
Long-Term Outcomes after Aortic Valve and Root Replacement in a Very High-Risk Population
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
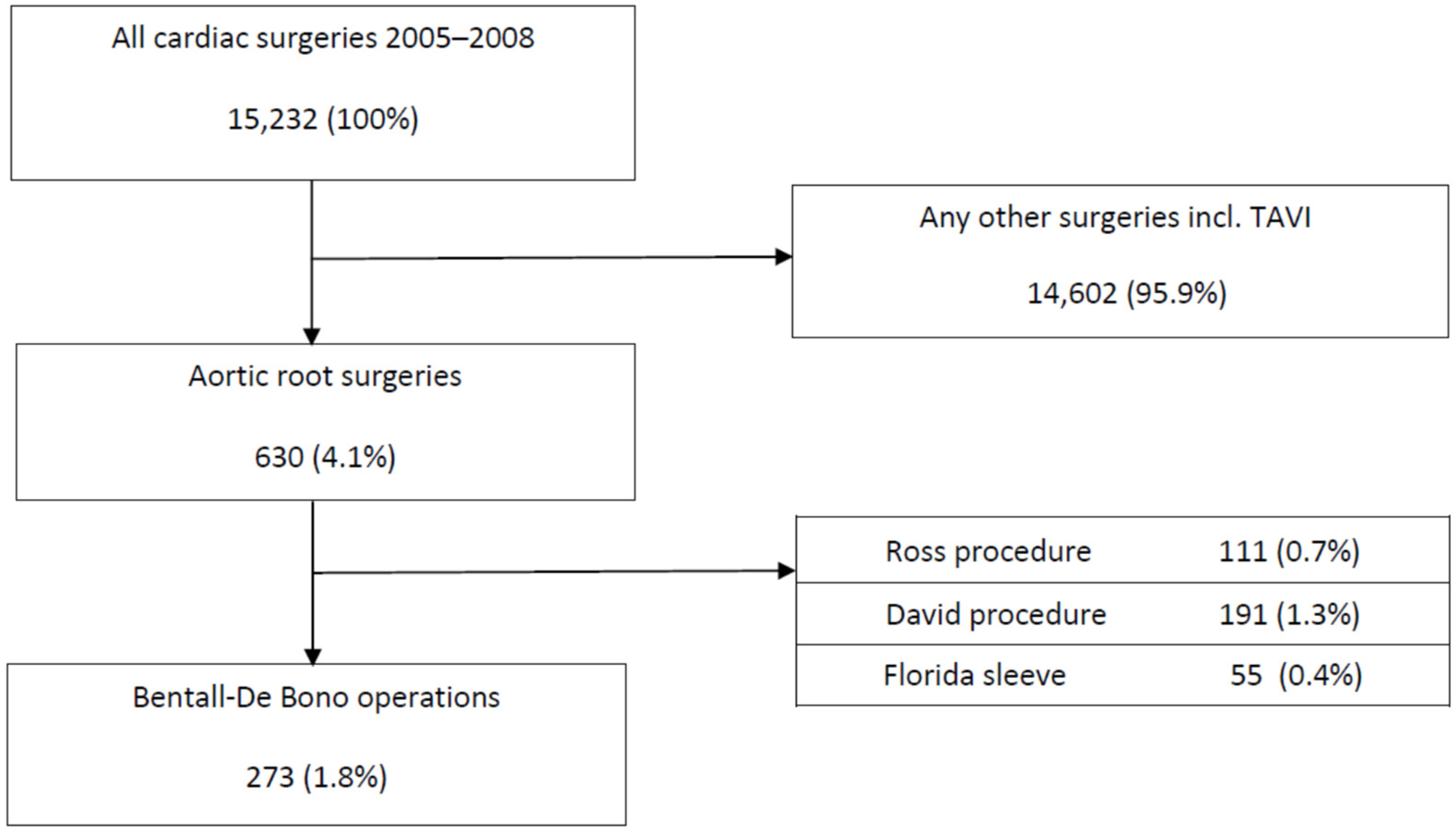
2.2. Study Design and Patient Selection
2.3. Patient Management
2.4. Surgical Technique
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Operative Data
3.3. Early Postoperative Outcomes
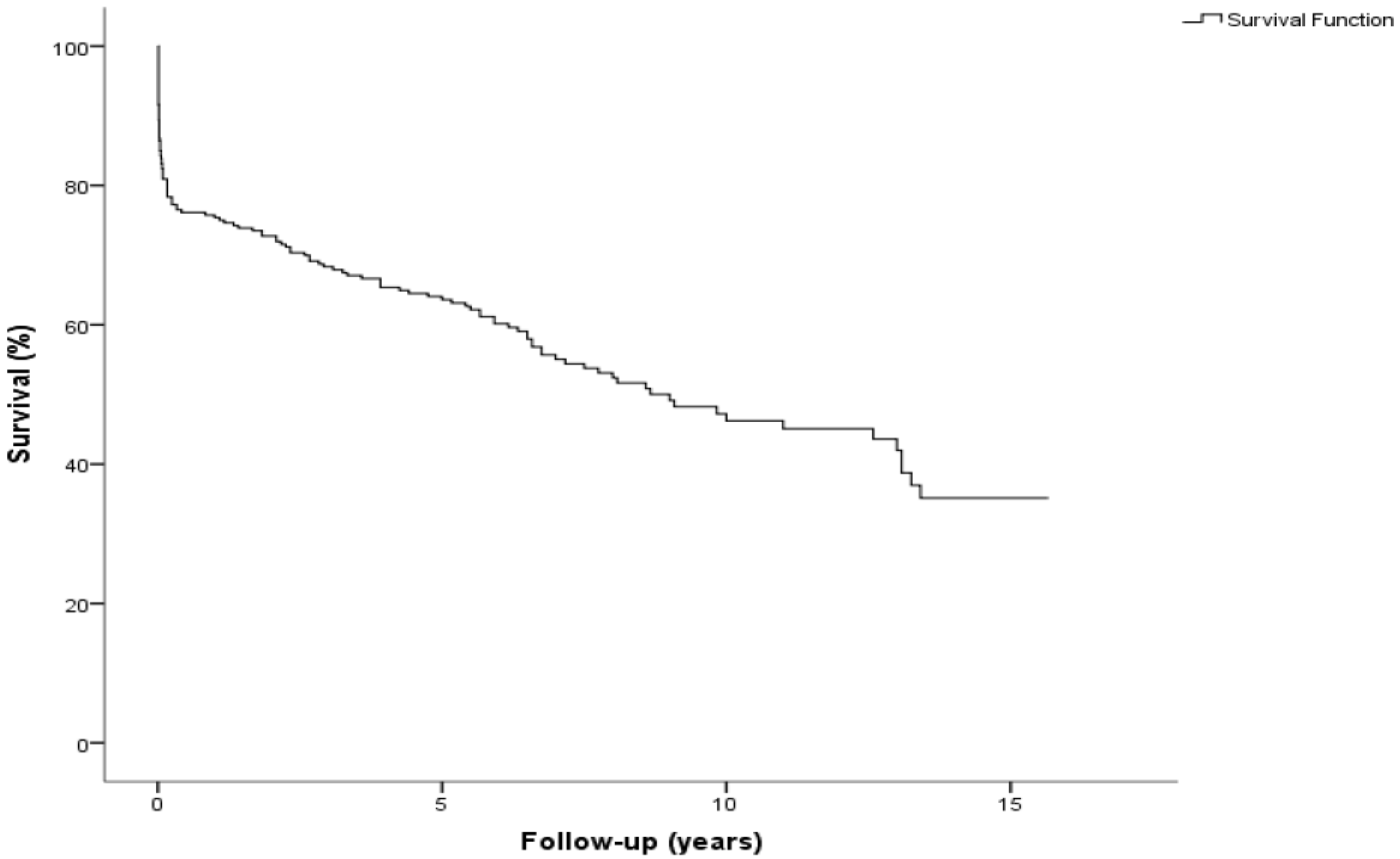
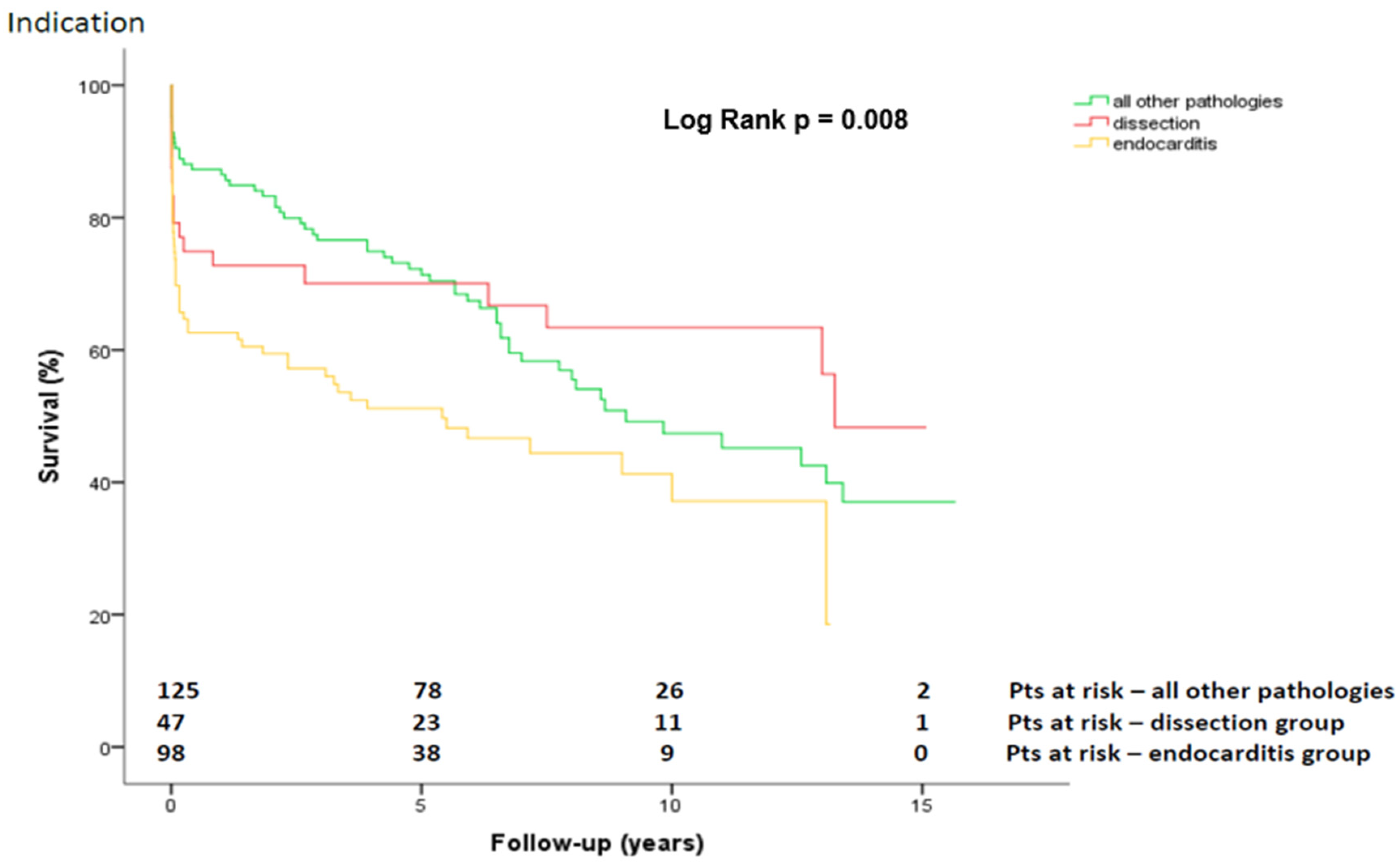
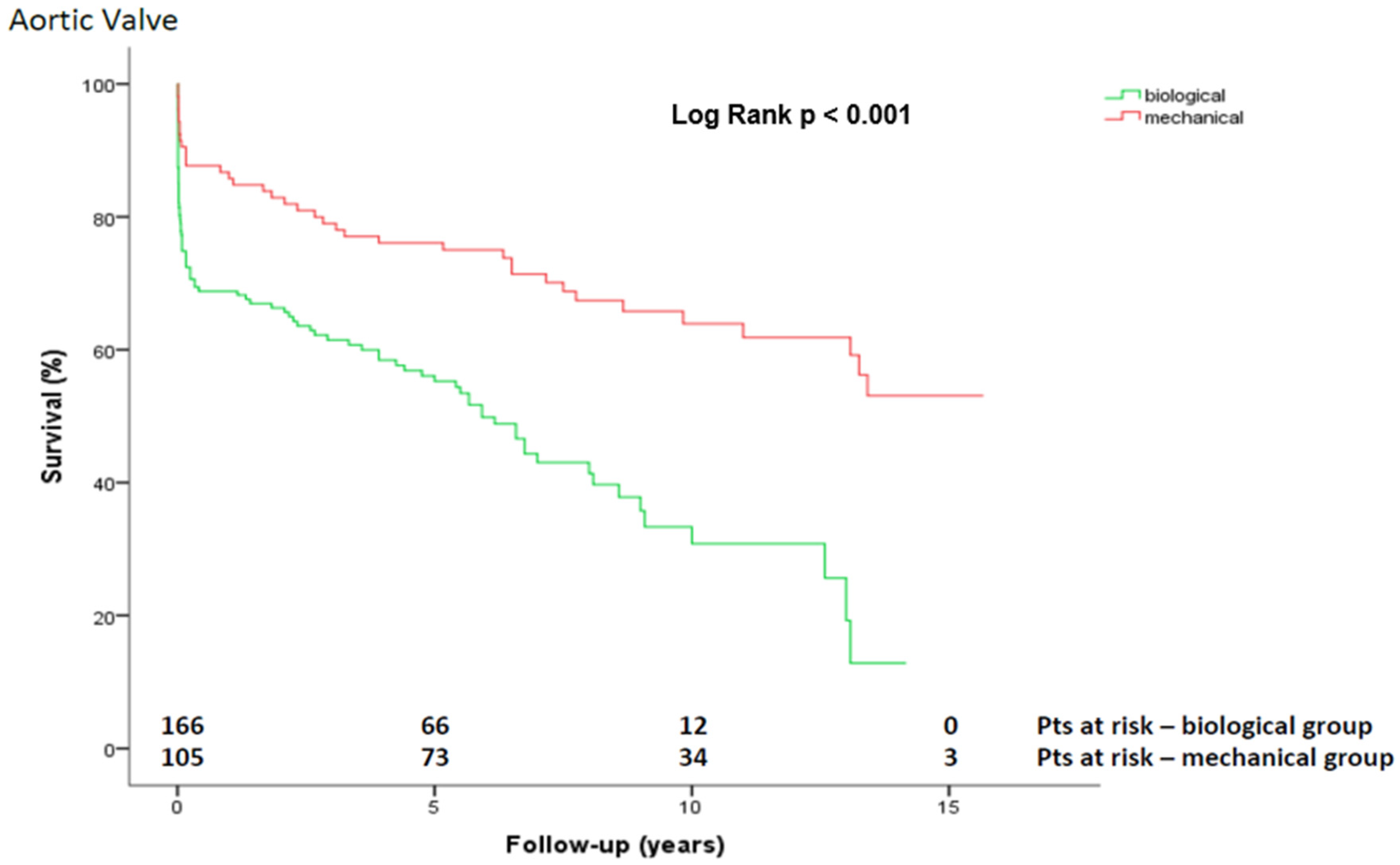
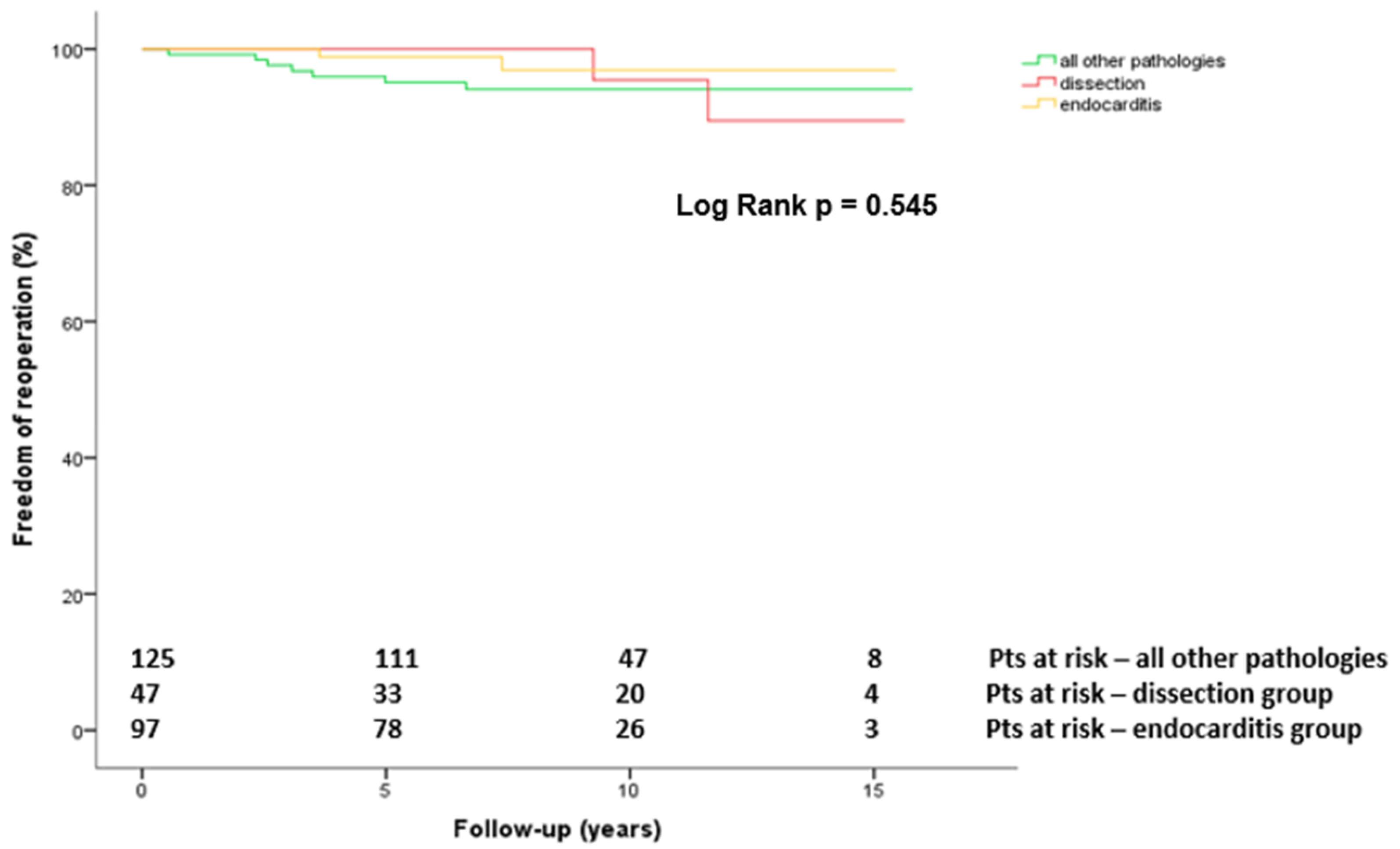
3.4. Late Postoperative Outcomes
4. Discussion
Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bentall, H.; De Bono, A. A technique for complete replacement of the ascending aorta. Thorax 1968, 23, 338–339. [Google Scholar] [CrossRef] [PubMed]
- Cabrol, C.; Pavie, A.; Gandjbakhch, I.; Villemot, J.P.; Guiraudon, G.; Laughlin, L.; Etievent, P.; Cham, B. Complete replacement of the ascending aorta with reimplantation of the coronary arteries: New surgical approach. J. Thorac. Cardiovasc. Surg. 1981, 81, 309–315. [Google Scholar] [CrossRef]
- Kouchoukos, N.T.; Wareing, T.H.; Murphy, S.F.; Perrillo, J.B. Sixteen-year Experience with Aortic Root Replacement. Ann. Surg. 1991, 214, 308–320. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.N. Replacement of aortic and mitral valves with a pulmonary autograft. Lancet Lond. Engl. 1967, 2, 956–958. [Google Scholar] [CrossRef]
