8) | 56 (28.6) | <0.001 |
| 2-vessel | 69 (31.4) | 70 (35.7) | 0.348 |
| 3-vessel | 37 (16.8) | 70 (35.7) | <0.001 |
| Multivessel disease | 106 (48.2) | 140 (71.4) | <0.001 |
| Lesion characteristics | |||
| Class B2/C lesion, n (%) | 135 (61.4) | 145 (74.0) | 0.006 |
| Bifurcation lesion, n (%) | 54 (24.5) | 71 (36.2) | 0.009 |
| Chronic total occlusion, n (%) | 23 (10.5) | 36 (18.4) | 0.021 |
| Pre-PCI stenosis, % | 85.86 ± 6.29 | 86.81 ± 8.20 | 0.189 |
| Average number of stents, n | 1.51 ± 0.71 | 1.63 ± 0.73 | 0.106 |
| DES-zotarolimus, n (%) | 98 (44.5) | 86 (43.9) | 0.891 |
| DES-everolimus, n (%) | 78 (35.5) | 76 (38.8) | 0.484 |
| DES-sirolimus, n (%) | 44 (20.0) | 34 (17.3) | 0.489 |
| Stent diameter, mm | 2.98 ± 0.40 | 2.84 ± 0.35 | <0.001 |
| Stent length, mm | 28.52 ± 2.57 | 28.13 ± 4.94 | 0.322 |
| Follow-up duration, months | 12.12 ± 0.82 | 12.23 ± 0.88 | 0.161 |
| Unadjusted r | Unadjusted p | * Adjusted r | * Adjusted p | |
|---|---|---|---|---|
| All | 0.331 | <0.001 | 0.324 | <0.001 |
| ISR | 0.433 | <0.001 | 0.441 | <0.001 |
| Non-ISR | 0.153 | 0.023 | 0.169 | 0.014 |
| Unadjusted OR | p-Value | Adjusted for Model 1 OR | p-Value | Adjusted for Model 2 OR | p-Value | |
|---|---|---|---|---|---|---|
| Log2 IgE per SD | 2.008 (1.613–2.500) | <0.001 | 2.066 (1.652–2.583) | <0.001 | 1.989 (1.567–2.526) | <0.001 |
| IgE tertiles | 1.831 (1.431–2.344) | <0.001 | 1.879 (1.461–2.417) | <0.001 | 1.773 (1.355–2.322) | <0.001 |
| 1st | Ref | Ref | Ref | |||
| 2st | 1.658 (1.019–2.697) | 0.042 | 1.757 (1.070–2.884) | 0.026 | 1.646 (0.971–2.790) | 0.064 |
| 3st | 3.346 (2.043–5.480) | <0.001 | 3.523 (2.129–5.829) | <0.001 | 3.137 (1.831–5.374) | <0.001 |
| Log2 CML per SD | 1.818 (1.445–2.287) | <0.001 | 1.824 (1.444–2.303) | <0.001 | 1.945 (1.507–2.509) | <0.001 |
| CML tertiles | 1.617 (1.268–2.061) | <0.001 | 1.608 (1.256–2.060) | <0.001 | 1.744 (1.333–2.282) | <0.001 |
| 1st | Ref | Ref | Ref | |||
| 2st | 1.334 (0.824–2.159) | 0.241 | 1.301 (0.797–2.124) | 0.292 | 1.543 (0.902–2.641) | 0.113 |
| 3st | 2.605 (1.604–4.231) | <0.001 | 2.574 (1.570–4.221) | <0.001 | 3.026 (1.768–5.179) | <0.001 |
| C-Statistic | p-Value | p for comparison | Categorical NRI | p-Value | IDI | p-Value | |
|---|---|---|---|---|---|---|---|
| Established risk factors | 0.705 (0.655–0.755) | <0.001 | Ref | Ref | Ref | ||
| Established risk factors + IgE | 0.759 (0.713–0.804) | <0.001 | <0.01 | 0.120 (0.047–0.194) | <0.01 | 0.074 (0.049–0.010) | <0.01 |
| Established risk factors + CML | 0.748 (0.701–0.794) | <0.001 | <0.01 | 0.099 (0.034–0.163) | <0.01 | 0.062 (0.038–0.086) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Chen, Q.; Lu, L.; Jin, Q.; Bao, Y.; Ling, T.; Lin, C.; Ding, F.; Wang, X.; Shen, W.; et al. Association of Circulating IgE and CML Levels with In-Stent Restenosis in Type 2 Diabetic Patients with Stable Coronary Artery Disease. J. Cardiovasc. Dev. Dis. 2022, 9, 157. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9050157
Liu J, Chen Q, Lu L, Jin Q, Bao Y, Ling T, Lin C, Ding F, Wang X, Shen W, et al. Association of Circulating IgE and CML Levels with In-Stent Restenosis in Type 2 Diabetic Patients with Stable Coronary Artery Disease. Journal of Cardiovascular Development and Disease. 2022; 9(5):157. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9050157
Chicago/Turabian StyleLiu, Jingmeng, Qiujing Chen, Lin Lu, Qi Jin, Yangyang Bao, Tianyou Ling, Changjian Lin, Fenghua Ding, Xiaoqun Wang, Weifeng Shen, and et al. 2022. "Association of Circulating IgE and CML Levels with In-Stent Restenosis in Type 2 Diabetic Patients with Stable Coronary Artery Disease" Journal of Cardiovascular Development and Disease 9, no. 5: 157. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9050157