- Aboud, A.; Charitos, E.I.; Fujita, B.; Stierle, U.; Reil, J.C.; Voth, V.; Liebrich, M.; Andreas, M.; Holubec, T.; Bening, C.; et al. Long-Term Outcomes of Patients Undergoing the Ross Procedure. J. Am. Coll. Cardiol. 2021, 77, 1412–1422. [Google Scholar] [CrossRef]
- El-Hamamsy, I.; Toyoda, N.; Itagaki, S.; Stelzer, P.; Varghese, R.; Williams, E.E.; Egorova, N.; Adams, D.H. Propensity-Matched Comparison of the Ross Procedure and Prosthetic Aortic Valve Replacement in Adults. J. Am. Coll. Cardiol. 2022, 79, 805–815. [Google Scholar] [CrossRef]
- Sarsam, M.A.; Yacoub, M. Remodeling of the aortic valve anulus. J. Thorac. Cardiovasc. Surg. 1993, 105, 435–438. [Google Scholar] [CrossRef]
- David, T.E.; Feindel, C.M. An aortic valve-sparing operation for patients with aortic incompetence and aneurysm of the ascending aorta. J. Thorac. Cardiovasc. Surg. 1992, 103, 617–621. [Google Scholar] [CrossRef]
- De Paulis, R.; Chirichilli, I.; Scaffa, R.; Weltert, L.; Maselli, D.; Salica, A.; Guerrieri Wolf, L.; Bellisario, A.; Chiariello, L. Long-term results of the valve reimplantation technique using a graft with sinuses. J. Thorac. Cardiovasc. Surg. 2016, 151, 112–119. [Google Scholar] [CrossRef]
- David, T.E.; David, C.M.; Ouzounian, M.; Feindel, C.M.; Lafreniere-Roula, M. A progress report on reimplantation of the aortic valve. J. Thorac. Cardiovasc. Surg. 2021, 161, 890–899. [Google Scholar] [CrossRef]
- Tamer, S.; Mastrobuoni, S.; Lemaire, G.; Jahanyar, J.; Navarra, E.; Poncelet, A.; Astarci, P.; El Khoury, G.; de Kerchove, L. Two decades of valve-sparing root reimplantation in tricuspid aortic valve: Impact of aortic regurgitation and cusp repair. Eur. J. Cardiothorac. Surg. 2021, 59, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Etz, C.D.; Homann, T.M.; Silovitz, D.; Spielvogel, D.; Bodian, C.A.; Luehr, M.; DiLuozzo, G.; Plestis, K.A.; Griepp, R.B. Long-Term Survival After the Bentall Procedure in 206 Patients with Bicuspid Aortic Valve. Ann. Thorac. Surg. 2007, 84, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, S.; Lentini, S.; Rinaldi, M.; D’armini, A.M.; Tancredi, F.; Raffa, G.; Gaeta, R.; Viganó, M. Treatment of ascending aorta disease with Bentall-De Bono operation using a mini-invasive approach. J. Cardiovasc. Med. Hagerstown Md. 2008, 9, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Mookhoek, A.; Korteland, N.M.; Arabkhani, B.; Di Centa, I.; Lansac, E.; Bekkers, J.A.; Bogers, A.J.; Takkenberg, J.J. Bentall Procedure: A Systematic Review and Meta-Analysis. Ann. Thorac. Surg. 2016, 101, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Salem, R.; Zierer, A.; Karimian-Tabrizi, A.; Miskovic, A.; Moritz, A.; Risteski, P.; Monsefi, N. Aortic Valve Repair for Aortic Insufficiency or Dilatation: Technical Evolution and Long-term Outcomes. Ann. Thorac. Surg. 2020, 110, 1967–1973. [Google Scholar] [CrossRef]
- Hogervorst, E.K.; Rosseel, P.M.J.; van de Watering, L.M.G.; Brand, A.; Bentala, M.; van der Meer, B.J.; van der Bom, J.G. Prospective validation of the EuroSCORE II risk model in a single Dutch cardiac surgery centre. Neth. Heart J. 2018, 26, 540–551. [Google Scholar] [CrossRef]
- Pacini, D.; Ranocchi, F.; Angeli, E.; Settepani, F.; Pagliaro, M.; Martin-Suarez, S.; Di Bartolomeo, R.; Pierangeli, A. Aortic root replacement with composite valve graft. Ann. Thorac. Surg. 2003, 76, 90–98. [Google Scholar] [CrossRef]
- Lawrie, G.M.; Earle, N.; DeBakey, M.E. Long-term fate of the aortic root and aortic valve after ascending aneurysm surgery. Ann. Surg. 1993, 217, 711–720. [Google Scholar] [CrossRef]
- Di Marco, L.; Pacini, D.; Pantaleo, A.; Leone, A.; Barberio, G.; Marinelli, G.; Di Bartolomeo, R. Composite valve graft implantation for the treatment of aortic valve and root disease: Results in 1045 patients. J. Thorac. Cardiovasc. Surg. 2016, 152, 1041–1048. [Google Scholar] [CrossRef]
- Gott, V.L.; Gillinov, A.M.; Pyeritz, R.E.; Cameron, D.E.; Reitz, B.A.; Greene, P.S.; Stone, C.D.; Ferris, R.L.; Alejo, D.E.; McKusick, V.A. Aortic root replacement. Risk factor analysis of a seventeen-year experience with 270 patients. J. Thorac. Cardiovasc. Surg. 1995, 109, 536–544. [Google Scholar] [CrossRef]
- Pantaleo, A.; Murana, G.; Di Marco, L.; Jafrancesco, G.; Barberio, G.; Berretta, P.; Leone, A.; Di Bartolomeo, R.; Pacini, D. Biological versus mechanical Bentall procedure for aortic root replacement: A propensity score analysis of a consecutive series of 1112 patients. Eur. J. Cardiothorac. Surg. 2017, 52, 143–149. [Google Scholar] [CrossRef]
- Puluca, N.; Burri, M.; Cleuziou, J.; Krane, M.; Lange, R. Consecutive operative procedures in patients with Marfan syndrome up to 28 years after initial aortic root surgery. Eur. J. Cardiothorac Surg. 2018, 54, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Joo, H.C.; Chang, B.C.; Youn, Y.N.; Yoo, K.J.; Lee, S. Clinical experience with the Bentall procedure: 28 years. Yonsei Med. J. 2012, 53, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Prifti, E.; Bonacchi, M.; Frati, G.; Proietti, P.; Giunti, G.; Babatasi, G.; Massetti, M.; Sani, G. Early and long-term outcome in patients undergoing aortic root replacement with composite graft according to the Bentall’s technique. Eur. J. Cardio-Thorac. Surg. 2002, 21, 15–21. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 273) | Dissection (n = 48) | Endocarditis (n = 99) | All Other Pathologies (n = 126) | p-Value |
|---|---|---|---|---|---|
| Mean age ± SD (years) | 64 ± 12.8 | 54.8 ± 14.5 | 65.8 ± 12.8 | 66.2 ± 10.4 | 0.10 |
| Female | 62 (22.7%) | 12 (25%) | 22 (22%) | 28 (22%) | 0.92 |
| NYHA ˃ II | 171 (62.6%) | 26 (54%) | 73 (73%) | 72 (57%) | <0.001 |
| Atrial fibrillation | 59 (21.6%) | 0 | 30 (30%) | 29 (23%) | <0.001 |
| Pacemaker rhythm | 19 (7%) | 2 (4%) | 6 (6%) | 11 (9%) | 0.006 |
| Previous cardiac surgery | 113 (41.4%) | 2 (4%) | 79 (80%) | 32 (25%) | <0.001 |
| CAD | 101 (36.9%) | 9 (19%) | 41 (41%) | 51 (40%) | 0.017 |
| Hypertension | 250 (91.6%) | 39 (81%) | 88 (89%) | 123 (98%) | 0.001 |
| Pulmonary hypertension | 105 (38.5%) | 3 (6%) | 48 (48%) | 54 (43%) | <0.001 |
| Heart failure upon admission | 98 (35.9%) | 12 (25%) | 50 (51%) | 36 (29%) | 0.001 |
| PAD | 16 (5.8%) | 3 (6%) | 8 (8%) | 5 (4%) | 0.42 |
| Diabetes | 43 (15.7%) | 6 (13%) | 21 (21%) | 16 (13%) | 0.174 |
| COPD | 90(32.9%) | 4 (8%) | 38 (38%) | 48 (38%) | <0.001 |
| Preoperative stroke | 50 (18.3%) | 5 (10%) | 34 (34%) | 11 (9%) | <0.001 |
| Renal insufficiency | 97 (35.5%) | 15 (31%) | 43 (43%) | 39 (31%) | 0.12 |
| Bicuspid AV | 70 (25.6%) | 11 (23%) | 9 (9%) | 50 (40%) | <0.001 |
| EF (%) | 56.428 | 58.41 | 55.894 | 56.53 | 0.96 |
| AV gradient mean (mmHg) | 24.49 | 17.15 | 20.06 | 27.87 | 0.90 |
| Ascending aortic diameter (mm) | 44.09 | 56.58 | 35.56 | 47.00 | <0.001 |
| AR ˃ moderate | 91 (33.3%) | 21 (42%) | 31 (31%) | 39 (28%) | 0.002 |
| Variable | Overall (n = 273) | Dissection Group (n = 48) | Endocarditis Group (n = 99) | All Other Pathologies (n = 126) | p-Value |
|---|---|---|---|---|---|
| Timing of operation | <0.001 | ||||
| Emergency | 62 (22.7%) | 44 (92%) | 15 (15%) | 3 (2%) | |
| Urgent | 69 (25.3%) | 2 (4%) | 45 (46%) | 22 (18%) | |
| Elective | 142 (52%) | 2 (4%) | 39 (39%) | 101 (80%) | |
| AV prosthesis | <0.001 | ||||
| Biological | 167 (61.2%) | 14 (29%) | 78 (79%) | 75 (60%) | |
| Mechanical | 106 (38.8%) | 34 (71%) | 21 (21%) | 51 (40%) | |
| Conduit diameter, mean (mm) | 25.1 | 25.5 | 24.6 | 25.4 | 0.05 |
| Concomitant surgery | <0.001 | ||||
| CABG | 62 (22.7%) | 10 (21%) | 14 (14%) | 38 (30%) | |
| MV replacement | 6 (2.2%) | 0 | 3 (3%) | 3 (2%) | |
| MV repair | 26 (9.5%) | 0 | 12 (12%) | 14 (11%) | |
| TV repair | 26 (9.5%) | 0 | 8 (8%) | 18 (14%) | |
| Minimally invasive | 48 (17.6%) | 2 (4%) | 10 (10%) | 36 (29%) | |
| CPB time, median (range), minutes | 193 (477–60) | 213 (477–106) | 211 (431–107) | 173 (439–60) | 0.58 |
| Cross-clamp time, median (range), minutes | 131 (374–47) | 137 (374–69) | 140 (239–71) | 122 (253–47) | 0.72 |
| Variable | Overall (n = 273) | Dissection (n = 48) | Endocarditis (n = 99) | All Other Pathologies (n = 126) | p-Value |
|---|---|---|---|---|---|
| Re-exploration for bleeding | 55 (20.1%) | 9 (19%) | 22 (22%) | 24 (19%) | 0.81 |
| Stroke | 13 (4.7%) | 3 (6%) | 6 (6%) | 1 (0.8%) | 0.003 |
| Renal failure (dialysis) | 68 (24.9%) | 11 (23%) | 39 (40%) | 18 (14%) | < 0.001 |
| Permanent pacemaker | 24 (8.8%) | 7 (15%) | 11 (11%) | 6 (5%) | 0.07 |
| Myocardial infarction | 7 (2.6%) | 1 (2%) | 3 (3%) | 3 (2%) | 0.93 |
| Pericardial effusion | 59 (21.6%) | 9 (19%) | 27 (27%) | 23 (18%) | 0.81 |
| Wound healing disorder | 20 (7.3%) | 2 (4%) | 9 (9%) | 9 (7%) | 0.62 |
| New onset AF | 39 (14.3%) | 1 (2%) | 14 (14%) | 24 (19%) | |
| 30-day mortality | 47 (17.2%) | 9 (19%) | 26 (26%) | 12 (10%) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hlavicka, J.; Antonov, K.; Salem, R.; Hecker, F.; Marinos, S.; Radwan, M.; Emrich, F.; Van Linden, A.; Moritz, A.; Walther, T.; et al. Long-Term Outcomes after Aortic Valve and Root Replacement in a Very High-Risk Population. J. Cardiovasc. Dev. Dis. 2022, 9, 197. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060197
Hlavicka J, Antonov K, Salem R, Hecker F, Marinos S, Radwan M, Emrich F, Van Linden A, Moritz A, Walther T, et al. Long-Term Outcomes after Aortic Valve and Root Replacement in a Very High-Risk Population. Journal of Cardiovascular Development and Disease. 2022; 9(6):197. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060197
Chicago/Turabian StyleHlavicka, Jan, Kiril Antonov, Razan Salem, Florian Hecker, Spiros Marinos, Medhat Radwan, Fabian Emrich, Arnaud Van Linden, Anton Moritz, Thomas Walther, and et al. 2022. "Long-Term Outcomes after Aortic Valve and Root Replacement in a Very High-Risk Population" Journal of Cardiovascular Development and Disease 9, no. 6: 197. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060197